
Abstract
Background:
The rapid expansion of telemedicine has increased the relevance of teleconsultations in everyday clinical practice. However, the manner in which teleconsultation competencies are conceptualized, taught, and assessed in undergraduate medical education remains unclear.
Methods:
A narrative review was conducted using a transparent methodology to identify and select studies. Several bibliographic databases were searched using predefined eligibility criteria, focusing on educational interventions that specifically targeted teleconsultation competencies among undergraduate medical students. The selection process emphasized conceptual clarity, curricular intent, and the inclusion of empirically reported educational outcomes. The eligibility criteria were intentionally designed to identify studies that explicitly conceptualized teleconsultation as a distinct undergraduate clinical competency.
Results:
The search process yielded 199 records. After screening and comprehensive full-text evaluation, only one study explicitly conceptualized teleconsultation as a distinct undergraduate clinical competency and met all predefined eligibility criteria. This study details a structured educational intervention that frames teleconsultation as a distinct clinical competency. The outcomes concerning communication, clinical reasoning in virtual environments, technical aspects of teleconsultation, and components of remote physical examination were reported.
Conclusions:
The principal finding was the identification of substantial evidence gaps in the conceptualization, assessment, and longitudinal teaching of teleconsultation competencies. Current evidence regarding the instruction of teleconsultation competencies in undergraduate medical education is limited. The prevailing literature addresses telemedicine primarily as a mode of care delivery rather than emphasizing teleconsultation as a distinct clinical skill. These observations highlight a discrepancy between contemporary clinical practice and undergraduate training, emphasizing the need for well-defined educational frameworks that incorporate teleconsultation competencies.
Keywords
Introduction
Teleconsultation has become an established form of healthcare delivery, moving beyond its applications as an emergency solution during the COVID-19 pandemic.1–3 In many healthcare systems, teleconsultation is routinely used in primary care, specialist clinics, and follow-up medical services.1,4,5 This shift has fundamentally changed the way clinical visits are conducted, introducing new organizational, communication, and ethical challenges that are distinct from those encountered during traditional face-to-face consultations.
Teleconsultations not only entail a change in the interaction environment but also a different clinical context that requires specific competencies.5–11 Fundamental elements of medical practice, such as history-taking, clinical reasoning, shared decision-making, and professional communication, must be adapted to environments characterized by physical separation, limited nonverbal cues, and reliance on digital interfaces.1,12–14 Teleconsultations offer a unique educational setting for developing clinical reasoning skills, as diagnostic decisions often must be made with limited opportunities for direct physical examination. This necessitates a greater reliance on structured history-taking and explicitly articulated reasoning. These conditions affect both the structure of the consultation and the dynamics of the interaction between the physician and the patient, particularly in relationship-building, situational awareness, and the interpretation of contextual cues.15–18 Given the structure of teleconsultations, effective teleconsultation training may be most beneficial when learners have already acquired basic competencies in history-taking, physical examination, and clinical assessment.19–22
Undergraduate medical education plays a key role in preparing future physicians for evolving forms of care.20,21 Traditional curricula have been largely developed based on face-to-face clinical encounters with patients.5,23–25 Medical interviews, along with unrestricted observation of nonverbal behaviors, informal contextual cues available in clinical settings, and direct physical examination, play key roles.26,27 In classical and conservative educational models, students may begin clinical practice without being sufficiently prepared for the specific requirements of teleconsultation, despite demonstrating competence in conventional consultation.28–33
Telemedicine education, telehealth education, and teleconsultation competency training are frequently used interchangeably in the literature, although they represent distinct educational constructs.19,21 Telehealth and digital health curricula commonly include health informatics, remote monitoring, legal and ethical issues, digital systems, and technology-enabled care delivery. In contrast, teleconsultation competency training focuses specifically on remote clinical encounters between medical professionals and patients, including communication, clinical reasoning, consultation structure, virtual professionalism, and remote examination skills training.
Existing educational initiatives for teleconsultation training vary considerably in scope, pedagogical approaches, and target competencies.22,34 Some programs emphasize technical aspects, such as platform use and medical records, whereas others focus on communication skills, clinical reasoning, and ethical issues.19,34 However, the extent to which different teaching methods effectively support the acquisition of teleconsultation competencies remains unclear.22,34 Furthermore, previous reviews in this field have often taken a descriptive approach, aggregating studies without distinguishing between skill areas, assessment strategies, and educational contexts. 35
Therefore, a structured synthesis of the available evidence is needed to clarify which competencies are being taught, how they are assessed, and where the gaps in the literature are. Rather than evaluating technological solutions in isolation from the context, such a synthesis should focus on teaching teleconsultation as a complex educational and clinical practice that integrates communicative, cognitive, organizational, and professional dimensions.36–38
An additional challenge is the place of teleconsultation training in undergraduate medical curricula. Many published educational initiatives have been implemented during the early years of medical education, including first-year and preclerkship education. While such approaches may increase familiarity with telemedicine and digital health concepts, teleconsultation differs from many introductory digital health topics because it relies heavily on pre-existing clinical competencies. Effective teleconsultation requires adapting history-taking, physical examination, clinical reasoning, and patient management skills to a remote environment, rather than replacing these competencies. Consequently, teleconsultation may not be viewed as a foundational competency but as an advanced clinical competency that builds upon prior experience in direct patient assessment and clinical decision-making.33,34,39 This raises important questions regarding the optimal timing, sequencing, and integration of teleconsultation training into undergraduate medical education.
Despite the extensive literature on telemedicine, it is often regarded merely as a mode of care delivery or educational exposure rather than as a distinct clinical competency. This narrative review investigates the instruction of teleconsultation competencies and skills in medical education. The objectives of this review include identifying the competencies taught, the educational strategies used, and the methods used to assess learning outcomes. By mapping current approaches and identifying areas of convergence and limitations, this review seeks to provide valuable insights for curriculum development and support a more structured, competency-based integration of teleconsultation training into medical school curricula.
Based on the reviewed literature, teleconsultation competency was operationally defined as an integrated set of knowledge, skills, and professional behaviors required to conduct a safe, effective, patient-centered remote clinical consultation.
Methods
STUDY DESIGN
This study employed a narrative review methodology, characterized by transparent procedures for study identification and selection, to critically examine the conceptualization and instruction of teleconsultation competencies in undergraduate medical education. This review did not aim to provide a comprehensive mapping of the literature or a quantitative synthesis. Instead, it focuses on a critical analysis of how these competencies are conceptualized and taught. Owing to the conceptual diversity within the literature, a structured narrative and interpretive synthesis were utilized. This review, based solely on the published literature, did not involve human participants, human data, or identifiable personal information. Consequently, ethical approval and informed consent were not required for this study.
RESEARCH QUESTIONS
This review was based on the following research questions: (1) What competencies and skills related to teleconsultations are included in undergraduate medical education? (2) Which educational strategies and teaching formats have been used to develop these competencies? (3) How are learning outcomes related to teleconsultation competencies assessed? and (4) What gaps and limitations have been identified in existing educational approaches?
SEARCH STRATEGY
A structured search was performed across multiple bibliographic databases, supplemented by targeted semantic and citation-based searches. A comprehensive literature search was conducted using PubMed, Scopus, and Web of Science databases. To enhance coverage and reduce database bias, additional semantic and citation-based searches were conducted using the Semantic Scholar, OpenAlex, and Google Scholar databases. Citation chasing and semantic searches were used to identify potentially relevant studies. Search terms were chosen to focus on educational interventions related to teleconsultation competencies rather than telemedicine technologies or service delivery models. The complete search strategy was iteratively refined to optimize conceptual relevance.
ELIGIBILITY CRITERIA
Studies were eligible for inclusion if they involved undergraduate medical students, described an educational intervention with an explicit focus on teleconsultation competencies, conceptualized teleconsultation as a distinct clinical skill set, and reported empirical educational outcomes. All four eligibility criteria had to be fulfilled simultaneously for inclusion in the study. Studies were excluded if telemedicine was used solely as a mode of care delivery, as an observational exposure, or as a logistical solution without explicit instructional intent related to teleconsultation competencies.
STUDY SELECTION
Study selection was independently performed by at least two reviewers each time. Discrepancies were resolved through discussion to reach consensus among the reviewers. A narrative review with a transparent study identification and selection procedure flow diagram was used to document the selection process and enhance transparency.
DATA EXTRACTION
The authors developed and piloted a predefined data extraction matrix before data extraction. This matrix encompassed study characteristics, educational settings, target competencies, instructional methods, assessment approaches, and reported educational outcomes. The extracted variables included study characteristics, educational context, target competencies, teaching methods, assessment strategies, and reported outcomes. Additionally, where applicable, details regarding the study design and assessment methods were documented to facilitate interpretive synthesis.
DATA SYNTHESIS
Due to the diversity of educational designs and outcome measures, data were synthesized using a structured narrative and interpretive approach rather than a quantitative aggregate method. The studies were categorized according to their primary areas of competence, educational strategies, and assessment methods. This approach facilitated the identification of recurring patterns, areas of convergence, and persistent gaps in the literature while preserving contextual and methodological diversity.
METHODOLOGICAL CONSIDERATIONS
Owing to the limited number of eligible studies, their characteristics are described narratively in the main text. Supplementary Table S1 summarizes the studies contributing to the broader interpretive synthesis, including educational settings, competency domains, teaching methods, assessment approaches, and reported outcomes. This study, as a narrative review employing narrative and interpretive synthesis, prioritizes breadth and conceptual mapping over a formal evaluation of the intervention’s effectiveness. The principles of narrative review guided the procedures for study identification and selection, ensuring transparency and reproducibility while allowing the flexibility necessary for a narrative and interpretive synthesis.
Results
SELECTION AND CHARACTERISTICS OF STUDIES
A comprehensive literature search yielded 199 records screened. After screening titles and abstracts and evaluating full texts, one study met all predefined eligibility criteria and was incorporated into the final narrative synthesis. This sole eligible study focused on teleconsultation training, emphasizing communication skills, structured history-taking, clinical reasoning, technical aspects of video consultations, and components of remote physical examinations. Similar competency domains have been described in the broader telemedicine education literature. The study included in the synthesis detailed a structured, skills-based educational intervention aimed at introducing teleconsultation competencies to undergraduate medical students within a preclerkship curriculum. The intervention specifically targeted communication strategies, clinical reasoning in virtual encounters, technical aspects of video-based consultations, and elements of remote physical examination.
The educational intervention by Cornes et al. 39 was selected because it explicitly conceptualized teleconsultation as a distinct clinical competency and described a structured, skills-based educational intervention in an undergraduate medical curriculum. Unlike most excluded studies, which used telemedicine primarily as a mode of care delivery or educational infrastructure, this intervention defined clear learning objectives related to teleconsultation. These objectives included communication strategies in virtual encounters, clinical reasoning in remote settings, technical aspects of video consultations, and elements of remote physical examination. Additionally, the study reported empirical educational outcomes aligned with these competencies, supporting their inclusion in the narrative synthesis. This study differed from most publications in that teleconsultation was not treated as an incidental component of clinical exposure or telehealth logistics but as a core clinical skill requiring structured instruction and evaluation. This distinction was central to the eligibility criteria applied in this review.
AREAS OF COMPETENCE INCLUDED IN TELECONSULTATION TRAINING
The eligible studies identified in this review focused primarily on verbal communication skills, structured history-taking, clinical reasoning in virtual encounters, technical aspects of teleconsultation, and selected components of remote physical examination. These competency domains are frequently discussed in the broader telemedicine and telehealth education literature. An emphasis was placed on the clarity of questioning, logical sequencing of information, and explicit verbalization of clinical reasoning in situations where opportunities for direct physical examination are limited.
The broader literature highlights the importance of clinical reasoning in remote contexts, often through case-based discussions, simulated consultations, and structured virtual encounters. These educational approaches are intended to support hypothesis generation, prioritization of differential diagnoses, and decision-making in conditions of diagnostic uncertainty. Technical and organizational competencies, including the use of teleconsultation platforms, documentation practices, privacy considerations, and consultation management, are commonly described as foundational requirements for effective teleconsultation practice.
In contrast, nonverbal communication skills, including the interpretation of body language, facial expressions, and subtle interactional cues, have been addressed less consistently in the literature. Similarly, competencies related to empathy, relationship building, and the management of emotionally complex consultations are rarely the primary focus of educational interventions and remain challenging to teach and assess in remote settings.
Based on the identified evidence gaps and interpretive synthesis of the broader telemedicine and digital health education literature, we developed a preliminary teleconsultation competency framework for undergraduate medical education. The framework is organized around four core competency domains and a cross-cutting domain of professionalism and reflective practice ( Table 1 ). Additional details regarding the studies contributing to the broader interpretive synthesis are provided in Supplementary Table S1. The framework should be regarded as a conceptual and hypothesis-generating framework intended to support future curriculum development and empirical evaluation, rather than as a formally validated competency model.
Proposed Teleconsultation Competency Framework for Undergraduate Medical Education
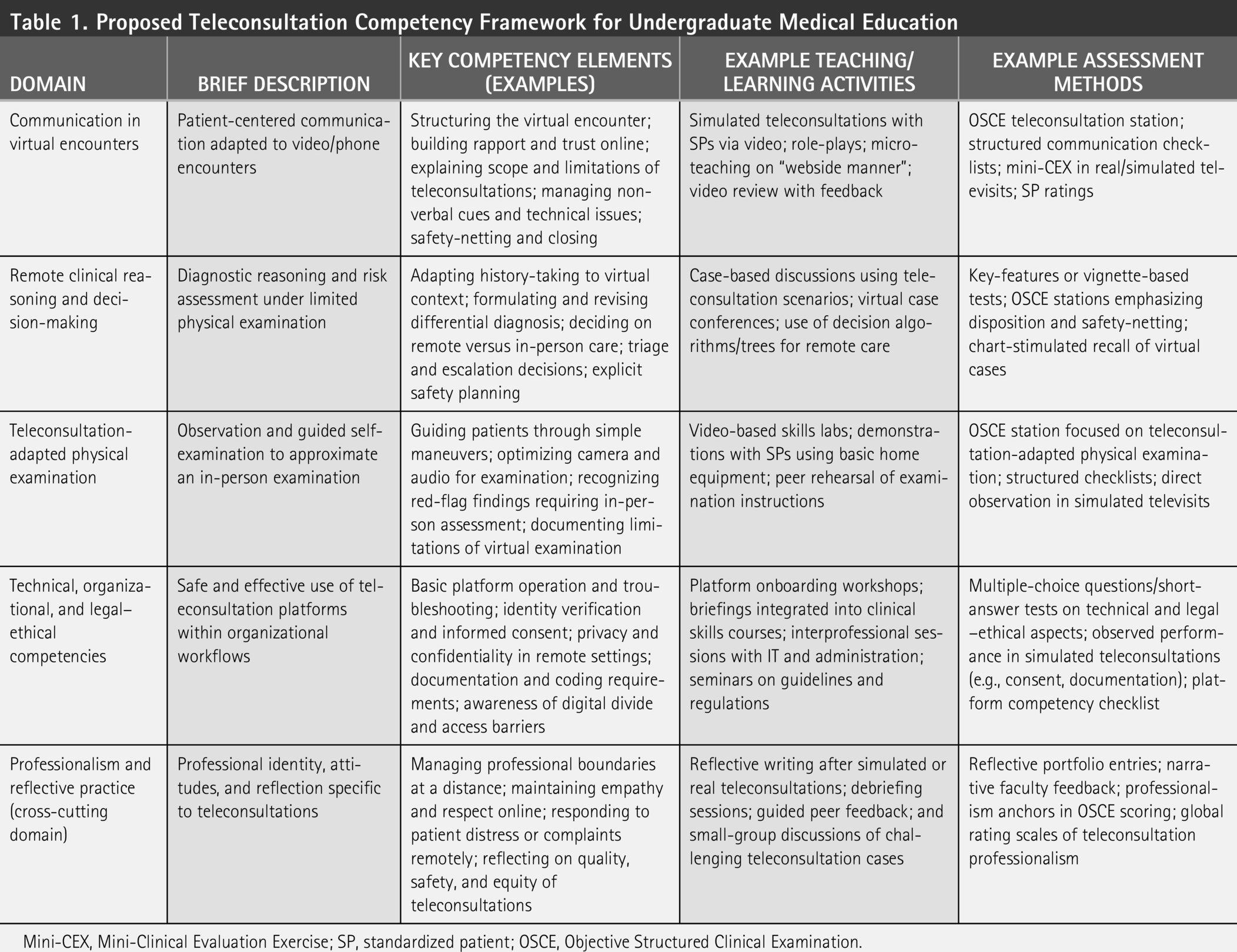
Mini-CEX, Mini-Clinical Evaluation Exercise; SP, standardized patient; OSCE, Objective Structured Clinical Examination.
EDUCATIONAL STRATEGIES AND TEACHING FORMATS
Although only one study met all the predefined eligibility criteria, the broader telemedicine education literature describes a wide range of educational strategies for introducing teleconsultation-related skills. Typical approaches include simulated teleconsultations, role-playing exercises, standardized patient encounters, and structured reflective activities. Some programs provided preparatory instructions followed by supervised practice, while others primarily relied on experiential learning during simulated or real-time teleconsultations. Teaching formats varied from synchronous, instructor-led sessions to asynchronous modules supplemented with feedback and self-reflection exercises. Despite this diversity, few studies have systematically aligned learning objectives, instructional design, and assessment methods.
ASSESSMENT OF LEARNING OUTCOMES
Assessment strategies in the broader telemedicine education literature remain highly heterogeneous and predominantly descriptive. The most reported outcomes were self-reported measures such as learner satisfaction, perceived confidence, and subjective competence. Although these measures provide insight into learners’ experiences, they offer limited information about actual outcomes or skills acquired. In some studies, typically during simulated consultations, observational assessments using checklists or rating scales were employed to evaluate the participants. However, the assessment tools varied greatly, and few were validated or explicitly linked to established competency frameworks in the literature.
A detailed overview of the assessment approaches identified across studies contributing to the broader interpretive synthesis is provided in Supplementary Table S2. Behavioral or outcome-based assessments, including objective evaluations of consultation structure, communication quality, and clinical decision-making, are relatively rare in the literature. This limits the comparability of the study results and makes it difficult to interpret the program’s educational effectiveness.
Overall, the reviewed literature demonstrates substantial heterogeneity in educational approaches, target competencies, and assessment methods. The limited availability of studies that explicitly conceptualize teleconsultation as a distinct clinical competency suggests important educational and conceptual gaps, which are explored further below.
EVIDENCE GAP ANALYSIS
The study identification and selection process revealed a substantial mismatch between the widespread implementation of teleconsultation in clinical practice and the available evidence regarding its structured teaching in undergraduate medical education. Beyond the scarcity of eligible studies, several recurring gaps were identified in the broader telemedicine education literature.
Gap 1. Lack of a clear definition of teleconsultation competency
Most educational publications have described telemedicine as a mode of care delivery or an educational environment rather than a distinct clinical competency. Consequently, teleconsultation-related learning objectives are often embedded in broader digital health or telehealth curricula without explicit definitions of competencies. This lack of conceptual clarity hinders curriculum development, competency mapping, and educational evaluation.
Gap 2. Lack of validated assessment tools
Assessment approaches were highly heterogeneous and frequently relied on learner self-reports, perceived confidence, and satisfaction measures. Few studies have employed validated instruments specifically designed to assess teleconsultation competencies, and no widely accepted assessment framework has been identified. The absence of standardized tools limits the comparability of educational interventions and impedes evidence-based curriculum development.
Gap 3. Lack of competency-based curricular frameworks
Teleconsultation training is most often reported as isolated workshops, pilot courses, or single educational interventions. Few publications have described explicit competency-based curricular frameworks that define learning objectives, expected progression of skills, assessment milestones, and integration across different stages of undergraduate medical education. Consequently, teleconsultation competencies are rarely embedded within longitudinal curricula that allow students to progressively develop and refine their skills over time. This limits the understanding of the optimal sequencing, timing, and educational pathways needed to acquire teleconsultation competencies and hinders systematic curriculum development.
Gap 4. Lack of structured frameworks for remote physical examination
Although some educational interventions have introduced elements of virtual examination, remote physical examination has rarely been conceptualized as a distinct competency domain with clearly defined learning objectives, instructional methods, and assessment strategies. This gap is particularly relevant in specialties where visual, functional, or movement-based assessments are important components of clinical decision-making. This limitation is particularly important because remote physical examination often represents the key distinction between communication-focused telemedicine training and preparation for independent teleconsultation practice.
Gap 5. Lack of outcome-based educational research
Most studies focused on educational feasibility, learner perceptions, or immediate postintervention outcomes. However, evidence demonstrating objective improvements in teleconsultation performance, skill transfer to clinical practice, or effects on patient-related outcomes remains scarce. Consequently, the educational effectiveness of existing approaches cannot be determined with confidence.
Overall, these findings suggest that the principal challenge in teleconsultation education is not the absence of educational activity but rather the absence of a coherent competency-based educational framework supported by robust evaluation methodologies.
Discussion
The principal finding of this review is not the effectiveness of a specific educational intervention but the identification of multiple evidence gaps that currently limit the development, implementation, and evaluation of teleconsultation training in undergraduate medical education.
The identification of a single study that meets all predefined eligibility criteria should not be interpreted as a failure of the search strategies. Rather, it reflects the conceptual distinction adopted in this review between telemedicine-related educational exposure and explicit teleconsultation competency training. Many educational initiatives incorporate telemedicine into undergraduate education; however, most focus on communication skills, technology use, learner attitudes, or general telehealth exposure rather than conceptualizing teleconsultation as a comprehensive clinical competency with explicit learning objectives and measurable educational outcomes.28,33,34,40,41
Although a substantial body of literature on telemedicine education exists, much of it focuses on learner attitudes, communication skills, virtual professionalism, technology use, and general exposure to telemedicine. A central finding of this review is that relatively few studies conceptualized teleconsultation as a comprehensive clinical competency that encompasses the full process of remote patient care. Consequently, the apparent abundance of telemedicine education studies may overestimate the extent to which undergraduate curricula prepare students to independently deliver telemedical care in the future.
The proposed teleconsultation competency framework ( Table 1 ) translates largely implicit expectations surrounding teleconsultation practice into explicit, teachable, and assessable competency domains for undergraduate medical education curricula.
Unlike broader telehealth competency frameworks, which frequently encompass digital systems, health informatics, legal issues, and population-level digital health concepts, the framework proposed in this review focuses specifically on the competencies required during remote clinical encounters. A complete teleconsultation requires the integration of history-taking, remote physical examination, clinical reasoning, risk assessment, management planning, and decisions regarding the need for in-person evaluation.39–42 However, the literature reviewed suggests that communication-focused training is considerably more common than educational approaches that address the full scope of teleconsultation practice. This discrepancy is particularly relevant for specialties in which remote physical examinations contribute substantially to diagnostic decision-making, including musculoskeletal medicine, rehabilitation, neurology, dermatology, and primary care.
Teleconsultation is not simply communication through a digital platform; it is the remote execution of a clinical consultation, encompassing patient assessment, clinical reasoning, risk stratification, management planning, and decisions regarding the need for in-person evaluation.39,40,42 Consequently, teleconsultation should be regarded as an extension of clinical competence rather than merely a digital communication skill.39,42
Notably, the eligible studies incorporated communication, history-taking, clinical reasoning, and remote physical examination within a single educational intervention, illustrating the multidimensional nature of teleconsultation competency. Despite the growing adoption of teleconsultation in clinical practice, undergraduate curricula remain heterogeneous in terms of the competencies taught, educational strategies employed, and assessment approaches used.42–46 Educational activities have focused on competencies aligned with remote consultations,15,16,37,38,47,48 particularly verbal communication, structured history-taking, and clinical reasoning articulation.49–53 These skills benefit from the dialogic nature of teleconsultations, in which physicians rely on verbal interactions without direct physical examinations.18,37,44,54,55
From an educational perspective, teleconsultation should not be viewed as a replacement for conventional clinical examination. Rather, it represents an advanced competency requiring learners to adapt previously acquired history-taking, physical examination, and clinical reasoning skills to a remote setting. Teaching teleconsultation before students have achieved basic proficiency in direct patient assessment risks reducing telemedicine education to communication training or platform familiarization while overlooking the broader clinical competencies required for safe and effective telemedical care.
This may partly explain why many published telemedicine curricula implemented during preclerkship training emphasize communication and technology use, whereas competencies requiring prior clinical experience, such as remote physical examination and teleconsultation-based clinical decision-making, remain less developed.
Teleconsultation training appears to be most meaningful when learners have already acquired foundational competencies in patient assessment, physical examination, and clinical reasoning.33,34,56 In this context, teleconsultation functions as an extension of existing clinical competence, rather than as a substitute for conventional clinical training. This perspective may also help explain the predominance of communication-focused educational interventions in the literature, as more advanced competencies related to remote examination and teleconsultation-based decision-making require prior clinical experience and are therefore more difficult to integrate into early undergraduate curricula.
In contrast, competencies related to nonverbal communication, empathy, and the relational aspects of care have been addressed less consistently and often implicitly in the literature.15,57–59 The limited availability of body signals, shared physical contexts, and opportunities for spontaneous human interaction pose challenges in teaching and assessing these skills in remote settings.15,16,57 This imbalance raises concerns that an overreliance on teleconsultation-based teaching may not adequately prepare students for the full interpersonal demands of clinical practice unless supplemented by in-person educational experiences.34,60,61
An important and closely related gap identified in this review concerns the teaching of physical examination skills adapted for remote consultations.33,47,56,62 Although a few studies have included elements such as verbal cues, visual inspection, or patient-assisted activities, remote physical examination has rarely been considered a distinct competency with clearly defined teaching objectives or assessment strategies. This limitation is particularly relevant in specialties such as orthopedics, neurology, pediatrics, and rehabilitation medicine, where structured visual and functional assessments play key roles in clinical decision-making.63–66 The lack of systematic educational approaches in this area suggests the need for clearer curriculum frameworks that explicitly include remote physical examination skills as an integral part of teleconsultation training.33,34,47,56
The assessment practices used in various studies further limit the interpretability of the educational outcomes. Most studies relied primarily on self-assessment, including student satisfaction and perceived confidence levels.33,34,41,56
Although these results provide valuable information about students’ experiences, they offer limited evidence of actual skill acquisition or transfer to clinical practice.34,56 Observation- and outcome-based assessments were used less frequently and were not standardized, reducing comparability across studies and hindering evidence-based curriculum development. 56
From the perspective of curricula, this review suggests that teleconsultation training should not replace traditional face-to-face consultations.67–69 Rather, it serves as a complementary method to support teaching objectives, particularly for structured communication and cognitive processes.34,60,70 Relational competencies and physical examination skills require special attention and cannot be adequately developed through teleconsultation teaching alone.34,42,54,71–73 The review findings should be interpreted with consideration of the limitations of the narrative synthesis. Although the heterogeneity of the research designs precludes formal comparisons of effectiveness, this review provides a structured overview. It identifies priority areas for future research, including competency frameworks, assessment strategies, and remote physical examination training methods to address these challenges.
If teleconsultation is regarded as a distinct clinical competency rather than simply a mode of digital communication, it has important implications for curriculum design. Teaching teleconsultation requires the structured development of competencies in patient assessment, remote examination, clinical reasoning, and clinical decision-making. These considerations form the basis of the recommendations presented below.
RECOMMENDATIONS FOR UNDERGRADUATE MEDICAL EDUCATION
The recommendations presented below were developed through a conceptual synthesis of the eligible studies, the broader telemedicine education literature, and the educational gaps identified during the review.
Define teleconsultation competencies
Undergraduate programs should clearly define competencies specific to teleconsultation, distinguishing them from those traditionally associated with in-person consultations. These competencies should include communication, clinical reasoning, organizational skills, and professional conduct in remote settings, while accounting for the specific requirements of physical separation and digital interactions.
Differentiate competencies according to educational relevance
Curriculum design should clearly distinguish between competencies that can be effectively introduced and practiced through teleconsultation-based teaching and those that require in-person or supervised clinical learning experiences. Verbal communication, structured history-taking, and explicit clinical reasoning are well suited to remote teaching. In contrast, nonverbal communication, empathic engagement, and physical examination skills, particularly those adapted for remote assessments, require thoughtful and complementary teaching strategies.
Recognize remote physical examination as a distinct competency domain
Remote physical examination should be conceptualized as a distinct competency within teleconsultation training, with clearly defined learning objectives and assessment strategies to ensure their effectiveness. The curriculum should include visual inspection, patient-directed activities, functional assessment, and camera-assisted examination as specific competencies, with clearly defined learning objectives, while acknowledging the limitations of virtual learning compared with in-person examinations.
Adapt assessment strategies to specific competencies
The assessment of teleconsultation competencies should extend beyond patient-reported outcomes to include structured, outcome-based assessment methods aligned with clearly defined learning objectives. The use of standard observation tools and competency-based assessment frameworks would enable more reliable assessment of student performance and facilitate the comparison of results across different educational settings.
Integrate teleconsultation training in a continuous manner
Teleconsultation competencies should be gradually introduced throughout undergraduate studies rather than being confined to isolated modules. Integration over time would allow students to revisit and refine their teleconsultation skills at increasingly complex levels and with greater clinical responsibility, thereby strengthening the alignment between the program’s educational goals and professional expectations.
Use teleconsultation as a complementary educational modality
Teleconsultation-based teaching should be considered a complementary element of medical education rather than a standalone substitute for traditional consultation-based teaching. Effective teaching programs should balance remote and face-to-face educational experiences to ensure comprehensive development of technical and interpersonal clinical competencies.
Although the proposed framework is intended to be broadly applicable across undergraduate medical education programs, its implementation should be adapted to local regulatory requirements, technological infrastructure, curricular structures, and healthcare system characteristics.
Limitations
This review has some limitations. First, it was designed as a critical narrative review rather than a systematic review or meta-analysis; therefore, its purpose was conceptual synthesis and evidence gap identification rather than exhaustive evidence mapping or quantitative evaluation of intervention effectiveness. Second, the eligibility criteria were intentionally restrictive, requiring studies to conceptualize teleconsultation as a distinct undergraduate clinical competency, describe an educational intervention, and report empirical outcomes. Only one study met all the predefined inclusion criteria. This limits the ability to draw conclusions regarding the comparative effectiveness of specific teaching methods.
Third, no formal risk-of-bias assessment was performed. This decision was consistent with the narrative and interpretive nature of the review and the very small number of eligible studies, but it limited the methodological appraisal of the available evidence. Fourth, the proposed competency framework was not developed through a formal Delphi process, a consensus workshop, or an external validation procedure. Therefore, it should be interpreted as a preliminary, hypothesis-generating framework that requires further refinement, validation, and testing in different undergraduate medical education contexts. Finally, because teleconsultation practices, regulatory requirements, digital infrastructure, and curricular structures vary across healthcare systems, implementing the proposed recommendations will require adaptation to local academic and clinical settings.
Conclusions
The principal finding of this review is not the identification of effective educational interventions but the recognition that teleconsultation remains insufficiently conceptualized as a distinct undergraduate clinical competency. Although telemedicine-related educational activities have been increasingly reported, many focus primarily on communication, technology use, or learner perceptions rather than on the full set of competencies required to safely deliver telemedical care.
This narrative review demonstrates that empirical evidence regarding the teaching of teleconsultation competencies in undergraduate medical education is limited. Although teleconsultation is becoming increasingly embedded in routine clinical practice, it is rarely addressed as a distinct competency with clearly defined learning objectives or assessment strategies at the undergraduate level of medical education.
These findings highlight the need for educational frameworks that explicitly define teleconsultation competencies, including communication in virtual encounters, clinical reasoning at a distance, technical aspects of teleconsultation, and structured approaches to remote physical examinations. Future research should focus on developing and evaluating such frameworks to align undergraduate medical education with contemporary healthcare models.
The principal challenge identified in this review is therefore not the absence of telemedicine education but the absence of coherent competency-based frameworks to prepare students for independent teleconsultation practice.
Authors’ Contributions
W.M.G.: Conceptualization, supervision, data curation, formal analysis, investigation, methodology, project administration, writing—original draft, and writing—review and editing. R.D. and T.C.: Investigation and writing—original draft. B.M.: Data curation and writing—review and editing. A.K.J.: Methodology, formal analysis, and writing—review and editing. A.Ś.: Formal analysis, visualization, supervision (supporting), and writing—review and editing.
Footnotes
Ethics Approval and Consent to Participate
This study was a narrative review of the published literature and did not involve human participants, human data, or identifiable personal information.
Acknowledgments
During the preparation of this article, the authors used ChatGPT (OpenAI, GPT-5 series) for language refinement, stylistic editing, and organizational support. Grammarly was used for grammar and language checking, and Paperpal was used for the final article journal submission check. All scientific content and final editorial decisions remained under the authors’ control. All scientific interpretation, literature analysis, classification development, and final article decisions were performed exclusively by the authors.
Data Availability
All data generated or analyzed in this study are included in this published article.
Disclosure Statement
The authors declare that they have no affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this article.
Funding Information
The authors did not receive any specific funding for this study. Funding was not provided for this study by the individual researchers.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.