
Abstract
Introduction
Clinical prediction models for response to epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitor (TKI) therapy in patients with advanced non-small cell lung cancer (NSCLC) with bone metastasis (BoM) and EGFR mutations are lacking. This study evaluated predictors of response to the EGFR-TKI icotinib in patients with NSCLC and BoM.
Methods
We retrospectively analysed patients with EGFR-mutated NSCLC and BoM treated with icotinib at Wuhan Union Hospital. Least absolute shrinkage and selection operator and multivariate Cox regression analyses identified independent predictors of progression-free survival (PFS). A prognostic nomogram was developed, and its effectiveness was assessed using receiver operating characteristic (ROC) curves, a decision curve analysis (DCA), and calibration curves.
Results
Among 194 patients (106 with and 88 without BoM), median PFS in the BoM group was 9.8 months, with a 35.8% overall response rate, and 66.0% disease control rate. In univariate and multivariate Cox regression analyses, BoM was an independent predictor of PFS in the overall cohort (hazard ratio [HR], 2.12; 95% confidence interval [CI], 1.34–3.07; P < 0.001). In the BoM subgroup, albumin (HR: 0.36; 95% CI: 0.21–0.62; P < 0.001), lactate dehydrogenase (LDH) (HR: 1.99; 95% CI: 1.21–3.28; P = 0.007), and the platelet–lymphocyte ratio (PLR) (HR: 1.85; 95% CI: 1.05–3.25; P = 0.033) were independently associated with PFS. A nomogram predicting 3-, 6-, and 12-month PFS achieved time-dependent areas under the ROC curve of 0.765, 0.743, and 0.724, respectively. Calibration plots and DCA demonstrated acceptable performance and potential clinical relevance.
Conclusions
Albumin, LDH, and PLR predict PFS in EGFR-mutated NSCLC with BoM treated with icotinib. The proposed nomogram may assist in preliminary risk stratification in this specific population.
Keywords
Introduction
Lung cancer remains the primary cause of cancer-related deaths globally, 1 with non-small cell lung cancer (NSCLC) accounting for 80–85% of all reported cases. 2 Approximately half of all instances of lung cancer result in bone metastasis (BoM), one of the most prevalent types of distant dissemination. BoM has been reported in 30–40% of individuals at the initial NSCLC diagnosis, with 35–60% subsequently developing BoM during disease progression.3,4 In general, patients with BoM have poorer clinical outcomes than those of patients with advanced NSCLC who have not developed metastases. 5 Accurate prediction of drug efficacy is crucial for patients with NSCLC and BoM.
Tyrosine kinase inhibitors (TKIs) have substantially improved the survival rates of patients with lung cancer, especially those harbouring sensitising mutations in the epidermal growth factor receptor (EGFR). 6 However, NSCLC treatments have limited effectiveness in terms of progression-free survival (PFS) and overall survival (OS) in patients with BoM. This may be attributed to the critical role of EGFR in osteoblast maturation: downregulation of the EGFR signaling pathway impairs osteoblast-mediated bone repair.7,8 Furthermore, aberrant activation of Wnt signaling contributes to the development of BoM, and this pathway also exerts a negative impact by enhancing resistance to TKI treatment. 9 The median PFS among patients without BoM ranges from 11.0 to 15.0 months, and the OS ranges from 17.5 to 38.0 months. In comparison, patients with BoM have a PFS of approximately 8.0–9.0 months and OS of 20.0–25.0 months.10,11 In a previous study, 220 patients with NSCLC with BoM and good performance status (Eastern Cooperative Oncology Group performance status 0, 1) exhibited greater benefit from EGFR-TKI treatment. 12 Huang et al have demonstrated that EGFR-TKIs, which are beneficial in treating primary lung cancer, can also be used to treat lung cancer with BoM. 13 Nevertheless, the impact of metastatic lesions on the efficacy of targeted therapies has not been clarified.
The spread of cancer is affected by systemic inflammation and nutritional status. Intense inflammatory responses, often indicating a poor prognosis, result from changes in tumour-infiltrating inflammatory cells.14,15 In addition, one-third of cancer-related deaths can be attributed to nutritional deficiencies. 16 Some routine blood indicators have been identified as meaningful inflammatory biomarkers in cancer. For instance, the neutrophil–lymphocyte ratio (NLR) and platelet–lymphocyte ratio (PLR) support early surgical decision-making and guide treatment strategies for advanced NSCLC; they are also correlated with the mortality of lung cancer.17,18 Furthermore, reduced albumin levels predict poor outcomes in lung cancer. 19 Elevated lactate dehydrogenase (LDH) levels reflect tumour burden and predict BoM status in digestive system tumours.20,21 However, correlations between these biomarkers and the therapeutic effects of TKIs have not been established.
The purpose of this study was to evaluate the therapeutic efficacy of the EGFR-TKI icotinib in patients with EGFR-mutated NSCLC with BoM and to identify predictive factors for PFS in this specific subgroup. We aimed to develop an exploratory, clinically accessible prognostic model for this specific subgroup.
Methods
Patients
This retrospective observational study included patients with stage IV EGFR-mutated NSCLC who received first-line icotinib treatment at Wuhan Union Hospital between January 2017 and October 2020. A total of 262 patients were initially screened, and 68 were excluded: 12 were lost to follow-up, 55 had incomplete clinical or laboratory data within 30 days after initiation of icotinib treatment, and 1 experienced severe adverse reactions within 30 days. The final analysis cohort comprised 194 patients: 106 with BoM (BoM+) and 88 without BoM (BoM-); the patient selection flowchart is presented in Figure 1. Eligible patients were those who received icotinib monotherapy or icotinib combined with clinically indicated concomitant treatments (radiotherapy, chemotherapy, or bone-protecting agents). Baseline clinical and laboratory variables were defined as measurements obtained within 30 days before icotinib initiation. This was a retrospective observational study. The study protocol was reviewed and approved by the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (No. 2022-0649-01; Date: November 12, 2022). Informed consent was waived by the ethics committee owing to the retrospective nature of the study and anonymous processing of all clinical data, in accordance with the Helsinki of Declaration (1975, 2024 revision). The reporting of this study conforms to the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis Or Diagnosis (TRIPOD) guidelines.
22
The TRIPOD checklist is displayed in the Supplementary. Flowchart of the study design.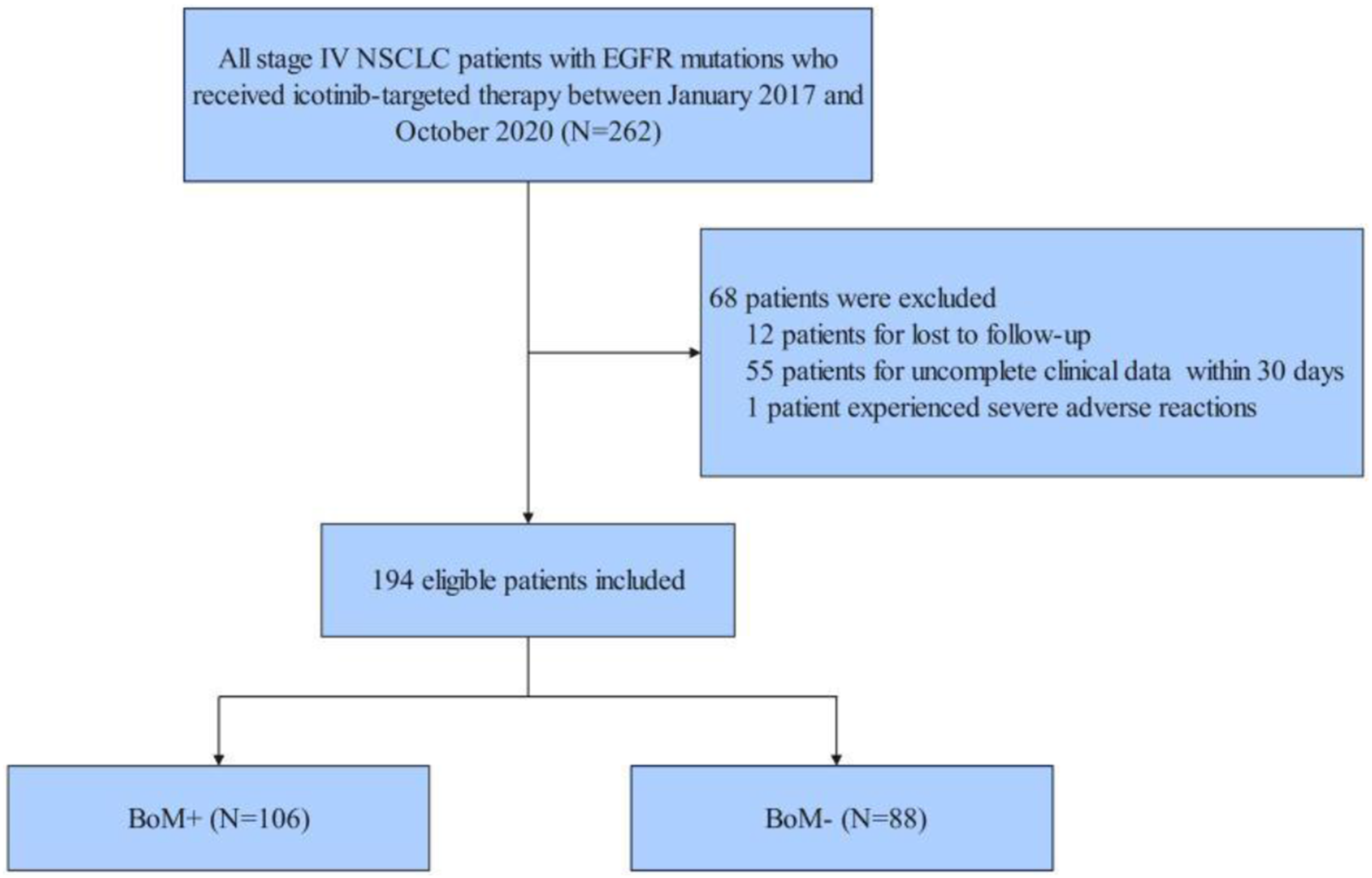
Data Collection
Patient data — including demographics (age, sex, and smoking status), tumour characteristics (pathological type, Eastern Cooperative Oncology Group performance status, EGFR mutation type, clinical stage, and extrapulmonary metastases other than BoM), and laboratory indicators — were obtained from patient records. In addition to the exon 19 deletion (19Del), exon 21 L858R (L858R), and compound mutations, rare EGFR mutations were identified.
The following were used to calculate a composite index: prognostic nutritional index (PNI), systemic inflammation response index (SIRI), lung immune prognostic index (LIPI), modified Glasgow Prognostic Index (mGRI), derived NLR (dNLR), neutrophil–platelet ratio (NPR), albumin–globulin ratio (AGR), monocyte–lymphocyte ratio (MLR), lymphocyte–monocyte ratio (LMR), systemic immune-inflammation index (SII), Naples prognostic score (NPS), and PLR and NLR. 23 Carcinoembryonic antigen (CEA), carbohydrate antigen (CA)-125, CA-199, albumin, and LDH levels as well as neutrophil, lymphocyte, monocyte, and platelet counts were utilised as laboratory markers.
Assessment of Outcomes
PFS was the primary outcome. The objective response rate (ORR) and disease control rate (DCR) were secondary outcomes. PFS was defined as the time between starting icotinib treatment and disease progression at any site or death. The best overall response (complete remission (CR), partial response (PR), stable disease (SD), or progressive disease (PD)) was evaluated using the revised Response Evaluation Criteria in Solid Tumours, version 1.1 criteria. The ORR was defined as the proportion of patients with CR and PR, while the DCR represented those who received CR, PR, and SD. The most recent follow-up examination was completed on 21 August 2021.
Statistical Analysis
Continuous variables were presented as mean ± standard deviation (SD), and comparisons between groups were performed using the t-test or Mann-Whitney U test (depending on data distribution). Categorical variables were expressed as frequency and percentage, with inter-group comparisons conducted via the Chi-square test. Variables with a skewed distribution were subjected to logarithmic transformation. The Youden index was used to determine the optimal cut-off values for prognostic indicators. First, least absolute shrinkage and selection operator (LASSO)-Cox regression with 10-fold cross-validation was applied to the total cohort (N = 194) to screen for prognostic factors associated with PFS. The optimal λ value was selected based on the minimum partial likelihood deviance criterion (1-standard error criterion as a supplement), and only variables with non-zero coefficients were retained. Subsequently, univariate and multivariate Cox regression analyses were performed to identify independent prognostic factors for patients with NSCLC treated with icotinib. Kaplan-Meier curves combined with the log-rank test were used for PFS analysis, which confirmed that BoM was an independent prognostic factor for NSCLC patients receiving icotinib. To further identify prognostic risk factors specific to BoM+ patients, LASSO-Cox regression with 10-fold cross-validation was repeated in the BoM+ subgroup (N = 106) to screen survival determinants from 33 candidate indicators. These indicators included age, sex, Eastern Cooperative Oncology Group (ECOG) performance status score, smoking status, histological type, EGFR mutation type, disease stage, combined treatment, brain metastases, pleural metastasis, platelets, neutrophil, lymphocyte, monocyte, LMR, NLR, PLR, MLR, SII, dNLR, NPR, PNI, SIRI, AGR, albumin, LDH, CEA, CA-125, CA-199, total cholesterol, LIPI score, mGRI score and NPS. Multivariate Cox regression analysis was then conducted to confirm that albumin, LDH and PLR were independent prognostic factors for BoM+ patients, based on which a nomogram was constructed. Internal validation of the nomogram was performed using time-dependent receiver operating characteristic (ROC) curves, calibration plots, and decision curve analysis (DCA). The efficacy of nomogram-based risk stratification for the BoM+ subgroup was verified using Kaplan-Meier curves. All analyses were performed using R software (version 4.3.1), and a two-tailed P-value < 0.05 was considered statistically significant.
Results
Baseline Characteristics and Survival Analysis for all Patients
Baseline Features and Survival Rate of Patients With Advanced NSCLC Treated With Icotinib (N = 194)
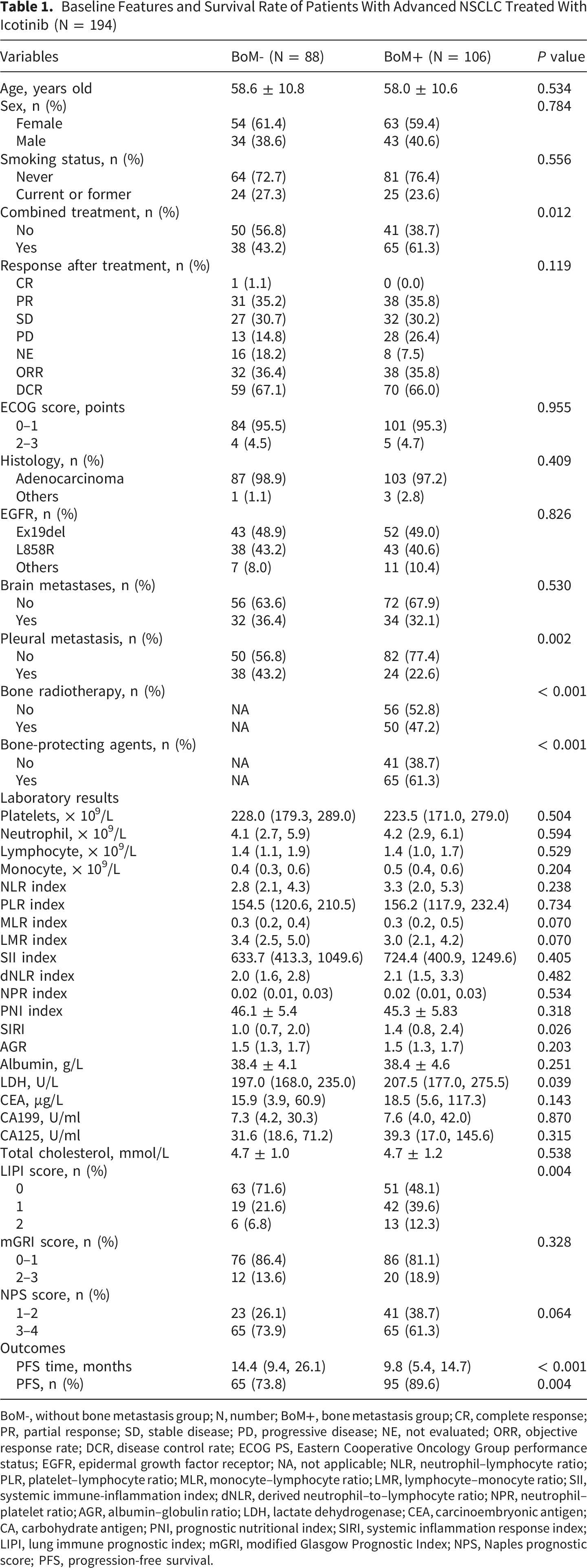
BoM-, without bone metastasis group; N, number; BoM+, bone metastasis group; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; NE, not evaluated; ORR, objective response rate; DCR, disease control rate; ECOG PS, Eastern Cooperative Oncology Group performance status; EGFR, epidermal growth factor receptor; NA, not applicable; NLR, neutrophil–lymphocyte ratio; PLR, platelet–lymphocyte ratio; MLR, monocyte–lymphocyte ratio; LMR, lymphocyte–monocyte ratio; SII, systemic immune-inflammation index; dNLR, derived neutrophil–to–lymphocyte ratio; NPR, neutrophil–platelet ratio; AGR, albumin–globulin ratio; LDH, lactate dehydrogenase; CEA, carcinoembryonic antigen; CA, carbohydrate antigen; PNI, prognostic nutritional index; SIRI, systemic inflammation response index; LIPI, lung immune prognostic index; mGRI, modified Glasgow Prognostic Index; NPS, Naples prognostic score; PFS, progression-free survival.
The efficacy of icotinib therapy is summarized in Table 1. In the BoM-group, 31 patients achieved PR, 27 had SD, and 13 experienced PD, yielding an ORR of 36.4% and DCR of 67.1%. In the BoM+ group, 38 patients achieved PR, 32 had SD, and 28 experienced PD, resulting in an ORR of 35.8% and a DCR of 66.0% (Table 1).
BoM+ Was an Independent Risk Factor for Prognosis in Patients Treated With Icotinib
By the completion of follow-up, the rates of progression/death events were 73.8% (65/88) and 89.6% (95/106) in the BoM- and BoM+ groups, respectively (P = 0.004). Compared with the median PFS in the BoM+ group, the BoM-group had a significantly higher median PFS (14.4 and 9.8 months, respectively; P < 0.001; Table 1).
BoM was associated with poorer PFS, according to Kaplan-Meier survival curves (P < 0.001). When compared with those for patients without metastases, patients with brain and pleural metastases did not have worse PFS results following icotinib treatment (Figure 2). Kaplan-Meier curves showing progression-free survival (PFS) for patients with metastases at several sites treated with icotinib. Patients with (A) bone, (B) brain, and (C) pleural metastases are included.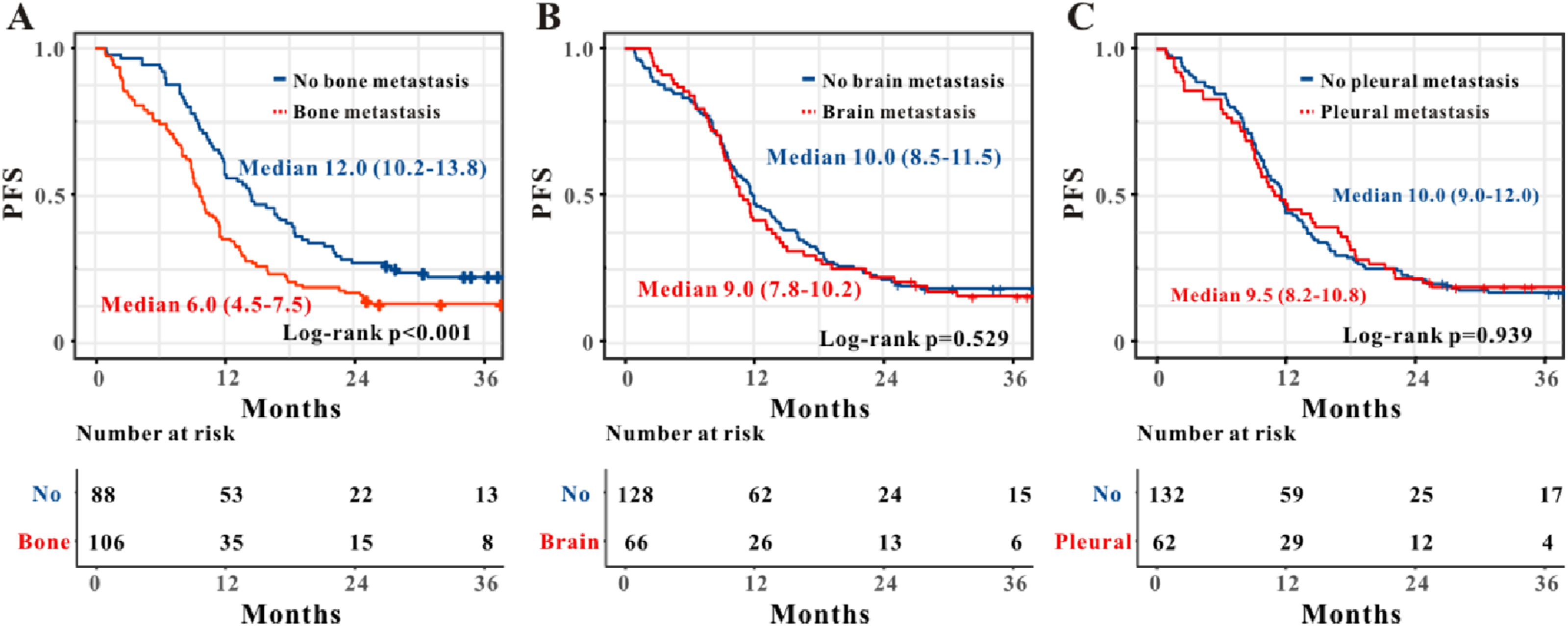
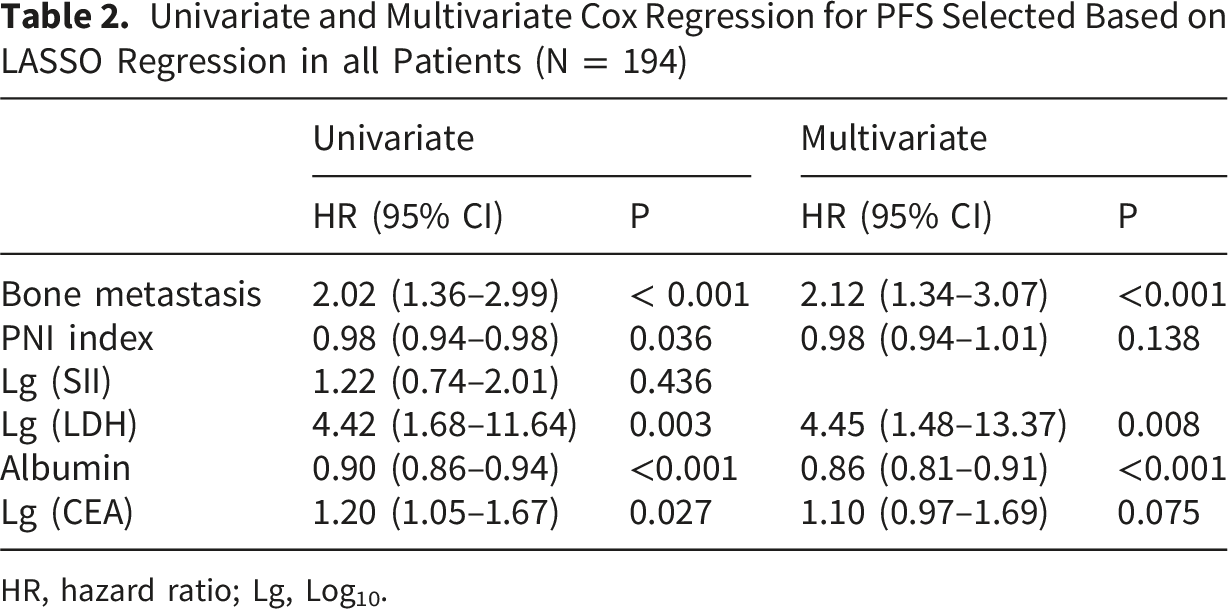
We evaluated whether malignant bone involvement is linked to poor clinical outcomes in patients receiving icotinib (Figure 3). In all patients, univariate and multivariate Cox regression analyses indicated that BoM (HR, 2.12; 95% CI, 1.34–3.07; P < 0.001) is an independent risk factor for PFS (Table 2). LASSO regression-based variable selection for PFS across all patients. (A) Cross-validation was used to identify the optimal parameter λ in the LASSO regression model. (B) Characteristics of variable coefficient changes. (C) Screening prognostic factors for PFS in all patients using LASSO regression. Univariate and Multivariate Cox Regression for PFS Selected Based on LASSO Regression in all Patients (N = 194) HR, hazard ratio; Lg, Log10.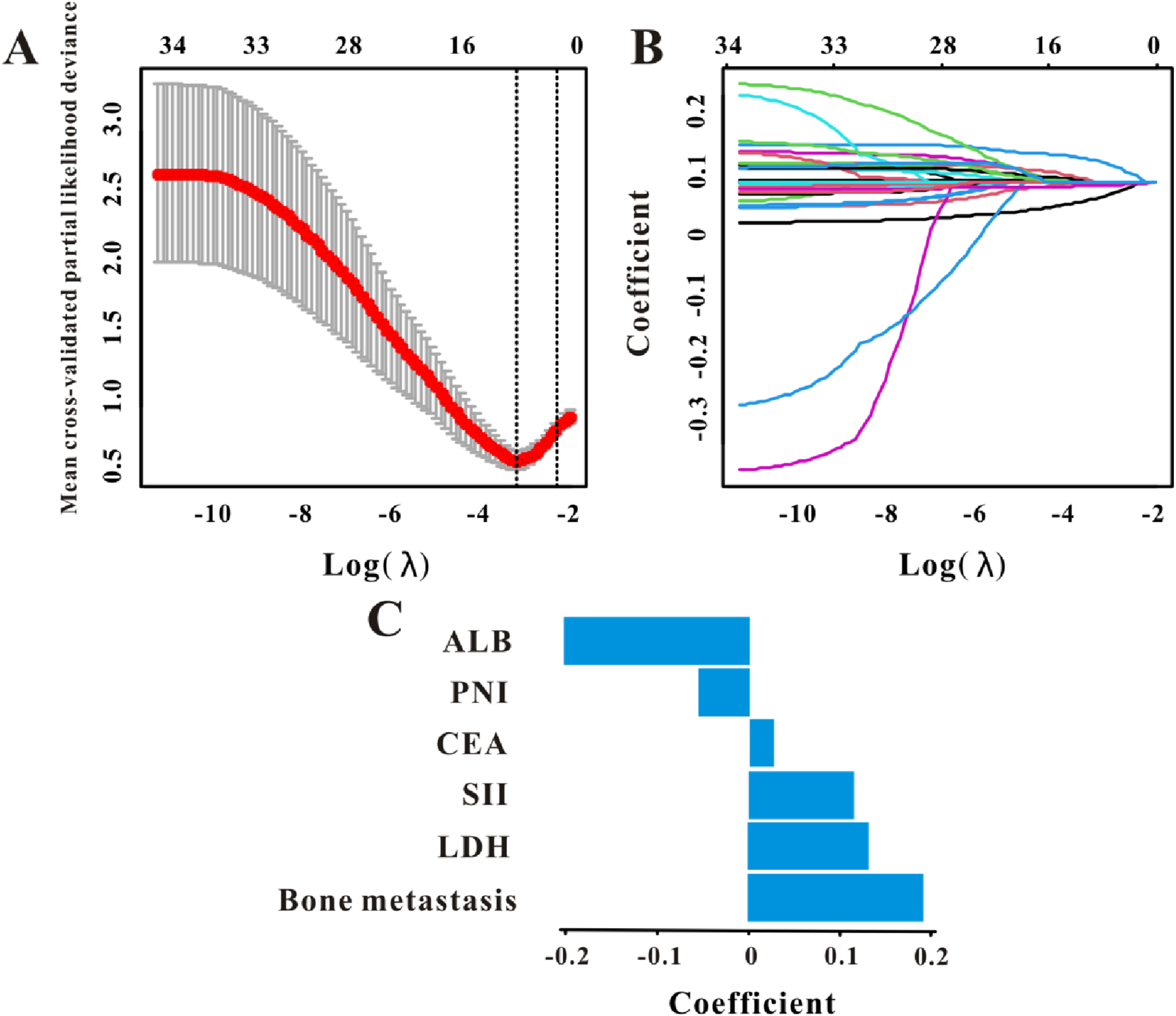
A subgroup analysis of PFS in BoM+ yielded a P-value for the interaction term of 0.568 for the presence of pleural metastasis, suggesting the absence of a significant interaction (Supplemental Table 1). Similarly, neither radiotherapy (P = 0.158) nor bone-protecting agents (P = 0.357) showed a significant interaction with PFS. These findings should be interpreted cautiously given the limitations inherent in a retrospective, single-centre study design.
Univariate and Multivariate Analyses of PFS in the BoM+ Group
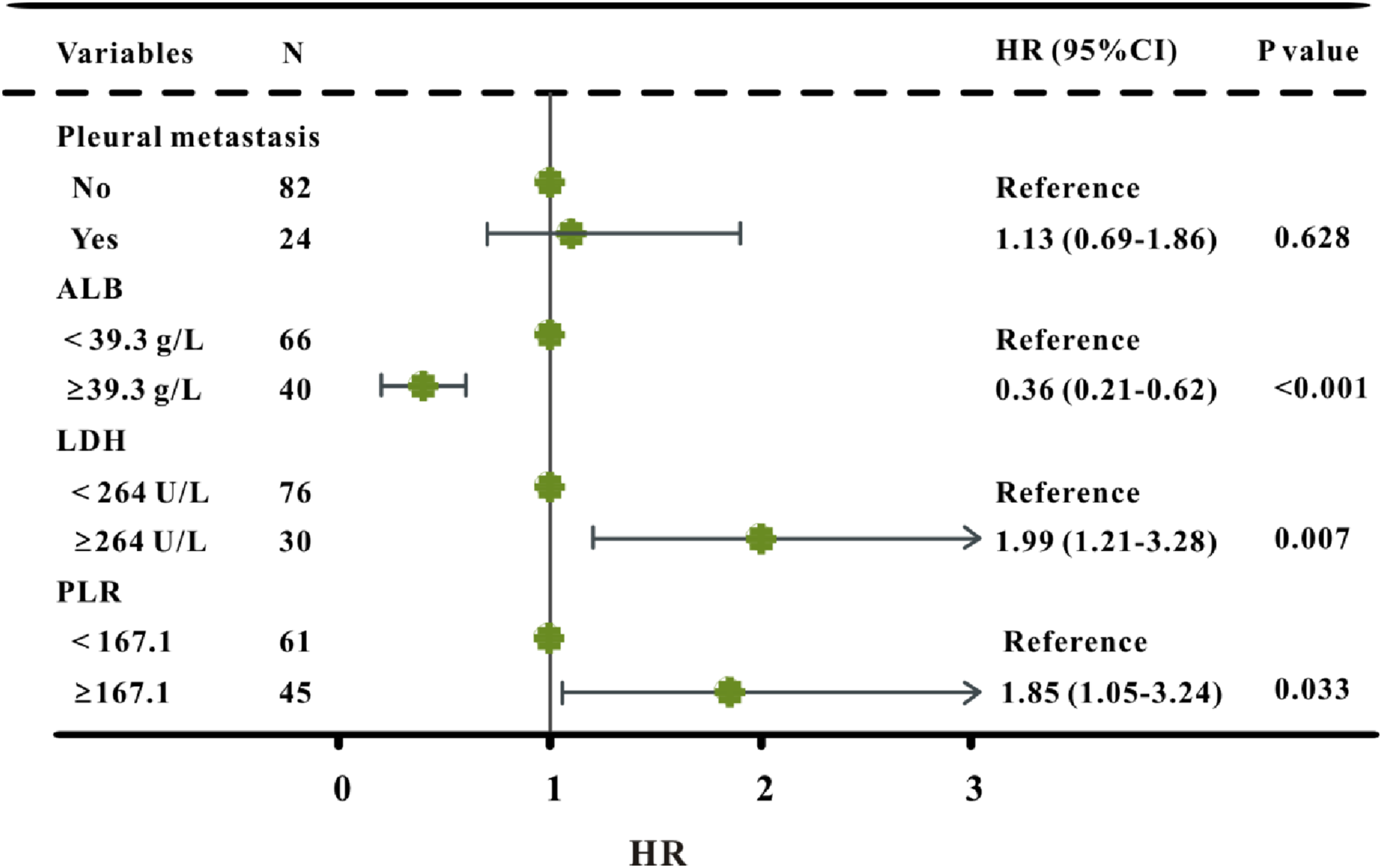
Since BoM was identified as an independent risk factor for PFS, further analyses of the BoM+ group were conducted. Among 33 factors included in the LASSO regression analysis, four variables (pleural metastasis, albumin, LDH, and PLR) were significantly correlated with PFS (Figure 4). Albumin (HR, 0.36; 95% CI, 0.21–0.62; P < 0.001) was linked to better PFS, while LDH (HR, 1.99; 95% CI, 1.21–3.28; P = 0.007), and PLR (HR, 1.85; 95% CI, 1.05–3.24; P = 0.033) were all linked to worse PFS in the BoM+ group, according to a multivariate Cox regression analysis (Figure 5). Variable selection for the BoM+ group using LASSO regression. (A) Ten-fold cross-validation to fine-tune the LASSO–Cox regression model’s parameter selection. (B) 33-variable LASSO coefficient profiles. Forest plot of variables in the multivariate analysis of PFS in the BoM+ group.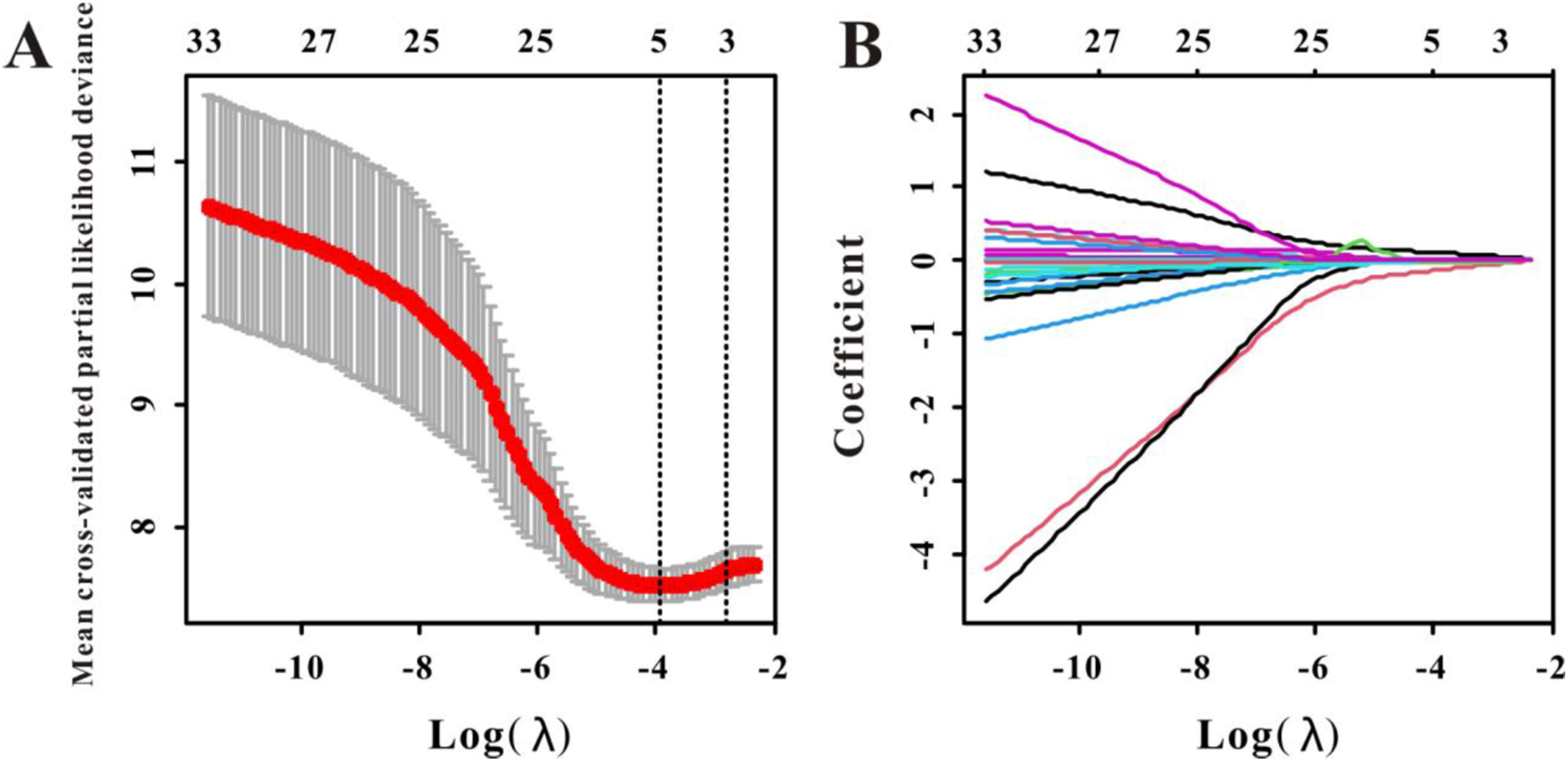
Establishment and Performance Evaluation of a PFS Nomogram Model for the BoM+ Group
We designed a risk prediction nomogram for individuals with NSCLC complicated by BoM, utilising three independent predictors obtained through the multivariate Cox regression analysis (Figure 6). The nomogram demonstrated favorable discriminative performance in this cohort. A cut-off value of 0.554 was used to differentiate between groups at high and low risk. Nomograms for predicting 3-, 6-, and 12-month PFS in the BoM+ group.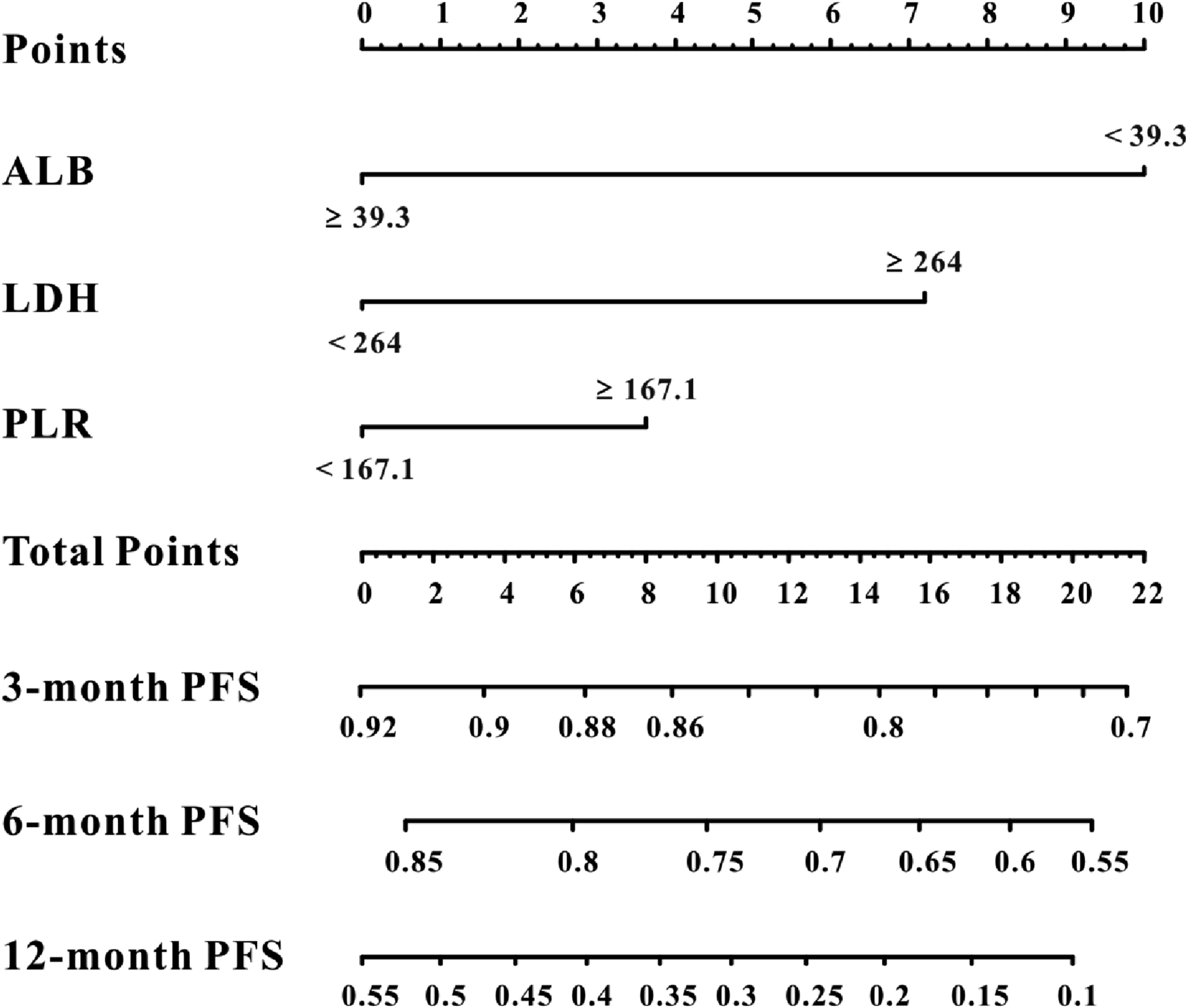
The ROC curve analysis of these independent risk factors is presented in Figure 7. The areas under the time-dependent ROC curve for predicting 3-, 6-, and 12-month PFS were 0.765, 0.743, and 0.724, respectively, suggesting moderate discrimination in this cohort. Furthermore, there was a significant degree of agreement between the calibration curve and expected outcomes. The DCA curves remained above the “treat-all” and “treat-none” lines at 3-, 6-, and 12-month, indicating potential predictive value. Calibration, receiver operating characteristic (ROC), and decision curve analysis (DCA) of the BoM+ nomogram. (A) Calibration curves for 3-, 6-, and 12-month PFS. (B) Validation of the nomogram model using 3-, 6-, and 12-month ROC curves. (C) DCA of 3-, 6-, and 12-month PFS. 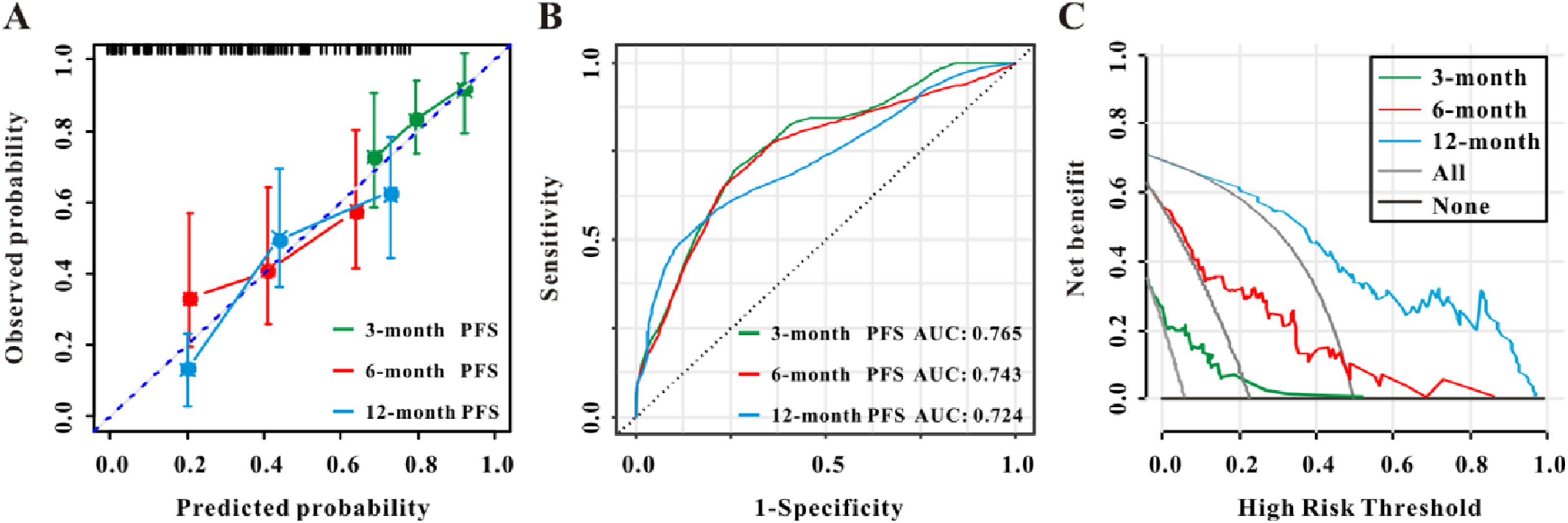
Predictive Performance of Several Risk Factors for PFS (N = 106)
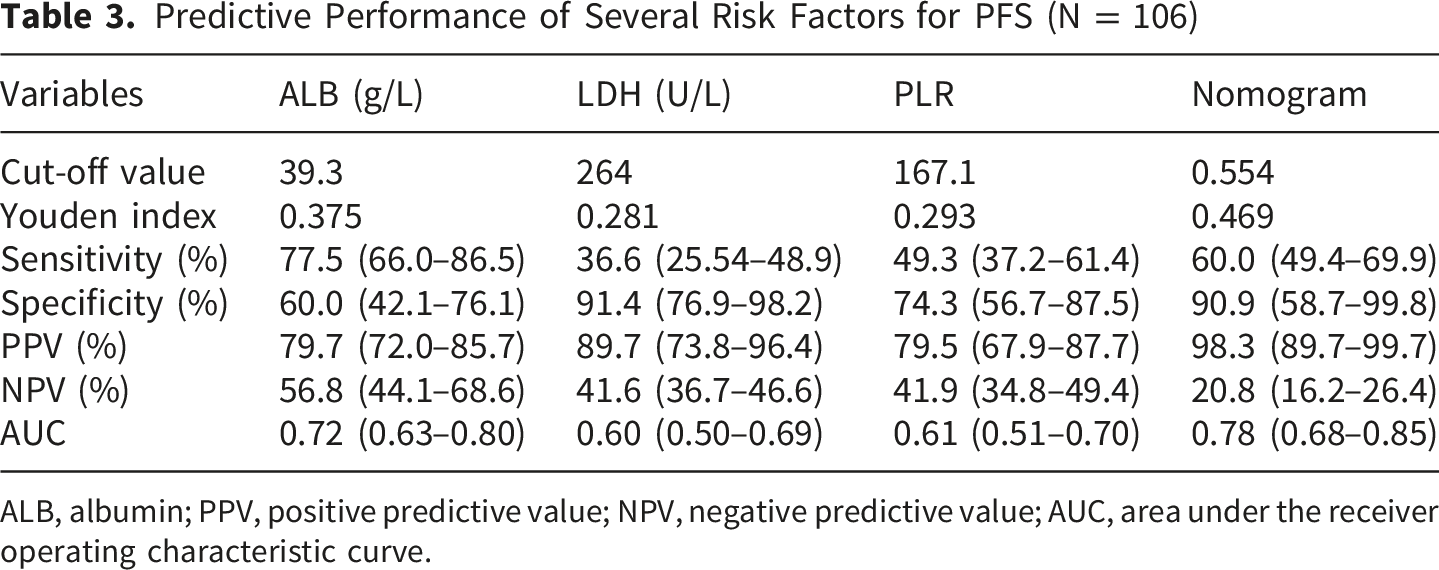
ALB, albumin; PPV, positive predictive value; NPV, negative predictive value; AUC, area under the receiver operating characteristic curve.
Risk Hierarchical System
The survival nomogram exhibited satisfactory predictive performance. We calculated the prognostic risk scores based on the three independent variables included in the nomogram. In the BoM+ group, patients were classified as low-risk (risk score < 0.554) or high-risk (risk score > 0.554). According to a Kaplan-Meier analysis, the low-risk group (N = 42) had a substantially longer PFS than the high-risk group (N = 64; P < 0.001; Figure 8). Kaplan-Meier curves of PFS for low- and high-risk patients with BoM+.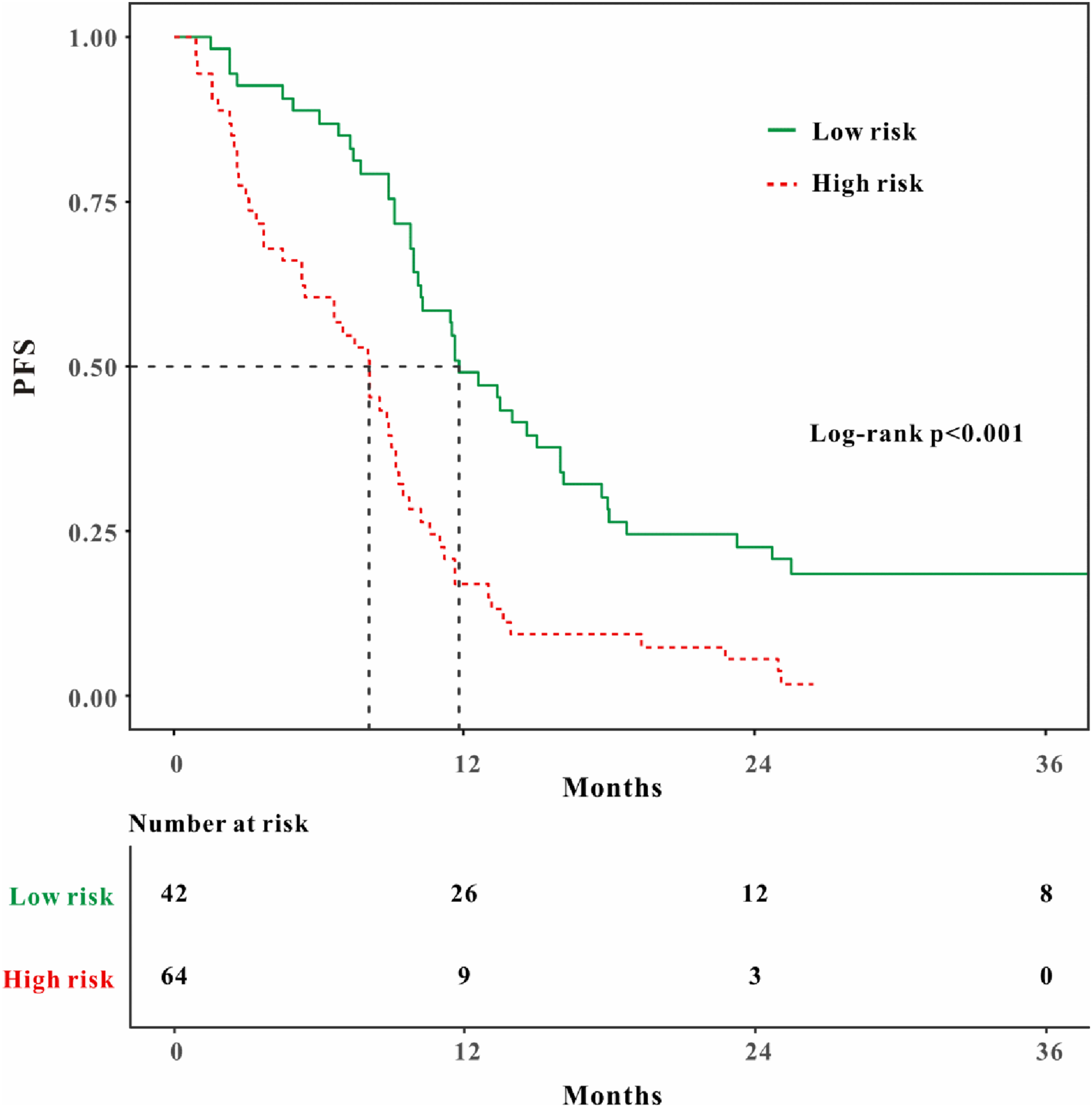
Discussion
Patients with advanced lung cancer have a median survival time of 5 months, and distant metastases are the primary cause of mortality in these patients. 5 The most frequent location of lung adenocarcinoma metastasis is the bone. Nevertheless, lung adenocarcinomas have a more favourable survival rate than those of other lung cancer types. 24 The survival rate of individuals with lung adenocarcinoma and BoM is lower than that of individuals with other NSCLC subtypes, according to Dong et al, 25 consistent with the basic clinical characteristics of the subgroup of BoM studied in this study. There is evidence for the efficacy of two EGFR-TKIs, erlotinib and gefitinib, in patients with distant metastases, which contribute to longer PFS and OS. 26 Our findings support the efficacy of TKIs, confirming that icotinib exerts a therapeutic effect on EGFR-mutant NSCLC with BoM; however, the prognosis of these patients is significantly worse than that of patients without BoM. This discrepancy may be attributed to the dense reticular structure of the bone microenvironment, which induces adhesive contacts between bone marrow stromal cells and tumour cells, thereby impairing the penetration of EGFR-TKIs into tumour tissue. 27 For clinicians, the stratification and prognosis of patients with NSCLC harbouring EGFR-sensitive mutations with BoM remain clinical challenges.
To the best of our knowledge, few studies have specifically developed a PFS nomogram for icotinib-treated EGFR-mutant NSCLC patients with BoM. Despite being suggested for patients with T790M mutations following TKI therapy, osimertinib exhibits limited efficacy as a salvage option for those with BoM, 27 consistent with our findings indicating that BoM is an independent predictor of unfavourable PFS. Currently, the primary treatment strategies for BoM include surgery, radiotherapy, bone-protecting agents (e.g., bisphosphonates/denosumab), chemotherapy, targeted therapy, and immunotherapy, among others. 28 In our study, patients with symptomatic bone metastases received radiotherapy and/or bone-protecting agents. Notably, these two variables were not significantly associated with PFS. Based on a multivariate regression analysis, lower PLR or LDH levels in patients with BoM undergoing icotinib treatment were associated with enhanced efficacy and prolonged PFS, whereas higher albumin levels were associated with longer PFS. These findings provide initial evidence for the prognostic value of these biomarkers in icotinib-treated patients with BoM, as well as a biological basis for constructing prognostic models.
Nutritional status and inflammation affect patient prognosis.29,30 In cancer, low albuminemia and elevated neutrophil, platelet, NLR, and LDH levels are associated with a poor prognosis.17,19-21,31 Patients with a low PLR had better OS and PFS when undergoing immunotherapy for advanced lung cancer, especially advanced NSCLC. 32 Chen et al created two nomograms based on NLR and PLR based on a variable Cox regression model and discovered that high values for these parameters are linked to a worse prognosis in limited-stage small cell lung cancer (SCLC). 33 In our study, poor outcomes in icotinib-treated patients with NSCLC and BoM were associated with a higher PLR, further validating the utility of PLR as an inflammation-related prognostic biomarker.
The serum LDH concentration serves as a proxy indicator of cancer cell metabolic activity. Baseline LDH levels, a biomarker associated with tumour burden, are correlated with unfavourable treatment outcomes in NSCLC. 34 This outcome may be attributed to several factors. For instance, by preventing the activation of CD8+ T lymphocytes and natural killers, LDH may help cancer cells evade the immune response. 35 Furthermore, by increasing vascular endothelial growth factor synthesis, LDH can promote tumour angiogenesis, cell motility, and metastasis. 36 We observed that higher baseline serum LDH and PLR levels were associated with shorter PFS. Additionally, we found that the cut-off values of these two indicators (LDH ≥ 264 U/L, PLR ≥ 167.1) may be related to poor efficacy of icotinib. Baseline serum LDH and PLR serve as optimal cut-off values to identify high-risk patient populations.
According to our findings, higher baseline albumin levels are associated with longer PFS in icotinib-treated NSCLC patients with BoM. Albumin is a prognostic marker for several cancers, such as lung cancer, 37 breast cancer, 38 renal cell carcinoma, 39 and gastrointestinal cancers. 40 It may be employed to assess the nutritional and systemic inflammatory status of patients with cancer. In patients with metastatic NSCLC, serum AGR acts as an independent and prognostic predictor of OS and PFS. 41 In the training and verification sets of two nomograms, Liu et al demonstrated that serum albumin and surgery are unique determinants of prognosis in lung cancer cachexia. 42 Although research has identified a link between low albumin levels and an unfavourable prognosis in advanced lung cancer with BoM, 43 the association between dysregulated albumin levels and TKI therapy has not been described. We observed that a reduced baseline albumin level (cut-off value: 39.3 g/L, determined by the Youden index) was predictive of inferior outcomes in icotinib-treated EGFR-mutant NSCLC patients with BoM, providing a rationale for the subsequent establishment of a prognostic nomogram.
The 5-year OS for most of individuals diagnosed with lung cancer and BoM cannot be estimated. 44 Consequently, PFS is frequently adopted as the primary endpoint in studies of such patients. Previous studies have mostly focused on developing models to predict the advantages of EGFR-TKIs in patients with advanced NSCLC or examining risk and prognostic factors for BoM in particular histological subtypes of lung cancer, failing to achieve stratified PFS prediction for the specific subgroup of EGFR-mutated NSCLC with BoM. 45 In contrast, we developed a nomogram tailored to this specific population, which not only enables the prediction of 3-, 6-, and 12-month PFS in this subgroup, but also determined the clinical cut-off values of three biomarkers and the risk stratification threshold of the nomogram for patient risk grouping. Interestingly, PFS in the low-risk group was significantly longer than that in the high-risk group. Treatment remains challenging for patients with high-risk scores.
This study had some limitations. First, as a retrospective single-centre study, treatment heterogeneity (e.g., variable use of radiotherapy and bone-protecting agents) may have introduced residual confounding bias, although combined treatment was included as a covariate in the statistical analysis. Second, the study focused exclusively on PFS as the primary endpoint and lacked an analysis of OS, which limits the model’s utility for long-term prognostic assessment. Third, this was an exploratory study lacking external cohort validation; further replication or external validation is warranted in future studies of contemporary EGFR-TKI cohorts. Fourth, this study focused on icotinib (a first-generation EGFR-TKI), which remains widely used in resource-limited settings due to its low cost and extensive insurance coverage. However, its applicability to later-generation EGFR-TKIs (e.g., osimertinib) remains unclear, which is a key limitation. Notably, the core biomarkers (albumin, LDH, PLR) reflect universal biological processes (inflammation, nutrition, tumour burden), suggesting potential generalizability, but this requires further validation. Finally, refining the study population to EGFR-mutant NSCLC with BoM improves predictive precision but reduces generalizability to broader NSCLC cohorts. To maximize the applicability of our model and minimize selection bias, we plan to conduct a multicenter study with a larger, more diverse cohort and validate the prognostic value of the identified factors in patients treated with third-generation EGFR-TKIs with an extended follow-up period.
Conclusions
In this single-centre retrospective study, baseline albumin, LDH, and PLR were associated with PFS in patients with EGFR-mutant NSCLC and BoM treated with icotinib. The exploratory nomogram constructed based on these indicators showed acceptable predictive performance for short-term PFS stratification in this cohort. Future large, multicenter prospective studies with external validation are required to further validate and optimize this nomogram for clinical application.
Supplemental Material
Supplemental Material - Survival Prediction in Patients With Epidermal Growth Factor Receptor-Mutated Non-small Cell Lung Cancer With Bone Metastases Receiving Icotinib Therapy: A Retrospective Observational Study
Supplemental Material for Survival Prediction in Patients With Epidermal Growth Factor Receptor-Mutated Non-small Cell Lung Cancer With Bone Metastases Receiving Icotinib Therapy: A Retrospective Observational Study by Yanling Ma, Hui Xia, Xueyun Tan, Siwei Song, Minglei Li, Juanjuan Xu, Feng Wu, Yaqi Cao, Mengjia Yi, Sufei Wang and Yang Jin in Technology in Cancer Research & Treatment
Footnotes
Acknowledgements
Ethical Considerations
The study protocol was reviewed and approved by the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (No. 2022-0649-01, Date: 2022-11-12).
Consent to Participate
Informed consent was waived for all patients.
Author Contributions
This study was designed by YJ and SW. The experiments were planned, designed, and interpreted by YM, HX, XT and SW. Clinical information was gathered by ML, JX, YC and FW. The data were examined by HX, XT, SS, MY and SW. The manuscript was drafted by YM, XT, HX, and SS. All authors in the study had complete access to all of the data, and they are all accountable for the accuracy of the data analysis and the data’s integrity. After reading the first draft of the work, each author offered suggestions for changes.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Technology of the People’s Republic of China (CN): 2022YFF1203300, Hubei Province key research and development project (2022BCA016; 2023BCB146), the National Natural Science Foundation of China (No.82270110).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.