
Abstract
Military efforts to limit ischemic time and reperfusion injury are being investigated with a focus on functional limb salvage as opposed to the more historic statistical salvage, since a dysfunctional limb may be a worse outcome than amputation. Translatable animal research, supported by reports from forward deployed surgeons in the field, is needed to improve care. Current studies have determined the threshold for meaningful recovery is less than 6 hours. Attempts at modeling vascular injury and ischemia reperfusion can be divided into 2 categories: chronic ischemia that mimics human age related disease and acute vascular injury that represents traumatic injury. A swine model to evaluate battlefield injuries and scenarios encountered in traumatic extremity vascular injury with a focus on functional limb salvage has been developed. Future endeavors should focus on understanding the factors that affect ischemic threshold as well as testing therapeutic and physical maneuvers to prolong this threshold.
Keywords
Introduction
The ischemic threshold of the extremity is a multifaceted concept. There are really many different thresholds that can be examined in multiple clinical scenarios. The muscles of the extremity, for instance, may tolerate severe ischemia without complete loss of function for a much longer period of time than it takes to render a nerve nonfunctional. However, mild ischemic muscle injury can result in complete loss of nerve function if significant swelling results from reperfusion and extremity compartment pressures become elevated. Additionally, the “threshold” for ischemia undoubtedly depends on the clinical setting in which it occurs. For example, one cannot accurately compare the ischemic times an extremity would tolerate if blending blunt trauma with severe musculoskeletal and vascular injuries, in situ arterial thrombosis from atherosclerosis, with a simple embolus to the femoral or popliteal artery.
The scope of this review will be restricted to ischemia and ischemia/reperfusion injury (I/R) in the setting of trauma. Specifically, animal models of I/R will be examined, focusing on large animal research. These data will be examined in the broader context of military vascular injury and trauma. Finally, the “ischemic threshold” of the extremity will be evaluated as it relates to the quality of limb function following restoration of flow and injury healing.
Relevance of Extremity Vascular Injury
Extremity vascular injury is a prevailing problem during current wartime efforts. 1 Historically, extremity injury has been a secondary concern, as thoracoabdominal penetrating injuries lead to early battlefield mortality. Patients would often succumb to these injuries long before the extremity was addressed. Currently, more soldiers are protected from severe torso injury, sustaining extremity trauma with time to intervention similar to routine stateside level I transport time. 2 With expedient evaluation of injury, immediate limb salvage rates are more than 90% in the short term, with more recent realistic reports of long-term outcomes approaching 80% limb salvage.2-7 Military efforts to limit ischemic time and reperfusion injury are currently under investigation with a new focus on functional limb salvage as opposed to the more historic statistical salvage often reported.
Advances in I/R knowledge extend beyond the battlefield to both local and regional hospitals. Trauma that occurs outside of metropolitan areas is often transferred to a higher level of care. Understanding how to mitigate ischemic consequences is important for the initial accepting hospital and the tertiary receiving facility. This problem is likely to increase in the future as national trauma numbers rise and facilities able to provide definitive vascular interventions decreases.8,9 Translatable animal research supported by reports from forward deployed surgeons in the field is needed to improve care provided in military and civilian centers.
With the pendulum of extremity injury swinging toward functional limb salvage as opposed to statistical limb salvage, it is important to reassess previous standards of care. One such dogma is the concept of ischemic threshold. Previous reports describe a 6-hour window during which extremity ischemia could be tolerated.10,11 The 6-hour window stemmed from initial research dating back to the 1940s and focused on the histological appearance of the muscle postischemia. 10 Current studies have focused on functional results and have determined that the threshold for meaningful recovery is less than 6 hours, and once breached, normal functional outcome is not obtainable.12,13 Additionally, ischemia in the context of hemorrhage, acidosis, hypotension, soft tissue loss, and venous injury all potentially affect this threshold and must be considered in the treatment plan. Emerging research focuses on further delineating a traumatic ischemic window for full functional recovery, taking all of the aspects of injury into consideration.
Past Ischemia Reperfusion Animal Studies
Attempts at modeling vascular injury and ischemia reperfusion can be divided into 2 categories. The first category includes models of chronic ischemia that mimics human age related disease. The second includes models of acute vascular injury that represent traumatic injury.
An initial murine model of ischemia was developed using rubber band ligation of the hind limb. 14 This model proved successful for inducing ischemia without open surgery and provided a reproducible platform for looking at the intricacies of ischemia and reperfusion injury.15-19 With this work, histologic grading scales that report damage to skeletal muscle following an ischemic insult were developed, potential treatments and maneuvers to mitigate the I/R injury were assessed, and systemic impact of regional I/R injury was evaluated. Additional small animal models have also been utilized to evaluate I/R injury and have contributed valuable information to help current and future investigators obtain knowledge in the subject.20-24
Given the inherent differences between humans and other species, mimicking human acquired disease is important to guide research protocols. Recently, the Apo E null mice have been used to create a model of demand ischemia that mimics human claudication. 25 Following femoral artery ligation, mice were subjected to treadmill testing in order to induce demand ischemia. This model was successful, as murine changes mirrored those seen in human claudication. In the future, this model can be expanded on for the evaluation of therapeutic maneuvers in the hope of finding better treatment for claudication.
Although murine models are useful, they are limited. Previous work has identified a lower ischemic threshold in mice than in canine species.26,27 Furthermore, the difference in mass between humans and mice has driven others to use larger animal models such as dogs or swine. The use of canines to study vascular injury and ischemic injury is minimally reported in the recent literature but remains of significant importance to earlier cardiovascular research. The use of swine continues to be the model of choice to study subjects ranging from traumatic vascular injury to limb transplant. 28
Despite the valuable information obtained from these studies and many others, limited research has focused on modern injury patterns in both the civilian and military environments. Specifically, neither have current treatment strategies been scrutinized in a rigorous scientific manner nor have clinically relevant injury patterns been assessed in the context of these new strategies. To fill this void, a new model of extremity injury needed to be developed.
Nonsurvival Swine Model
Dawson et al 29 developed a large animal model to test the feasibility of temporary shunt usage in porcine iliac arteries in 1996. They demonstrated that patency could be maintained for extended periods using commonly used carotid shunts. Using this model as a basis, Gifford et al 30 altered the porcine model to allow for a more comprehensive assessment of I/R injury, the impact of various ischemic times, the effect of concomitant venous and arterial injury, and to confirm overall safety and efficacy of temporary vascular shunts (TVS). 30 Using a nonsurvival animal model, iliac vessels were isolated, ligated for a predetermined period, and then released with reperfusion accomplished using temporary shunts (Figure 1).
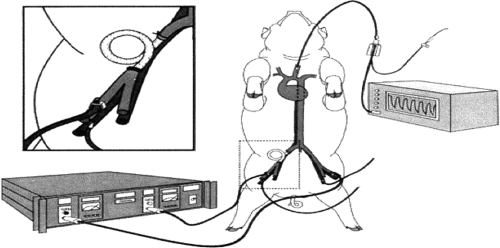
Experimental porcine design
The ischemic insult resulting from hind limb flow occlusion for 1, 3, or 6 hours was monitored for a period of time using common markers of tissue injury. Figure 2 demonstrates that increased tissue damage occurs in the setting of prolonged ischemia with a sharp increase after 3 hours of ischemia. Resultant arterial flow after reperfusion was inversely related to total ischemic time (Figure 3). Patency for all shunts was 90% in the absence of heparin, an important factor in the context of the severely injured patient with multiple injuries.
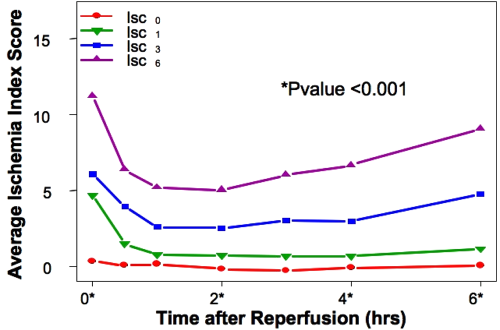
Ischemia index score over time: all groups
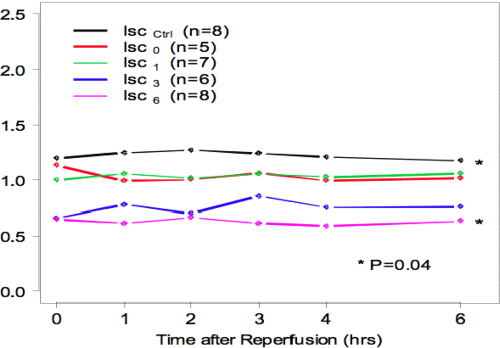
Flow rate proportions relative to baseline
The authors concluded that TVS use is safe in an animal model of extremity vascular injury and does not lead to increased tissue damage. In addition, early placement of TVS before the 3-hour time period in select cases is justified based on increased tissue damage with delayed placement.
Understanding that venous injury often occurs in conjunction with arterial injury, the above experiment was expanded to look at venous ligation and subsequent venous hypertension. 31 Treatment consisted of either continued venous ligation or reestablishment of outflow. Results from this set of experiments showed that venous ligation increased tissue injury, as measured by the previously established ischemia index score, and increased tissue edema on histologic analysis. Similarly, the authors concluded that venous repair should be performed when possible in the setting of concomitant arterial and venous injury.
Survival Swine Models
Early on in the evaluation of the aforementioned experiments, it was obvious that an assessment of functional outcome was necessary to accurately quantify and comment on the impact of extremity injury. Over the past decade, more focus has been placed on patient and quality based outcomes. Recognizing this deficit in the nonsurvival model, Burkhardt et al 13 identified functional measures that could be used to provide a qualitative assessment of outcome and extend beyond just the biochemical evaluation that previous investigators employed.
Using the porcine model as a basis, neuromuscular function via electromyographic assessment and gait analysis were evaluated over a 14-day survival period. Nerve function was combined with serology and histology analyses to create a physiologic measure of recovery. The concept of an ischemic threshold could now be examined with limb function as the outcome variable.
Employing ischemic intervals similar to the nonsurvival model, Burkhardt et al 12 were able to determine an ischemic threshold of 4.7 hours beyond which functional outcome was no better than that accomplished with ligation (Figure 4). The authors concluded that restoration of extremity perfusion early after extremity vascular injury would most likely provide a measurable outcome benefit compared with delayed restoration of flow or ligation. Furthermore, the ischemic threshold of the extremity after which neuromuscular recovery is significantly diminished is less than 5 hours, less than the generally accepted 6-hour time period.
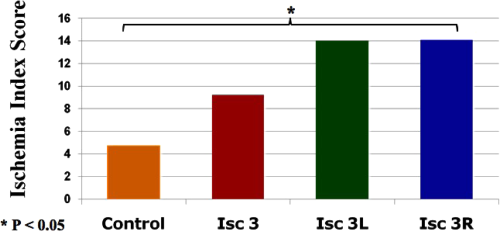
Estimation of the ischemic threshold
In an effort to more closely represent battlefield scenarios, Hancock et al 32 included blood loss into the assessment. Here, 35% hemorrhage was achieved at the simulated point of injury to mimic expected battlefield blood loss and induce class III shock prior to initial control. After hemorrhage and a period of hypotension, shed blood was returned to the animals simulating resuscitation. The same ischemic interval, repair, recovery, and functional evaluation were performed on each group. Overall, 35% hemorrhage associated with a period of hypotension in the context of ischemia led to a decrease in functional recovery in each group (Figure 5). This more realistic vascular injury model demonstrated that hemorrhage compounded the effect of ischemia and decreased the ischemic threshold of the extremity to less than 3 hours.
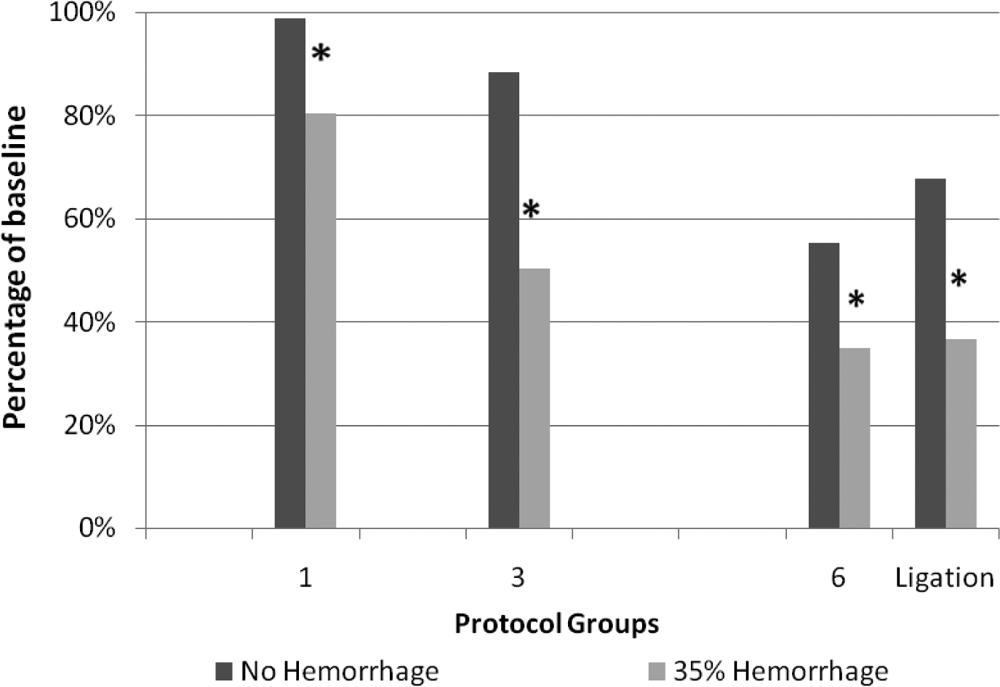
The percentage baseline of physiologic measure of recovery (PMR) at the 14-day endpoint between 35% hemorrhage and nonhemorrhage groups
The sequence of experiments outlined above has been used to define a more realistic and translatable model that can be employed to evaluate battlefield injuries and scenarios encountered in traumatic extremity vascular injury. They have provided a foundation on which further investigation can be done in hopes of improving quality outcome and limiting the impact of devastating extremity injury.
Future Directions
The swine model, published by Burkhardt et al, 12 was constructed to serve as a general template for inducing reproducible acute hind limb ischemia. Currently, the expanded model of Hancock et al 32 serves as the basic traumatic acute hind limb ischemia model. Both models focus on the ability to examine functional limb salvage as an endpoint, realizing that a dysfunctional limb may be a worse outcome than amputation. This concept has been well accepted as a more relevant endpoint during the current conflicts in Iraq and Afghanistan. The addition of different variables in conjunction with the ischemia model more closely reproduces civilian and combat traumatic injury and allows for better study of functional recovery.
Current and future endeavors are focused on understanding the factors that affect the ischemic threshold, and testing therapeutic and physical maneuvers that may prolong the ischemic threshold. Areas of consideration include
early fasciotomy as a maneuver to limit damage and allow for an extended ischemic window prior to repair,
use of ultrasound to clinically evaluate compartment syndrome and document compartment morphology over time,
use of isolated limb perfusion to limit reperfusion injury and enhance functional recovery,
limb cooling during ischemia to enhance functional recovery and limit ischemic injury,
use of free radical scavengers to limit ischemic damage, and
pharmacologic pretreatment of subjects to make tissues less susceptible to ischemic damage.
The future foci of this model aim to enhance the care of patients who experience acute traumatic injury, both abroad and stateside.
As mentioned earlier, the original swine model was primarily developed to study vascular injury in combat. Despite this initial focus, the model has the potential to be applied to the study other relevant clinical scenarios. There has yet to be a focus on bony trauma and recovery in the setting of ischemia; however, the effects of I/R on fracture recovery play a vital role in functional recovery. Additionally, the military has spent considerable resources in an attempt to provide reconstructive surgery to the extremity. This model could also be used to investigate nerve repair and plastic reconstruction following an ischemic insult.
Conclusion
Functional recovery following extremity trauma remains a focus point for current military research. Forward advancement in medical care has led to increased survival and more individuals with extremity injury. Increased focus on extremity injury has demanded a reevaluation of statistical limb salvage (ie, ambulation) alone as an endpoint. It is now realized that the mere presence of a limb is not a surrogate for functionality.
Current investigation and reports have only scratched the surface of meaningful limb salvage. For research in these areas to progress, the inclusion and cooperation of civilian centers needs to be fostered. These data will undoubtedly be useful throughout all facets of extremity care and ultimately serve patients to improve limb function.
Footnotes
The views and opinions expressed in this article are those of the authors and do not reflect the official policy or position of the US Air Force, US Army, US Navy, US Department of Defense, or the US Government.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.