
Abstract
Background:
Telemedicine adoption in gastroenterology has accelerated rapidly in recent years. Virtual interventions offer disease activity control comparable to standard in-person care. However, factors determining patient satisfaction and personal perceptions of virtual clinics remain poorly explored. This study identifies the clinical, demographic, and socioeconomic predictors of clinic format preference among patients with inflammatory bowel disease.
Methods:
We conducted a cross-sectional observational study at King Fahad Medical City in Riyadh, Saudi Arabia. The study included adult patients diagnosed with Crohn’s disease or ulcerative colitis. Authors collected demographic parameters, clinical covariates, and patient experience ratings using a structured questionnaire. A multivariable binary logistic regression model was employed to isolate independent predictors of virtual clinic preference.
Results:
The cohort comprised 1,005 patients. Overall, 55.6% preferred in-person appointments and 44.4% preferred virtual clinics. Prior telehealth exposure served as the strongest predictor for future virtual care (odds ratio [OR] = 4.10; 95% confidence interval [CI]: 2.90, 5.82). Patients utilizing subcutaneous injections (OR = 2.02) or oral medications (OR = 1.81) demonstrated significantly higher odds of selecting virtual care. Conversely, an ulcerative colitis diagnosis predicted a preference for physical visits (OR = 0.63). Prioritizing ease of access (OR = 1.47) and the use of technology (OR = 2.14) underpinned virtual choices. Strict privacy concerns (OR = 0.57) and inadequate physician communication (OR = 0.05) deterred patients from the remote clinic.
Conclusion:
Prior telehealth experience and the use of home-based therapies drive virtual clinic adoption. Disease phenotype, reliance on intravenous treatments, and privacy concerns may necessitate accessible in-person care. Health care systems must abandon uniform digital strategies and implement tailored, hybrid care models to optimize resource allocation.
Keywords
Introduction
The adoption of telemedicine within gastroenterology accelerated rapidly as a direct consequence of the COVID-19 pandemic, transitioning from a localized necessity to a rapidly advancing field of virtual care.1–4 Clinical efficacy data demonstrate that telemedicine interventions for patients with inflammatory bowel disease (IBD) yield disease activity control and clinical remission rates comparable to those achieved through standard in-person care. 5 Moreover, digital health interventions have been shown to significantly reduce overall health care utilization by decreasing the rate of outpatient office visits and, in some studies, lowering the rates of IBD-related hospitalizations and health care costs.6,7 Patient acceptance and satisfaction rates for virtual IBD clinics are high and reflect a willingness to adopt digital health technologies in routine clinical practice. 8
Patients and providers report numerous benefits associated with virtual care driven by improved convenience, enhanced flexibility, and cost savings.7,9 Virtual clinics eliminate the need for travel, finding parking, taking time off work, and arranging childcare for individuals living in rural communities or distant from specialized centers. 9 Remote care also minimizes patient exposure to communicable pathogens and severe winter weather, providing reassurance to those on immunosuppressive therapies. 9 Providers note that telemedicine enables greater flexibility in scheduling, allowing for timely, impromptu check-ins that can resolve acute issues faster and improve work-life balance.9,10
Technical barriers such as delayed platform responses, variable audio or video connections, lack of stable internet, and low digital health literacy among certain patient demographics hinder effective virtual consultations.9,11 In addition, both patients and providers encounter challenges regarding privacy, as virtual care often lacks the guaranteed private physical space inherent to traditional clinical encounters. 12 Intravenous (IV) biologics also necessitate scheduled visits to an outpatient clinic or infusion center. 13 These infusions require direct supervision by medical staff, tying clinical workflows tightly to facility capacity and staffing availability. 13 In contrast, subcutaneous (SC) and oral therapies enable patients to self-administer treatment at home, significantly reducing dependence on hospital infrastructure and lowering drug delivery–related health care resource utilization. 14 Home administration saves patients considerable time and directly mitigates the risk of exposure to hospital-acquired pathogens.13,14 However, SC therapies introduce the need for extensive patient education to ensure correct self-injection practices and to manage compliance risks, including missed doses or improper storage. 14 Because the method of delivery dictates whether routine in-person evaluations are required, IV therapies, by mandating physical attendance, can paradoxically lead some patients to resist switching to SC formulations, as they value the direct clinician interaction and view infusion appointments as essential in-person assessments. 13
While previous studies have demonstrated high levels of patient satisfaction with virtual IBD clinics, few studies have explored the factors important in determining this satisfaction or examined patients’ personal perceptions of virtual clinics. 15 Extant literature suggests IBD phenotype, severity, age as disease-related determinants.9,11–15 Yet, the acceptance and applicability of digital health technologies in populations enshrined in negative social determinants of health constitutes an exigent knowledge gap.5–6 This study strives to address these gaps by identifying the demographic, clinical, and socioeconomic predictors of clinic format preference among patients with IBD. Furthermore, we evaluate how distinct motivating factors, such as privacy concerns and ease of access, drive patient preferences. By understanding these dynamics, we aim to provide insights for optimizing tailored care models in IBD management.
Methods
STUDY DESIGN AND SETTING
We conducted a cross-sectional observational study at the gastroenterology department of King Fahad Medical City (KFMC) in Riyadh, Saudi Arabia. KFMC is considered a tertiary referral governmental center and receiving referral from all other 12 administrative Saudi regions Fig. 1. Data collection occurred between April 1, 2025, and December 31, 2025. We structured this article in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 16
Map of Saudi Arabia showing the study location in Riyadh. Adapted from a vector image obtained from Vecteezy.
CONTENT VALIDITY
To evaluate content validity, 6 experts rated questionnaire items on a 4-point scale, resulting in Item-Level Content Validity Indices ranging from 0.75 to 1.00. Scale-level analyses revealed an Average Method score (S-CVI/Ave) of 0.909 and a Universal Agreement score (S-CVI/UA) of 0.545. Ultimately, these findings demonstrate strong overall content validity for the instrument, while identifying specific items that may require further refinement to achieve complete expert consensus.
STUDY PARTICIPANTS
The study population comprised patients receiving medical care for IBD. Eligible participants included adults aged 14 years or older with a confirmed diagnosis of either Crohn’s disease or ulcerative colitis. Participants were required to have attended at least one virtual or in-person clinic appointment within the preceding year. We excluded patients younger than 14 years and individuals exhibiting cognitive impairments or language barriers that prevented independent survey completion. We employed systematic random sampling from electronic clinic records to recruit subjects to ensure a proportional representation of patients using both in-person and virtual care models. Our virtual care group encompassed participants who received care through telephone, video, or the department’s health portal.
SAMPLE SIZE
We calculated a minimum target sample size of 384 participants. This estimation utilized a 95% confidence level, a 5% margin of error, and an assumed response variability of 50%.
VARIABLES, MEASUREMENTS, AND DATA COLLECTION
We collected primary data using a structured questionnaire via telephone and internet. The primary outcome was the patient’s preferred clinic type for future appointments, defined as a binary choice between virtual and in-person care. We extracted demographic covariates including age, sex, nationality, marital status, living situation, and region of residence. Socioeconomic indicators encompassed education level, employment status, and monthly income, thereafter, we calculated body mass index (BMI) systematically using self-reported weight and height. Clinical covariates included the IBD subtype, age at diagnosis, and total disease duration. We recorded medical histories detailing prior IBD-related surgeries, hospitalization frequencies, current treatment administration methods, and comorbid chronic diseases. We also evaluated patient experience through scaled ratings of appointment waiting times, clinic accessibility, physician communication adequacy, and overall service quality. We then gauged factors influencing the choice of care model, including privacy concerns, location proximity, and technology utilization.
STATISTICAL ANALYSIS
We executed all data preprocessing and statistical analyses using R v4.4.1. We summarized continuous variables using means and standard deviations or medians and interquartile ranges, dictated by the normality of the data distribution. We presented categorical variables as absolute frequencies and percentages. We conducted bivariate analyses to compare baseline characteristics across the future clinic preference cohorts and applied the Wilcoxon rank-sum test to evaluate continuous variables. We employed Pearson’s chi-squared test or Fisher’s exact test to assess categorical variables and subsequently constructed a multivariate binary logistic regression model to isolate independent predictors of virtual clinic preference. We deployed a bidirectional stepwise selection algorithm to optimize model fit. Regression estimates were presented as adjusted odds ratios (OR) with 95% confidence intervals (CI). Statistical significance was established at a predefined alpha level of p < 0.05.
Results
PARTICIPANTS AND DESCRIPTIVE DATA
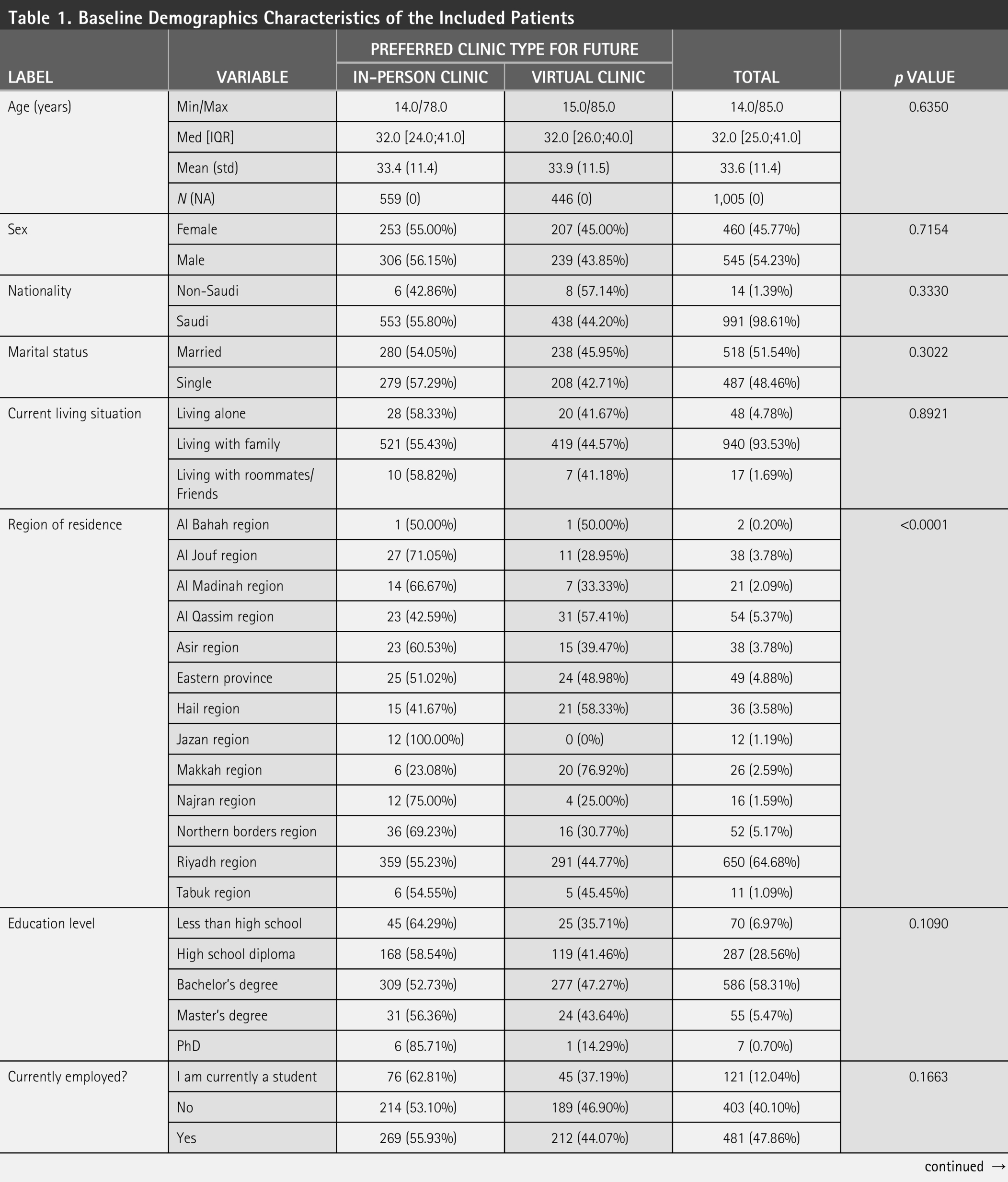
The study included 1,005 patients diagnosed with IBD. A total of 559 patients (55.6%) preferred in-person clinics for future appointments, whereas 446 patients (44.4%) preferred virtual clinics. The median age of the overall cohort was 32.0 years (interquartile range: 25.0–41.0). Males constituted 54.2% of the sample. Most participants were Saudi nationals (98.6%) and held a bachelor’s degree (58.3%). Almost half of the cohort earned a monthly income of less than 5,000 SAR (45.7%). Patient demographics showed no significant associations with future clinic preferences Table 1 .
Baseline Demographics Characteristics of the Included Patients
CLINICAL CHARACTERISTICS
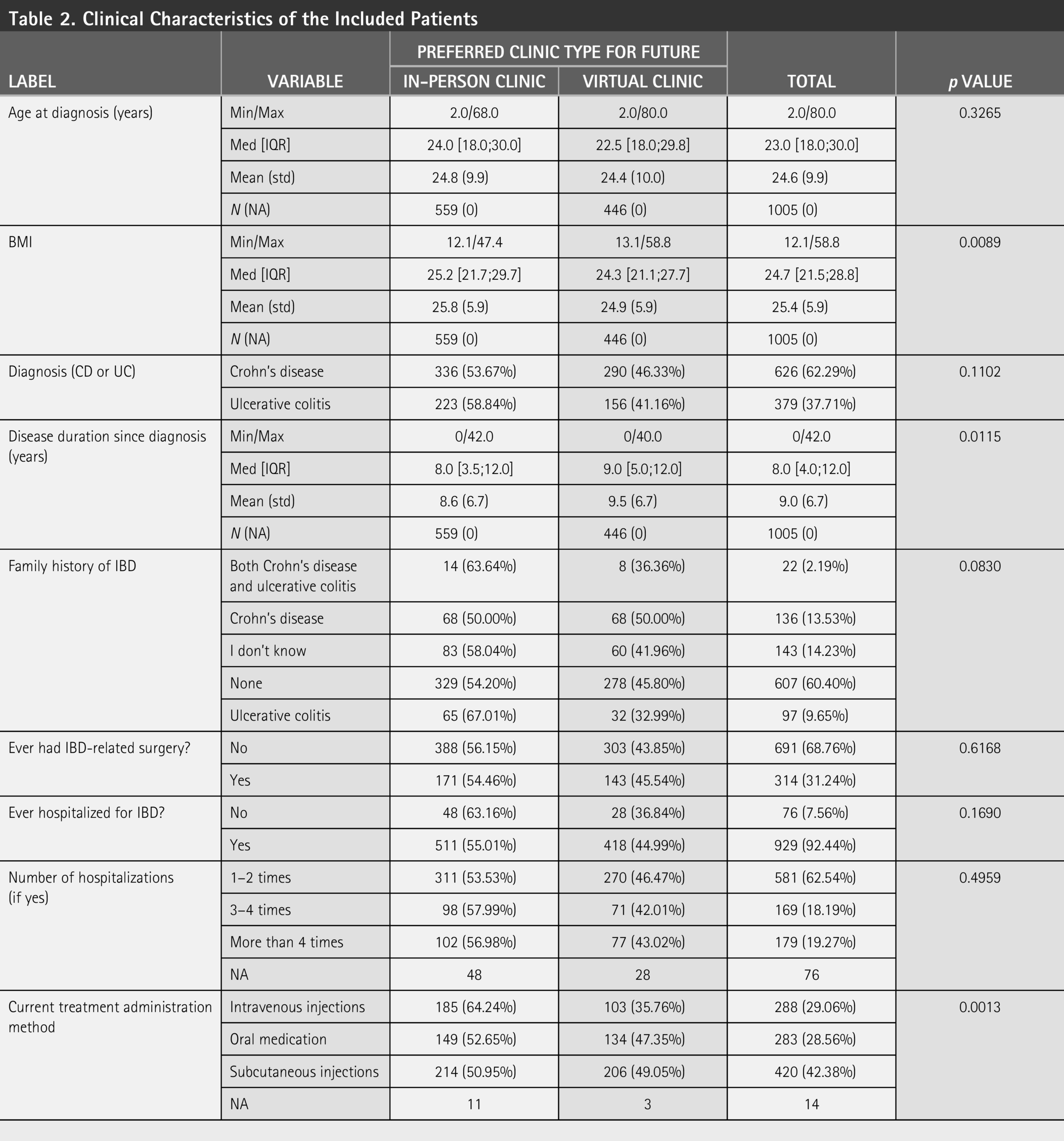
Crohn’s disease was the primary diagnosis for 62.3% of the participants, and ulcerative colitis accounted for the remaining 37.7%. Patients preferring virtual clinics had a lower median BMI (24.3 kg/m2) compared with those preferring in-person clinics (25.2 kg/m2) (p < 0.05). The virtual preference group also exhibited a slightly longer median disease duration (9.0 years) than the in-person group (8.0 years) (p = 0.012). Current treatment administration methods differed significantly between the two groups (p = 0.001), as patients receiving IV injections predominantly favored in-person care (64.2%). Other clinical features are presented in Table 2 .
Clinical Characteristics of the Included Patients
CLINIC USE AND SATISFACTION FACTORS
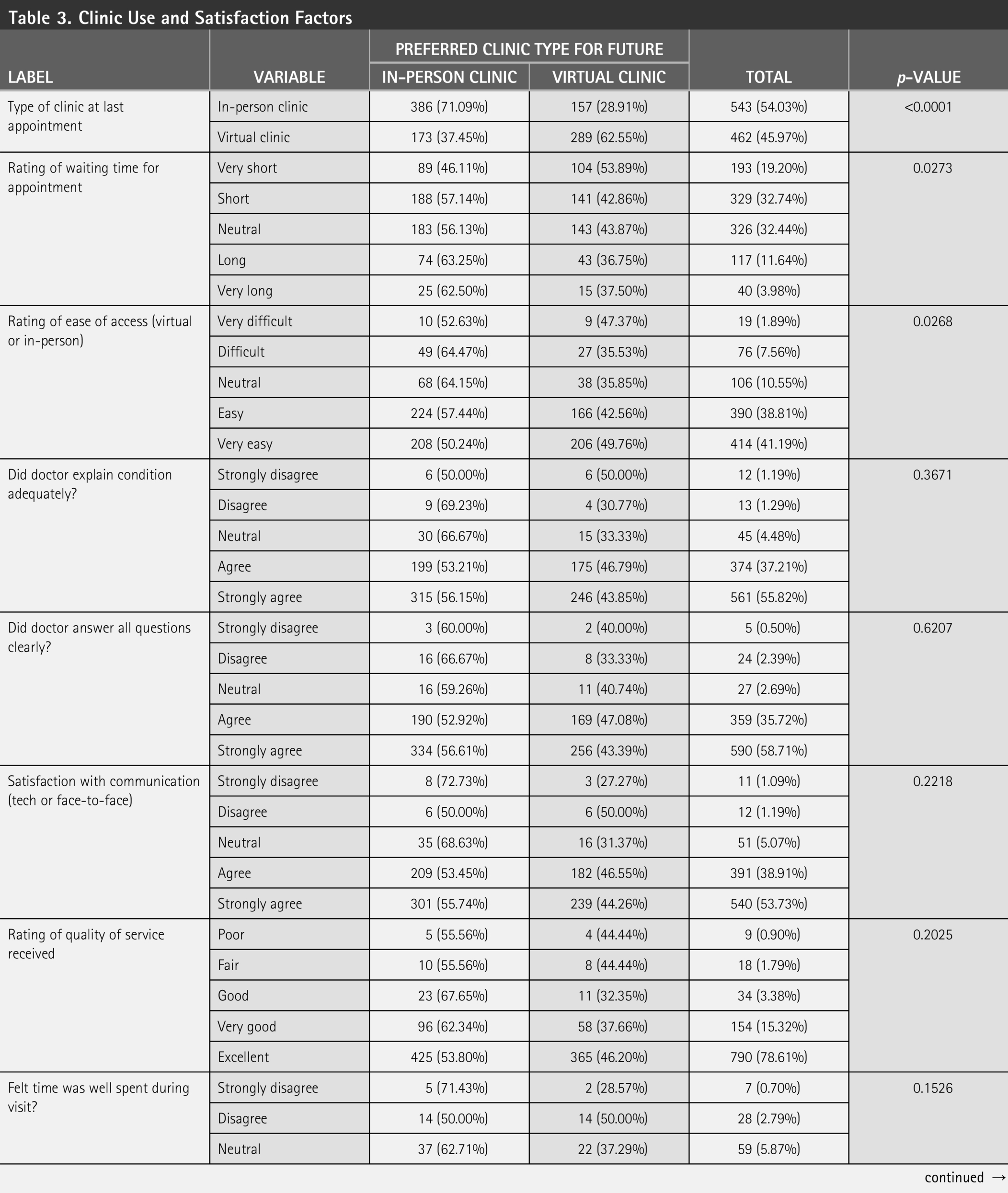
Prior clinic experience was significantly associated with future preferences (p < 0.0001); most patients who attended an in-person clinic for their last appointment preferred to continue in-person care (71.1%). Conversely, patients who attended a virtual clinic preferred to continue virtual care (62.6%). Fifty-three percent of patients who experienced “very short” waiting times favored virtual clinics, while 62.5% of those rating it as “very long” had predilection toward in-person clinics (p = 0.027). Self-reported ease of clinic access also showed a significant bivariate association with future preferences (p = 0.027). Patients who prioritized “ease of access” (p < 0.001) and the “use of technology” (p = 0.001) chose virtual care more frequently. All satisfaction factors and related clinical patterns are summarized in Table 3 .
Clinic Use and Satisfaction Factors
PREDICTORS OF CLINIC PREFERENCE
We fitted a multivariable logistic regression model to identify independent predictors of virtual clinic preference. Table 4 details the adjusted OR and 95% CI. Clinical factors significantly predicted patient choices. Patients diagnosed with ulcerative colitis had lower odds of preferring virtual clinics compared with patients with Crohn’s disease (OR = 0.63; 95% CI: 0.43, 0.90). Higher BMI negatively predicted virtual clinic preference (OR = 0.97; 95% CI: 0.94, 1.00). Treatment modality determined clinic preference; patients using SC injections showed twice the odds of selecting virtual care compared with those receiving IV injections (OR = 2.02; 95% CI: 1.36, 3.01). Patients taking oral medications also exhibited a higher likelihood of preferring virtual care (OR = 1.81; 95% CI: 1.15, 2.87).
Predictors of Clinic Preference
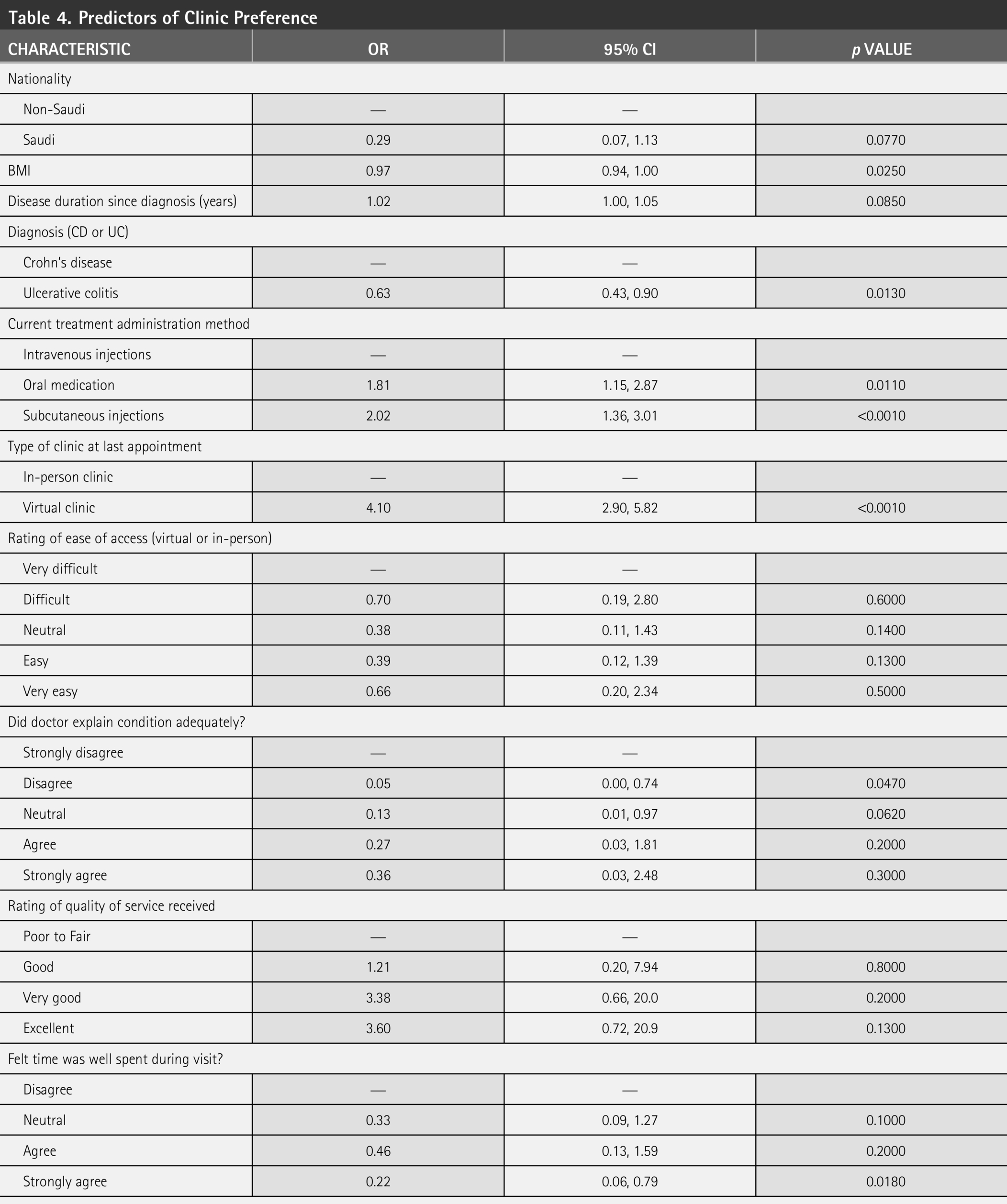
OR represents the odds of choosing Virtual versus In-person clinic.
CI, confidence interval; OR, odds ratio.
Prior clinic exposure was the most predictive factor in our model, as patients who attended a virtual clinic for their last appointment were four times more likely to prefer virtual clinics in the future (OR = 4.10; 95% CI: 2.90, 5.82). Moreover, prioritizing ease of access increased the odds of choosing virtual care (OR = 1.47; 95% CI: 1.00, 2.14), and prioritizing the use of technology similarly increased these odds (OR = 2.14; 95% CI: 1.34, 3.47). In contrast, prioritizing privacy significantly reduced the odds of selecting a virtual clinic (OR = 0.57; 95% CI: 0.33, 0.94). Disagreement with the adequacy of the doctor’s explanation also strongly reduced the likelihood of choosing a virtual clinic (OR = 0.05; 95% CI: 0.00, 0.74).
Discussion
Our analysis revealed that prior clinic experience was the strongest independent predictor in the model, with patients who attended a virtual clinic for their last appointment being four times more likely to prefer a virtual clinic in the future (OR = 4.10), aligning with the concept of exposure effect in digital health adoption. 17 Adwi et al. observed that previous use of online telepsychiatry was the absolute strongest predictor for choosing online services (OR = 28.90), whereas a history of previous in-person visits strongly predicted a preference for face-to-face care (OR = 0.11). This psychological pattern dictates that individuals develop a distinct preference or bias toward familiar health care delivery options as a result of increased comfort, perceived safety, and a reduction in the cognitive effort required to navigate the clinical encounter. 17
Chen et al. stated that past experience with digital health technologies acts as a critical moderating factor that makes patients significantly more likely to translate their willingness to use virtual care into actual usage behavior (β = −0.452, p < 0.001). 18 Likewise, Richter et al. found that prior therapeutic experiences also shape patient preferences toward known and familiar modalities, helping to overcome initial resistance to digital health interventions. 13
Conversely, patients who lack prior experience with remote care often exhibit lower adoption rates and a preference for face-to-face visits, a phenomenon attributed to technological unfamiliarity, heightened technology-related anxiety, and persistent concerns regarding information privacy and security.12,17,18 Therefore, as patients gain practical exposure to virtual clinics, their initial privacy and security apprehensions are mitigated, fostering the necessary trust and familiarity that drives the sustained preference for telemedicine observed in our cohort. 17
The route of therapeutic administration significantly influenced a patient’s decision on telehealth in our multivariate model. IV biological therapies inherently demand fixed logistical commitments, including scheduled travel to an infusion center, parking expenses, lost work hours, and reliance on clinical staff for drug delivery.13,14 In contrast, SC and oral therapies afford patients the flexibility of at-home self-administration, which mitigates the necessity for routine facility visits, reduces the risk of exposure to hospital-acquired infections, and minimizes drug delivery-related health care resource use. 14 Since IV therapies mandate in-person attendance, many patients rely on the infusion appointment itself as their primary clinical evaluation and resist transitioning to SC therapies in favor of regular face-to-face interactions with nurses and medical staff. 13
Corroborating this resistance, Richter et al. noted that 54.5% of patients actively undergoing IV treatment declined to switch to SC administration; within this resistant cohort, 57.7% cited the reassuring presence of medical staff during treatment as their primary justification, and 31.9% expressed a specific desire to see a physician after each infusion. 13 Our finding that patients utilizing SC injections (OR = 2.02) and oral medications (OR = 1.81) have almost twice the odds of preferring virtual care compared with IV users reflects this paradigm, as patients on at-home therapies are already decoupled from facility-based care workflows.
Patients with ulcerative colitis showed significantly lower odds of preferring virtual care (OR = 0.63) compared with those with Crohn’s disease. Ulcerative colitis is a nontransmural inflammatory disease restricted to the colon that presents with distressing symptoms, such as hematochezia and the passage of blood and mucus per rectum, which are rare in Crohn’s disease. 19 On the other side, patients with Crohn’s disease more experience abdominal pain or nonspecific abdominal symptoms rather than bloody diarrhea. 19 Because ulcerative colitis patients regularly experience alarming symptoms like urgency and visible bleeding, their comprehensive clinical evaluation stipulates hands-on physical assessments, including digital rectal examinations and inspection of the perineum. 19 Troch et al. unveiled that up to 69.8% of patients consider the lack of a physical examination to be a primary disadvantage of telemedicine. 8 Telemedicine restricts the ability of health care providers to perform these comprehensive visual and physical assessments, which challenges the delivery of optimal care for individuals who prefer or require direct physical evaluation. 9
Furthermore, clinicians acknowledge regularly asking about pain in Crohn’s disease due to its transmural nature and potential to excite the peritoneum, while overlooking pain assessments in ulcerative colitis under the mistaken assumption that superficial mucosal inflammation is painless or solely linked to urgency. 20 Pain affects approximately 70% of IBD patients, persists for 5 or more years in 49% to 55% of individuals, and is reported as moderate to severe by up to 34% of patients even during endoscopically confirmed disease remission, yet a survey revealed that 29% of patients report never being asked about their pain during consultations. 20 This potential for remote symptom invalidation, paired with the inability to conduct physical examinations during virtual visits, may drive the ulcerative colitis patient’s reliance on traditional face-to-face clinical encounters.9,20
Our findings that prioritizing ease of access (OR = 1.47) and the use of technology (OR = 2.14) significantly promoted virtual care choices are consistent with studies emphasizing convenience, time savings, and scheduling flexibility as primary motivators for digital health adoption.9,17 In addition, Adwi et al. identified that the top reasons for choosing online therapy were ease and convenience (mean score 1.62) and saving time (mean score 1.60), while users of online services also reported significantly higher internet usability (mean 4.57) compared with offline users (mean 4.14). 17 Contrary to that, our observation that prioritizing privacy strongly reduced the likelihood of choosing virtual care (OR = 0.57) may stem from the concerns patients harbor regarding the security and confidentiality of remote consultations. 17
Unlike traditional in-person encounters, virtual care lacks a guaranteed private clinical space, exacerbating patient anxiety regarding the presence of family members or other eavesdroppers in their home environment. 12 For example, Andreadis et al. indicated that more than one-third of respondents consider a lack of privacy to be a larger barrier than technological challenges, a concern that disproportionately affects people of color, who are two to three times more likely than White individuals to express concerns about health information security and privacy. 12 Furthermore, patients may perceive interactions as less private if the provider conducts the visit from a home office with potential distractions, which detracts from the undivided attention expected during sensitive medical discussions. 12
Patient preferences for IBD clinic formats vary by treatment route, disease phenotype, prior telehealth exposure, and individual values regarding convenience and privacy. These variations require establishing a hybrid triage algorithm; clinicians should incorporate treatment complexity, disease activity, technological literacy, and patient preferences to assign appropriate care pathways.21,22 Health care systems must employ identified patient-specific predictors, such as treatment modality and specific IBD diagnosis, to optimize this triage process. Clinics should also implement dynamic reassignment protocols with predefined thresholds for escalation from virtual to in-person care based on clinical judgment and biomarker data.5,22 Because privacy concerns and communication quality strongly drive patients toward physical visits, maintaining accessible in-person pathways remains crucial to address digital health disparities.4,23 Furthermore, integrating robust e-health infrastructure and AI-assisted predictive analytics can enhance the precision of this pathway assignment.3,24,25 Engaging patients as active partners and providing mechanisms to request physical encounters will ultimately optimize resource allocation and patient satisfaction within a hybrid care model.7,26
The rapid expansion of telemedicine in our cohort aligns with the Saudi Vision 2030 Health Sector Transformation Program, which prioritizes digital innovation to improve health care access and deliver patient-centered services.27,28 Government-led platforms like Sehhaty and the Seha Virtual Hospital have already established a strong foundation for virtual care. 27 Our patients prioritized ease of access and technology, aligning with the Kingdom’s shift toward value-based health care.27,28 Nevertheless, privacy concerns and the digital divide remain significant barriers that policymakers must address to alleviate these security apprehensions.27,28 Strengthening data governance will ensure these telemedicine models achieve the Vision 2030 goal of equitable health care delivery.27,28
This study possesses several strengths, including a large sample size and the use of a validated questionnaire to comprehensively evaluate patient preferences. However, certain limitations exist. The cross-sectional design precludes the establishment of causal relationships, and the single-center setting may limit the generalizability of these findings to other populations. The reliance on self-reported data also introduces the potential for recall bias. Future research should leverage longitudinal designs to assess how clinic preferences evolve alongside disease progression. We also recommend multicenter studies to validate these predictors across diverse geographic and health care settings.
Conclusion
Patient preferences for IBD care models are variable. A preference for virtual clinics is strongly driven by prior telehealth experience, the use of SC or oral medications, and prioritizing ease of access and technology. Conversely, a diagnosis of ulcerative colitis and reliance on IV treatments predict a preference for in-person care. Strict privacy concerns and dissatisfaction with physician communication deter patients from virtual formats. Health care systems should abandon uniform digital health strategies and instead implement a tailored, hybrid care model that systematically incorporates these clinical and experiential predictors to optimize resource allocation and ensure equitable health care delivery.
Authors’ Contributions
A.A.: Conceptualization; review and supervision; S.A.: Data curation; review and editing; H.A.: Conceptualization and methodology; A.A.: Formal analysis; writing—review and editing; A.A.: Literature search and identification; H.A.: Data collection; A.A.: Data collection; B.A.: Data collection; B.A.: Data collection; H.K.: Data collection; R.A.: Data collection; A.A.: Data collection; T.A.: Data collection; A.B.: Conceptualization; writing—review and editing.
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
The study was conducted after obtaining approval from the Institutional Review Board at KFMC (IRB registration number: IRB00010471, Log Number:25-154). We obtained explicit informed consent from all subjects prior to participation and anonymized all collected data to guarantee patient confidentiality.
Footnotes
Author Disclosure Statement
Authors declare that they have no conflict or competing interests.
Funding Information
This study did not receive any funding.