
Abstract
Introduction:
Medically complex community-based health center (CHC) patients face barriers accessing specialty care. Electronic consultations (eConsults) could mitigate these barriers by improving CHC providers’ access to specialist knowledge. We described patient, provider, and clinic characteristics of eConsult utilization in CHCs.
Study Design:
Analyzed electronic health record data from adult patients from April 1, 2021, to March 31, 2024.
Results:
Among 1,690,788 patients and 13,769 providers from 437 CHC sites (18 states), there were 20,066 eConsults (17,066 patients; 1,390 providers), with wide variation in the characteristics of patients for whom providers requested eConsults. Ten percent of providers ever requested an eConsult, with the highest rates among nurse practitioners and physicians; 73% of providers who requested an eConsult did so <10 times. eConsult documentation rates were highest in urban CHCs.
Conclusions:
We found substantial variation in eConsult use in CHCs. Opportunities to support specialty care access for CHC patients should be further explored.
Introduction
Community-based health centers (CHCs), which include Federally Qualified Health Centers and rural health clinics, provide primary care to low-income patients regardless of patient ability to pay; these clinics serve 1 in 12 people nationally.1,2 Two-thirds of patients served by CHCs are from households below the federal poverty level, 20% are uninsured, and 50% are insured by Medicaid. 1 Patients served by CHCs are more medically complex than the general population and have higher rates of chronic conditions. 1
Primary care services include helping patients manage chronic conditions,3,4 but primary care clinicians do not always have the expertise needed for medically complex patients. 1 In some care settings, primary care providers are readily able to refer such patients to specialists and/or consult with specialists directly. For CHC patients and their providers, however, this is not the case. Access to specialists can be limited for many reasons, including specialty care providers’ unwillingness to accept Medicaid-insured or uninsured patients 5 and an increasing shortage of specialists in rural areas. 6 Even when specialist referrals are ordered by a primary care provider, many CHC patients are unable to complete them. In one study, nearly a quarter of specialty care referrals in CHCs were not completed, and patients experiencing more barriers to accessing this care were less likely to complete their referral. 7 These limitations in specialty care access among low-income/rural populations have substantial health implications, since lack of access to specialist care is associated with increased mortality. 8
One way to overcome some of these barriers includes CHC primary care providers consulting virtually with specialists through the use of electronic consultations (eConsults). eConsults enable CHC providers to obtain specialist advice by virtually connecting them with a specialist for input on a patient’s treatment plan, including whether a referral for an in-person visit is needed. Studies in CHCs showed that eConsults enhanced CHC provider knowledge 9 and decreased time to specialty care input. 10 There is emerging evidence for the benefits eConsults can confer. In one study, CHC providers used eConsults for a variety of specialty care needs and followed specialist recommendations in three-quarters of these cases. 11 Another study showed that eConsults resulted in avoidance of subsequent referral for in-person consultation in 23 − 76% of cases, varying by specialty. 12
This evidence suggests that potential benefits of eConsult use in the CHC setting include ensuring that primary care providers obtain specialist input on a given patient and reduce the need for in-person specialist visits. However, the few studies on eConsults conducted in CHCs were primarily restricted to a single clinic or health system.7,9–11,13,14 As a result, little is known about the extent to which eConsults are used in CHC primary care clinics across the United States (U.S.) and the type of patients for whom they are used. To address this knowledge gap, this study describes patient, provider, and CHC characteristics of eConsult utilization in a network of CHCs across the U.S. Results will help inform the development of strategies for increasing access to specialty care for CHC patients.
Methods
STUDY DESIGN, SETTING, AND POPULATION
This retrospective descriptive study used electronic health record (EHR) data from the Accelerating Data Value Across a National Community Health Center Network (ADVANCE) Clinical Research Network (CRN). Data for these analyses are from the OCHIN network, which provides a single instance of the Epic EHR to >2,000 CHC clinic sites. 15 We included encounters from patients 18 and older with at least one visit during the study period (April 1, 2021–March 31, 2024) to one of the 437 primary care CHCs within 18 states during the study period.
DEPENDENT VARIABLE
To identify completed eConsult requests, we utilized encounter data, billing codes, and internal procedure codes referencing use of one of the three eConsult platforms available within the OCHIN EHR. If an eConsult was identified in one of these areas, we considered the visit to have resulted in a completed eConsult request. Patients were identified as ever or never having an eConsult requested by a provider during the study period. We grouped eConsults by unique National Provider Index (NPI) to identify providers who ever or never requested an eConsult as well as to identify the number of eConsults requested by each provider. Finally, clinics were uniquely assigned as ever or never requesting an eConsult within the study period.
INDEPENDENT VARIABLES
Patient characteristics were derived from EHR data and included age (18–29, 30–39, 40–49, 50–64, 65+), sex (female, male), race and ethnicity (Hispanic White, Hispanic all other races, Non-Hispanic Asian, Non-Hispanic Black, Non-Hispanic White, Non-Hispanic all other races, unknown ethnicity all races, unknown ethnicity and race), preferred language (English, Spanish, Other), Carlson Comorbidity Index 16 (CCI) (0,1, 2, and 3+), insurance type (Medicaid, Medicare, other public insurance, private insurance, and uninsured), patient’s place of residence at the time of the visit (urban, large rural, small/isolated rural/unknown residence), and region (West, South, Midwest, and Northeast).
Analyses included provider type (Doctor of Osteopathic Medicine, medical doctor, nurse practitioner [NP], physician assistant, certified medical assistant, medical assistant, registered nurse, and other/unknown). Provider type was assigned using the NPI number, and primary taxonomy was utilized where available, and the EHR provider type was used when NPI taxonomy data were unavailable.
Clinic characteristics included rurality (urban, large rural, small/isolated rural, and unknown), region (West, South, Midwest, and Northeast), percentage of encounters conducted via telehealth, and average number of eConsults completed by clinic size: small (46–892 patients), medium (894–2,530 patients), medium-large (2,531–4,794), and large (≥4,795).
DESCRIPTIVE ANALYSES
We conducted descriptive analyses to examine patient, provider and clinic characteristics in cases where an eConsult request was completed in the study’s primary care CHCs. We compared characteristics of patients for whom at least one eConsult was requested (patients with eConsults) versus those for whom an eConsult was never requested (patients with no eConsults) during the study period. Similarly, we compared characteristics of providers who requested at least one eConsult (providers with eConsults) versus those who had never requested an eConsult (providers with no eConsults); we also examined the number of eConsults requested by each provider. Last, we compared characteristics of CHCs at which at least one eConsult was requested (clinics with eConsults) versus those at which none were requested (clinics w/no eConsults).
SAS EG 8.4 was used for all analyses. This study was deemed exempt by the Advarra Institutional Review Board.
Results
The study sample included 1,690,788 patients with 11,034,262 encounters from 13,769 providers. We identified 20,066 eConsult requests (17,066 patients; 1,390 providers). These eConsults resulted from both in-person (73.0%) and telehealth (27.0%) visits.
The characteristics of patients with eConsults and those without an eConsult are presented in Table 1. Only 1.0% of patients received ≥1 eConsult. A greater percentage of patients for whom an eConsult was requested were 65 years or older (18.4% with an eConsult vs. 12.8% without), female (64.3% with vs. 56.9% without), Non-White Hispanic (19.3% with vs. 10.4% without), or Medicaid insured (44.7% with vs. 41.8% without), or uninsured (36.5% with vs. 31.5% without); primarily spoke Spanish (32.2% with vs. 24.3% without); had a CCI of ≥3 (31.8% with vs. 22.2% without); and lived in an urban area (93.3% with vs. 85.4% without) or in the Western part of the United States (92.7% with vs. 63.7% without). A smaller percentage of patients with eConsults compared to those with none were 18–29 years old (18.1% with vs. 24.1% without), Hispanic White (20.8% with vs. 25.0% without), had a CCI of zero (32.0% with vs. 48.8% without), and were privately insured (6.3% with vs. 15.4% without).
Patient Characteristics of Those with a Documented eConsult and Those without
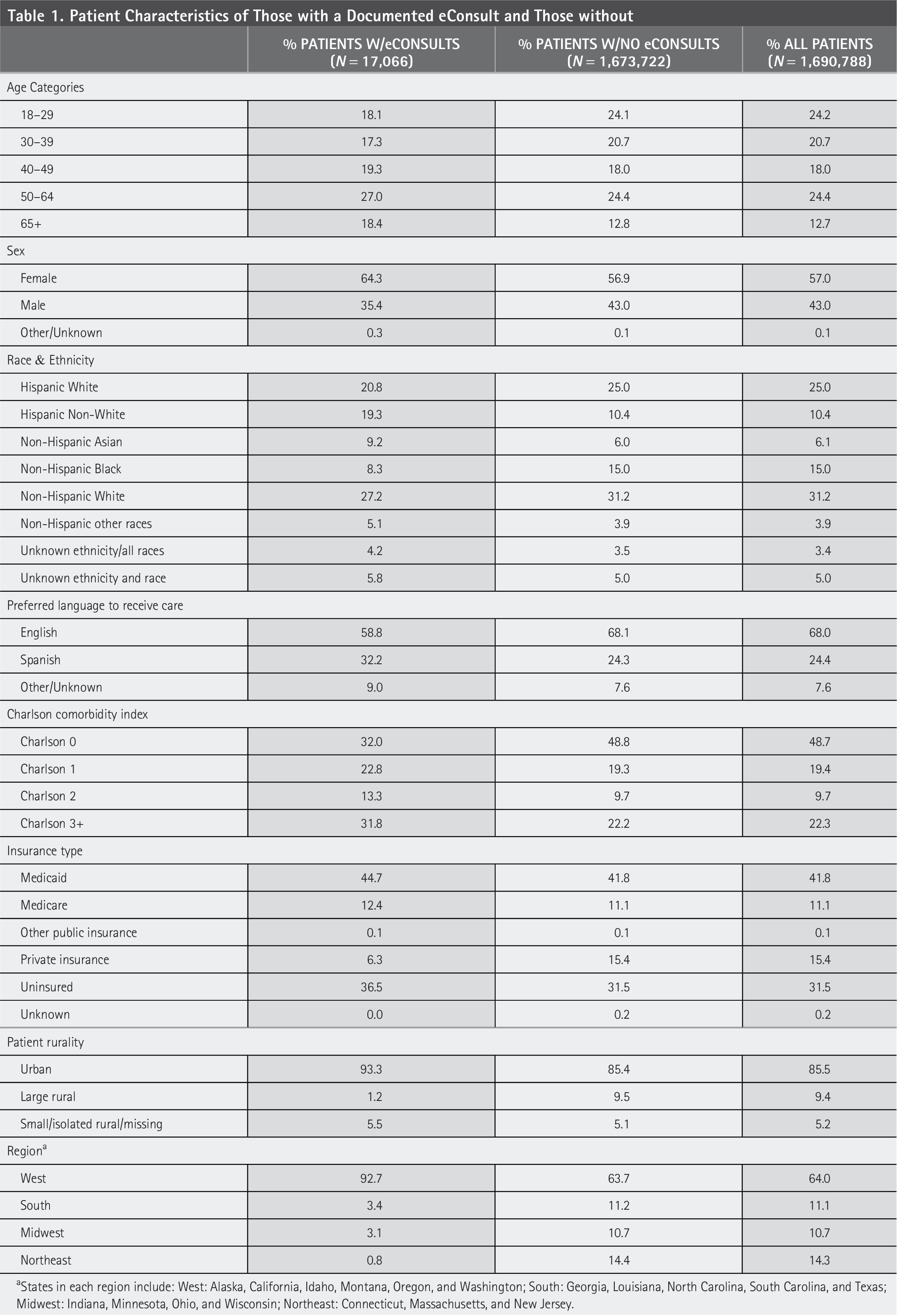
States in each region include: West: Alaska, California, Idaho, Montana, Oregon, and Washington; South: Georgia, Louisiana, North Carolina, South Carolina, and Texas; Midwest: Indiana, Minnesota, Ohio, and Wisconsin; Northeast: Connecticut, Massachusetts, and New Jersey.
Only 10% (1,390/13,769) of providers requested an eConsult (Table 2). Among providers requesting an eConsult, 37.8% requested just one eConsult, 34.7% requested 2–9 eConsults, 20.1% requested 10–49 eConsults, and 7.4% requested ≥50 eConsults. Finally, a greater percentage of physicians (36.4% vs. 17.2%), NPs (29.0% vs. 11.6%), and PAs (10.3% vs. 3.0%) requested an eConsult as compared to none.
Provider Characteristics: Number of eConsults Provided and Type of Provider Using eConsults
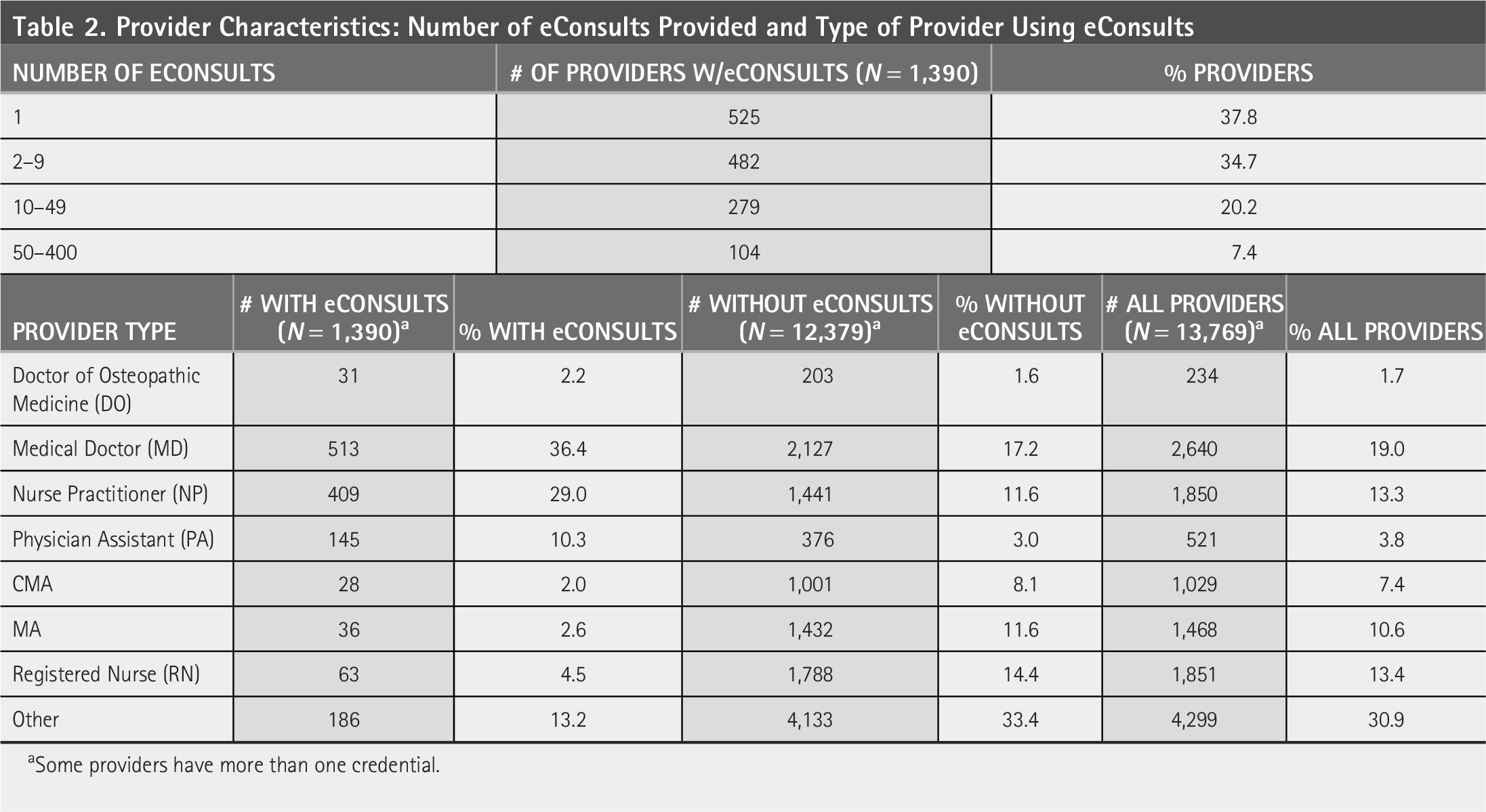
Some providers have more than one credential.
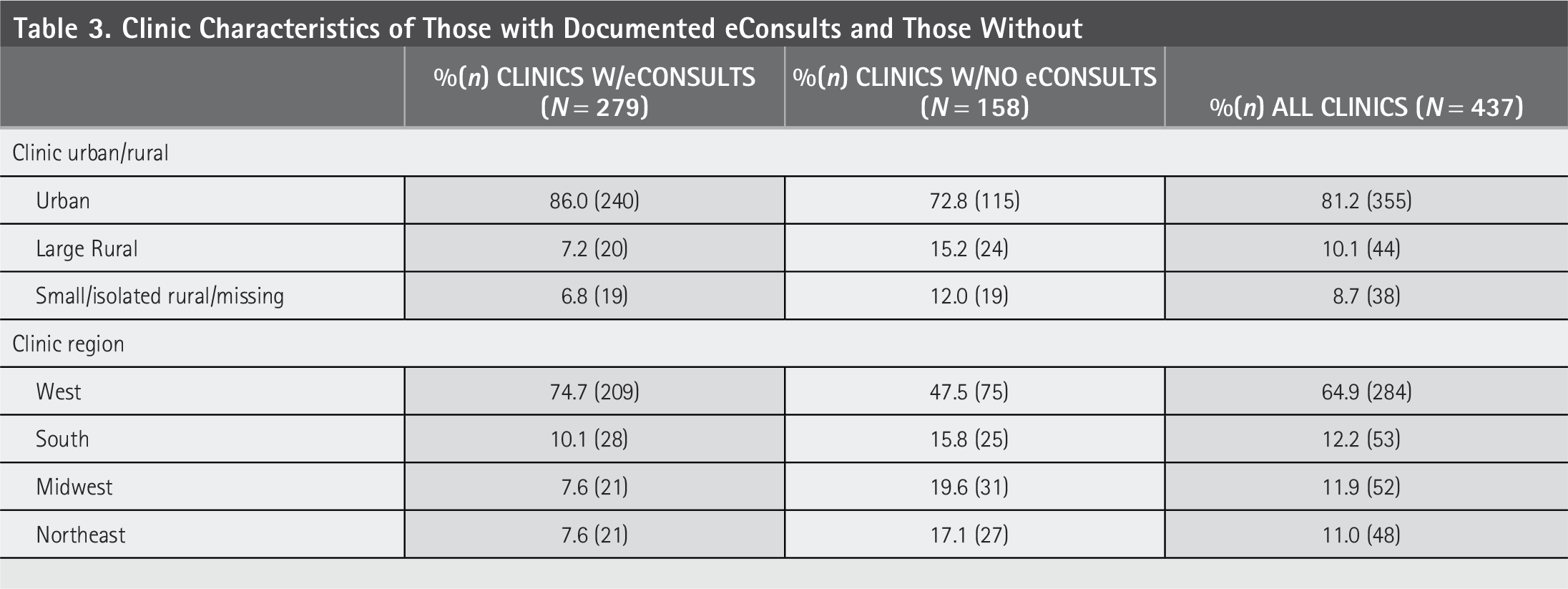
Table 3 shows characteristics of CHCs with an eConsult compared to CHCs without eConsults. A greater percentage of clinics in urban areas (86.0% vs. 72.8%) or in the West (74.7% vs. 47.5%) requested at least one eConsult versus never requesting them, whereas a lower percentage of CHCs in large rural areas (7.2% vs. 15.2%) or small/isolated rural areas (6.8% vs. 12.0%) requested eConsults as compared to never requesting them.
Clinic Characteristics of Those with Documented eConsults and Those Without
At a majority of clinics (63.8%), at least one eConsult was requested during the study period (Table 4). Among large clinics, a higher rate requested eConsults versus not (31.2% vs. 14.6%), whereas in small clinics, a lower rate requested eConsults versus not (20.1% vs. 33.5%). Clinics requesting eConsults, regardless of clinic size, also provided a higher rate of telehealth visits than those that did not request eConsults (large clinics: 25.3% vs. 22.8%). Furthermore, the rate of telehealth visits was more consistent in clinics requesting eConsults across all sizes (18.8% in small clinics vs. 25.3% in large clinics) as compared to clinics not requesting eConsults (9.4% in small clinics vs. 22.8% in large clinics).
Clinic Sizes a and Provision of eConsults and Other Telehealth Services
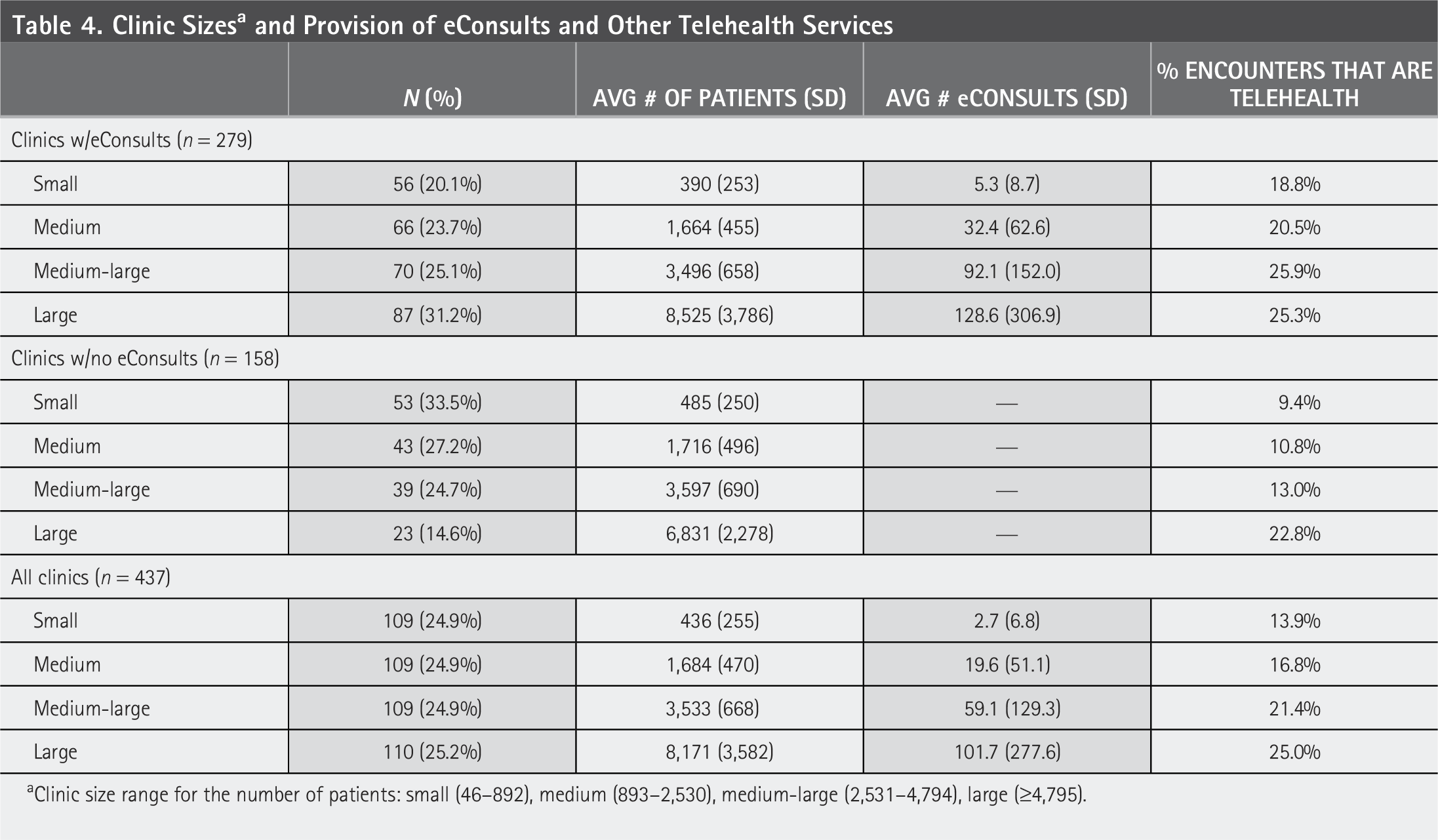
Clinic size range for the number of patients: small (46–892), medium (893–2,530), medium-large (2,531–4,794), large (≥4,795).
Discussion
As 63% of study CHCs ever requested eConsults, and many of these clinics requested very few, there is still substantial opportunity for expansion within this setting. There is a need to understand clinic and provider differences in eConsults use given their potential benefits, especially since patients served by CHCs face barriers to directly accessing specialty care.
Previous research found that cost and lack of resources/infrastructure are barriers to clinics’ use of eConsults 17 and that increased workload, inadequate technology, and inadequate reimbursement are barriers to providers requesting eConsults.17,18 These barriers may underlie our findings that a small percentage of rural clinics requested eConsults. This finding is particularly concerning given that rural patients face increasing challenges accessing specialty care. These clinics have less access to virtual technologies, supported by our finding that telehealth use was lower in clinics not using eConsults and smaller clinics, pointing to the need to provide support for all forms of digital health care in these settings.
These barriers may also underlie our finding that even among providers requesting eConsults, most requested nine or fewer. As providers face increasing workloads, 19 supporting eConsult adoption may require finding ways to reduce administrative burdens to their use. Despite known barriers to eConsult requests, primary care providers report high satisfaction with eConsults because they can continue to manage patients who may have otherwise required a referral to a specialist. 20 It is possible that low eConsult use among some providers reflects gained knowledge and skills from even a few eConsults.12,20,21
Results also found a lower rate of eConsults among privately insured patients. This could suggest these patients are able to see a specialist directly. While we found higher rates of eConsult requests versus none among patients who are Medicaid insured or uninsured, these differences were relatively small. It is possible that while specialty care access is less available to Medicaid and uninsured patients, these patients are also more medially complex and thus more likely to require face-to-face consultation.22,23
Of note, while the rate of eConsult requests in all clinics was 63%, we found that just over two-thirds of urban clinics requested eConsults, while about half of both large and small/isolated rural clinics requested eConsults. Strategies to help overcome initial access barriers to eConsults in rural clinics could help bring needed specialty care recommendations to rural patients.
Limitations
This study has some limitations. eConsults resulting from informal provider-to-provider communications or those documented in chart notes only were not included in this study. However, by using a combination of billing codes, internal integrated eConsult platform utilization codes, and encounter data, we believe the majority of eConsults were captured. Future research should consider conducting chart reviews to better identify and understand the use of eConsults in primary care settings. In addition, future research should explore challenges and opportunities for use of eConsults in CHCs.
Conclusions
Even though eConsults are a promising tool in managing the health of medically complex patients, especially for those who may not otherwise easily access specialty care, their use remains low and highly variable in CHCs. A better understanding of strategies to increase eConsult requests among CHC providers and clinics, especially those in rural areas, could improve health for CHC patients.
Footnotes
Acknowledgments
The research reported in this work was powered by PCORnet®. PCORnet has been developed with funding from the Patient-Centered Outcomes Research Institute® (PCORI®) and conducted with the ADVANCE CRN. ADVANCE is a Clinical Research Network in PCORnet® led by OCHIN in partnership with Health Choice Network, Fenway Health, University of Washington, and Oregon Health & Science University. ADVANCE’s participation in PCORnet® is funded through PCORI Award RI-OCHIN-01-MC.
Funding Information
This work is supported by a grant from the Agency on Healthcare Research and Quality (K01HS028732).
Disclosure Statement
No competing financial interests exist.