
Abstract
Background:
Cardiovascular diseases remain a leading cause of global morbidity and mortality. Cardiac rehabilitation (CR), particularly cardiac physiotherapy, is crucial for secondary prevention; yet access is suboptimal, especially for patients in rural and underserved populations due to logistical and socioeconomic barriers. Telehealth offers a promising solution to address these disparities.
Objective:
This systematic review aimed to synthesize evidence on the effectiveness, feasibility, and acceptability of telehealth-delivered cardiac physiotherapy interventions in rural and underserved populations and identify the associated barriers and facilitators.
Methods:
A comprehensive search was conducted across multiple databases. Studies investigating telehealth-delivered cardiac physiotherapy in rural/underserved populations were included. Due to heterogeneity in study designs, interventions, and outcomes, a narrative synthesis was performed. Qualitative and quantitative data were extracted on effectiveness, feasibility, acceptability, barriers, and facilitators.
Results:
Nine studies were included, employing diverse designs (randomized controlled trials, multimethod, feasibility, qualitative, codesign, and mixed methods). Telehealth-delivered cardiac physiotherapy demonstrated effectiveness in improving exercise capacity, cardiac risk profiles, weight management, and quality of life. It also enhanced CR attendance and completion rates. High feasibility and acceptability were reported, with patients valuing convenience and home access. Key facilitators included personalized support, staff adaptability, and codesign approaches. Persistent barriers included digital literacy, technological infrastructure limitations, socioeconomic factors, staffing issues, and potential patient isolation.
Conclusion:
Telehealth-delivered cardiac physiotherapy holds significant promise for expanding access and improving outcomes for rural and underserved populations. While effective and acceptable, successful implementation requires addressing digital, technological, and socioeconomic barriers. Leveraging identified facilitators and designing patient-centered interventions are crucial for equitable cardiovascular care.
Keywords
Introduction
Cardiovascular diseases (CVDs) remain the predominant cause of global mortality and a substantial contributor to disability-adjusted life years worldwide, with an escalating burden in low-resource and geographically isolated settings. 1 Cardiac rehabilitation (CR), a multidimensional intervention encompassing structured exercise, education, and behavioral1 support, is a cornerstone in the secondary prevention of CVDs. Evidence has consistently demonstrated its effectiveness in improving functional capacity, mitigating modifiable cardiovascular risk factors, and reducing hospital readmissions and mortality.2,3 However, despite its well-established benefits, participation in conventional CR programs remains critically suboptimal, particularly among patients in rural and underserved regions, where logistical, infrastructural, and socioeconomic barriers persist.4,5
To address these persistent inequities, telehealth-based cardiac physiotherapy, or telerehabilitation, has emerged as a promising alternative model of care. Defined as the remote delivery of rehabilitation services using digital technologies such as phone consultations, mobile applications, web-based interfaces, and wearable devices, telerehabilitation enables care continuity while circumventing geographic and mobility-related constraints. 6 By leveraging remote monitoring, virtual coaching, and digital education platforms, this model has the potential to increase patient engagement, enhance adherence, and promote autonomy, all of which are vital for long-term health behavior change and cardiovascular risk reduction. 7
Preliminary evidence suggests that telerehabilitation can deliver outcomes comparable with traditional CR programs in terms of physical activity, weight management, quality of life (QoL), and exercise adherence, particularly in rural populations.8,9 Nonetheless, the variability in implementation modalities, population characteristics, and contextual barriers, such as digital literacy, infrastructure limitations, and socioeconomic disparities, necessitates a focused and structured synthesis of current evidence.10,11 Importantly, identifying key facilitators and barriers to telerehabilitation adoption can inform scalable, context-specific interventions tailored to underserved settings.
This systematic review aims to comprehensively evaluate and synthesize the current evidence on the effectiveness, feasibility, and acceptability of telehealth-delivered cardiac physiotherapy interventions, specifically within rural and underserved populations. The review assesses a range of outcomes including exercise capacity, cardiovascular risk factor control, adherence rates, patient satisfaction, and program completion. Moreover, it explores implementation-related challenges and enablers that influence the success of telerehabilitation in these contexts. By mapping the facilitators and barriers identified across diverse study designs, including randomized controlled trials (RCTs), qualitative inquiries, and implementation studies, this review seeks to provide actionable insights for health systems, clinicians, and policymakers striving to expand equitable access to CR through telehealth innovations.
Methods
This systematic review was registered in the International Prospective Register of Systematic Reviews ([PROSPERO]; Registration ID: CRD420251041452) and follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines.
ELIGIBILITY CRITERIA
Eligible studies included adult participants (≥18 years) diagnosed with CVD, residing in rural or medically underserved areas, and receiving physiotherapy as part of CR through telehealth modalities.
The intervention of interest was telehealth-delivered cardiac physiotherapy. This included programs delivered through videoconferencing, web-based platforms, mobile applications, and telephone- or wearable-supported monitoring systems. Acceptable comparators were standard in-person CR, usual care, or no intervention.
Outcomes
Primary outcomes included facilitators/barriers to CR; feasibility and acceptability of telerehabilitation; exercise capacity (6-minute walk test, VO2 max, etc.); QoL, assessed using validated instruments (SF-36, EQ-5D, etc.); cardiovascular risk markers (blood pressure, lipid profile, body weight, etc.); or hospital readmission rates. Secondary outcomes included program adherence and retention, patient satisfaction, or indicators of access and equity.
Study types
Eligible designs were RCTs, controlled clinical trials, cohort studies, quasi-experimental studies, feasibility studies, and mixed-method studies. Qualitative studies were included to capture patient and provider experiences related to facilitators and barriers.
EXCLUSION CRITERIA
Studies were excluded if they only evaluated in-person CR without a telehealth component, included populations not clearly described as rural or underserved, or were non-peer-reviewed literature (e.g., conference abstracts, protocols, or theses).
SEARCH STRATEGY
A comprehensive literature search was conducted across five databases: MEDLINE, AMED, SPORTDiscus, CINAHL, and PEDro. Searches were limited to peer-reviewed articles published in English from January 1, 1970 to May 1, 2025. Search terms combined with keywords are included in Table 1.
Keywords Used While Conducting the Search
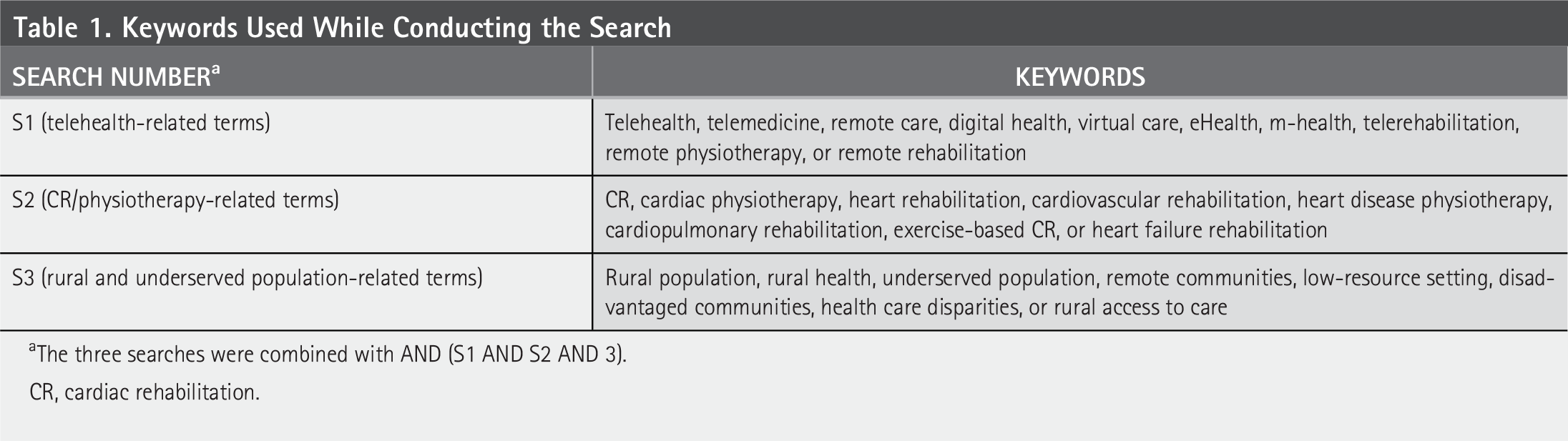
The three searches were combined with AND (S1 AND S2 AND 3).
CR, cardiac rehabilitation.
STUDY SELECTION
Search results were imported into EndNote X20, and duplicates were removed. Two independent reviewers (A.A. and M.Z.D.) screened the titles and abstracts against the inclusion criteria. Full texts of potentially eligible studies were retrieved and evaluated in duplicate. Discrepancies were resolved through discussion or consultation with a third reviewer, if necessary.
DATA EXTRACTION
A standardized data extraction form was used. The following information was collected: Author(s) and year of publication; study design and sample size, population characteristics, telehealth modality, and comparator (if applicable); outcomes measured; key findings, reported barriers, and facilitators. Data were extracted by the first reviewer and verified independently by the second reviewer. Disagreements were resolved through consensus.
RISK OF BIAS ASSESSMENT
The methodological quality of all included RCTs was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool. This tool evaluates five domains: bias arising from the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each domain was judged as having low risk, some concerns, or high risk of bias, leading to an overall risk of bias judgment for each study. For studies that were not RCTs (e.g., feasibility, implementation, or qualitative studies), the RoB 2 tool was adapted descriptively to assess potential sources of bias and inform the interpretation of findings. All assessments were independently conducted by two reviewers, and disagreements were resolved through discussion or consultation with a third reviewer.
Results
STUDY SELECTION AND CHARACTERISTICS
The comprehensive literature search yielded a total of 26 records. Following duplicate removal and title/abstract screening, full-text review was performed on potentially eligible articles. Ultimately, nine studies met the predefined eligibility criteria and were included in this systematic review. The PRISMA flowchart indicating the included and excluded trials is presented in Fig. 1. The data extracted from the trials that are included in this review are presented in Table 2.
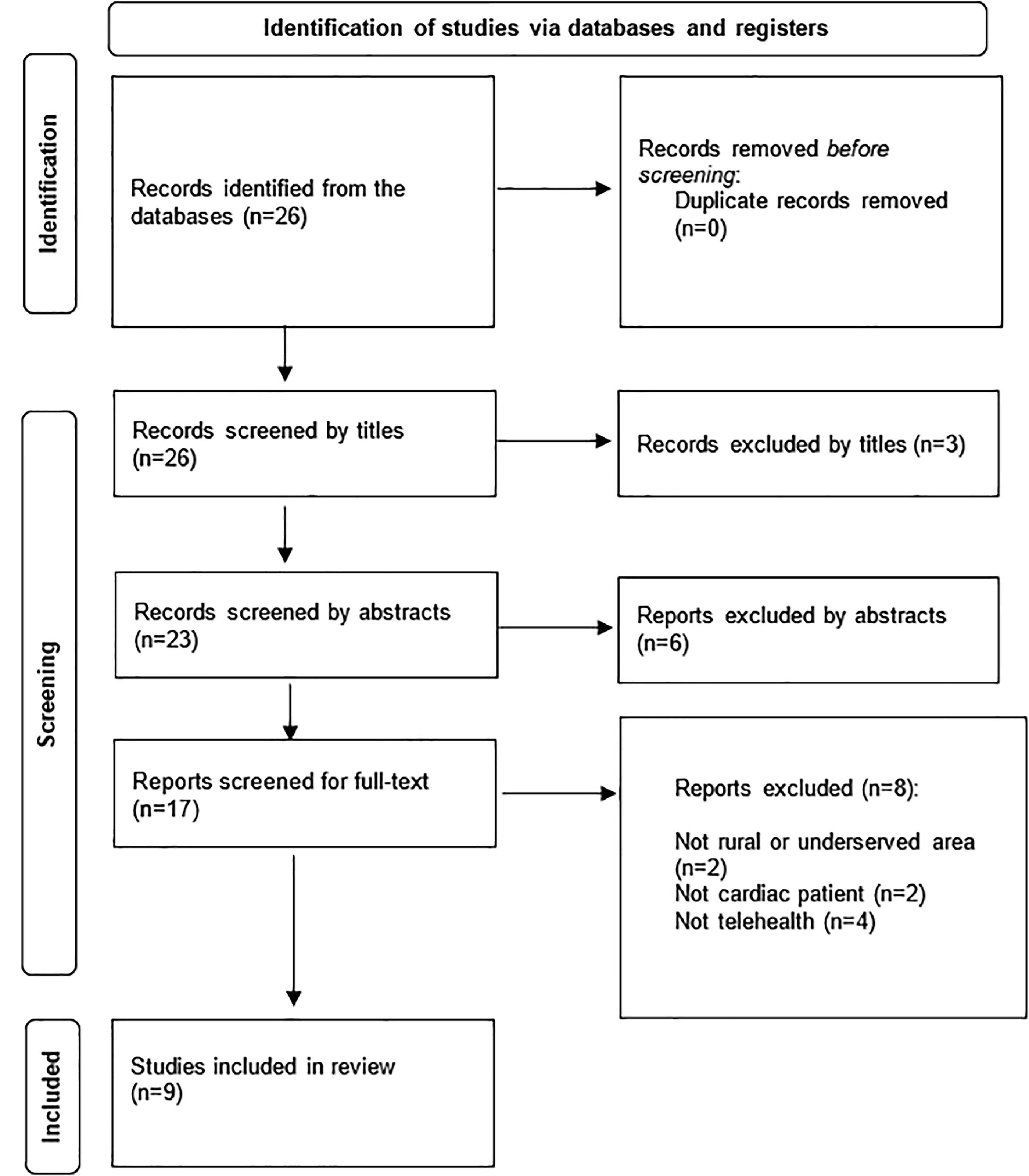
PRISMA flowchart of the systematic review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data Extraction: Telerehabilitation in Cardiac Rehabilitation for Rural Populations
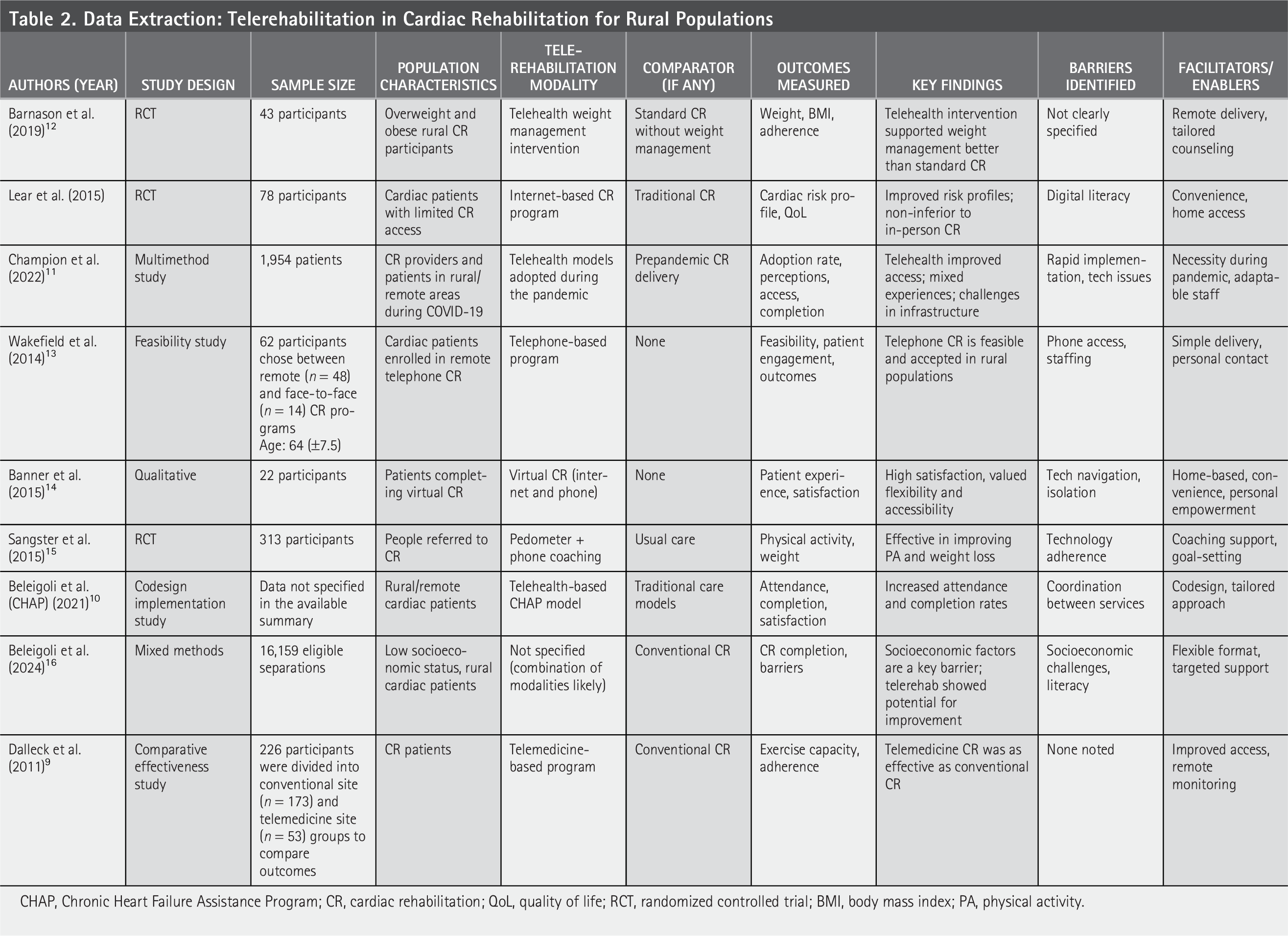
CHAP, Chronic Heart Failure Assistance Program; CR, cardiac rehabilitation; QoL, quality of life; RCT, randomized controlled trial; BMI, body mass index; PA, physical activity.
These studies investigated the effectiveness, feasibility, and acceptability of telehealth-delivered cardiac physiotherapy interventions, specifically within rural and underserved populations.
The included studies employed a variety of research designs, reflecting the diverse nature of inquiry in this field. These designs comprised RCTs,8,9,12,15 a multimethod study, 11 a feasibility study, 13 a qualitative study, 14 a codesign implementation study, 10 and a mixed-method study. 10 Sample sizes varied considerably across the studies included, ranging from qualitative inquiries with smaller participant numbers to larger comparative effectiveness studies. The populations studied predominantly included adult cardiac patients, with some studies specifically targeting overweight and obese rural participants, 12 individuals with limited access to conventional CR, 8 or those in low-socioeconomic-status rural settings. 10
Telehealth modalities utilized across the interventions were diverse, encompassing telehealth weight management interventions, 12 internet-based CR programs, 8 telephone-based programs, 13 virtual CR delivered via internet and phone, 14 pedometer-plus-phone coaching, 15 telehealth-based Chronic Heart Failure Assistance Program (CHAP) models, 10 and telemedicine-based programs. 9 Comparators, where applicable, included standard in-person CR, usual care, or no specific intervention. Due to substantial heterogeneity in study designs, intervention types, population characteristics, and outcome measures, a statistical meta-analysis was not feasible. Therefore, a narrative synthesis of the findings is presented.
RISK-OF-BIAS ASSESSMENT
Using the RoB 2 tool, among the nine included studies, four were RCTs and demonstrated an overall low risk of bias across all five domains—the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported results. These studies were considered to provide high-quality evidence. The rest of the studies were nonrandomized or descriptive studies. For these, the RoB 2 tool was adapted where possible, and most showed concerns related to incomplete outcome reporting, lack of randomization, and potential measurement bias, leading to an overall high risk of bias. These limitations highlight the need for more rigorously designed trials evaluating telerehabilitation for cardiac patients in rural settings (see Table 3).
RoB 2 Results
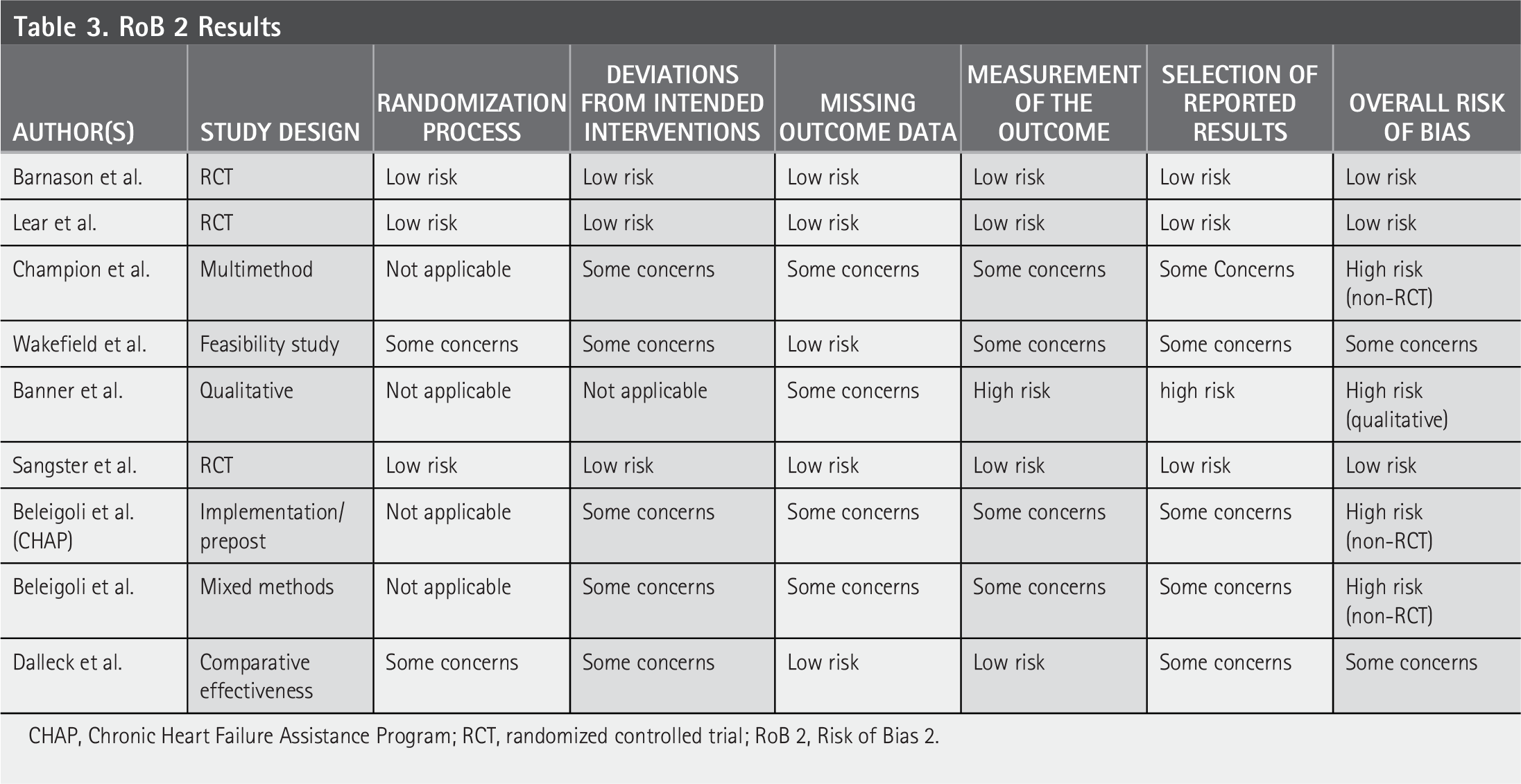
CHAP, Chronic Heart Failure Assistance Program; RCT, randomized controlled trial; RoB 2, Risk of Bias 2.
EFFECTIVENESS ON CLINICAL AND BEHAVIORAL OUTCOMES
Several studies reported positive impacts on clinical outcomes. An internet-based CR program demonstrated improvements in cardiac risk profiles and was found to be noninferior to traditional in-person CR. 8 Similarly, a telemedicine-based program was as effective as conventional CR in improving exercise capacity and adherence. 9 Besides, pedometer-plus-phone coaching intervention was effective in improving physical activity and weight loss. 15 A telehealth weight management intervention effectively supported weight management in overweight and obese rural CR participants, outperforming standard CR without such an intervention. 12 Moreover, improvements in QoL were observed with internet-based CR. 8 Furthermore, telehealth-based models, such as the CHAP model, were associated with increased attendance and completion rates in rural/remote cardiac patients. 10 In addition, telerehabilitation showed potential for improving CR completion, particularly in low-socioeconomic-status rural cardiac patients. 16
FEASIBILITY AND ACCEPTABILITY
Telephone-based CR programs were found to be feasible and well accepted within rural populations. 13 Patients completing virtual CR reported high satisfaction, valuing the flexibility and accessibility offered by the home-based approach. 14 Patient engagement was also a key outcome assessed in feasibility studies. 13
ACCESS AND IMPLEMENTATION
Telehealth models significantly improved access to CR, especially for rural and remote areas, a benefit particularly highlighted during the COVID-19 pandemic.9,11 The rapid adoption of telehealth during the pandemic led to mixed experiences, with challenges related to infrastructure but also demonstrating adaptable staff responses. 11 Codesign approaches in telehealth models were found to increase attendance and completion rates, suggesting that tailored approaches are beneficial for implementation. 10
IDENTIFIED BARRIERS
Several barriers were consistently identified across the studies, hindering the optimal implementation and uptake of telehealth-delivered cardiac physiotherapy. For instance, challenges related to patients’ digital literacy 8 and general technological issues, particularly during rapid implementation, were noted. 11 In addition, insufficient phone access and broader technological infrastructure challenges were reported.11,13 Furthermore, socioeconomic factors were identified as a key barrier to CR completion in rural patients. 16 Also, staffing limitations 13 and coordination issues between services 10 posed challenges. Moreover, potential feelings of isolation for patients in virtual CR 14 and technology-adherence issues 15 were also highlighted. One study did not clearly specify the barriers. 12
IDENTIFIED FACILITATORS/ENABLERS
Conversely, several factors were found to facilitate the successful adoption and effectiveness of telehealth interventions. For example, the convenience of home-based access and remote delivery was consistently reported as major enablers, enhancing patient engagement and satisfaction.8,9,12,14 Also, tailored counseling, 12 coaching support, 15 and simple delivery with personal contact 13 contributed to positive outcomes. Moreover, the necessity driven by the pandemic and the adaptability of staff were crucial in successful telehealth adoption. 11 In addition, virtual CR fostered a sense of personal empowerment among patients. 14
Discussion
This systematic review aimed to synthesize the current evidence regarding the effectiveness, feasibility, and acceptability of telehealth-delivered cardiac physiotherapy interventions in rural and underserved populations, as well as identify the associated barriers and facilitators. Our findings underscore the significant potential of telehealth to bridge critical gaps in CR access for these vulnerable groups, aligning with the growing global emphasis on equitable health care delivery. 1
The review’s findings on the effectiveness of telerehabilitation in improving clinical outcomes are largely consistent with the broader literature on CR, which consistently demonstrates its efficacy in enhancing functional capacity, mitigating cardiovascular risk factors, and reducing adverse events.2,3 Specifically, several studies included in this review reported positive impacts on exercise capacity, cardiac risk profiles, and weight management.8,9,12,15 The noninferiority of internet-based or telemedicine-based programs compared with traditional in-person CR in some outcomes8,9 is a particularly encouraging finding, suggesting that remote delivery can achieve comparable clinical benefits. Furthermore, improvements in patient-reported QoL 8 highlight the holistic benefits of these interventions. Importantly, increased attendance and completion rates observed with telehealth models10,16 directly address a well-documented challenge in conventional CR programs, where participation remains suboptimal, especially in rural settings due to logistical and socioeconomic barriers.4,5
Beyond clinical effectiveness, this review highlights the high feasibility and acceptability of telehealth-delivered cardiac physiotherapy among rural and underserved populations. Patients reported high satisfaction, valuing the flexibility and convenience of receiving care from home.8,9,14 This aligns with previous qualitative research indicating a strong user preference for alternative, home-based delivery models for CR. 7 The inherent ability of telehealth to circumvent geographic and mobility-related constraints is a key enabler for access, 6 and our findings confirm that telehealth models significantly improve access to CR, particularly in rural and remote areas, a benefit acutely recognized during the COVID-19 pandemic.9,11 The adaptability of health care staff and the necessity imposed by the pandemic were also critical facilitators in the rapid adoption and implementation of these models. 11 Moreover, the success of codesign approaches10,16 underscores the importance of involving the target population in the development of interventions to ensure cultural relevance and practical applicability, leading to better engagement and outcomes.
Despite these promising findings, the review also identified several persistent barriers to the widespread and equitable implementation of telehealth-delivered cardiac physiotherapy. Digital literacy and technological issues, including insufficient phone access and broader infrastructure challenges, emerged as significant impediments.8,11,13 These findings resonate with broader concerns about the “digital divide” and its impact on health care equity, particularly in low-resource and geographically isolated settings. 1 Socioeconomic factors were also highlighted as a key barrier to CR completion in rural patients, 16 indicating that technological solutions alone may not overcome deep-seated systemic inequities. Staffing limitations and coordination issues between services10,13 further complicate implementation, pointing to the need for robust organizational support and interprofessional collaboration. Furthermore, while telehealth offers convenience, some patients experienced feelings of isolation 14 or faced challenges with technology adherence, 15 suggesting that purely virtual models may not suit all individuals and a blended approach or enhanced virtual support might be necessary.
A strength of this systematic review is its comprehensive search strategy across multiple databases and the inclusion of diverse study designs, including RCTs, feasibility studies, and qualitative inquiries. This multifaceted approach allowed for a holistic understanding of not only the effectiveness but also the crucial contextual factors, such as feasibility, acceptability, barriers, and facilitators, which are vital for successful implementation in real-world settings. However, several limitations must be acknowledged. The significant heterogeneity in study designs, intervention modalities, population characteristics, and outcome measures precluded a meta-analysis, necessitating a narrative synthesis. This limits the ability to draw definitive quantitative conclusions and generalize findings across all contexts.
Future research should prioritize rigorously designed RCTs with standardized outcome measures to enable meta-analysis and stronger quantitative conclusions. Studies should explicitly report on the digital literacy levels and socioeconomic status of participants and explore how these factors mediate intervention effectiveness. Research is also needed to develop and evaluate tailored interventions that address specific barriers identified in rural and underserved populations, such as providing digital literacy training or subsidized internet access. Longitudinal studies are crucial to assess the long-term sustainability of engagement and outcomes. Finally, qualitative research should continue to explore patient and provider experiences to refine telehealth models, particularly focusing on strategies to mitigate feelings of isolation and enhance technology adherence.
In conclusion, telehealth-delivered cardiac physiotherapy holds considerable promise for improving access to and participation in CR for rural and underserved populations. While demonstrating effectiveness and high acceptability, successful implementation hinges on addressing persistent barriers related to digital infrastructure, technological literacy, and socioeconomic disparities. By leveraging identified facilitators and designing context-specific, patient-centered interventions, telehealth can play a transformative role in advancing equitable cardiovascular care globally.
Authors’ Contributions
M.Z.D. and A.A. were responsible for the study’s conception and design. R.B. and S.A. extracted the data. M.Z.D., A.A., H.A.S., S.A., Y.A.M., and K.M.B.H. were responsible for data interpretation. All the authors have participated in the drafting, editing, and completion of the article. All the authors have read and agreed to the published version of the article.
Footnotes
Funding Information
No funding was received for this study.
Disclosure Statement
No competing financial interests exist.