
Abstract
Objective:
To evaluate how patient characteristics are associated with telemedicine visit modality (video, phone, or converted from video to phone) and patient satisfaction, to better understand the digital divide in telemedicine.
Methods:
A retrospective cohort study conducted at a tertiary care center during the early phase of the COVID-19 pandemic (March–October 2020). Adult patients (≥18 years) who completed a telemedicine satisfaction survey following a visit during the study period were included. Visit modality was classified as video, phone, or converted (scheduled as video but completed as phone). Sociodemographic characteristics and broadband access data (by ZIP code and county) were linked to patient records. Multivariable logistic regression was used to identify predictors of visit conversion and satisfaction.
Results:
Of 30,578 patients surveyed, 17,859 (58%) responded. The median age was 59 years; 63% were female, and 74% were White. Visit modalities included video (43%), phone (39%), and converted (18%). Conversion from video to phone was significantly associated with older age, Medicare insurance, lower income, and reduced broadband access. Patient satisfaction was highest for video visits, followed by phone, and lowest for converted visits (p < 0.0001). Satisfaction declined with increasing age for phone and converted visits, but not for video visits. A previsit phone call was consistently associated with higher satisfaction across all modalities.
Conclusions:
Conversion from video to phone visits is a marker of digital access barriers and is associated with reduced patient satisfaction. Interventions such as previsit support calls should be used to improve patient experiences and help mitigate disparities in telemedicine access and outcomes. Inclusion of phone visits as a form of telemedicine recognized and reimbursed by insurance companies will allow for our most vulnerable patients to have equitable access to the health care system.
Introduction
The COVID-19 pandemic catalyzed an unprecedented transformation in health care delivery, with telemedicine rapidly evolving from a niche service to a central modality for outpatient care across the United States (U.S.) and globally. However, despite telemedicine’s rapid implementation, with some health systems reporting over 80% of outpatient encounters to be conducted remotely during the early pandemic period, 1 very little work has sought to examine its effectiveness and associated drivers. With telemedicine reimbursement continuing to require emergency extensions and audio-only reimbursement being limited to mental health services, 2 it is important to better understand the implications of limiting a crucial modality of health care engagement. Telemedicine’s rapid implementation was a Herculean effort that successfully increased health care access and efficiency, but intentional refinement and policy-level changes will exacerbate preexisting disparities in health care utilization. 3
Despite the rapid adoption of telemedicine, research on its effectiveness, patient satisfaction, and the factors driving its use remains limited and sometimes conflicting. Patient satisfaction with the provider encounter is considered critical for the telemedicine success, 4 which can influence the extent to which telemedicine services are adopted. 5 Satisfaction has additionally been found to affect medical outcomes and patient participation in continuing care.6,7 Systematic reviews and large cohort studies have consistently shown high levels of patient satisfaction across medical specialties, though satisfaction is not uniform and is influenced by both the modality and sociodemographic factors. Video visits are generally associated with higher satisfaction and perceived quality, 8 but access to video-based telemedicine is not equitably distributed. Patients who are older, from lower-income households, of racial or ethnic minority status, have limited English proficiency, or are insured by Medicaid or Medicare are less likely to complete video visits and more likely to rely on audio-only encounters (i.e., phone calls).3,9 These disparities are often attributed to the “digital divide,” a multifactorial phenomenon encompassing differences in access to broadband internet, digital devices, and digital literacy.10–12
The digital divide is a critical determinant of telemedicine access and satisfaction. High-speed internet and access to appropriate technology are prerequisites for video-based telemedicine, yet over a quarter of the U.S. population lacks broadband at home, with the greatest deficits among those with annual incomes below $30,000. 10 Studies have shown that broadband availability is strongly associated with both individual and neighborhood-level telemedicine use and that lack of internet access remains a significant barrier, particularly for rural, low-income, and minority populations. 12 Older patients face hurdles as they encounter more technological barriers that make telemedicine engagement difficult, as well as mobility impairments and chronic ailments that make leaving the house difficult for in-person visits.9,13 Furthermore, language barriers, lower educational attainment, and limited digital literacy further restrict the ability of vulnerable groups to engage with telemedicine platforms, compounding disparities in care. 14 Addressing disparities in telemedicine access and satisfaction is essential to ensure that telemedicine fulfills its promise of expanding equitable health care access rather than reinforcing existing inequities.
Current Centers for Medicare and Medicaid Services (CMS) reimbursements are extended a few months at a time without certainty on future extension. 1 When CMS extensions cease, it can be expected for only audio-visual telemedicine visits to be reimbursed, excluding the audio-only visits that are often used by historically vulnerable populations. Additionally, telemedicine would be limited to rural area use only, which may exacerbate preexisting disparities in access without infrastructure to integrate rural patients into a digital health care system. Understanding patterns of utilization and satisfaction among patients can help us better understand how policy changes can maximize the benefit of telemedicine among populations who need it the most.
The aim of this study is to characterize patient satisfaction with telemedicine and to examine the impact of the digital divide on telemedicine modality use and satisfaction in a large tertiary care hospital during the early COVID-19 pandemic when reimbursement was least restrictive on telemedicine utilization. Elucidating the interplay between sociodemographic factors, digital access, and patient experience can inform strategies for promoting equitable telemedicine adoption and optimizing patient-centered care in the evolving health care landscape.
Methods
This study was conducted at a single tertiary care center in the Southeast. All ambulatory patients aged 18 years or older who were seen during the study period (March–October 2020) by telemedicine were included. This study period was selected to focus on utilization patterns during the height of pandemic-related waivers, allowing for a better understanding of patient use and satisfaction that may not be generalizable to current, postemergency conditions that are limited by insurance reimbursement. Prior to the telemedicine encounter, each patient was called by the clinic staff for medication reconciliation and asked if help was needed with troubleshooting video technology. This is described in the study as a “previsit phone call.” All patients included in this study received this phone call.
Following the visit, each patient was given a survey of their telemedicine experience, independent of modality. The survey included patient satisfaction as measured through a single-item satisfaction measure (0 = “very dissatisfied,” 1 = “dissatisfied,” 2 = “satisfied,” 3 = “very satisfied”). A similar question measured the effectiveness of the previsit phone call (0 = “not at all helpful,” 1 = “not helpful,” 2 = “helpful,” 3 = “very helpful”). The electronic medical record was used to determine the type of interaction and categorized into three groups: real-time, face-to-face interaction between patient and provider using audio-visual communication technology (“video”); real-time, audio-only interactions (“telephone” or “phone”); and real-time visits that started as video but had to be completed telephone (“conversion”). Other covariates measured included social determinants of health on individual (age, reported race, reported gender, insurance status, estimated income, and date of visit) and community (estimated internet accessibility) levels. Income and internet accessibility were estimated using ZIP and county of residence, respectively. While these data do not represent individual-level device access or literacy, they serve as a proxy for structural measures of the patient’s digital access. This retrospective observational cohort study was approved by the University of Alabama at Birmingham Institutional Review Board under protocol number IRB-300005473. Informed consent was not needed, as this was a retrospective cohort study.
The primary outcome measured was conversion from a video to a phone visit. The secondary outcome measured was patient satisfaction. The three cohorts (video, phone, and conversion) were compared with unadjusted analysis. Continuous variables were characterized using means or medians and the range of values or 95% confidence intervals for medians for nonnormally distributed variables. The differences between groups of visit types were evaluated using the student t-test, chi-square, and ANOVA. Logistic regression analysis was used to determine the impact each measured covariates had on patients who experienced converted and video visits. The results of the logistic regression analyses were quantified and graphed using odds ratios with 95% confidence intervals.
Results
A total of 30,578 patients were surveyed between March 16, 2020, and October 3, 2020, with 17,859 (58%) included for answering the question “Overall, how satisfied or dissatisfied were you with your eMedicine experience?”. As shown in Table 1, the patients mostly identified as female (63%) and White (74%) and had a median age of 59 years. Most (50%) had commercial insurance. The median income of their ZIP was $58,000. On average, patients came from counties with broadband internet available to 91% of the population. Video visits were most common (43%), followed by phone (39%) and conversion (18%).
Overall Study Population
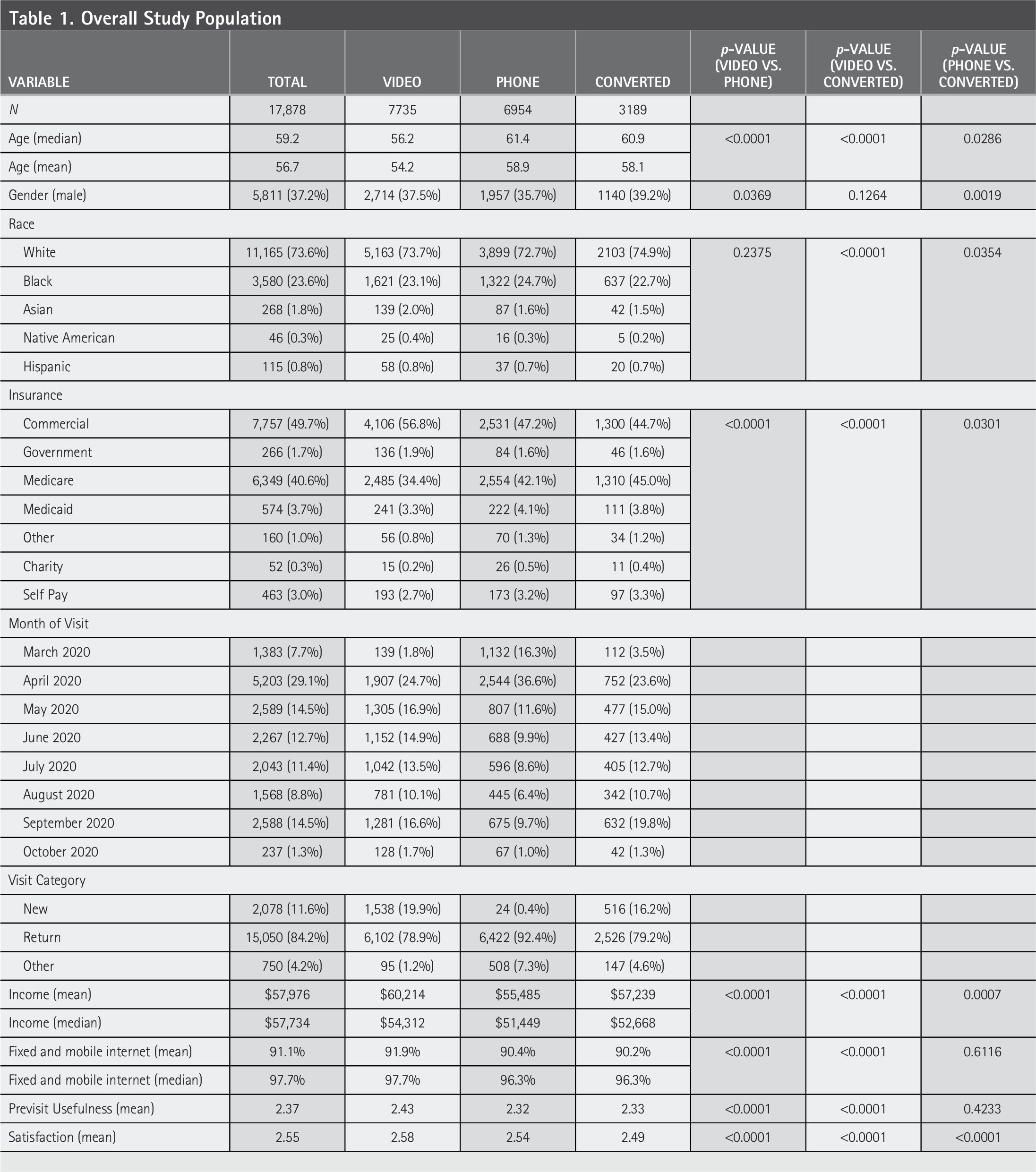
In unadjusted analysis, when compared to those who completed a video visit, patients who had a converted visit were more likely to be older (p < 0.0001), less likely to have commercial insurance (p < 0.0001), come from areas with lower median income (p < 0.0001), and have less access to broadband internet (p < 0.0001). Patients who had a completed video visit were less likely to identify as Black (p < 0.0001) and had greater satisfaction with their previsit phone call (p < 0.0001). In adjusted logistic multivariable analysis (Table 2), the predictors of conversion were increasing patient age and Medicare compared to private insurance. Higher estimated median household income and increased broadband internet availability were protective against conversion.
Multivariable Analysis of Conversion from Video to Phone Visit
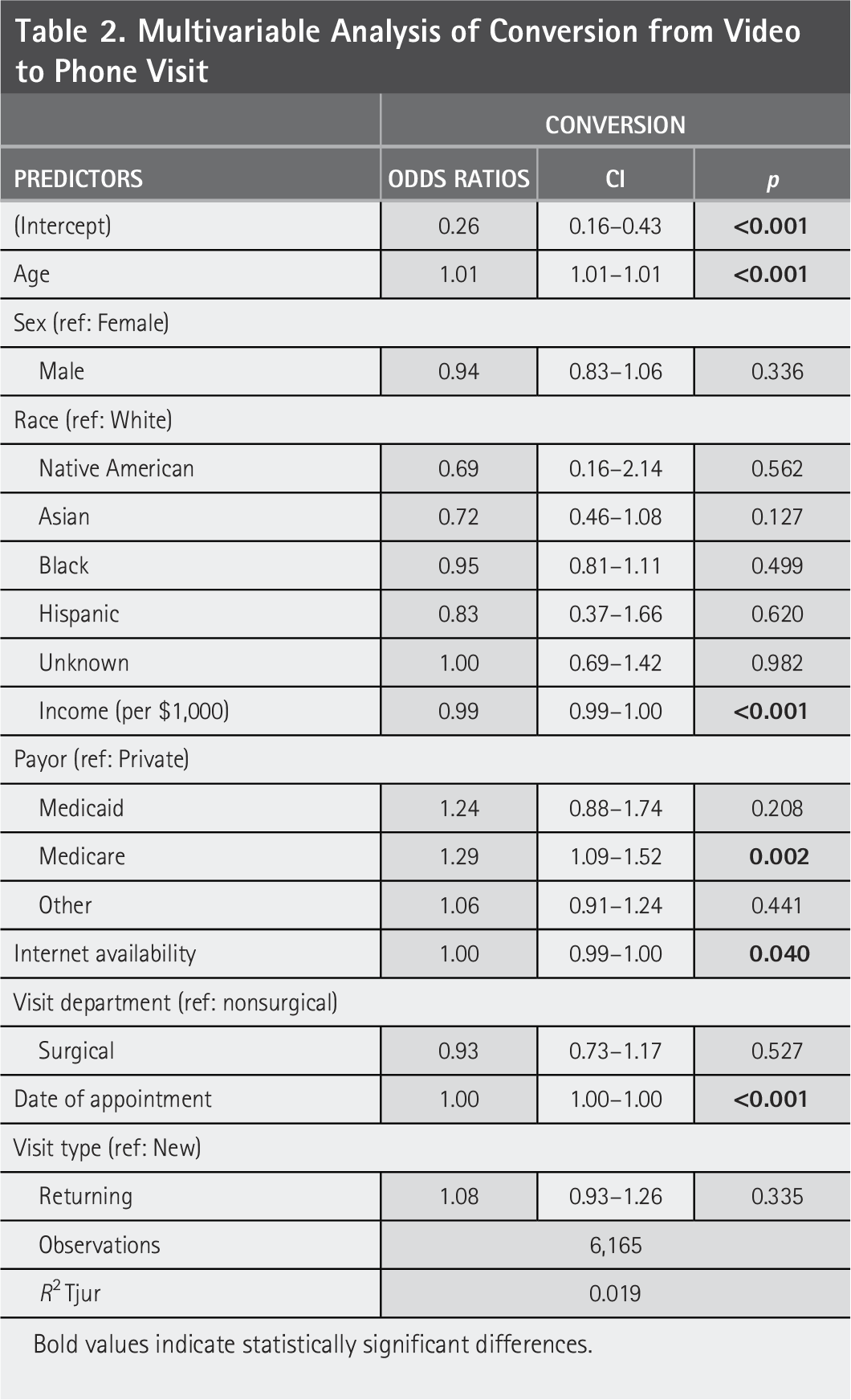
Bold values indicate statistically significant differences.
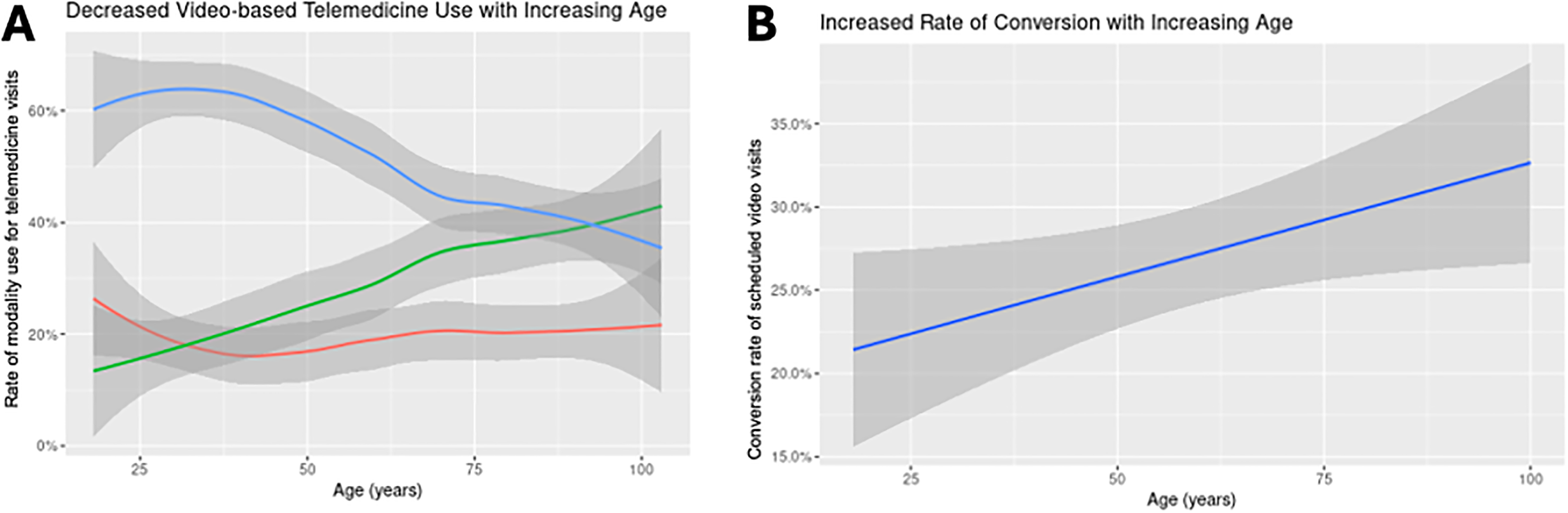
There was a significant decline in the proportion of patients who used video visits as patients aged (Fig. 1A). Many of these visits were replaced by phone visits. The proportion of converted visits remained constant with increasing patient age; however, a linear regression model shows an increase in conversion from video visits as a function of patient age (Fig. 1B). In logistic regression comparing video and converted visits, conversion was associated with increased age (odds ratio [OR]: 1.01, 95% confidence interval [CI]: 1.01–1.01) and Medicare compared to private insurance (OR: 1.3, 95% CI: 1.1, 1.5). Higher median household income of home ZIP (OR: 0.99, 95% CI: 0.99, 1.0) and increased internet availability (OR: 1, 95% CI: 0.99, 1.0) were protective against conversion.
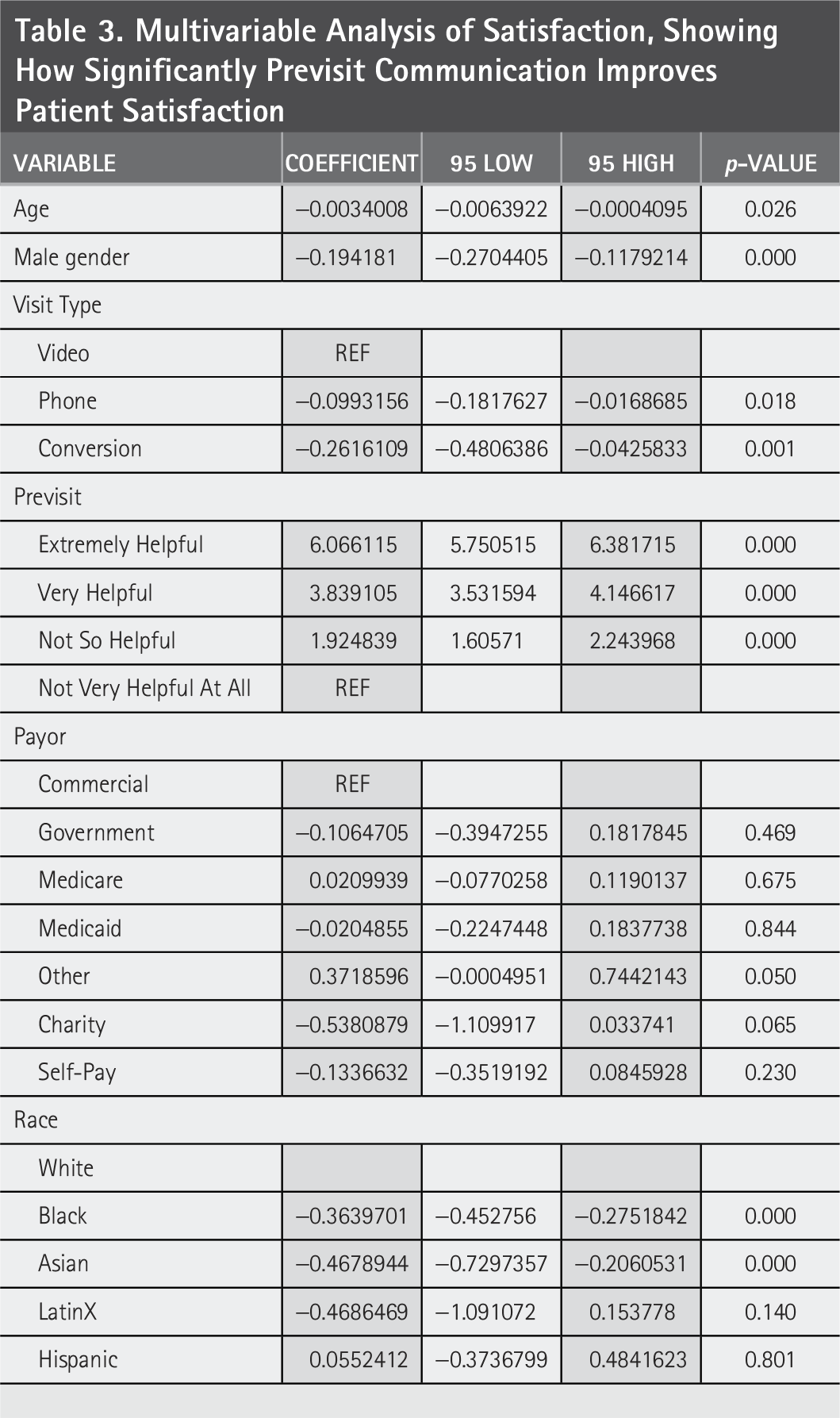
Video visits were associated with greater overall satisfaction than phone (p < 0.0001) and converted (p < 0.0001) visits. In multivariable analysis (Table 3), increasing patient age, male gender, and Black and Asian races were all predictive of decreased patient satisfaction with their visit. Video visits were still associated with better satisfaction than either of the other two modalities, but phone visits had more satisfaction than converted visits. Video visits had the same high level of satisfaction throughout all patient ages. However, satisfaction with phone and converted visits decreased with age, and phone visits outperformed converted visits throughout all ages (Fig. 2). Improved satisfaction of the previsit phone call was associated with higher satisfaction with the visit.
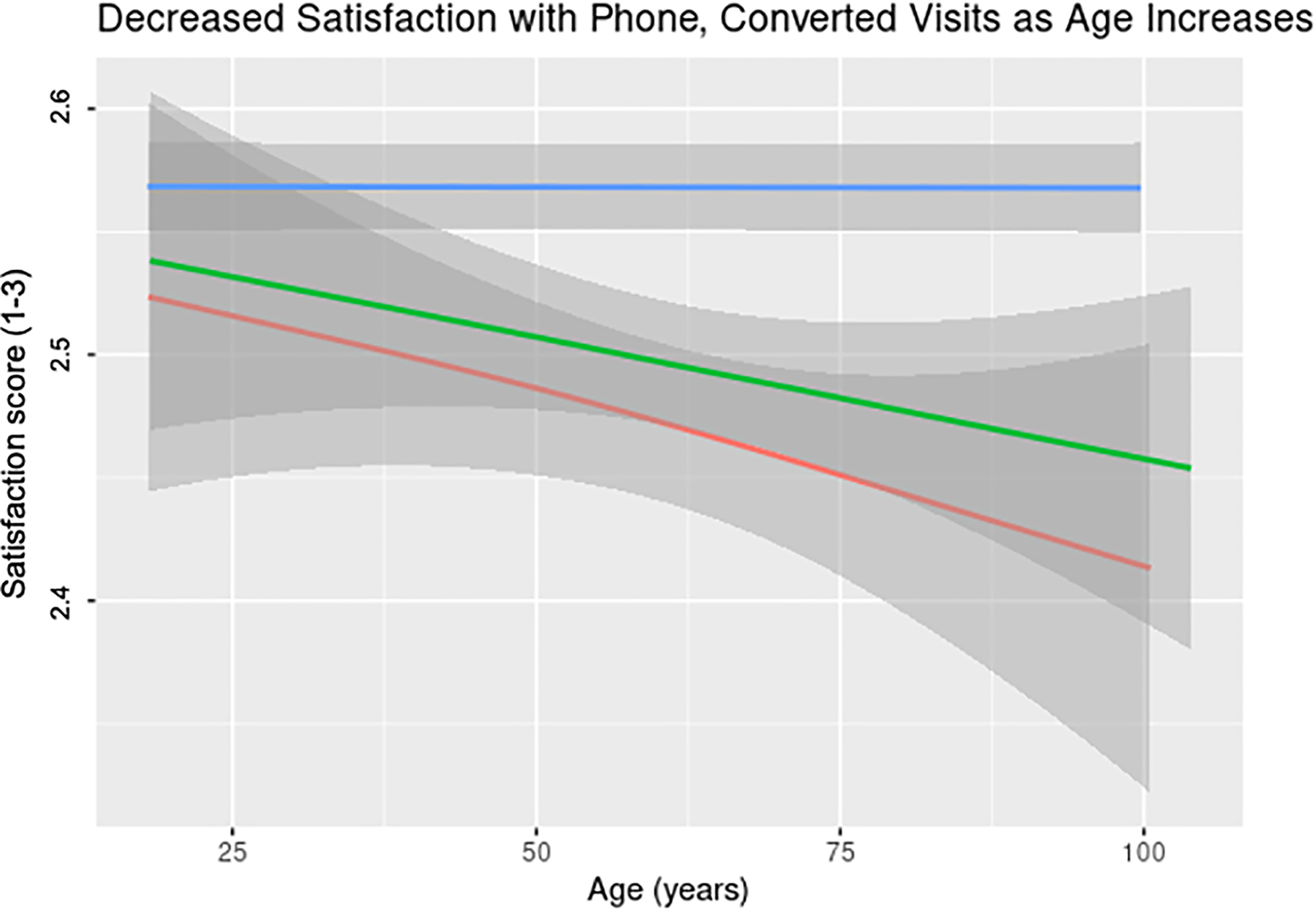
Satisfaction decreases with patient age.
Multivariable Analysis of Satisfaction, Showing How Significantly Previsit Communication Improves Patient Satisfaction
Discussion
Nearly one in five telemedicine visits in our cohort required conversion from video to phone, and these converted visits were associated with the lowest patient satisfaction, even lower than scheduled phone-only encounters. This finding suggests that successful video completion is not only a technical issue but a critical determinant of patient experience. Consistent with prior work, conversion was more common among older patients, those with public insurance, lower neighborhood income, and reduced broadband access—groups already known to face digital access disparities.4–6 Notably, this association persisted despite patients coming from counties with high overall broadband availability (91%), indicating that household-level factors such as device access or digital literacy likely contribute beyond infrastructure alone. 7
Our most novel finding is that converted visits result in lower satisfaction than both video and phone-only visits. This pattern is best explained by expectation violation and technology failure attribution. Patients scheduled for video visits likely anticipate a richer, more personal interaction; when technical failure forces conversion, dissatisfaction may arise from frustration, perceived system failure, or diminished trust. In contrast, patients scheduled for phone visits enter with aligned expectations, which may mitigate dissatisfaction despite the absence of video. Thus, dissatisfaction appears driven not solely by modality, but by disruption of the intended care experience. 8 These findings are particularly salient as health care systems shift toward remote care models, often driven by reimbursement structures that favor video over phone encounters, risking worse satisfaction without infrastructure to support successful video encounters. 13
While prior studies have validated the clinical effectiveness and acceptability of video-based telemedicine,3,9 few have examined how failed video attempts—those that are converted—impact patient perceptions. Satisfaction with video visits remained high across all ages, whereas satisfaction with phone and converted visits declined with increasing age, suggesting that older patients may experience greater frustration when video attempts fail. Importantly, higher-rated previsit phone calls were independently associated with improved satisfaction across all modalities, highlighting previsit communication as a modifiable intervention to improve patient experience and potentially reduce conversion. This suggests that effective previsit communication improves patient experience even when technical failure occurs, rather than simply serving as a proxy for successful video visit completion. Establishing infrastructure within health care systems for not only patient intake but also reassurance and outreach can significantly improve patients’ experience with video-based telemedicine and consequent retention within the health care system.
The implications for policy and practice are clear: equitable telemedicine access requires more than broadband expansion. Health care systems must consider patient-level interventions, such as digital literacy training, enhanced previsit support, and technological access to ensure that all patients can access and benefit from telemedicine visits. 15 Preservation of reimbursed audio-only options is essential to keep our most vulnerable populations within the health care system. 16 Clinicians and institutions must be aware that failed video connections are not merely logistical issues. They directly influence patient perceptions and satisfaction, potentially exacerbating health inequities. 17 As reimbursement structures increasingly favor video visits, failure to account for conversion risks may unintentionally worsen disparities and undermine patient trust in telemedicine.
In our analysis, insurance type and median income of patient home ZIP represent related but distinct dimensions of socioeconomic status and were modeled as separate covariates in our multivariable analyses. While these variables are correlated, they capture different mechanisms of disadvantage: insurance type reflects eligibility, coverage stability, and reimbursement structures, whereas ZIP code-level median household income reflects neighborhood-level socioeconomic context and access to resources such as broadband, a structural factor previously found to be correlated with telemedicine use. 12 In our adjusted models, both Medicare insurance (relative to commercial insurance) and lower median household income at the patient home ZIP were independently associated with increased likelihood of video-to-phone conversion, suggesting that their effects are at least partially additive rather than fully overlapping. Lack of commercial insurance does not simply serve as a proxy for income but may reflect age-related eligibility, fixed income, or disability status that independently affects telemedicine access and experience.
Limitations
This study has limitations. Data reflect the early COVID-19 period, when telemedicine utilization and reimbursement were at their peak, which may limit generalizability. However, this period offers a unique lens into telemedicine under maximal policy support. Broadband and income were measured at the neighborhood level and do not capture individual literacy or device access. Selection bias is possible given survey response rates, as evidenced by the predominantly White and female demographic imbalance. Lastly, satisfaction is not the same as use. Patients may report high satisfaction with telemedicine but still reject its use as a replacement for face-to-face consultations. Future studies will include comparison to in-person visits as well.
Ongoing qualitative work will further explore patient- and provider-reported barriers to successful video visits and perceptions of previsit support. Preliminary data parallel quantitative data, revealing that patients are often satisfied with audio-only visits, especially if they have a pre-established relationship with the surgeon. Technological burdens from either the patient or provider side affect the overall encounter, jeopardizing communication and therefore the surgeon-patient relationship. Understanding what patients and providers value in virtual visits, characterizing the value of video versus phone visits, and identifying ways to optimize virtual visits via both access and utilization will allow for improved determination of appropriate telemedicine use and therefore reimbursement by insurance companies and system-wide goals for utilization. Standardizing previsit communication based on patient preferences will likely include expectation-setting, reassurance, and clarity regarding visit logistics, allowing us to best support patients before and after virtual visits.
Conclusion
Telemedicine conversion from a video to phone visit is associated with patient level factors and leads to decreased satisfaction. This is particularly prevalent among patients who are older, publicly insured, from lower income areas, and from areas with reduced internet availability. Expanding accessibility or and assistance with video-based telemedicine for older patients can help bridge this digital divide and increase health care equity. Phone visits must be recognized and reimbursed by insurance companies as a valid form of telemedicine to allow for our most vulnerable patients to have equitable access to the health care system.
Authors’ Contributions
C.C.S.: Conceptualization; methodology; formal analysis; investigation; data curation; writing—original draft; visualization; M.C.M.: Methodology; formal analysis; validation; writing—review and editing; L.E.L.: Data curation; project administration; writing—review and editing; E.L.W.: Resources; supervision; writing—review and editing; D.I.C.: Conceptualization; supervision; funding acquisition; writing—review and editing; and S.R.: Conceptualization; supervision; funding acquisition; writing—review and editing. All authors have read and approved the final article and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgments
Presented at the 31st Annual Society of Black Academic Surgeons 2021 Meeting and the ACS Quality and Safety Meeting 2021. Data are available upon request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Health Services/Comparative Effectiveness Research Training Program supported by the Agency for Health care Research and Quality through T32 institutional National Research Service Awards (5T32HS013852-18) and the American College of Surgeons Resident Research Scholarship Award.