
Abstract
Introduction:
Provider-to-provider consultations may improve primary health care (PHC), but empirical data are limited. Hospitalizations for ambulatory care sensitive conditions (ACSC) indicate PHC quality. We aim to address the effects of synchronous telephone-based discussions on ACSC hospitalizations.
Methods:
We performed an ecological observational temporal series study based on secondary data. All municipalities of Rio Grande do Sul (Brazil’s southernmost state) were eligible; lack of data was the sole exclusion criterion. The main factor explored was the annual rate of consultations per 1,000 inhabitants from 2014 to 2019. Other factors considered included municipality typology (urban or nonurban), poverty, hospital bed rate, PHC coverage, and non-ACSC hospitalizations. The primary outcome was the rate of ACSC hospitalizations per 1,000 inhabitants from 2014 to 2019. Both comparisons between and within municipalities were assessed. The association between the exposure variables and the outcome was explored using a hierarchical multivariable model with a generalized estimating equations (GEE) analysis.
Results:
Out of 497 municipalities, one was excluded due to lack of data. Between 2014 and 2019, there was an increase in the usage of consultations and a reduction in ACSC hospitalizations. In the final model, time, poverty, municipality typology, hospital bed rate, non-ACSC hospitalization, and consultations were all associated with ACSC hospitalization. After adjusting for the possible confoundings, the GEE model prediction showed that a higher number of consultations between- and within-municipalities was associated with a lower rate of ACSC hospitalization.
Discussion:
The presented data suggest that increased consultation usage is associated with improved PHC performance.
Keywords
Introduction
The Brazilian public health care system (Sistema Único de Saúde [SUS]) is based on strong primary health care (PHC) through the Family Health Strategy.1–3 However, despite the reorganization and integration of health services, structural challenges and access bottlenecks are compounded by geographical regions’ vast territory, and economic and health care inequities. 4
Telemedicine has emerged as a promising approach to address some of these challenges. Evidence consistently demonstrates that telehealth interventions in PHC improve access, quality, efficiency, and care accountability while supporting the pursuit of universal health coverage.5–8 Telehealth encompasses multiple applications, including interactions between patients and health care professionals, peer-to-peer professional consultations, and managerial actions.6,7 Despite the diversity of functions, these telehealth activities contribute synergistically to strengthening health system performance. International evidence indicates that provider-to-provider consultations facilitate access to specialized knowledge, improve problem-solving capacity in PHC, and optimize referral pathways.8–10 In some cases, provider-to-provider consultations prevent the need for in-person specialized appointments.10,11
The Brazilian Ministry of Health created the National Telehealth Program in 2007 to foster telehealth programs. Initially, there were programs in nine states, with later nationwide expansion. They are mostly nested in public hospitals and/or universities. Among these programs, TelessaúdeRS is nested in the Federal University of Rio Grande do Sul (Brazil’s southernmost state). 12 One of the initiatives developed by TelessaúdeRS is a synchronous telephone provider-to-provider consultation service, available free of charge to physicians (and other professionals) working in PHC. Consultations provided by colleagues (family physicians and focal specialists) assist these professionals in resolving any clinical questions from any medical specialty in real time.12,13 Often, health units lack the resources to provide comprehensive patient care. These remote consultations help provide access to evidence-based information, discussions with focal specialists, and clinical peer advice for primary care physicians.
One way to assess PHC quality is the care provided to ambulatory care sensitive conditions (ACSC). Billings et al., developed this concept in the 1990s, based on avoidable deaths. ACSC is a list of situations or diseases in which primary care can reduce the risk of hospitalization if provided in a qualified, effective, and timely manner. 14 Thus, ACSC hospitalizations have been used to evaluate access and quality of care provided. 15 Also, strengthening PHC is directly related to reducing hospitalizations for various chronic conditions and ACSC. 15
Using mobile technologies to support health care professionals reduces the time between presentation and treatment and decreases referrals.16,17 However, research on the impact of telehealth on ACSC hospitalizations is limited.16–18 Observational survey data suggest improving communication between primary care physicians and specialists reduces hospitalization rates. 18 Communication might be achieved through telecommunication technology, allowing for better coordination of primary care and supporting the treatment of ACSC. As such, this study aimed to evaluate whether using a provider-to-provider synchronous consultation service through a toll-free telephone number impacts ACSC hospitalizations.
Methods
STUDY DESIGN, CONTEXT, AND REPORTING
This is a time series study using observational ecological data. The report follows the Strengthening the Reporting of Observational Studies in Epidemiology Statement. 19 We used data from Rio Grande do Sul, a southern state of Brazil comprising 497 municipalities. Data between 2014 and 2019 were used to avoid the impact of the Coronavirus pandemic influence on hospitalizations.
This research was evaluated by the ethics in research committee from Hospital de Clínicas de Porto Alegre and is approved under 62602522.9.0000.5327. Direct patient consent was exempted.
PARTICIPANTS
All municipalities from Rio Grande do Sul were eligible for the study. The sole exclusion criterion was the lack of data to explore the hypothesis.
VARIABLES
This study evaluates the rate of consultations per 1,000 inhabitants as the main exposure. Following the theoretical model described by Nedel et al., 20 additional independent covariates included municipality characteristics, sociodemographic factors, indicators of health service organization, and health system performance.
The information regarding consultation records is stored in a database from the university in which TelessaúdeRS is nested. Regarding the municipality typology (urban or nonurban), the 2017 data from the Brazilian Institute of Geography and Statistics classification was used (based on the 2010 national census). To include a socioeconomic factor, we assessed the proportion of persons living with less than $1 USD/day in 2010 (last data available) within each municipality, that is, extreme poverty, which is available at https://www.ipea.gov.br. Variables relevant to health service organization and health system performance were PHC coverage, public hospital beds per 1,000 inhabitants (excluding private hospital beds), and non-ACSC hospitalizations per 1,000 inhabitants. This information is available in the Ministry of Health databases in the primary care and hospital admissions information systems (https://sisab.saude.gov.br/ and http://sihd.datasus.gov.br, respectively).
OUTCOME
The rate of hospitalizations due to ACSC per 1,000 inhabitants by municipality between 2014 and 2019 was the outcome of interest. The Ministry of Health defines the Brazilian ASCS list. 21 The data was obtained from the hospital admissions information system. Data files were processed using R statistical software version 4.0.2, employing the csapAIH package. 22 The total number of hospitalizations, excluding births, and the total number of ACSCs were extracted. ASCS rates per 1,000 inhabitants and rates of “non-ACSC” hospitalizations were calculated. Estimates of the population size for each municipality are available annually, according to the Brazilian Institute of Geography and Statistics.
STATISTICAL ANALYSES AND SAMPLE SIZE
Data were processed using the Statistical Package for the Social Sciences, version 29, and grouped by municipality and year. Descriptive analysis presented medians and interquartile ranges (IQR) for skewed continuous variables, and proportions for categorical variables. As the variables did not follow a normal distribution, the differences in characteristics between groups were analyzed using the Mann–Whitney U and chi-square tests.
To assess the association between ACSC hospitalizations and the use of consultations of correlated repeated measures in municipalities of Rio Grande do Sul between 2014 and 2019, the Generalized Estimating Equation (GEE) model, with gamma distribution and exchangeable working correlation matrix, was employed.23–26 This approach was selected as this study dealt with time-dependent variables (both outcome and predictors). As the GEE predicts mean responses for the population, to reduce the possibility of collinearity and to include the effects of predictor variation within and between municipalities on the outcome, time-dependent covariates were centered on the mean of municipalities for each variable over the period and on the difference from the value of a specific year to the mean of each municipality.27,28 This allowed assessing the effects of “within-municipality” and “between-municipalities” changes in time-dependent predictors on ACSC hospitalizations. Despite these advantages, as a marginal model, GEE provides population-average estimates and does not allow inferences for the individual subjects (i.e., municipalities).26,27 Due to this limitation and to improve results visualization, the predicted relation of consultations and ACSC hospitalizations were presented as predicted responses considering the between- and within-municipality effects.
The selection of covariates for multivariable analysis was performed using the hierarchical method, including (a) sociodemographic information (poverty and municipality typology) at the distal level; (b) indicators of health service organization and health system performance (primary care coverage, SUS hospital bed rate per 1,000 inhabitants, and non-ACSC hospitalization rates per 1,000 inhabitants) in the intermediate level; and (c) consultation rate per 1,000 inhabitants in the proximal level. 29 All variables were tested for interaction with the study years. The final model included variables that achieved significance levels of 5% in the initial models.
The GEE model was constructed using R statistical software version 4.0.2, employing the geepack and emmeans packages.30,31 The modified Wald test evaluated associations between predictor variables and the outcome. Results are expressed as coefficients and confidence intervals. As this is an ecological study involving the evaluation of all municipalities in Rio Grande do Sul, no sampling calculations were conducted, and all available data were used.
Results
Rio Grande do Sul had 497 registered municipalities between 2014 and 2019. However, one municipality was funded in 2013 and lacked hospitalization, economic, and typology data, so it was excluded from the study. We compiled annual data from a final sample of 496 municipalities. Table 1 shows the overall characteristics of the set. The municipalities were predominantly nonurban, and there was an increase in PHC coverage, with the median increasing from 97.3% in 2014 (IQR = 71.9 − 100%) to 100% in 2019 (IQR = 83.9 − 100%). Overall, extreme poverty was infrequent in the included sample. On the other hand, there was a reduction in the rate of public hospital beds per 1,000 inhabitants; by 2019, most municipalities did not have SUS-accredited hospital beds registered.
Characteristics of the Included Municipalities. Data is Presented in Median and (Q1–Q3) Quartiles
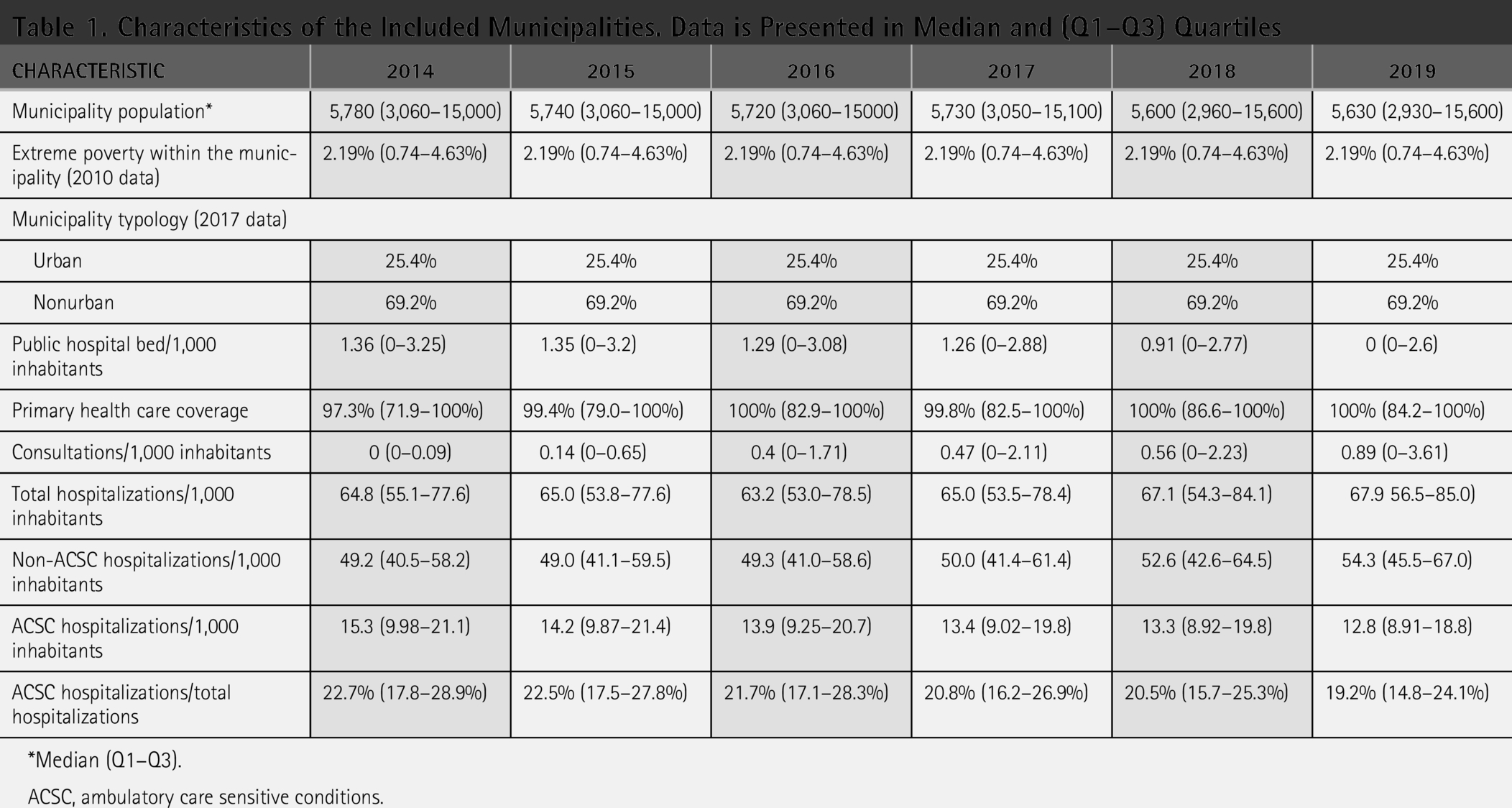
Median (Q1–Q3).
ACSC, ambulatory care sensitive conditions.
Between 2014 and 2019, 106,076 consultations were performed by physicians working in PHC in Rio Grande do Sul. Over the years, there has been an increase in municipalities’ usage of consultations: by 2014, 157 municipalities registered at least one consultation; this number rose to 371 in 2019. The consultation rate per 1,000 inhabitants was 0 (IQR = 0–0.1) in 2014 and increased to 0.89 (IQR = 0–3.63) in 2019. Of the 496 included municipalities, 414 recorded at least one consultation during the study period. The comparison between municipalities that performed or did not have consultations is shown in Table 2 (selected years) and Supplementary Table S1 (all years). Initially, consultation usage occurred more in urban municipalities with larger populations and lower PHC coverage. Over time, consultations expanded to smaller and more nonurban municipalities. Of note, one municipality may be considered with consultation in 1 year and without in the other, as it may have performed no consultation in the following year.
Comparison Between Municipalities With and Without Consultations Divided by Year in 2014, 2017, and 2019
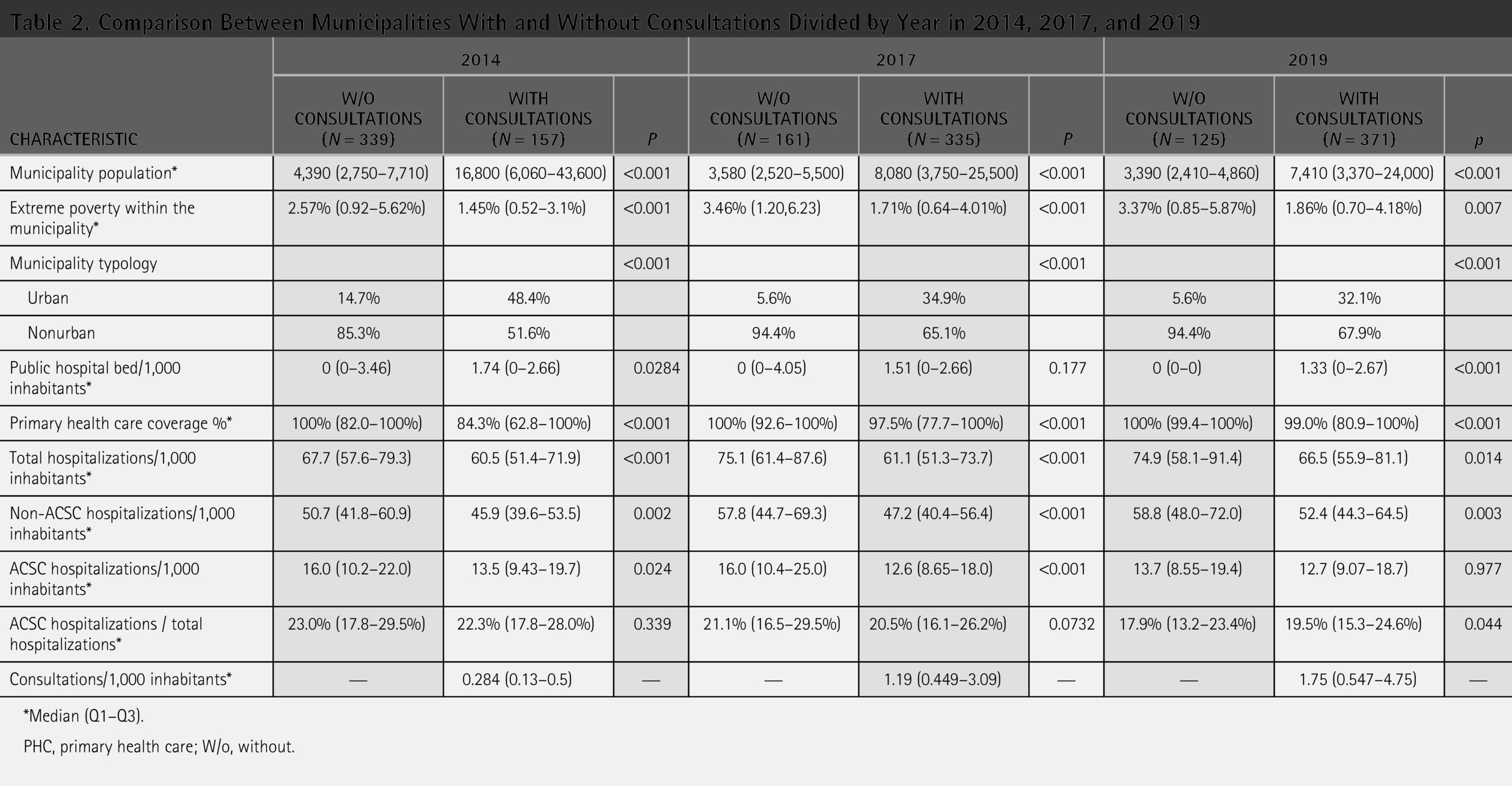
*Median (Q1–Q3).
PHC, primary health care; W/o, without.
As shown in Table 1, the median rate of hospital admissions by residence location was 64.8 per 1,000 inhabitants (IQR = 55.1–77.6) in the first year of the study (2014). ACSC hospitalizations accounted for 22.6% (IQR = 17.8 − 28.9%) of all admissions, representing 15.3 admissions per 1,000 inhabitants (IQR = 9.9–21.2). Throughout the study period, there was a reduction in ACSC hospitalizations, and by 2019, it was 12.8 per 1,000 inhabitants (IQR = 8.9–18.8), representing 19.2% (IQR = 14.8–24.2) of all admissions. Conversely, we identified an increase in total hospital admission rates over the years, reaching 67.8 (IQR = 56.4–84.9) per 1,000 inhabitants in 2019. Fig. 1 depicts the number of municipalities performing consultations, the consultation rate and ACSC hospitalizations per 1,000 inhabitants over the years. As shown in Table 2 (selected years) and Supplementary Table S1 (whole set), ACSC hospitalizations are less frequent in municipalities that performed consultations in every included year.
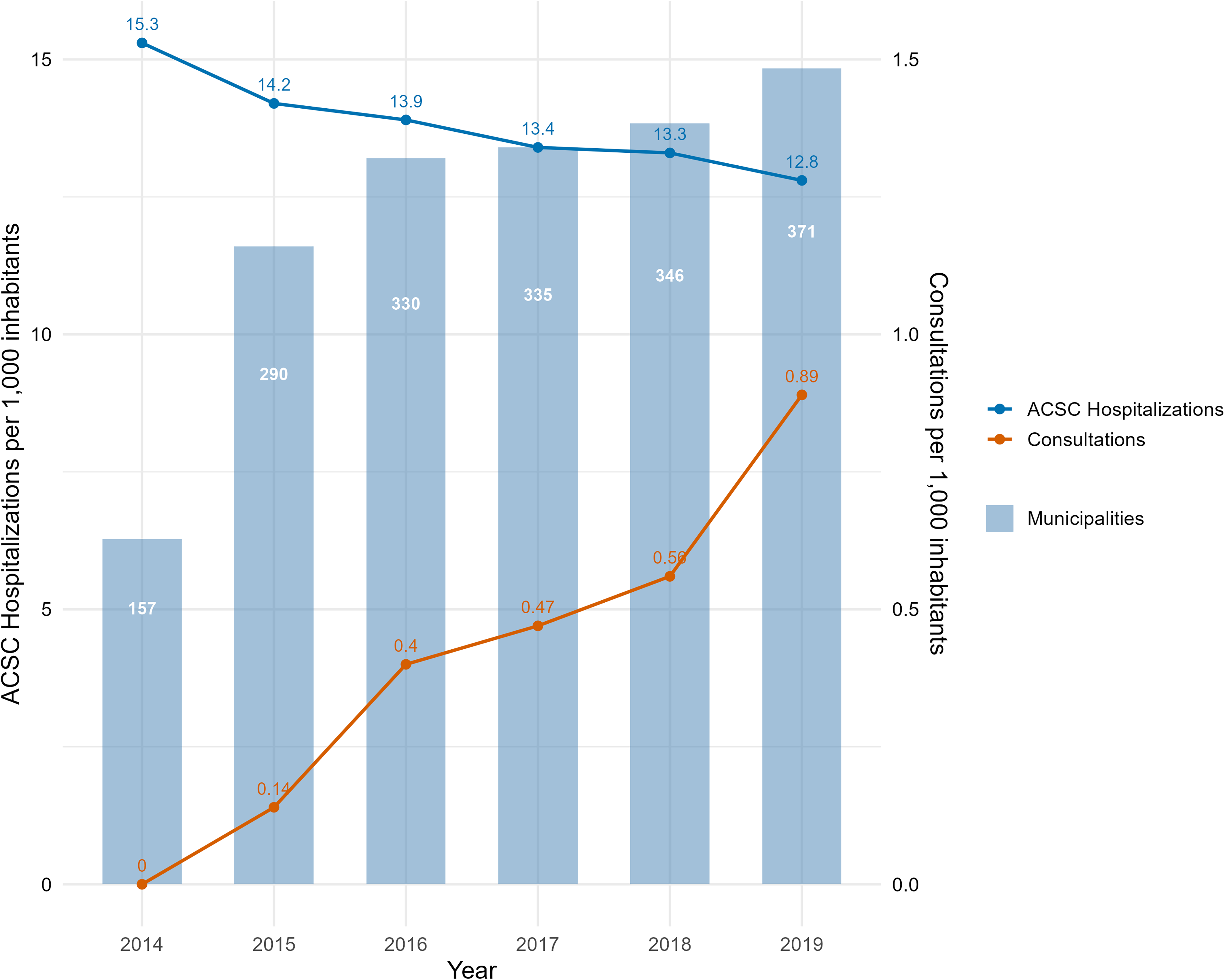
Number of municipalities performing consultations, consultation rate and ACSC hospitalizations per 1,000 inhabitants over the years. ACSC, ambulatory care sensitive conditions.
Following the predefined hierarchical approach, we identified that the following variables were independently associated with ACSC hospitalizations in the final model: time (year), extreme poverty, municipality typology, public hospital bed availability, non-ACSC hospitalizations, and consultations performed by the municipality. There was a significant interaction between year and municipality typology, public hospital bed availability, and consultations. The coefficients and the confidence interval of the statistically significant factors of this analysis are presented in Table 3; in summary, ASCS hospitalizations reduced over the years with higher consultation usage and increased with higher public hospital bed availability. The detailed model is presented in Supplementary Table S2.
Regression Coefficients and 95% Confidence Intervals of Variables Associated with ACSC Hospitalizations per Thousand Inhabitants in Rio Grande Do Sul between 2014 and 2019 in the Final Model
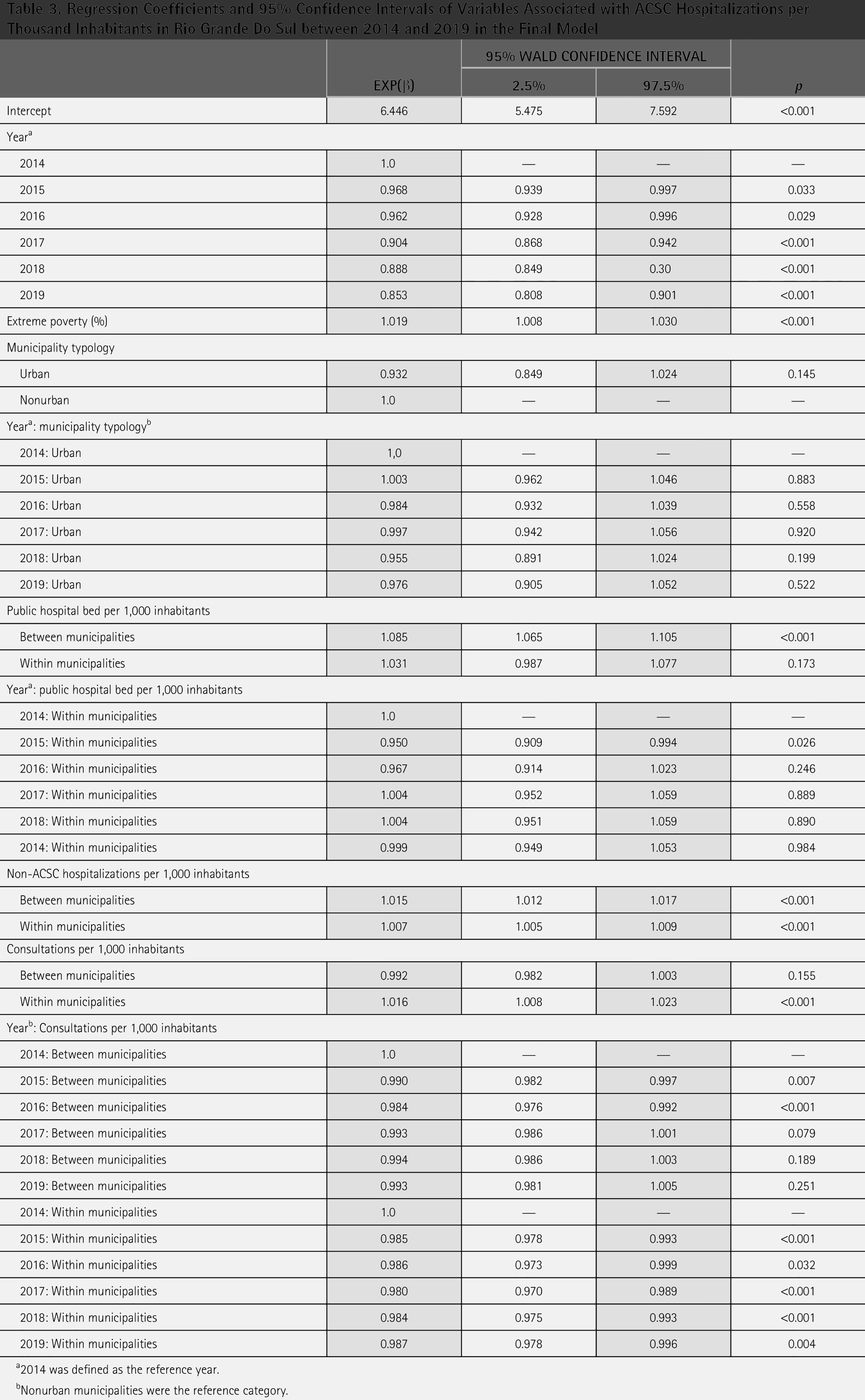
2014 was defined as the reference year.
Nonurban municipalities were the reference category.
The predicted ASCS hospitalization according to consultation usage is presented in Fig. 2. Over the years and in all scenarios, municipalities that performed more consultations per 1,000 habitants had a lower predicted rate of ASCS hospitalization. This relation was maintained (and even increased) with different scenarios of within-municipality consultation variation; that is, municipalities with a higher increase of consultation usage had a greater reduction in ACSC hospitalizations.
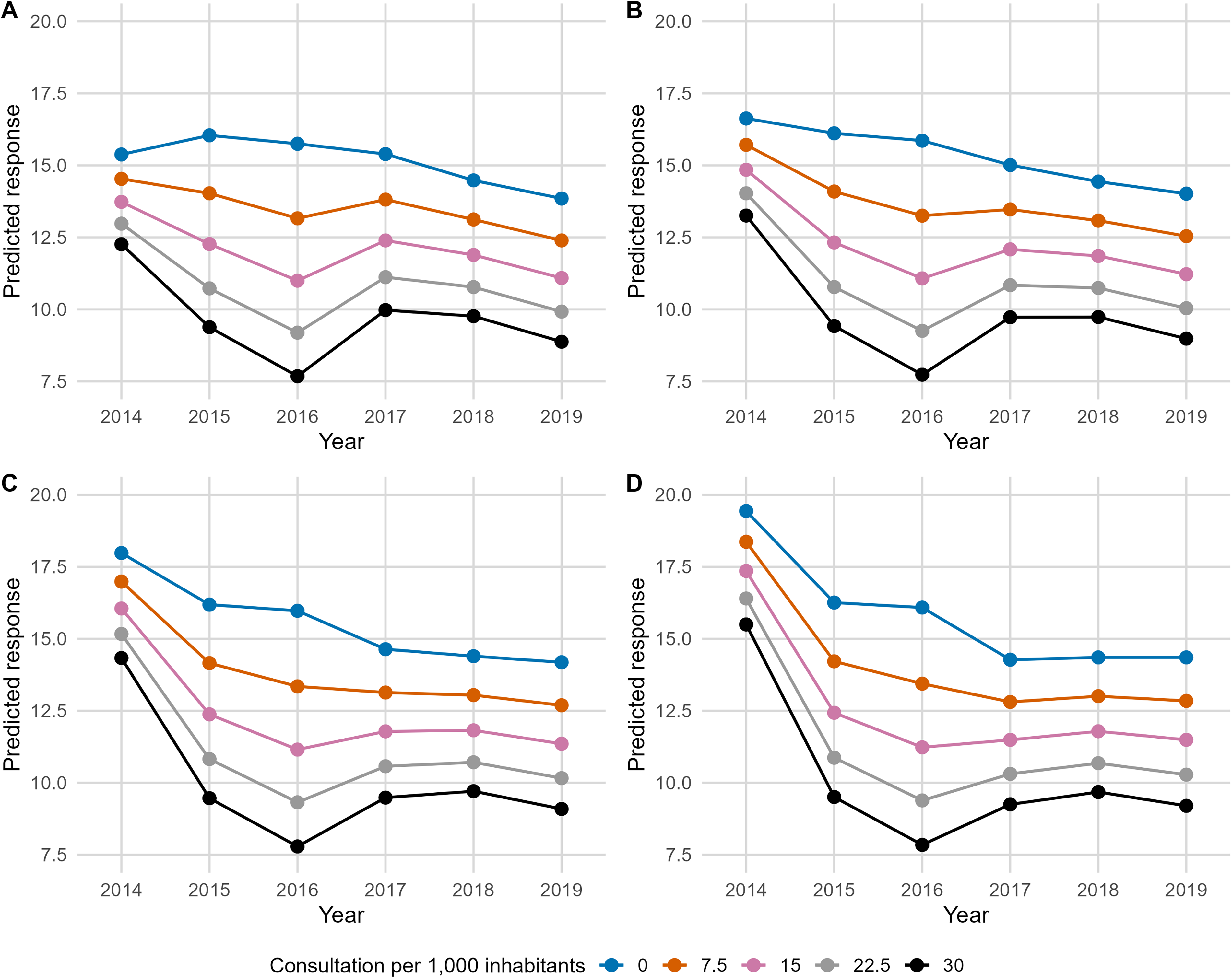
Relation between predicted ACSC hospitalization and consultations in different scenarios as predicted by GEE model:
Discussion
Data from our study indicate a reduction in hospitalizations for ACSC from 2014 to 2019 and suggest that some of this effect may be due to synchronous remote consultations. This relation was maintained (and even increased) with different between- and within-municipalities consultation variation scenarios. An expansion in the use of the TelessaúdeRS service was also observed, even in a state with high PHC coverage.
Consultancy between a primary care doctor and a consultant doctor is a powerful moment of continuing education, as it encourages the knowledge acquired to be applied to other patients. 8 Both synchronous and asynchronous provider-to-provider remote consultation models have demonstrated significant advantages for primary care by improving access, efficiency, clinical outcomes, and provider and patient satisfaction.8–10 By reducing unnecessary referrals, supporting clinical decision-making, and proving cost-effective, consultations represent a valuable strategy for strengthening PHC and improving care for ACSC.9,10 Since 2013, TelessaúdeRS has been offering spontaneous synchronous consultations, when the primary care doctor contacts our hotline, or induced consultations, for referrals of patients on the waiting list for specialized medical consultation.
Studies evaluating the evolution of ACSC over time commonly find that strengthening PHC reduces this type of hospitalization, even in different contexts and despite methodological variations. Achieving this effect requires promoting access and improving the quality of care at this level, especially for the most vulnerable populations.15,32,33 Additionally, systematic training for PHC professionals has been shown to reduce ACSC. 34 In summary, our study is consistent with these findings. It suggests that providing a support service for primary care physicians can help prevent avoidable hospitalizations—a key indicator of improved service delivery.
In the interplay between telehealth and hospitalizations, evidence has shown that telehealth can reduce overall hospitalizations, including ACSC, although the magnitude of these effects varies by context and study design.8,35,36 Regarding provider-to-provider remote consultations, our results also align with previous evidence suggesting that these initiatives may reduce the use of acute and specialized services.8–10 Specifically, Cruz et al. analyzed 132 text-based endocrinology consultations performed by PHC physicians and found that, despite the small sample size, these interactions were associated with fewer emergency visits or hospitalizations. 37
Similarly, a subsequent study by the same group, which evaluated consultations across a broader range of specialties (cardiology, gastroenterology, hematology, infectious diseases, nephrology, pulmonology, rheumatology, and sleep medicine), showed that few patients required emergency care or hospital admission for issues related to the initial consultation. 38 A broader review covering 13 telephone-based teleconsultation services for PHC professionals in 7 countries also reported reductions in hospitalizations, emergency visits, and specialist referrals, despite substantial variation in the number of consultations assessed (from 19 to 4,500). 9 However, none of these studies specifically examined their impact on ACSC hospitalization rates.
Since health in general and health-related behaviors are determined by socioeconomic, cultural, individual, and health service delivery factors, as well as differences in governance and institutional protocols, 39 careful interpretation is required when analyzing the impact of PHC on avoidable hospitalizations.20,33 For ACSC to be used as an indicator of primary care quality, adjustments must be made to the factors inherent to the population and the health system.15,20 Our study accounted for this necessity, and the analyses were adjusted for various confounding factors.
First, we considered the typology of municipalities. Consistent with findings in the literature,32,33,40 our study results indicate a more significant reduction in ACSC hospitalizations in urban municipalities compared with rural and intermediate ones. Despite poverty’s improvement in Rio Grande do Sul during the study period, it was not associated with changes in ACSC hospitalizations in the evaluated municipalities. Both factors were included in our analyses. Second, we assessed the effect of the number of available hospital beds on the outcome of interest. An increase in available hospital beds is associated with higher rates of avoidable hospitalizations.41,42
Similarly, we included changes in the availability of public hospital beds in our evaluation. Notably, during the analyzed period, there was a reduction in hospital beds in Rio Grande do Sul. Finally, we incorporated PHC coverage into our model, as this factor is inversely associated with ACSC hospitalizations.41,43 However, this association was not observed in our study, possibly due to the low variation in this indicator within our population.
Limitations
Despite these strengths, it is important to highlight the limitations regarding causal inferences due to the ecological design of this study. Therefore, caution is needed when interpreting these results. We attempted to address this limitation by employing a robust and conservative statistical analysis of the data and, as discussed above, adjusting for the most significant determinants of ACSC hospitalizations described in both national and international literature.15,44,45 On the other hand, this kind of complex analysis may limit the interpretability of the results—a problem we addressed by presenting predicted scenarios graphically.
Other potentially relevant confounding factors were not explored due to their unavailability in secondary data sources within the context of this study. These include individual-level aspects of health teams, such as the presence of multidisciplinary teams, involvement in teaching activities, the duration of professionals and teams’ work in the territory, the availability of family and community physicians, and access barriers. Furthermore, the chosen statistical model does not allow for generalizing results to the individual level (municipalities).
Future research should include a longer study period to determine whether the increased use of TelessaúdeRS consultations over time consistently reduces ACSC hospitalizations. Additionally, it is suggested that other covariates, such as age distribution and specific population groups, be investigated to assess their potential influence on the association between consultations and avoidable hospitalizations. Moreover, applying other tools to evaluate PHC quality could enhance the investigation of this relationship. Finally, further studies should explore the influence of characteristics inherent to health teams and factors related to the use of consultations by PHC physicians, such as awareness and dissemination of the TelessaúdeRS 0800 hotline and local management incentives for utilizing this tool.
Conclusion
In conclusion, the data from this study suggest that consultations may play a role in reducing ACSC hospitalizations. In other words, remote clinical discussions appear to enhance PHC professionals’ performance and improve patient care, improve the performance of PHC professionals and the quality of patient care. These findings support decision-making by health managers regarding promoting and funding remote consultations as a strategy to improve care quality and potentially limit costs associated with avoidable hospitalizations.
Authors’ Contributions
L.E.B.M. contributed to conceptualization, data curation, formal analysis, writing—original draft preparation, and writing—review and editing. D.V.R. contributed to conceptualization, data curation, and writing—review and editing. R.R. contributed to conceptualization, data curation, and writing—review and editing; E.B.O. contributed to conceptualization and writing—review and editing. N.K. conceptualization and writing—review and editing. M.R.G. contributed to conceptualization and writing—review and editing. C.G. contributed to supervision and writing—review and editing.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest to disclosures for current work.
Funding Information
This research was supported by grants and material support from the following Brazilian agencies: Committee for the Development of Higher Education Personnel (CAPES), National Council for Scientific and Technological Development (CNPq), Universidade Federal do Rio Grande do Sul e Hospital de Clínicas de Porto Alegre. TelessaúdeRS is funded by multiple sources, including the Brazilian Ministry of Health and Rio Grande do Sul state health agency.
Data Availability Statement
Artificial Intelligence Usage
This article was written by the authors and AI was used for improving language as a nonnative speakers (Grammarly premium subscription).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.