
Abstract
Introduction:
Native Americans enlist in the military at the highest per capita rate among racial or ethnic groups. Approximately 49% of Native Veterans live in rural areas, facing multiple barriers to health care and a high prevalence of mental health concerns. Video telehealth can improve access to care, and Veterans Health Administration has developed a culturally centered telehealth model for native Veterans. Personalized Implementation of Virtual Treatments for Rural Native Veterans (RNVs), an approach emphasizing cultural safety, helped expand the impact of existing telehealth clinics.
Methods:
Recent efforts included a systematic program review and mixed-methods evaluation to identify logistical and administrative considerations for implementation and outreach.
Results:
Key lessons emphasize protected clinical time for specific regions, building sustained community partnerships, collaborating with leadership, and streamlining messaging to improve patient engagement.
Conclusions:
These practices expand care access and quality for RNVs, with potential application to other populations.
Introduction
Native Americans (defined by Veterans Health Administration [VHA] as American Indian, AK Native, and Native Hawaiian Veterans but used in this article to refer to those individuals in the lower 48 states) enlist in the military at the highest per capita of any racial or ethnic group.1–4 Nearly half (49%) of Native Veterans live in rural or highly rural areas, making them the most rural of any racial or ethnic Veteran group,1,5 and they experience the highest rates of posttraumatic stress disorder and other mental health (MH) concerns of any Veterans.2,3 Native Veterans also face multiple barriers to health care, including travel time and distance, family or work responsibilities, and stigma.5–8
Video telehealth (VTH) has emerged as one solution to improve access to care for Native Veterans, helping mitigate barriers to care and provider shortages in rural areas. Two decades of collaboration between VHA’s Office of Rural Health-Salt Lake City Rural Resource Center and the Centers for American Indian and Alaska Native Health led to the development of a culturally centered model of MH care that uses telehealth to expand care access while addressing the unique sociocultural, historical, and contextual factors of Native Veterans. 9 VHA has successfully operated telehealth clinics as one avenue to address barriers and improve access to MH care, resulting in numerous studies detailing strong practices and recommendations for effective engagement of Native Veterans.10–12
Recent implementation research has indicated benefits of integrating social determinants of health to address disparities in implementation across groups. 13 VHA has endeavored to establish partnerships with relevant shareholders and be responsive to Native Veteran feedback, consistent with community-engaged research principles and priorities. 14 Research specifically examining the implementation of virtual treatment with rural Native Veterans (RNVs) has highlighted important cultural considerations and strategies to optimize success. Recommendations have emphasized the value of local engagement with both Native Veterans and Native communities or tribes, as well as training for providers on overarching Native cultural values and local tribal communities. These early lessons informed the development of Personalized Implementation of Virtual Treatments for Rural Native Veterans (PIVOT-RNV), an implementation approach that expanded and formalized earlier efforts to leverage telehealth technology with Native Veterans. 15 Through PIVOT-RNV efforts, cultural safety emerged as a critical component for effective implementation with Native Veterans.
While there is a growing body of literature that addresses cultural considerations and adapted implementation approaches for working with RNVs, there remains little attention to or understanding of the logistical and administrative aspects of establishing and sustaining virtual MH clinics for RNVs. Despite the success of tailored and culturally centered approaches, notable access, bandwidth, and infrastructure challenges remain for engagement of RNVs. 16 Thus, nearly two decades of virtual MH clinics within VHA strongly indicate logistical and administrative components are critical for successful execution of Native Veteran-focused telehealth clinics, including integration of telehealth into regular clinical practice, retention of dedicated providers, and continuity of telehealth during staff turnover or vacancies.
Methods
The previously described telehealth clinics for Native Veterans have continued to operate and expand, with PIVOT-RNV used at two new VHA sites in fiscal year (FY) 2022 and two new sites in FY 2023. 15 Recent efforts involved a systematic program review and an iterative, mixed-methods evaluation process that included a qualitative feedback from local site partners and RNVs and quantitative data review of VTH utilization at PIVOT-RNV sites. Ongoing analysis and collaborative discussions with key personnel (i.e., project team members, local leadership, rural providers and staff, and community and tribal members) highlighted the importance of logistical and administrative considerations for supporting implementation and outreach efforts. These lessons learned were initially identified from efforts focused at one site, presented to partners for feedback, and refined/finalized in response to comments.
Results
VIDEO TELEHEALTH USE BY RURAL NATIVE VETERANS
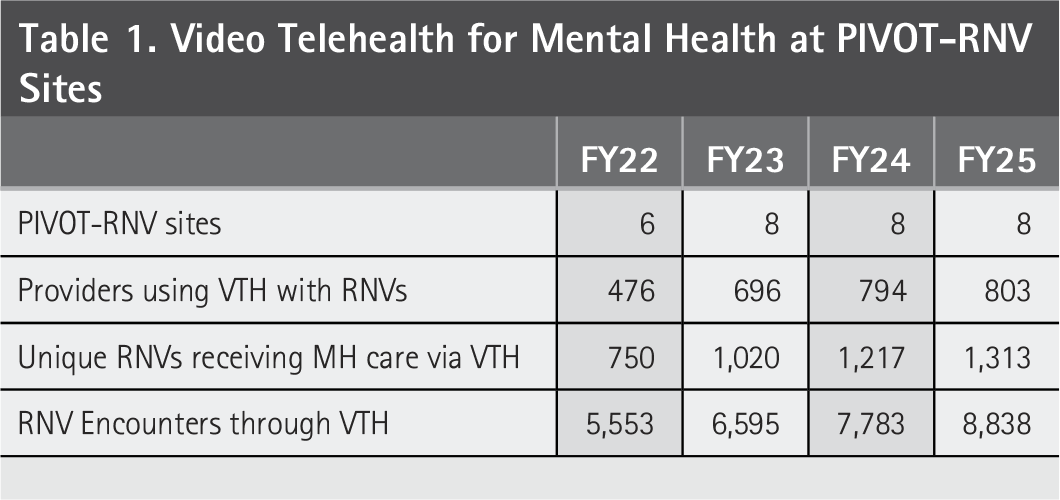
Throughout PIVOT-RNV implementation, VTH use by RNVs increased at all partner sites. From FY 2022 to FY 2025, all PIVOT-RNV sites increased each year on three key VTH metrics: number of MH providers using VTH with RNVs, number of unique RNVs using VTH for MH care, and number of VTH encounters with RNVs (Table 1). Please see our earlier publication for details about the previous success of PIVOT-RNV. 15
Video Telehealth for Mental Health at PIVOT-RNV Sites
LESSONS LEARNED—LOGISTICAL AND ADMINISTRATIVE CONSIDERATIONS
Set aside provider clinical time to treat specific tribes or regions to optimize flexibility and efficiency
RNVs are a high priority within VHA but may be present in limited numbers at individual clinics/sites, which makes it impractical and inefficient to have an RNV-dedicated provider at each facility or clinic. Protecting a small amount of clinical time enables more providers to be involved, increasing potential coverage. Virtual care maximizes efficiency and access for RNVs, as it entails seamless scheduling and allows coverage across a geographic region. The flexibility and reach of virtual care can facilitate MH services for an area serving multiple clinics/facilities or tribes while increasing provider productivity by balancing patient encounters across sites serving differing numbers of RNVs. Providers with an interest in RNVs are situated within existing clinics (e.g., general or specialty MH) and identified as a point of contact for RNVs among colleagues, while devoting most of their effort to the regular demands of their clinic. This approach is more localized than a regional hub model, which enables providers to gain expertise in and build relationships with the specific Native Veteran populations (i.e., tribes, geographic area) for whom they provide care.
Build ongoing community partnerships to extend outreach
Outreach is a critical component to support awareness of and engagement with MH care, particularly with underserved patient populations, but can be difficult to do well. Identification of tribal agencies, the Indian Health Service, or state employees already working with Native Veterans and wanting a consistent VHA point of contact can be one way to expedite introductions and align a focus on continuously building stable relationships with non-VHA entities, typically more effective than periodic/occasional outreach events and may be enhancing VHA’s credibility and reputation by demonstrating an ongoing commitment to RNVs. Partnering with Veteran Service Officers who are already engaged in outreach to tribal communities can be another way to increase awareness among RNVs who are not enrolled in VHA care.
Collaborate with leadership to align goals and garner support
Direct communication with local facility leadership is one way to improve understanding of the goals and benefits of telehealth clinics for RNVs, who have been identified as a special population for VHA. Discussing the clinical needs of RNVs, challenges in engaging RNVs in MH care, and ways telehealth addresses barriers to care can increase understanding and buy-in from leadership. As VHA struggles with workforce retention, highlighting the possible benefits for providers may also enhance leadership support. Participation in virtual MH clinics for RNVs may help provider recruitment and retention by improving provider job satisfaction and reducing burnout.
VHA has emphasized the importance of specifically engaging historically underserved Veteran groups at higher risk of MH concerns, including RNVs. High case complexity and a higher no-show rate may mean that providers in virtual MH clinics for RNVs with protected time have productivity that is slightly below usual VHA targets/metrics. Furthermore, it might be useful to include administrative time into provider labor mapping to address the additional time needed for clinic building and coordination with tribal agencies. Direct conversations with local leadership throughout the process can help manage expectations and ensure questions or concerns are readily addressed.
Streamline messaging to emphasize addressing historical inequities and health access barriers
Despite significant financial concerns and an emphasis on productivity metrics, VHA has an established history of creating specialty care clinics to meet the needs of underserved Veterans or populations with unique care needs that can also be applied to RNV clinics. Specialty MH care clinics that serve a specific group (e.g., geriatric clinic, women Veterans’ clinic) have a robust history within VHA and recognize the unique needs of some Veteran populations. Using existing specialty clinics as a model for improving access for RNVs highlights components for success. Specialized training (i.e., cultural safety, Native culture) for providers in virtual MH clinics for RNVs can improve competence and confidence working with RNVs. Bidirectional collaboration with those involved in supporting benefits (e.g., enrollment specialists, outreach managers, tribal Veteran Service Officers), referring Veterans to apply for benefits, and accepting health care referrals can optimize RNVs’ awareness and use of VHA services. Building trust with tribal communities and Native Veterans can be a reparative experience and help identify providers as trusted contacts at VHA. By investing in those relationships, providers in RNV clinics can help improve the perception of VHA among Native Veterans and act as a pathway for RNVs to engage in other VHA care or resources.
Conclusions
These key lessons learned highlight strong practices for improving access and quality of care for RNVs by going beyond implementation strategies to emphasize critical logistical and administrative considerations. Yearly increases in the number of providers and RNVs using VTH suggest that targeted implementation efforts can lead to success. Focusing on identified providers who are integrated into clinical teams/clinics and have some protected time for RNV care, rather than providers solely dedicated and in silos, is an effective model of care. This model prioritizes longevity, sustainment, and provider satisfaction by offering multiple providers the opportunity to work with a patient population of interest while benefiting from being part of a regular clinical team and minimizing individual impact on productivity metrics.
The lessons learned outlined here have relevance for and may be broadly applicable to general rural patient populations, though they were identified while implementing virtual MH clinics for RNVs. Overarching similarities in rural culture or values and insular communities that may view VHA or other health systems as outsiders mean that MH providers with interest in or knowledge/expertise for working with rural patients may improve patient engagement.
Similarly, these lessons learned may be applicable to other underserved populations. When working to establish or maintain clinics aimed at expanding health care, these lessons help to clearly delineate ways to garner and sustain leadership support or provider engagement. By offering practical considerations and describing the reasoning or value for each, we hope these lessons might serve as a guide or model for using virtual care to engage other populations, ultimately improving access to much-needed care.
Authors’ Contributions
J.S. and S.D.—Conceptualization; data curation—all authors; Formal analysis—all authors; J.S. and J.L.—Funding acquisition; Investigation—all authors; J.S. and J.L.—Methodology; J.S. and J.L.—Project administration; J.S. and J.L.—Resources; J.S.—Software; J.S. and J.L.—Supervision; Validation—all authors; J.S. and S.D.—Visualization; S.D. and G.H.—Writing—original draft; and Writing—review and editing—all authors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was funded by the Department of Veterans Affairs, Veterans Health Administration, Office of Rural Health, NOMAD #PRFY—10197. The contents do not represent the views of the Department of Veterans Affairs or the United States government. This work is partly the result of the use of resources and facilities at the Houston VA Center for Innovations in Quality, Effectiveness and Safety (CIN13-413) and the South Central Mental Illness Research, Education and Clinical Center. The contents are those of the authors and not necessarily those of the Department of Veterans Affairs, the U.S. Government or Baylor College of Medicine.