
Abstract
Background:
Patient portals have become widespread since the passage of the American 21st Century Cures Act. However, little is known about how people are using these portals, especially for accessing telemedicine.
Methods:
We investigated patterns patient portal usage among a nationally representative sample of United States adults, focusing on the demographic factors influencing access and engagement. Using the RAND American Life Panel, we surveyed 1,672 people to assess their experiences with various portal functions, including viewing test results, messaging providers, and scheduling appointments.
Results:
Our findings reveal that about three-quarters of respondents had used portals to view test results and to access health records, about half have used to message a provider, schedule an appointment, or pay a bill. However, we found significant differences in portal usage with women, non-Hispanic white people, people with college degrees, and those with higher self-reported technological proficiency all more likely to use portals.
Conclusions:
These results highlight the need for targeted interventions to enhance accessibility and usability of patient portals, ensuring access to health care resources for all individuals, particularly those from underrepresented populations.
Keywords
Introduction
With the widespread adoption of electronic health records in the United States (U.S.) over the past decade and the American 21st Century Cures Act mandating that patients have access to those records, about 60% of Americans have accessed a patient portal as of 2022.1,2 Patient portals can have both clinical and administrative functions; for example, they allow patients to view test results, exchange secure messages, and pay bills online.3,4 Although portal use has been associated with positive health outcomes, its impact on health service utilization is unclear. 5 Older and socioeconomically disadvantaged populations may also have worse access to patient portals due to lack of familiarity with technology or lack of private access to the tools, such as high-speed internet, that make it possible.1,6
While patient portals support a variety of clinical and administrative functions, one increasingly important capability is facilitating telehealth visits. Telemedicine has emerged as a critical component of modern health care delivery, particularly following the COVID-19 pandemic, offering patients greater accessibility to care, reduced travel burden, and convenience, though telehealth use is lower in rural areas. 7 Portal-integrated telehealth represents a key technological advancement in expanding equitable access to health services. 8
Understanding the use of patient portals could enhance our understanding of specific functions patients utilize the most and help practitioners, portal developers, and policymakers better align portal functionality with patient needs. Therefore, we assessed patterns of patient portal use in a nationally representative sample to determine how often portals were used for specific purposes as well as to identify associations of use of such with demographics and other patient characteristics to better understand the role patient portals play in U.S. health care today.
Methods
We conducted an online survey using the RAND American Life Panel (ALP), which produces nationally representative estimates from a probability-based representative sample of the U.S. adult population aged 20 years or older. 9 The ALP recruited its first wave of participants in 2002 and is continually refreshed to create a total current panel size of approximately 6,000 participants. 9 Participants have been recruited from other nationally representative probability-based panels, sampling in zip codes with high percentages of racial minority groups, and random digit dialing. 9 Participants consented to be a part of the panel. Panel participants are given internet-connected devices and are paid $13 for completing this survey. For the present survey study, the data were obtained from a survey fielded between August 21 and September 4, 2024.
The survey contained questions regarding technology in health care, focusing specifically on patient portal use: “Have you ever used a patient portal (a secure website from your doctor that lets you access your health information, like MyChart) to do any of the following?” and provided respondents with a list of different patient portal functions, such as viewing test results or messaging providers, and then asked respondents to check any functions they had used. The relevant questions asked in the survey and answer options can be found in Supplementary Data.
This study was deemed exempt from human subjects review under the adult interview and survey exemption by the RAND Institutional Review Board, so informed consent was waived. We followed the American Association for Public Opinion Research reporting guideline.
Statistical Analysis
We used response weights to produce nationally representative estimates of answers to the survey questions. 9 Weights were generated through a raking process using the demographic data of participants (sex, age, race and ethnicity, educational level, household income, and number of household members). 9 Analyses were conducted using version 9.4 of the SAS system for Linux and SAS/STAT software, version 15.1, 10 employing SAS survey analysis procedures where appropriate. The threshold for statistical significance was set at p < 0.05.
We calculated descriptive statistics (counts, means, and SEs) and cross-tabulated frequencies and percentages. We used logistic regression for multivariate predictions of agreement, controlling for demographic variables (sex, age, race and ethnicity, educational level, marital status, employment status, general health, and urbanicity) and self-reported time spent on social media and self-reported technological savvy. Some demographic categories were combined for regression analysis. Missing data were limited (<1% of all variables) and likely random; entries with missing values were dropped from the adjusted analyses.
Results
The survey was fielded to 2,295 members of the panel; 1,672 respondents completed the survey (73% completion rate). Of the weighted sample, 51% of respondents were women; the average age was 49, and 61% were white. More details about the survey sample can be found in Table 1.
Demographics of Survey Respondents
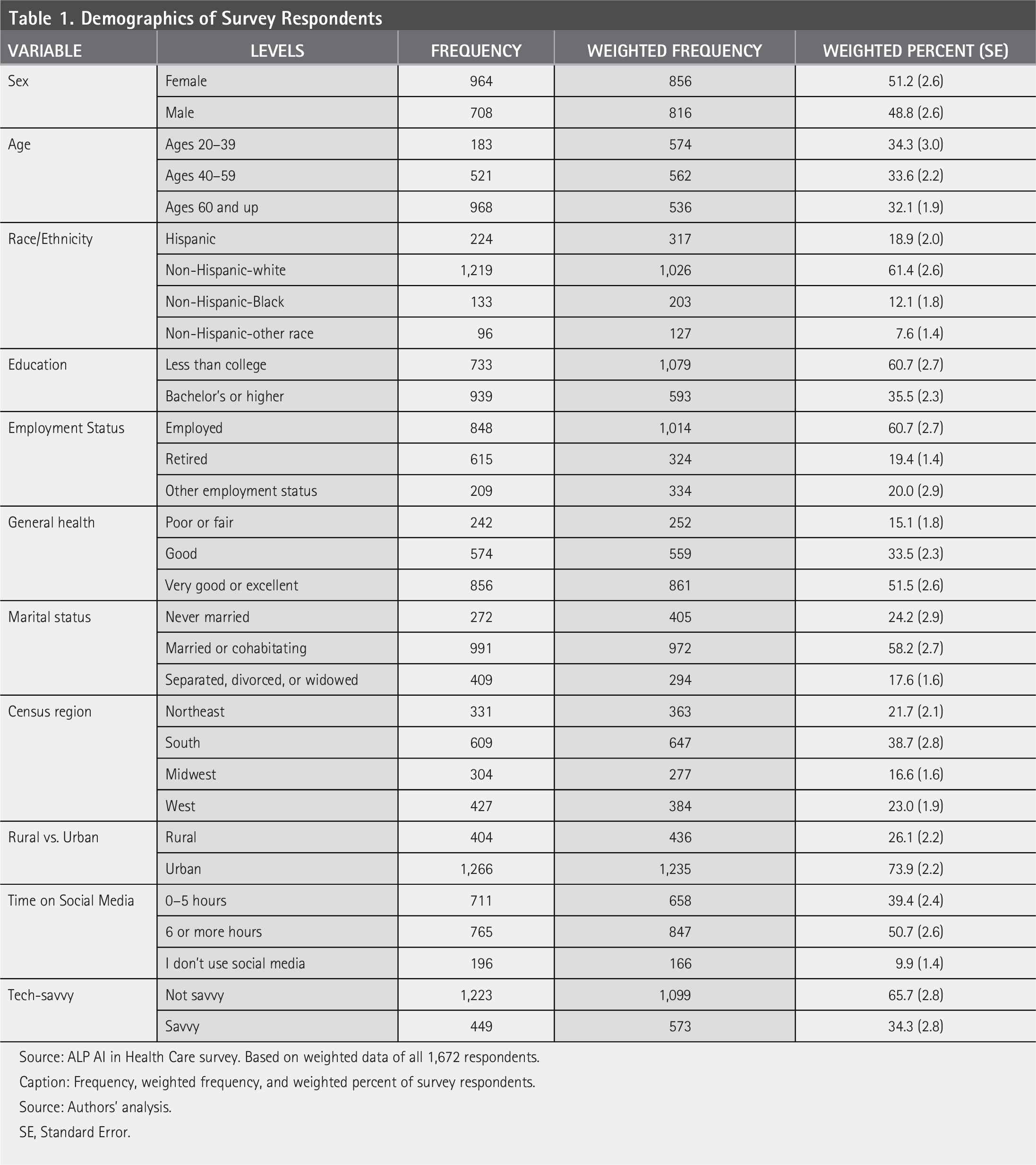
Source: ALP AI in Health Care survey. Based on weighted data of all 1,672 respondents.
Caption: Frequency, weighted frequency, and weighted percent of survey respondents.
Source: Authors’ analysis.
SE, Standard Error.
We found that about 85% of the public has used a patient portal at least once (Fig. 1). More than 70% of people have used a patient portal to view test results or access health records. About half have messaged a provider, scheduled an appointment, or paid a bill. Two fifths have requested a medication refill, about 1 in 5 had a telehealth visit through the portal, and fewer than 1 in 10 have accessed education resources. About 14% of respondents had either never used a patient portal or were uncertain if they had.
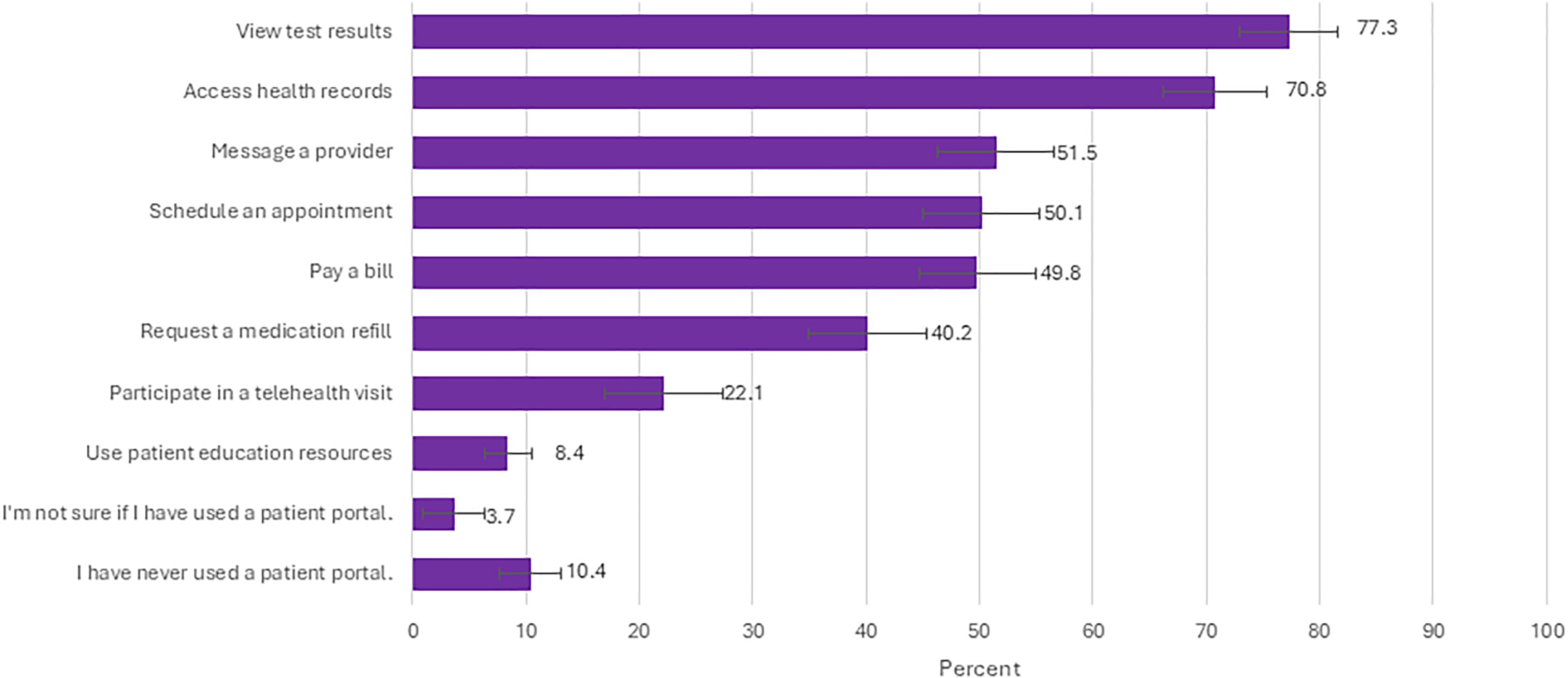
Use of patient portal for different use cases (respondents could choose multiple uses, or that they weren’t sure, or that they had never used one).
We employed logistic regression to identify factors predicting any use of the portal (Table 2). Women were more likely than men to report using the portal (odds ratio [OR] = 2.52, p = 0.001). Respondents who felt they were tech-savvy were more than three times as likely to have used a portal (OR = 3.16, p = 0.016), and those with an above-average use of social media were almost twice as likely (OR = 1.95, p = 0.045). Respondents without a college degree were less likely to report portal use than those with a college degree (OR = 0.44, p = 0.031).
Significant Factors Associated with Different Types of Portal Use
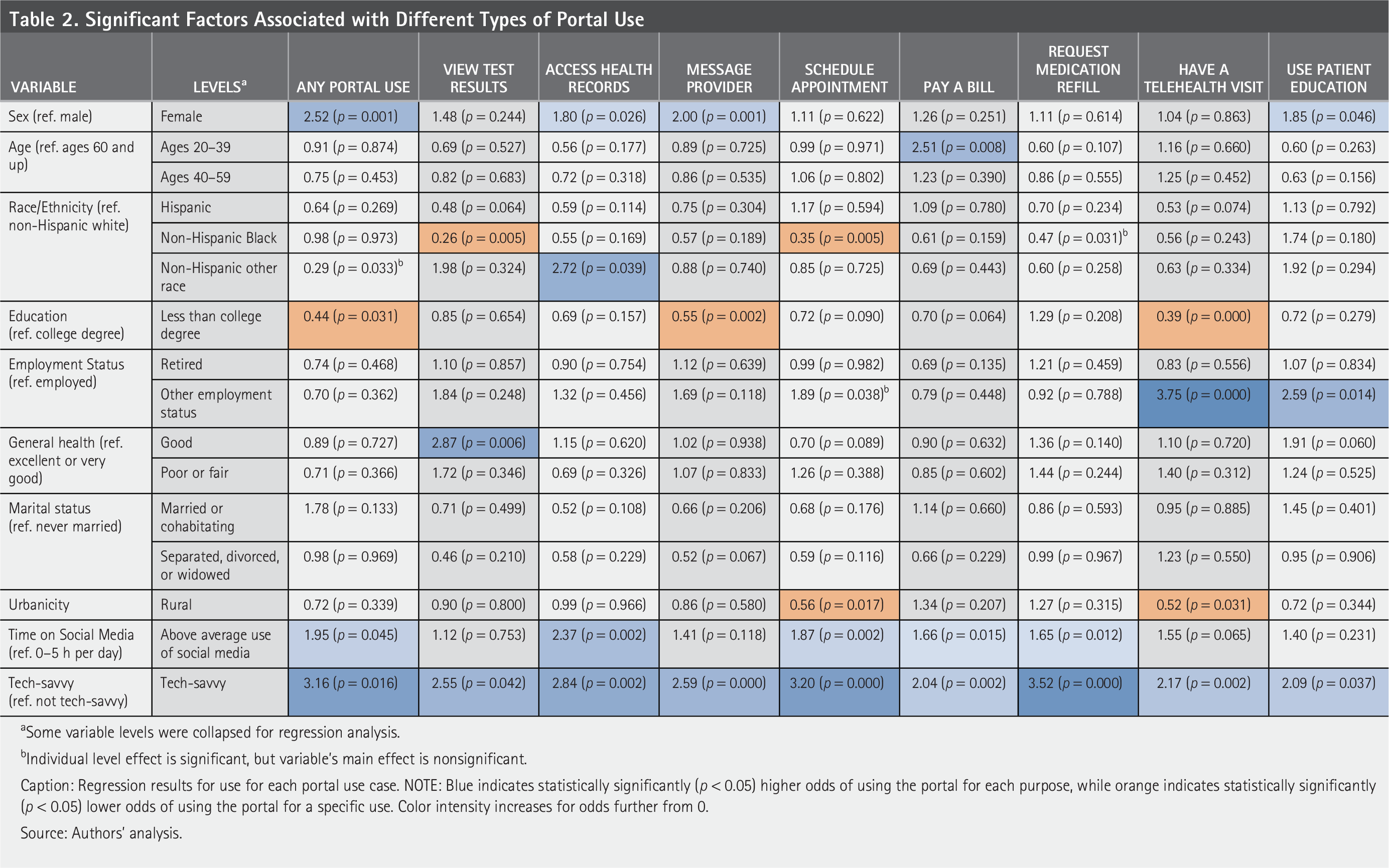
Some variable levels were collapsed for regression analysis.
Individual level effect is significant, but variable’s main effect is nonsignificant.
Caption: Regression results for use for each portal use case. NOTE: Blue indicates statistically significantly (p < 0.05) higher odds of using the portal for each purpose, while orange indicates statistically significantly (p < 0.05) lower odds of using the portal for a specific use. Color intensity increases for odds further from 0.
Source: Authors’ analysis.
We also used logistic regression to predict specific portal uses. For all specific uses, those who defined themselves as tech-savvy were more likely to use the portal for that purpose, from 2 times more likely to pay a bill or use patient education resources to more than 3 and a half times likely to request a medication refill. Those reporting above average social media use also used the portal for more use cases (including accessing health records, scheduling appointments, paying bills, and requesting medication refills). Women also had increased odds of using the portal to message providers, access health records, and use patient education resources.
For each use case, we identified other statistically significant demographic predictors of use. Over three-quarters of people used their portal for viewing test results. Compared to those with excellent health, those with good health were almost three times as likely to look at a portal for test results (OR = 2.87, p = 0.006). Non-Hispanic Black people were less likely than non-Hispanic white people to use portals for this purpose (OR = 0.26, p = 0.005). Almost 71% of people accessed health records on their portal. Non-Hispanic, non-Black/non-white respondents were significantly more likely than white respondents (OR = 2.72, p = 0.039).
More than half of respondents messaged a provider through a patient portal. People without a college degree were less likely to message a provider via their portal (OR = 0.55, p = 0.002).
Just over 50% scheduled an appointment through a patient portal. However, non-Hispanic Black respondents (OR = 0.35, p = 0.005) and those living in rural areas (OR = 0.56, p = 0.017) were less likely to have done so. Almost half of respondents used their portal to pay a bill. Younger people (OR = 2.51, p = 0.008) were more likely to have used a portal to pay their bills. 40% of people had requested a medication refill.
About 22% of respondents participated in a telehealth visit through their patient portal. Compared to employed people, those who are not employed and not retired were more likely to have a telehealth visit (OR = 3.75, p < 0.001). Respondents with lower education (OR = 0.39, p < 0.001) and those who lived in rural areas (OR = 0.52, p = 0.031) were less likely to have engaged in telehealth through their portals. The least frequent use of the portal was for patient education, something less than 10% of people had done. Respondents who were neither employed nor retired were more likely to report use of a portal for education (OR = 2.59, p = 0.014).
Discussion
With patient portals now widely adopted among the general population, this nationally representative study offers insights into specific uses and how those uses vary across different patient demographic groups. The different administrative and clinical functions of patient portals likely have different impacts on patient care and experience. We found that patients are using portals more for clinical functions, such as viewing test results or accessing health records, than for administrative functions like scheduling appointments and paying bills; those were less commonly used but still used by a sizable portion of respondents.
Overall, portals are used more by women, those with college degrees, heavy social media users, and those who describe themselves as tech-savvy. Some factors driving increased specific uses of portals are straightforward, such as educational attainment, which was correlated with portal use. Similarly, those who consider themselves technologically adept demonstrate higher engagement with the portal across nearly all functions.
Notably, only about one-fifth of respondents reported using their patient portal to participate in telehealth visits, suggesting that portal-integrated telehealth remains underutilized relative to other portal functions. This is particularly concerning given telemedicine’s demonstrated potential to improve care access and outcomes. Our finding that rural residents and those with lower educational attainment were significantly less likely to engage in portal-based telehealth suggests that digital disparities extend to this increasingly essential mode of care delivery. These barriers may reflect not only technological challenges but also underlying disparities in broadband access and digital literacy that threaten to widen health inequities. Future efforts must prioritize removing these barriers to ensure telemedicine fulfills its promise as a tool for equitable, accessible health care.
However, other differences were less readily explained, such as those related to race, education, and employment status. Urbanicity also played a role; while those living rurally have less access to care, they were significantly less likely to use the portal for scheduling or telehealth, perhaps due to internet access or another factor associated with rural living. While some disparities are specific to particular use cases, others are more pervasive; for example, women are generally more likely to use portals, whereas non-Hispanic Black respondents and people living rurally tend to use them less across multiple use cases.
This study has some limitations. Though the ALP produces nationally representative estimates and attempts to reach individuals without computers, it may not reach individuals who do not speak English. Additionally, while we had a large overall sample, our study was not powered to detect differences by each demographic group or to explore interactions between demographic groups. Also, each health system’s patient portal is different, so all functions may not be available to every patient surveyed (i.e., some patients may not have the ability to schedule visits in their patient portal).
Increasing access and use are important because portals can potentially help patients with ongoing medical needs, streamlining adherence to medication schedules and chronic disease management. 11 However, despite potential savings of patient portals, early research showed no change in the number of face-to-face visits conducted after a portal was adopted despite an anticipated decrease in visits,12,13 and the messaging feature may in fact increase the burden on physicians outside of clinical visits, 14 thus the direct impact on cost is not yet known.
While patient portals provide numerous benefits, they also present challenges, particularly for individuals with limited technological proficiency or inadequate broadband access—both of which can restrict access to essential services and resources in today’s digital age. We found that self-reported tech-savviness was an especially powerful predictor of portal use, though only about a third of people describe themselves as tech-savvy. As technology becomes a larger part of health service delivery, providers could consider how this approach could harm less tech-savvy patients who are not willing or easily able to access information in patient portals, particularly elderly patients. Efforts are ongoing to enhance portal accessibility and usage among those less likely to currently use portals, such as men, racial minorities, and individuals with lower educational levels. Initiatives have been undertaken to address these disparities, including training programs to improve digital literacy (including skills navigating the internet and communicating electronically), outreach campaigns, and collaborations with providers and community organizations to provide support and resources.15,16 Additionally, the development of more intuitive and user-friendly portal interfaces may help bridge the gap for those less familiar with technology.
Future research should continue to explore the underlying causes of these disparities and evaluate the effectiveness of interventions aimed at increasing portal use among diverse demographic groups. Understanding these dynamics is critical to ensuring equitable access to health care resources and maximizing the potential benefits for all individuals.
Ethical Considerations
This study was approved by RAND’s institutional review board, approval 2024-N0039.
Consent to Publish
Respondents gave written consent before starting survey.
Authors’ Contributions
S.H.F., D.K., and Z.P.: Conceptualization and design. S.H.F., E.R., and Y.L.: Analysis. S.H.F., E.R., Y.L., D.K., and Z.P.: Drafting article—Revision.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was funded by the National Institute for Health Care Reform (contract number: NIHCR-112023).
Consent to Participate
Respondents gave written consent before starting survey.
Data Availability
The data from this study are available at alpdata.rand.org.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.