
Abstract
Objective. To compare outcomes of abdominal aortic aneurysm repairs before and after the endovascular era. Methods. Group A (1997-1998) included 331 patients, 321 (97%) with open repair (OR) and 10 (3%) with endovascular aneurysm repair (EVAR). Group B (2007-2008) included 330 patients, 136 (41%) with OR and 194 (59%) with EVAR. Results. Patients in Group B were older (74 ± 8.5 vs 73 ± 7.0 years, P = .02), had higher comorbidity scores (8.3 ± 4.8 vs 7.5 ± 4.6, P = .04), shorter hospitalization (5.1 ± 6.4 vs 9.8 ± 6.3, P < .001), less intensive care unit days than in Group B (0.9 ± 2.1 vs 2.2 ± 2.7, P < .001). Early mortality was 0.6% in both groups. Two-year survival was similar (88% vs 89%), with less reinterventions in Group A (4% vs 17%, P = .004). OR patients had similar 30-day mortalities (0.9% vs 0.7%, P = .89). Conclusion. EVAR and OR have low mortalities. However, in the post-EVAR era we treat older patients with more comorbidities, hospitalization is shorter, and intensive care unit days are less; interventions in EVAR are, however, high.
Introduction
Abdominal aortic aneurysm (AAA) continues to be a major cause of death in the elderly and elective repair is recommended to decrease the high mortality due to rupture of the aneurysm. Open repair (OR) has been the traditional approach for repair of an AAA, but endovascular aneurysm repair (EVAR) has been used with increasing frequency in the past 2 decades since the first series of endograft repairs were reported by Parodi et al in 1991. 1 Prospective randomized multicenter studies in the United Kingdom 2 and Holland 3 confirmed that EVAR can be performed with lower perioperative mortality than OR; however, long-term survival was equivalent after EVAR or OR in the Dutch Randomized Endovascular Aneurysm Management (DREAM), the United Kingdom Endovascular Aneurysm Repair 1 (EVAR-1), and the Open versus Endovascular Repair (OVER) trials2-4 and in a meta-analysis. 5 In addition to decreased early mortality, the OVER trial also observed lower early mortality, shorter hospital stay, and less intensive care unit (ICU) days after EVAR when compared with OR. 6
Previous reports from our group confirmed the low mortality of elective ORs 7 and the obvious early benefits of EVAR. 8 Low mortality of a minimally invasive intervention coupled with shorter hospitalization and earlier return to an active lifestyle stimulated patients and interventionists alike to perform more EVAR than OR for repair of AAAs. 9 A meta-analysis of retrospective studies and the 3 randomized controlled trials have stimulated the preferential use of EVAR when compared with OR, in spite of the higher rate of late complications, increased costs, and need for surveillance and reinterventions.6,10
Few studies have investigated, however, the effect of EVAR on overall outcome of patients who needed elective treatment for AAA.11,12 The purpose of our study was to review our experience of elective AAA repair, comparing 2 different time periods before and after the EVAR era, in terms of early and midterm mortality, morbidity, and freedom from reinterventions in consecutive patients who underwent elective repair of AAAs using either OR or EVAR during 1997 to 1998 with those who had repair during 2007 to 2008 at a tertiary medical center.
Methods
Database and Patients
Clinical data of patients who underwent repair of AAAs was retrospectively reviewed and entered into the Mayo Clinic Aortic Registry. For this study, data were collected from 2 separate time periods: Group A, from January 1, 1997, to December 31, 1998, before the endovascular era; Group B, from January 1, 2007, to December 31, 2008, after the endovascular era. Clinical data included demographic information, comorbidities, perioperative data, and early and midterm outcomes. The current version of the Social Security Death Index was used to confirm survival status; follow-up information was obtained from mailing questionnaires.
To assess the impact of EVAR on overall outcome after AAA repairs, patients who underwent OR in Group A were stratified into 3 subgroups: “suitable for EVAR,” “not suitable for EVAR,” and those who were “suitable for EVAR but unknown from the available data”. Suitability for EVAR was based on anatomic criteria, as determined by a preoperative computed tomography (CT) scan: proximal neck length ≥15 mm, neck diameter between 18 mm and 32 mm, angle <60° relative to the long axis of the aneurysm, and angle <45° relative to the axis of the suprarenal aorta.
Exclusion and Inclusion Criteria
Patients who underwent elective repair for asymptomatic infrarenal AAAs were included in this study. Patients with pararenal or suprarenal AAAs, symptomatic or ruptured AAAs, those who underwent concomitant renal or visceral revascularization, patients with isolated iliac aneurysm, nonconventional endovascular repairs for treatment of complex AAA (using surgeon modified stent graft, fenestrated and branched graft), mycotic AAA or abdominal aortic pseudoaneurysms, previous AAA repair, or patients who were unwilling to give informed consent were excluded from the study.
Outcomes Measure
Primary endpoints included early and midterm mortality, major complications, and procedure-related freedom from reinterventions. Secondary endpoints included hospital days and ICU stays. The Society of Vascular Surgery (SVS) comorbidity scores were used to evaluate outcomes based on surgical risks. 13
Outcomes of the 2 main groups and, separately, between EVAR and OR were compared. Outcomes between the following subgroups were also compared: (a) EVAR patients and those OR patients who were potentially suitable for EVAR in Group A versus EVAR patients in Group B; (b) OR patients not suitable for EVAR in Group A versus OR patients in Group B; (c) OR patients in Group A versus OR patients in Group B; and (d) EVAR patients versus OR patients in Group B.
Definition
Data regarding preexisting medical comorbidities, such as the Society for Vascular Surgery comorbidity grading score (SVS score; cardiac, respiratory, renal, hypertension, age), were collected. 13 Other variables recorded included family history and the site of aortic cross-clamping.
Major complications at 30 days were defined as follows.
Major Medical Complications (30 Days)
Myocardial infarction = symptomatic and/or electrocardiogram changes alone or with Troponin increase
Dysrhythmia = requiring cardioversion or device positioning (defibrillator, pacemaker)
Heart failure = acute heart failure or reactivation of chronic heart failure
Respiratory = all causes requiring prolonged mechanical ventilation (>2 days)
Renal = requiring temporal or definitive dialysis
Neurologic = ischemic event (transient ischemic attack, minor or major stroke), requiring carotid endarterectomy.
Major Surgical Complications (30 Days)
Leg ischemia/emboli, bowel ischemia, bleeding, laparotomy wound complications, and endograft conversion to OR. Endograft complications included graft thrombosis and infection. Endograft complications were considered major if it required reintervention.
Minor Complications (30 Days)
Bleeding = requiring >3 units of blood transfusion but not surgical early reintervention
Minor dysrhythmia = controlled with drugs or spontaneously reversed
Respiratory = pneumonia or all other causes resolved with medical therapy
Renal = creatinine increase >0.5 mg/dL but not requiring dialysis
Leg ischemia/emboli = treated with vasodilator
Bowel ischemia = treated conservatively
Wound complications = superficial separation or infection treated conservatively
Reintervention was defined as any type of additional surgical or endovascular procedure performed to treat complications specifically related to the primary AAA repair operation.
Procedures
All procedures including EVAR and OR were performed by vascular surgeons, with interventional radiologists participating in the procedures in Group A. Selection of EVAR or OR was left to the discretion of the surgeon depending on anatomy, comorbidities, and consideration of patient preferences.
OR involved transperitoneal or retroperitoneal repair of AAA with a straight or bifurcated polyethylene graft. The level of aortic clamping was decided by the surgeon depending on the extent of the aneurysm and the quality of the aorta proximal to the aneurysm. EVAR involved transfemoral or transiliac introduction of an US Food and Drug Administration–approved expandable stent graft to exclude the aneurysm.
Follow-Up
Follow-up visits were usually scheduled at 1, 6, and 12 months after aneurysm repair and subsequently yearly. The 1- and 6-month follow-up visits after EVAR included enhanced CT or CT angiography of the abdomen, whereas after OR physical examination was generally performed; however, if in presence of suspicious clinical finding a duplex scan or CT imaging was performed. Up-to-date information was obtained from mailing questionnaires.
Statistical Analysis
Mean values and standard deviations were compared using the 2-sample t-test. The Pearson, χ2, and Fischer exact tests were used for analysis of categorical variables. Kaplan–Meier survival curves for death and freedom from reinterventions were estimated, and the log-rank P value was used to compare the 2 groups. Univariate analysis was performed using a Pearson correlation coefficient to compare early and midterm mortality, survival, and freedom from reinterventions in the different groups and subgroups. A value of P < .05 was used to determine statistical significance.
Results
During the 4 years of the 2 separate time periods (1997-1998 and 2007-2008) of this study, a total of 903 patients underwent AAA repair at Mayo Clinic, Rochester, MN. Based on inclusion and exclusion criteria, a total of 661 consecutive patients who underwent elective infrarenal AAA repair were included in the study. In Group A (n = 331), 321 (97%) patients underwent OR and only 10 (3%) patients underwent EVAR; in Group B (n = 330), 136 patients (41%) underwent OR and 194 (59%) had EVAR.
Of the patients who underwent OR in Group A, 31% (n = 100) have been identified using preoperative CT scan as suitable for EVAR, and 35% (n = 112) were not suitable for EVAR; for the remaining 109 patients (34%), determination of suitability for EVAR was unreliable because of inconsistent documentation, and so these patients were excluded from subgroup analysis (Figure 1).
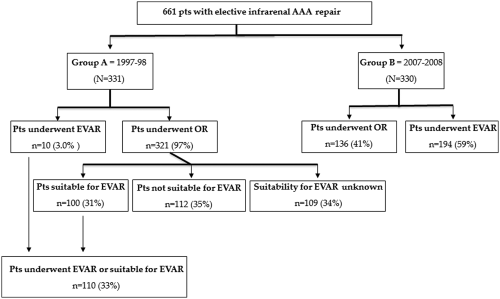
Treatment strategy of 661 patients with elective AAA repair treated between 1997 and 1998 (Group A) and between 2007 and 2008 (Group B).
Preoperative data are reported in Table 1. There was no difference in individual SVS comorbidity scores (cardiac, renal, and pulmonary) between the 2 groups, but the total comorbidity score was significantly higher in Group B than in Group A (8.3 vs 7.5, P = .04). Mean age was higher (74 ± 8.5 vs 73 ± 7.0 years, P = .02), and hypertension, diabetes, chronic obstructive pulmonary disease, and family history of AAA was more frequent in Group B than in Group A (Table 1).
Demographics and Comorbidities of 661 Patients With Elective AAA Repair Treated Between 1997 and 1998 (Group A) and Between 2007 and 2008 (Group B).
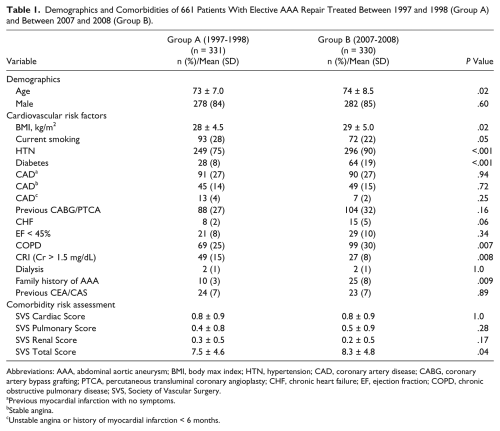
Abbreviations: AAA, abdominal aortic aneurysm; BMI, body max index; HTN, hypertension; CAD, coronary artery disease; CABG, coronary artery bypass grafting; PTCA, percutaneous transluminal coronary angioplasty; CHF, chronic heart failure; EF, ejection fraction; COPD, chronic obstructive pulmonary disease; SVS, Society of Vascular Surgery.
Previous myocardial infarction with no symptoms.
Stable angina.
Unstable angina or history of myocardial infarction < 6 months.
Operative data of Groups A and B are listed in Table 2. General anesthesia was used for most patients although the introduction of EVAR resulted in more frequent use of epidural anesthesia in Group B than in Group A (P = .01). Thirty-one patients underwent minilaparotomy in Group B versus none in Group A (P < .001), and OR became more complex in Group B than in Group A with significant increase in the number of patients requiring suprarenal aortic clamping (40% vs 17%, P = .001).
Operative Data of 661 Patients With Elective AAA repair Treated Between 1997 and 1998 (Group A) and Between 2007 and 2008 (Group B).
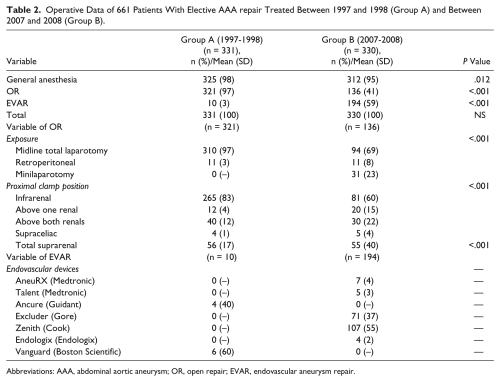
Abbreviations: AAA, abdominal aortic aneurysm; OR, open repair; EVAR, endovascular aneurysm repair.
Mean hospital stays were less and ICU stays were shorter in Group B than in Group A (5.1 ± 6.4 vs 9.8 ± 6.3, P < .001, and 0.9 ± 2.1 vs 2.2 ± 2.7, P < .001). There was no difference in 30-day mortality and major complications between the groups (0.6% for both groups, P = 1.0; 10% vs 7.6%, P = .17; Table 3). There was, however, a decrease in the incidence of postoperative CHF (0% vs 0.9%, P = .08) and respiratory complications in Group B than in Group A (0.9% vs 2.7%, P = .08). There was no difference between the 2 groups in major surgical complications (3.3% vs 3.9%, P = .67) and minor complications (15% vs 12%, P = .49). Survival at 2 years was similar in both groups (88% vs 89%, P = .69; Figure 2). Freedom from reinterventions, however, was significantly higher in Group A when compared to Group B (96% vs 83%, P = .004; Figure 3).
Early Outcome After Elective AAA Repairs Treated Between 1997 and 1998 (Group A) and Between 2007 and 2008 (Group B). a
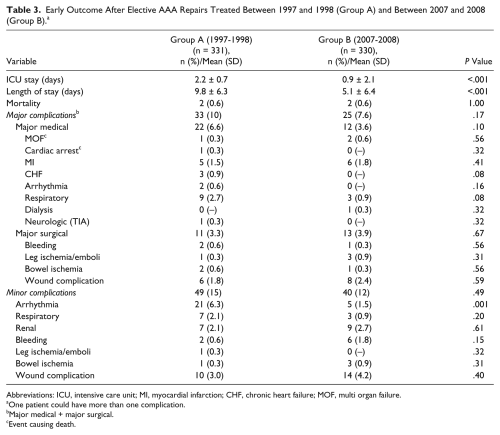
Abbreviations: ICU, intensive care unit; MI, myocardial infarction; CHF, chronic heart failure; MOF, multi organ failure.
One patient could have more than one complication.
Major medical + major surgical.
Event causing death.
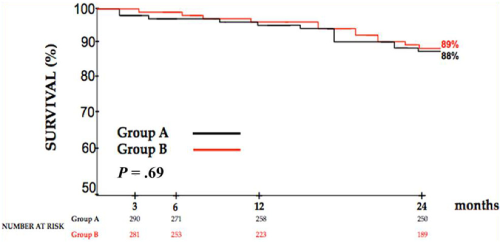
Survival after 661 elective AAA repairs treated between 1997 and 1998 (Group A) and between 2007 and 2008 (Group B).
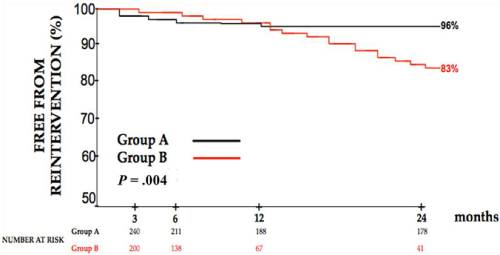
Freedom from reintervention after 661 elective AAA repairs treated between 1997 and 1998 (Group A) and between 2007 and 2008 (Group B).
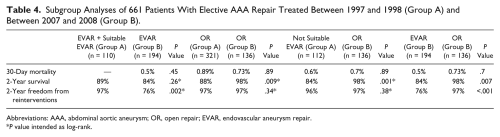
In subgroup analyses, EVAR patients and those considered suitable for EVAR but underwent OR in Group A were compared with those who underwent EVAR in Group B. There was no difference in 30-day mortality (0% vs 0.5%, P = .45) and 2-year survival (89% vs 84%, P = .26). At 2 years, more patients required reinterventions in Group B versus Group A (24% vs 3.0%, P = .002; Table 4). For OR patients between Groups A and B, there was no difference in 30-day mortality (0.9% vs 0.7%, P = .89) and freedom from reintervention at 2 years (97% vs 97%, P = .34). For OR patients not suitable for EVAR in Group A and OR patients in Group B, there were no differences in 30-day mortality (0.6% vs 0.7%, P = .89) and 2-year freedom from reintervention (96% vs 97%, P = .38). In Group B, EVAR patients had significantly higher total, cardiac, and pulmonary comorbidity scores than OR patients (Table 5). Hospital stay was significantly shorter (2.6 ± 2.8 vs 8.6 ± 8.2, P < .001) and ICU days were less in EVAR patients when compared with OR patients (0.2 ± 0.7 vs 1.6 ± 2.7, P < .001). There was no difference in 30-day mortality (0.5% vs 0.7%, P = .80), but patients with EVAR had a lower freedom from reinterventions compared to OR patients (76% vs 97%, P < .001; Table IV).
Subgroup Analyses of 661 Patients With Elective AAA Repair Treated Between 1997 and 1998 (Group A) and Between 2007 and 2008 (Group B).
Abbreviations: AAA, abdominal aortic aneurysm; OR, open repair; EVAR, endovascular aneurysm repair.
P value intended as log-rank.
SVS Score, ICU, and Length of Stay in EVAR and OR Within Group B Treated Between 2007 and 2008.
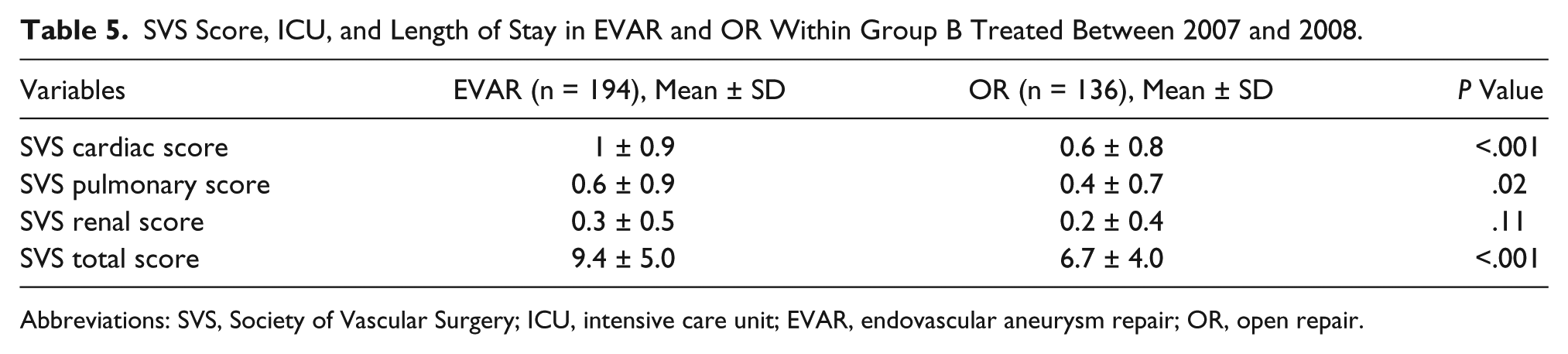
Abbreviations: SVS, Society of Vascular Surgery; ICU, intensive care unit; EVAR, endovascular aneurysm repair; OR, open repair.
Discussion
The evolution of endovascular technologies and new approved devices has resulted in rapid increase in the number of EVAR procedures relative to the traditional OR in the past 2 decades. The advantages of EVAR include shorter hospitalization and ICU stay, decreased recovery time, and superior early outcome.2,3,6,14-19 In spite of negative reports on EVAR citing increased cost, lack of decreased late all-cause late mortality, lack of late improvement in quality of life, increased reintervention rate, and a low but definite risk of late rupture,2-4,19,20 EVAR in different institutions is performed in 50% to 80% of the patients today who present with AAA.19,2021-23 In our experience, during the years of this study (2007-2008), 59% of the patients with AAA underwent EVAR.
In our series early mortality was below 1% in both groups, and it was similar in both EVAR and OR; major complications were also similar (10% vs 7.6%). Costin et al 11 reviewed results of ORs before and after the endovascular era (1996-2004); mortality and morbidity rates were also similar to those observed in patients operated on before the endovascular era. A similar conclusion was reached by Ballotta et al, 12 who reported on outcome of OR in octogenarians, before and after the endovascular era. Hiromatsu et al 22 reported identical results.
Since aneurysm with suitable anatomy frequently undergo EVAR, there has been a significant increase of challenging cases performed by OR. The relative percentage of suprarenal clamping increased from 17% to 40% in our study periods; this finding is supported by Costin et al, 11 who reported increased percentage of suprarenal cross-clamping from 6% to 20% between the pre (from 1996 to 1999) and post (from 1999 to 2004) EVAR era.
Nevertheless, in our experience, the subgroup analyses performed within OR in the 2 time periods did not show any difference in 30-day mortality, complications, and freedom from reintervention. A similar conclusion was reached by Ballotta et al 12 in a cohort of octogenarians patients with AAA treated with OR in the modern era. However, we found 10% of decreased survival at 2 years in the OR in Group A compared to OR in Group B and 14% in those patients not suitable for EVAR in Group A compared to OR in Group B. The better survival found in the modern era in these subgroups could be explained by the fact that today higher risk patients are more frequently treated by EVAR, while OR is performed in patients with unsuitable anatomy but normal or low surgical risk. It is also possible that better perioperative care today contributes to better outcome in high-risk patients.
OR has also changed in the past decade, and the introduction of minilaparotomy decreased the invasiveness of the procedure. In our study, 23% of the patients in Group B underwent minilaparotomy while in Group A no minilaparotomy was used. A previous case–control study conducted by Bakoyiannis et al 24 comparing OR for AAA with and without minilaparotomy showed significant better outcomes for minilaparotomy in terms of faster recovery and shorter hospital length of stay (4.0 ± 0.8 vs 9.7 ± 2.7, P < .05).
EVAR has so far failed to improve significantly long-term survival.3-5,20 Our estimated survival between Groups A and B failed to demonstrate significance between the pre- and post-EVAR era in the overall 2-year survival after AAA repair. This finding could be influenced by many variables and does not definitely answer the question whether EVAR significantly affected the overall survival after AAA repair. The temporal interval of 10 years between the 2 groups and the older and higher risk patients operated in the modern era (Group B) represents an important bias.
EVAR results in higher rate of reinterventions. In our study, 2-year freedom from reintervention was significantly higher in the pre-EVAR era compared to the EVAR era. This was also confirmed in our subgroup analysis, in which patients who were suitable for EVAR in Group A were compared with patients who underwent EVAR in Group B: those who did not undergo EVAR had a higher freedom from reintervention (97% vs 76%, P = .002).
As a retrospective study, this study has some obvious limitations. The choice of EVAR or OR was left to the discretion of the surgeon. The comparison of 2 different time periods with a gap of 10 years can be biased by several factors, including advances in medical therapy for cardiovascular risk prevention and earlier diagnosis and treatment of some diseases including heart disease, pulmonary disease, and malignancies. Nevertheless, subgroup analyses were helpful to support our conclusions that the results were related mostly to EVAR and not to other confounding factors.
Management of AAAs has dramatically changed in the past decade and now approximately 60% to 80% of patients are treated with EVAR. Both EVAR and OR can be performed with a low rate of mortality and an acceptable rate of complications; mortality at our institution has not changed in the post- versus pre-EVAR era. EVAR, however, has allowed us to treat older patients with more comorbidities and has resulted in shorter hospital stays and less ICU days. These advantages came at a price of higher reintervention rates in the modern era.
Footnotes
Acknowledgements
We thank Ms Marianne Huebner, Ms Catherine E. Dvorak, and Mr Patrick D. Fitz-Gibbon for their assistance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.