
Abstract
Introduction
The 3-degree-of-freedom (3DOF) and 6-degree-of-freedom (6DOF) couches can enhance the accuracy of tumor localization in radiotherapy. However, the relationship between rotational and translational error corrections remains unclear. This study aims to evaluate the setup errors of three common tumor types using cone-beam computed tomography (CBCT) and registration analysis, with a focus on elucidating the coupling between rotational and translational errors, to optimize setup correction strategies and provide data support for the clinical application of 3DOF correction.
Methods
A total of 46 patients with nasopharyngeal carcinoma (NPC), 48 with esophageal cancer(EC) and 23 with rectal cancer (RC) were enrolled in this cross-sectional study. For each patient, the pre-treatment CBCT images and planning CT images were registered offline using the same region of interest (ROI) and bony registration algorithm. Registration was performed in 3DoF and 6DoF modes, amounting to 1,720 registrations in total. The setup errors of registrations were analysed to investigate the relationship between rotational and translational deviations.
Results
Significant registration errors were found only in the vertical direction for NPC and EC patients (P < 0.05), but not for RC patients (P > 0.05). The linear vector directions (D3D for 3DoF and D6D for 6DoF) showed strong linear correlations to varying degrees, R2NPC = 0.597, R2EC = 0.798, R2RC = 0.781 (P<0.01). Strong coupling correlations were observed between rotational and translational errors, particularly at the NPC site (pitch vs. ΔVrt: r = - 0.893; yaw vs. ΔLat: r = 0.826), the EC site (pitch vs. ΔLng: r = 0.544) and the RC site (pitch vs. ΔVrt: r = - 0.579).
Conclusion
A site-specific coupling exists between rotational and translational errors. When rotational errors exceed threshold ranges, performing site-specific rotational adjustments followed by translation is requisite. This strategy significantly enhances radiotherapy precision and patient safety in non-6DoF environments.
Keywords
Introduction
In the last few years, technological developments in the medical field have been rapid and are continuously evolving. One of the most revolutionizing breakthroughs was the introduction of the Internet of Things (IoT) concept within medical practice, 1 especially in the field of radiation oncology, modern radiotherapy is characterized by the integration of multiple advanced technologies. Precise patient setup correction is a key element in the broader trend toward digital healthcare and precision image-guided therapy.2,3 Precise patient positioning is essential for the successful implementation of advanced contemporary radiotherapy modalities.4,5 Ultimately, the accuracy of target localisation directly affects treatment precision and influences clinical outcomes, particularly for volumetric modulated arc therapy (VMAT). Image-guided radiation therapy (IGRT) significantly improves overall accuracy by enabling precise alignment of planning CT images with pre-treatment localisation images, such as CBCT.6-10 This process is also critical for achieving dosimetric fidelity and defining the planning target volume (PTV) margins. Consequently, treatment couches offering 3DoF and 6DoF correction capabilities have been developed. However, these systems exhibit significant disparities in inherent positioning accuracy and correction potential.11-13
The 3DoF strategy, which only corrects translational errors (lateral [Lat: left-right], longitudinal [Lng: superior-inferior], and vertical [Vrt: anterior-posterior]), without regard for rotation. This approach frequently results in poor conformity and under-dosage (reduced D95%) in non-spherical or distal targets.14,15 Although 4DoF systems add yaw (rotation around vertical axis) correction, residual pitch (rotation around the lateral axis) and roll (rotation around the longitudinal axis) errors can still cause a reduction in the dose in elongated targets, such as during craniospinal irradiation. By contrast, the 6DoF approach uses full-freedom correction to align high-dose isodose lines precisely with anatomy. 13 This prevents organs at risk (OAR), such as the spinal cord, 16 from rotating into high-dose gradients. Crucially, this strategy significantly minimises residual geometric errors. According to the van Herk formula (M=2.5Σ+0.7σ), 17 the reduction in systematic and random errors with 6DoF correction effectively suppresses displacements caused by the rotational “lever-arm effect”. This enables PTV margins to be safely contracted from the traditional 3-5 mm to 1-2 mm, particularly in stereotactic body radiation therapy (SBRT) and stereotactic radiosurgery (SRS), maximising dosimetric fidelity and normal tissue sparing while ensuring clinical target volume (CTV) D95% coverage for 90% of patients,and for longer targets as well.18,19
The current literature often focuses on specific anatomical sites or isolated error analyses, failing to provide a comprehensive explanation of the coupling mechanism between residual rotational and translational errors. For example, the foundational work by Xu et al 11 on 6DoF correction for rectal cancer has yet to be validated in other anatomical regions. Similarly, studies by Cereno et al 12 and Ngangom et al 17 either lacked full integration of rotational components or provided only localised investigations. Furthermore, although Fu et al 18 examined multiple treatment sites, limitations remain. While some studies have explored compensating for roll and pitch errors by adjusting gantry and collimator angles (up to 3°/2° for nasopharyngeal and prostate VMAT), 20 concerns persist regarding the scope and precision of these methods. Moreover, the relationship between rotational and translational components has not been analysed sufficiently to formulate more rational and practical solutions.
This study aims to address existing gaps in the research literature by conducting a systematic analysis of setup errors in NPC, EC and RC patients. Patient alignment was performed using 3DoF and 6DoF strategies via CBCT registration. Furthermore, this investigation characterises the linear relationship between residual translational errors following 3DoF correction and the corresponding rotational deviations. It is anticipated that these findings will provide valuable evidence for optimising treatment couch selection and clinical workflows, particularly in settings with limited resources where 3DoF or 4DoF couches remain prevalent.
Methods
Patients
This retrospective study included 117 patients who were randomly selected and underwent VMAT for three distinct tumor sites between January 2020 and December 2022. The patient cohort was stratified into three groups:
NPC: 46 patients (mean age 49.87 ± 11.45 years; 34 males, 12 females)
EC: 48 patients (mean age 62.27 ± 8.05 years; 41 males, 7 females, upper-middle esophagus)
RC: 23 patients (mean age 64.30 ± 9.81 years; 15 males, 8 females)
The maximum, median, and minimum values for each group on the number of the registrations on each patient were as follows: NPC group—10, 7, and 4; EC group—10, 8.5, and 4; RC group—10, 7 and 4. All participants provided informed written consent for radiotherapy (This study received ethical approval from the appropriate institutional committee). Importantly, no modifications or interventions were made to the patients’ original treatment plans during the course of this study for RC and EC patients. For NPC patients, the treatment duration is relatively long, during which patients are required to adhere to dietary management and side effect control. However, some patients may experience weight loss during radiotherapy. When significant reductions in body contour are observed, it becomes necessary to replan the radiotherapy treatment. All patient details have been de-identified. The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2024.
CT Simulation Positioning
All patients were positioned in the supine position and immobilized using customized thermoplastic masks on carbon fiber couch tops (Orfit Industries, Belgium). EC patients received additional immobilization with 3D-printed arm fixtures while RC patients were additionally immobilized using a leg separator. CT simulation was performed with a Siemens large-bore CT simulator (Siemens, Germany), generating images with a resolution of 512 × 512 pixels and a pixel size of 1.27 mm × 1.27 mm. The slice thickness was set at 3 mm for NPC cases and 5 mm for both EC and RC cases.
Registration
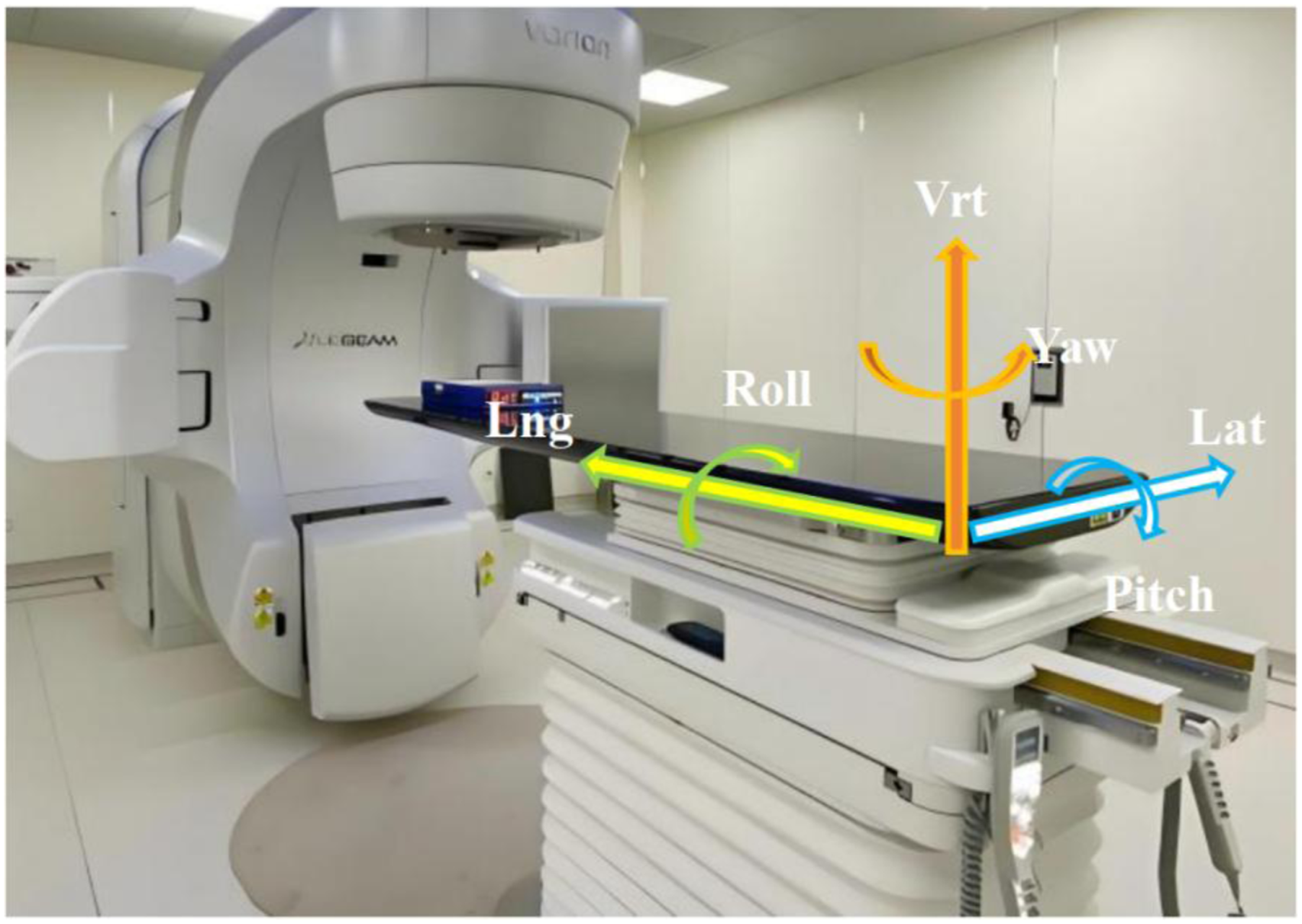
All treatment plans were developed using the Varian Eclipse treatment planning system (v15.6, Varian Medical Systems, USA) and delivered by Varian VitalBeam (Varian Medical Systems, USA) equipped with a 6DoF couch for comprehensive setup correction. CBCT was utilized for online positioning verification during the first three fractions, followed by weekly CBCT scans thereafter. The 6DoF available for couch-based setup correction are illustrated in Figure 1. • CBCT images acquired pre-treatment were registered to the planning CT using bony anatomy, with 3DoF and 6DoF auto matching, respectively. To maintain consistency and minimize the influence of region of interest (ROI) selection on mutual information-based registration algorithms,21,22 standardized ROIs were predefined for all patients within the same tumor site during offline registration procedures. In the course of the registration process, the NPC incorporated the following anatomical structures: the skull base, the sphenoid bone, the maxilla, the mandible and the cervical vertebrae. Conversely, the EC included the sternum, the ribs and the thoracic vertebral bodies. The RC encompassed the femoral neck, the proximal femur, the pubic symphysis, the pelvic ring, the sacrum and the lumbosacral junction. Coordinate diagram of 6DoF couch marked with translational and rotational axes. Lat (lateral: left - right), Lng (longitudinal: superior - inferior), Vrt (vertical: anterior - posterior), and roll (rotation around the longitudinal axis), yaw (rotation around vertical axis), and pitch (rotation around the lateral axis)
Both the 3DoF and 6DoF bony registrations were subsequently performed to quantify setup errors. Translational displacements were measured along the Lat, Lng, and Vrt axes, while rotational deviations were recorded as pitch, roll, and yaw. All resulting registration data were systematically documented and exported for subsequent statistical analysis.
Data Processing and Evaluation Criteria
Setup errors in radiotherapy and the relationships between rotational and translational directions were analyzed. Positional deviations derived from both registration methodologies are reported as mean ± standard deviation (SD). All linear data across three and six dimensions were subjected to normality and homogeneity of variance tests. Clinical action thresholds specific to tumor sites were defined for CBCT-based registration: translational tolerances were established at 3 mm for NPC, and 5 mm for both EC and RC along the Lat, Lng, and Vrt axes. A consistent rotational action threshold of 1.5° was maintained for pitch, roll, and yaw across all anatomical sites.
In secondary analysis, stricter translational tolerance criteria were applied—specifically, 2 mm for NPC and 4 mm for both EC and RC. To additionally evaluate the consistency and systematic patterns of the registration techniques, the proportion of treatment fractions demonstrating rotational errors beyond ±1.5° were quantitatively analyzed.
Three-Dimensional Linear Translation
A comparative analysis of translational deviations was performed between CBCT-guided 3DoF and 6DoF couches using bony registration. Displacements were quantified along the Lat (X-Lat), Lng (Y-Lng), and Vrt (Z-Vrt) axes. Additionally, the resultant three-dimensional vector displacement (Δd) was calculated according to Equation (1).

Differences in the translational components along the three principal axes (ΔX, ΔY, ΔZ) were computed, alongside the resultant 3D vector difference (ΔD).




The following nomenclature is adopted for positional deviations: (1) X3D and X6D denote the translational registration results in the lateral direction (Lat, or X-Lat) for 3D and 6D registrations, respectively, as defined in Equation (2). (2) Y3D and Y6D represent the translational registration results in the longitudinal direction (Lng, or Y-Lng) for 3DoF and 6DoF registrations, respectively, as defined in Equation (3). (3) Z3D and Z6D indicate the translational registration results in the vertical direction (Vrt, or Z-Vrt) for 3DoF and 6DoF registrations, respectively, as defined in Equation (4).
Δd3D and Δd6D signify the overall three-dimensional vector deviation (ΔD) for 3D and 6D registrations, respectively, calculated using the formula mentioned earlier, as defined in Equation (5).
Correlation Analysis Strategy
The correlation between translational vectors (D3D and D6D) obtained from the two registration methods was assessed using the Pearson correlation coefficient (PCC, denoted as r),
23
with a two-tailed P < 0.05 considered statistically significant. Linear regression was applied to variable pairs demonstrating strong correlations. Additionally, the relationship between rotational deviations (roll, pitch, and yaw) and translational differences following 6DoF registration was evaluated using PCC which has become rule of thumb in statistical teaching and practice. Correlation exhibits both positive and negative relationships. Consequently, a positive “r” value signifies a positive correlation, whereas a negative “r” value denotes a negative correlation. The strength of correlation was interpreted as follows: (1) Weak: 0 < |r| ≤ 0.4 (2) Moderate: 0.4 < |r| ≤ 0.7 (3) Strong: 0.7 < |r| ≤ 1.0
Linear regression was also conducted for rotational–translational variable pairs, which showed strong correlations.
Statistical Analysis
Statistical analysis was performed using SPSS software (version 27.0.1; IBM Corp., Armonk, NY, USA). All quantitative data are presented as mean ± standard deviation (SD). Data normality was assessed using histograms and probability-probability (P-P) plots, while homogeneity of variance was evaluated using Levene’s test. For group comparisons, independent samples t-tests were used when variance was homogeneous; otherwise, the rank-sum test was employed. Statistical significance was defined as a two-tailed P-value < 0.05.
Furthermore, positioning errors across the three anatomical sites were analyzed in relation to various tolerance ranges and rotational data magnitudes. To investigate these relationships, linear regression and Pearson correlation analyses were employed to assess: the association between rotational deviations(Angular deviation with and without rotation) and translational differences (Difference in linear translation between 3DoF correction and 6DoF correction), and the relationship between linear translational vector direction and rotational deviations. The reporting of this study conforms to the STROBE guidelines. 24
Results
Linear Direction Data Analysis
Translational and Rotational Setup Errors After Registration (Mean ± SD, t, P)

*Nasopharyngeal carcinoma (NPC), esophageal cancer (EC), and rectal cancer (RC).
According to t-test/P-value comparisons when comparing 3DoF vs 6DoF registration, NPC and EC patients showed statistically significant differences in the Vrt (P < 0.05), while no significant differences were observed in the Lng and Lat directions (P > 0.05). For RC patients, there were no significant differences in any of the three linear directions (P > 0.05).
Linear tolerance Analysis
The Percentage of Setup Errors Distribution in Translational Direction After Registration
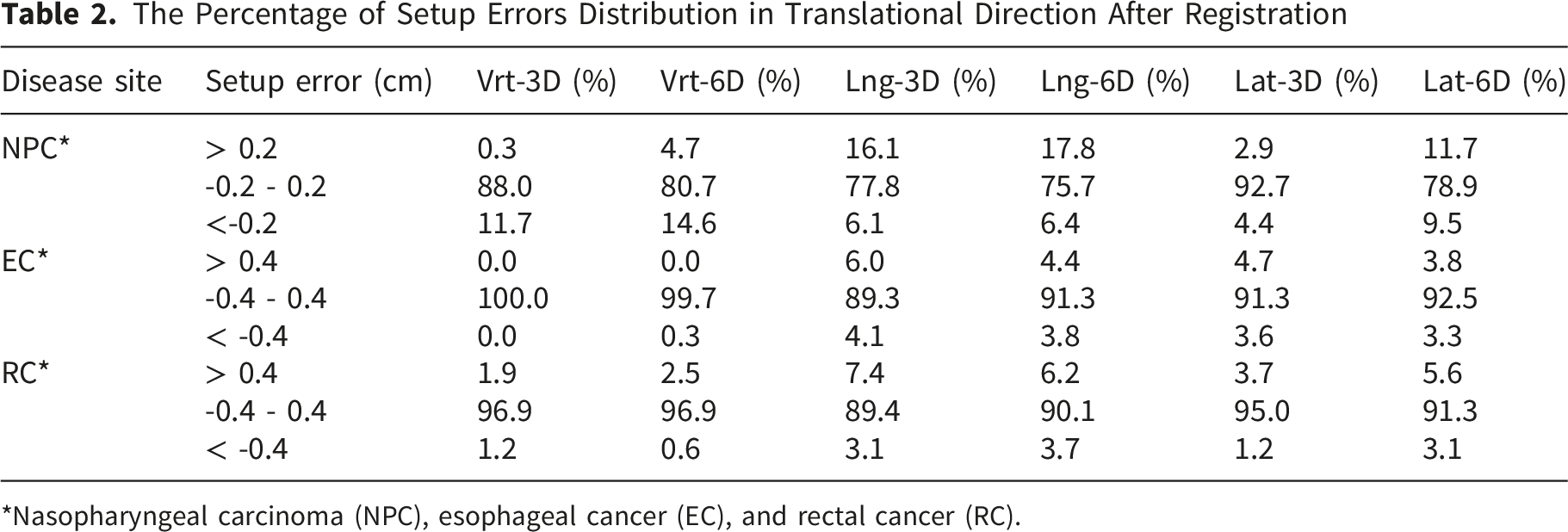
*Nasopharyngeal carcinoma (NPC), esophageal cancer (EC), and rectal cancer (RC).
Table 2 demonstrates that, following registration, the majority of setup errors in NPC patients were within the range of -0.2 cm to 0.2 cm, with both 3D and 6D couches exhibiting high positioning accuracy across all directions, especially laterally, with 92.7% for the 3D couch and 78.9% for the 6D couch. The proportion of errors greater than 0.2 cm in the longitudinal direction was slightly higher for the 6D couch compared to the 3D couch (17.8% vs. 16.1%), while the proportion of vertical errors less than -0.2 cm was higher for the 3D couch (11.7%) than for the 6D couch (14.6%). Overall, both 3D and 6D couches effectively controlled most setup errors within clinically acceptable limits; however, rotational correction resulted in subtle changes in error distribution.
For EC, the 6DoF registration demonstrated limited optimization. In the Lng and Lat directions, which had larger inherent deviations, the proportion of large errors (>0.4 cm) decreased compared to the 6DoF registration (Lng: 6.04% → 4.40%; Lat: 4.67% → 3.85%). This suggests that 6DoF registration may offer marginally better safety and stability for esophageal cancer.
For RC, the results were contradictory. The 6DoF registration reduced large errors in the Lng direction (7.45% → 6.21%) but increased them in the Lat direction (3.73% → 5.59%). This trade-off indicates that the net benefit of 6DoF registration regarding translational accuracy in rectal cancer may remain unclear.
Rotational Tolerance Analysis
A comparative analysis of the cumulative distribution function (CDF) plots in Figure 2 reveals four distinct characteristics. Overall magnitude: Rotational errors were generally minimal. All three pictures curves indicated that over 80% of registrations fell within ±2°, demonstrating a high level of positioning precision. Proportion of setup error distribution in the direction of rotation greater than 1.5° and less than -1.5° after registration for patients with nasopharyngeal carcinoma (NPC), oesophageal cancer (EC) and rectal cancer (RC)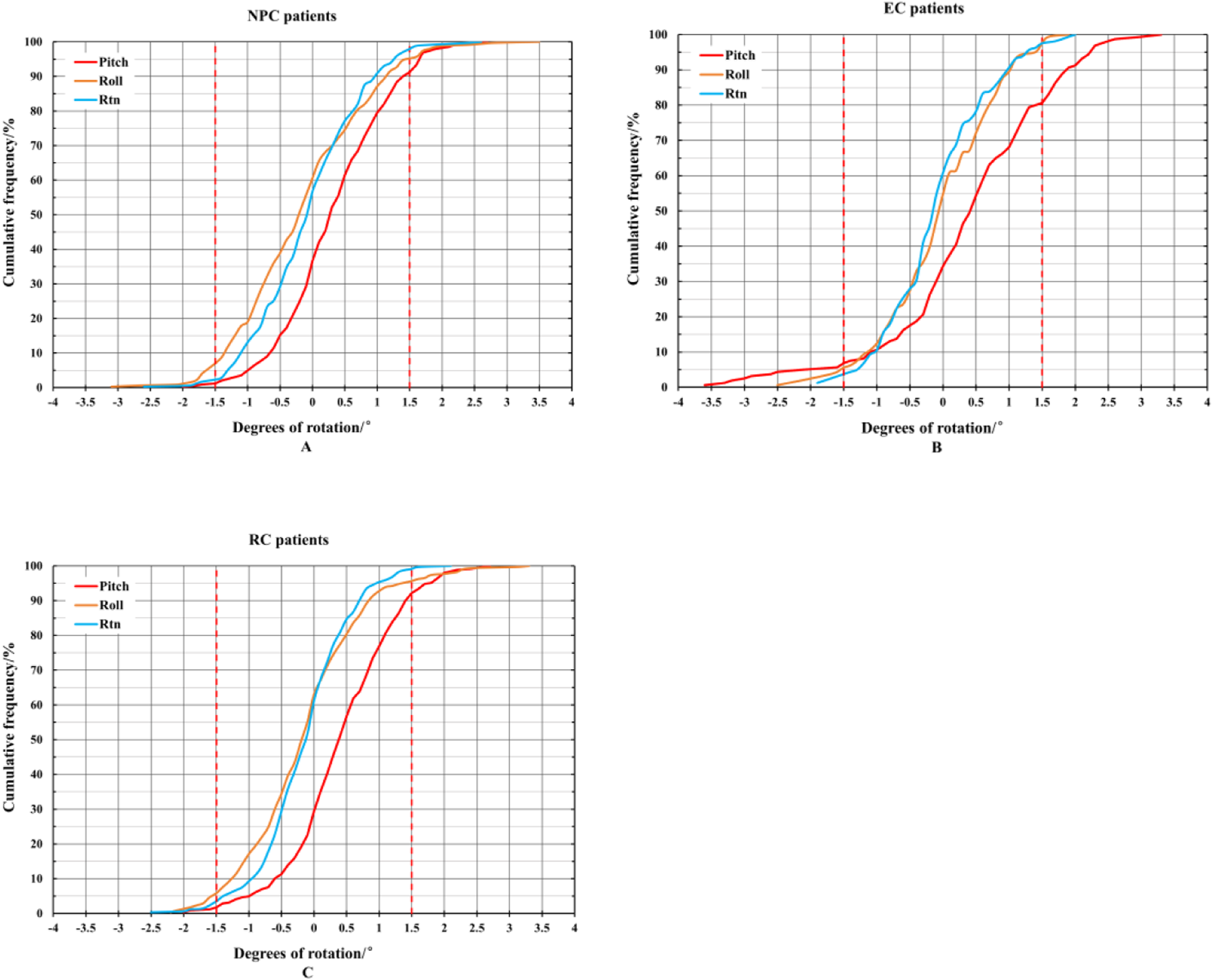
Anatomical gradient: A clear gradient in error magnitude was observed across anatomical sites. The steepness of the curves decreased sequentially from NPC (Figure A) to EC (Figure B) to RC (Figure C). Specifically, approximately 90% of NPC cases exhibited Pitch and Roll errors ≤1°, whereas this proportion decreased to 80% for EC and to 60–70% for RC. This suggests that rotational stability diminishes as the treatment site moves caudally from the head and neck to the pelvis.
Intra-site directional patterns: A consistent pattern of “Pitch ≈ Roll < Yaw” was evident. In the NPC and EC groups, the Pitch and Roll curves almost overlapped, while the Yaw curve shifted slightly to the right. For RC, the 80th percentile width for yaw was approximately 0.3–0.5° wider than for pitch or roll. This suggests that controlling rotation around the vertical axis (yaw) is most challenging, potentially due to external lasers having lower sensitivity for detecting pelvic rotation.
Threshold compliance: Significant disparities in compliance were noted at the 1.5° clinical action threshold. Approximately 98% of NPC fractions, 90% of EC fractions, and 75% of RC fractions remained within this limit. If a stricter 1° threshold were applied, however, compliance in the RC group would drop below 60%, necessitating the use of a 6DoF couch or more rigorous positioning protocols.
Correlation Between Rotational Deviations and Translational Discrepancies
A correlation analysis was conducted to investigate potential interdependencies between the linear translational discrepancies (from both registration methods) and the rotational angles (from the 6DoF registration). As presented in Table 3, the PCC analysis identified robust associations between particular rotational deviations and specific translational discrepancies. Specifically: (1) For NPC patients, pitch was strongly correlated with ΔVrt (r = -0.893, P < 0.01); roll was moderately correlated with ΔLat (r = 0.534, P < 0.01); and yaw was strongly correlated with ΔLat (r = 0.826, P < 0.01). (2) For EC patients, pitch was weakly and moderately correlated with ΔVrt and ΔLng (r = 0.397 and 0.544, respectively, P < 0.01); roll and yaw were weakly and moderately correlated with ΔLat (r = -0.310 and -0.444, respectively, P < 0.01). (3) For RC patients, pitch was moderately correlated with ΔVrt (r = -0.579, P < 0.01), and yaw was weakly correlated with ΔLat (r = 0.306, P < 0.01). The r and P Values of the Correlation Between Rotational and Translational Discrepancies *Nasopharyngeal carcinoma (NPC), esophageal cancer (EC), and rectal cancer (RC). Correlation exhibits both positive and negative relationships. Consequently, a positive ‘r’ value signifies a positive correlation, whereas a negative ‘r’ value denotes a negative correlation. The bolded numerical values in the table are used to highlight correlations, particularly strong correlations, for the reader’s notice.
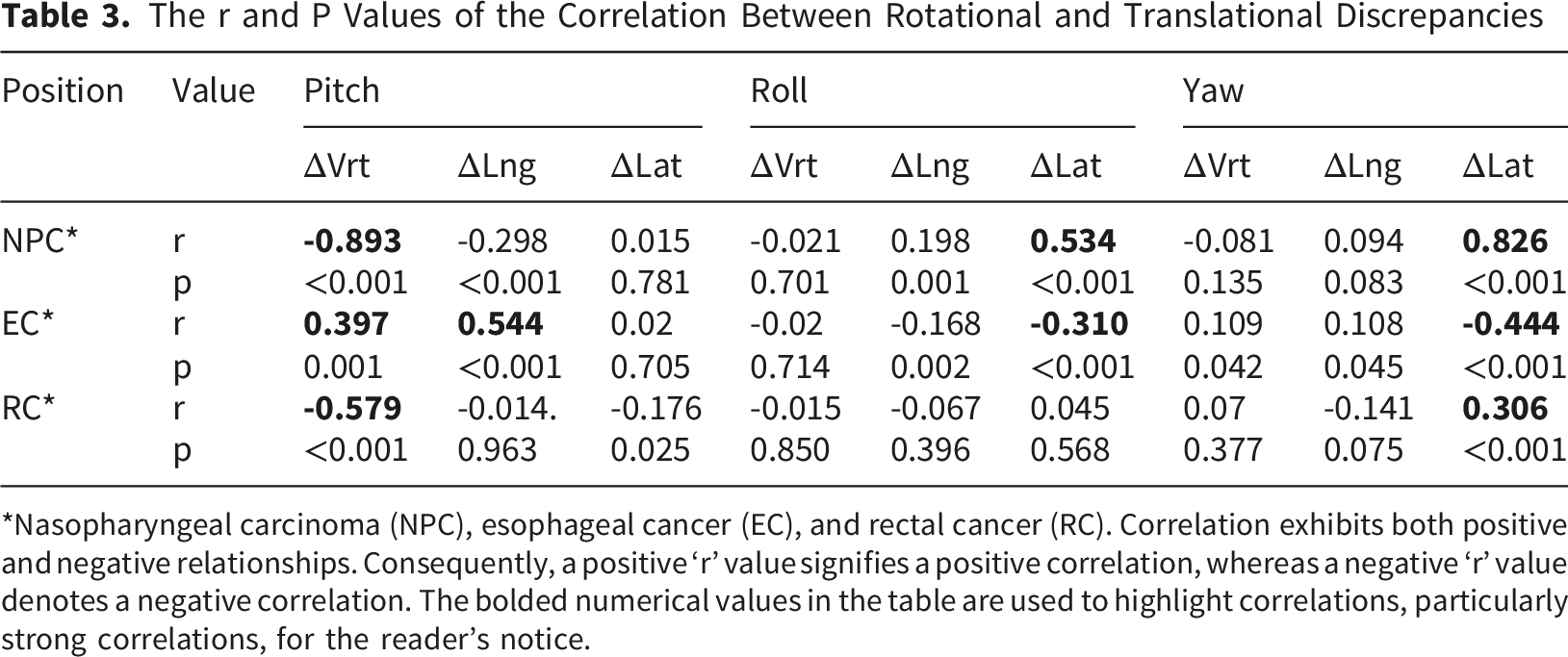
Pitch is the predominant consideration for RC and EC, but all three rotational parameters are relevant for NPC.
Linear Fitting Analysis for Linear Translation Vector Directions
The mean and standard deviation (SD) of the linear translation vector directions were calculated for patients across the three distinct cancer types, considering both the 3DoF couch (D3D) and the 6DoF couch (D6D) approaches. These results are presented in Figure 3. For all three anatomical sites, the linear translation vector magnitudes obtained from the two registration methods demonstrated considerable similarity, with no statistically significant differences observed (P > 0.05). A consistently strong linear correlation between D3D and D6D was observed across all cohorts (P < 0.01). Furthermore, linear fitting analysis was conducted on the vector direction data, as illustrated in Figure 4. In this analysis, the y-axis represents D6D and the x-axis represents D3D. The coefficient of determination (R2) serves as an indicator of fit quality: values approaching 1 signify an excellent fit, whereas values approaching 0 suggest a poor fit. (1) For NPC patients, the fitting equation was y = 6.72e-02+8.54e-01*x, with R2 = 0.597, indicating a moderate fit. (2) For EC patients, the fitting equation was y = 5.01e-02+8.57e-01*x, with R2 = 0.798, indicating a good fit. (3) For RC patients, the fitting equation was y = 6.22e-02+8.61e-01*x, with R2 = 0.781, indicating a good fit. Comparison of 3D vectors in D3D and D6D for patients with three anatomical sites (mean ± SD) and the analysis of linear relationships to the nasopharyngeal carcinoma (NPC) patients, esophageal cancer (EC) patients, and rectal cancer (RC) patients The linear fitting relationship between D3D and D6D in the vector direction of the linear translation to the nasopharyngeal carcinoma (NPC) patients, esophageal cancer (EC) patients, and rectal cancer (RC) patients
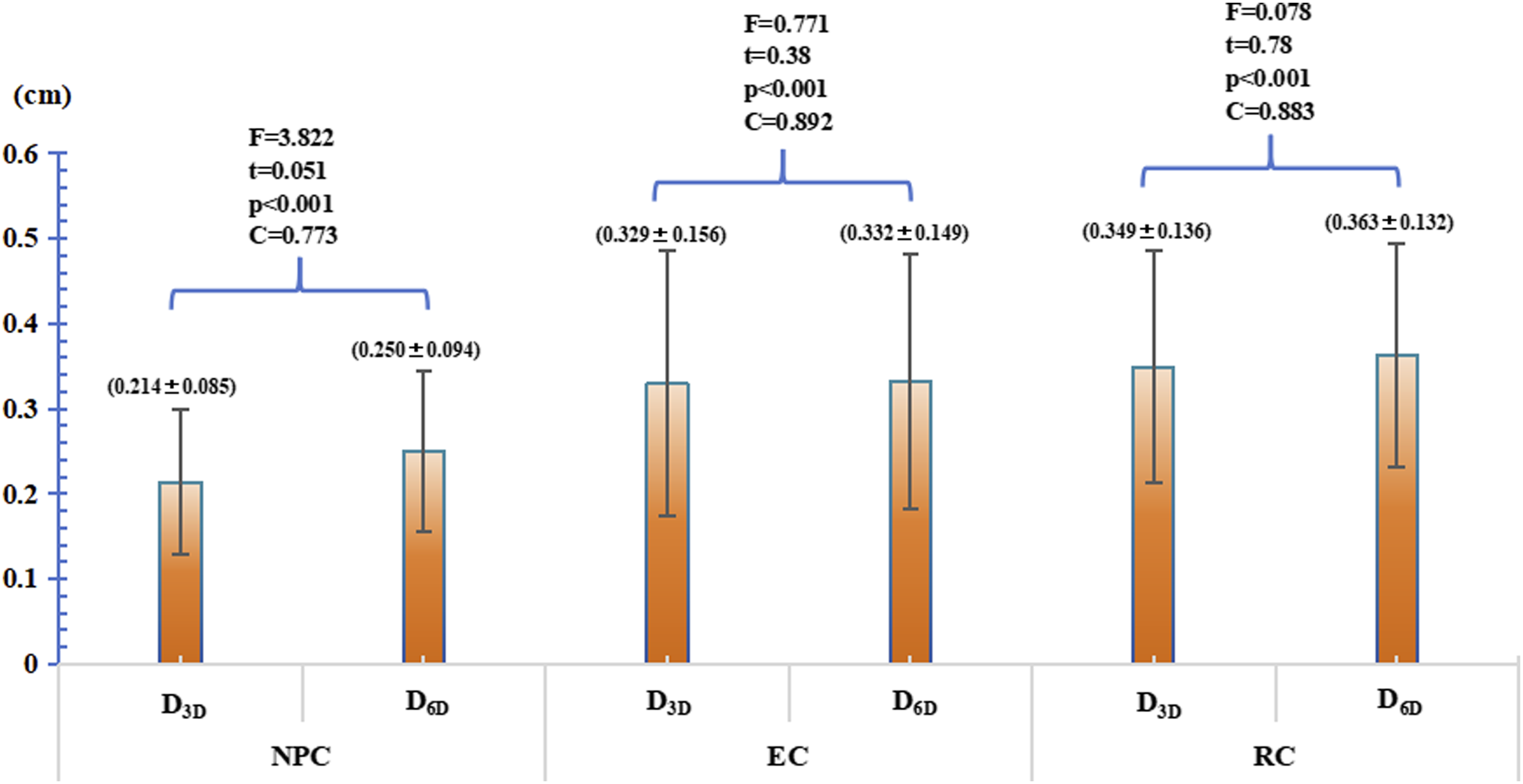
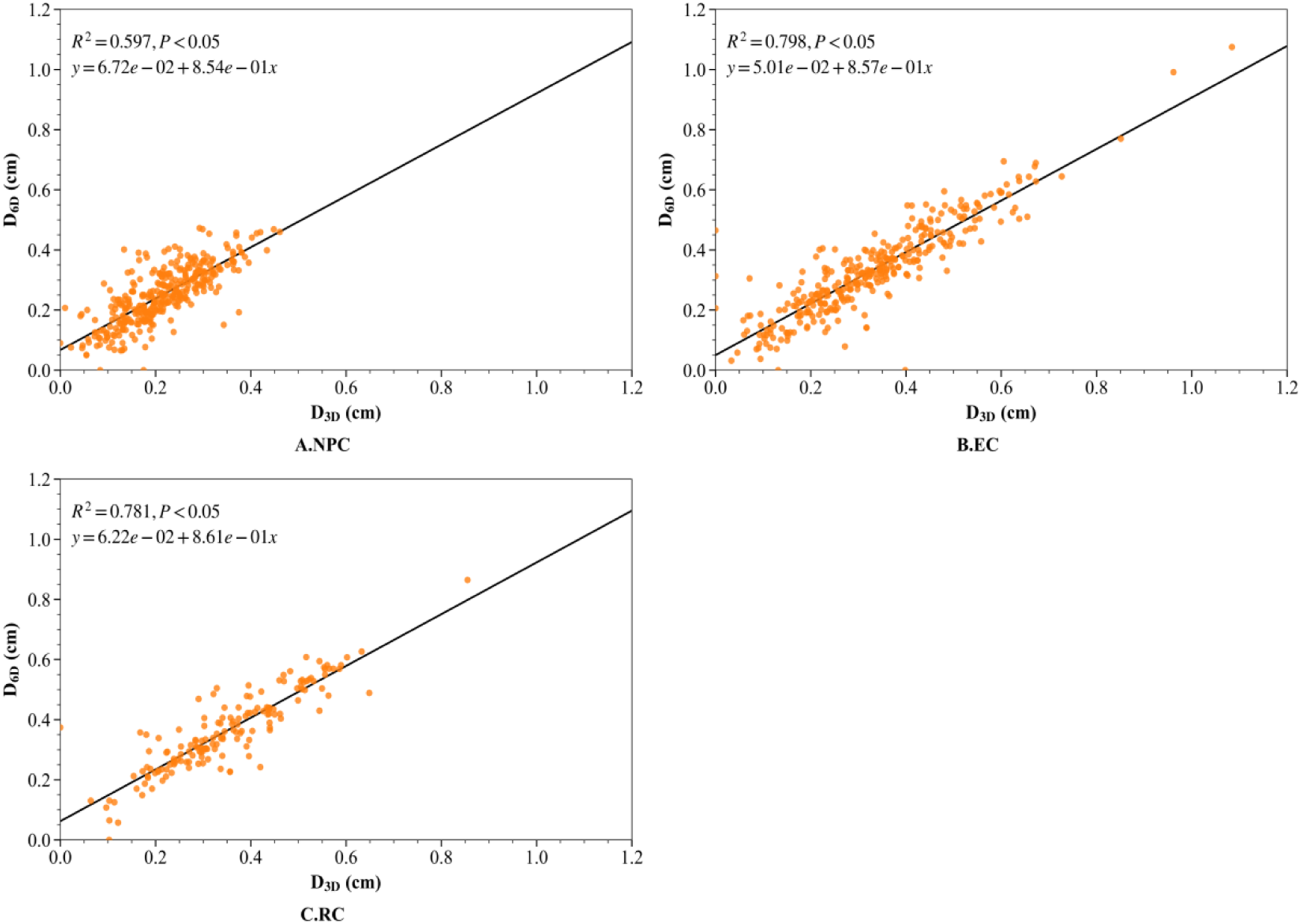
Similar linear patterns were observed in the linear translation vector directions for all three anatomical sites.
Linear Fitting Between Rotational Errors and Translational Deviation
Linear fitting was performed for the degrees of rotation and translational deviation with strong and moderate correlations, respectively.
For NPC patients, as shown in Figure 5A, the fitting equation for the degrees of rotation in the pitch direction(x) and the translational deviation in the Vrt direction (ΔVrt, y) was ΔVrt = 1.71e-03-9.01e-02*pitch, with R2 = 0.797, which is close to 1 and indicates a good fit. As shown in Figure 5B, the fitting equation for the degrees of rotation in the yaw direction(x) and the translational deviation in the Lat direction (ΔLat, y) was ΔLat = -4.67e-03+9.01e-02*yaw, with R2 = 0.729, indicating a relatively good fit. For EC patients, the fitting equation for the degrees of rotation in the pitch direction(x) and the translational deviation in the Lng direction (ΔLng, y) was ΔLng = 9.35e-03+4.20e-02*pitch, with R2 = 0.293 (Figure 5C), indicating a poor fit. For RC patients, the fitting equation for the degrees of rotation in the pitch direction (x) and the translational deviation in the Vrt direction (ΔVrt, y) was ΔVrt = -4.90e-03+-3.06e-02*pitch, with R2 = 0.260 (Figure 5D), indicating a poor fit. Based on the linear fitting and correlation analysis, it can be concluded that in NPC patients, the pitch direction is strongly correlated with the linear direction, whereas only weak correlations are found for RC and EC patients. The linear fitting relationship between rotational deviations and translational discrepancies after 3D and 6D registration in the nasopharyngeal carcinoma (NPC) patients, esophageal cancer (EC) patients, and rectal cancer (RC) patients.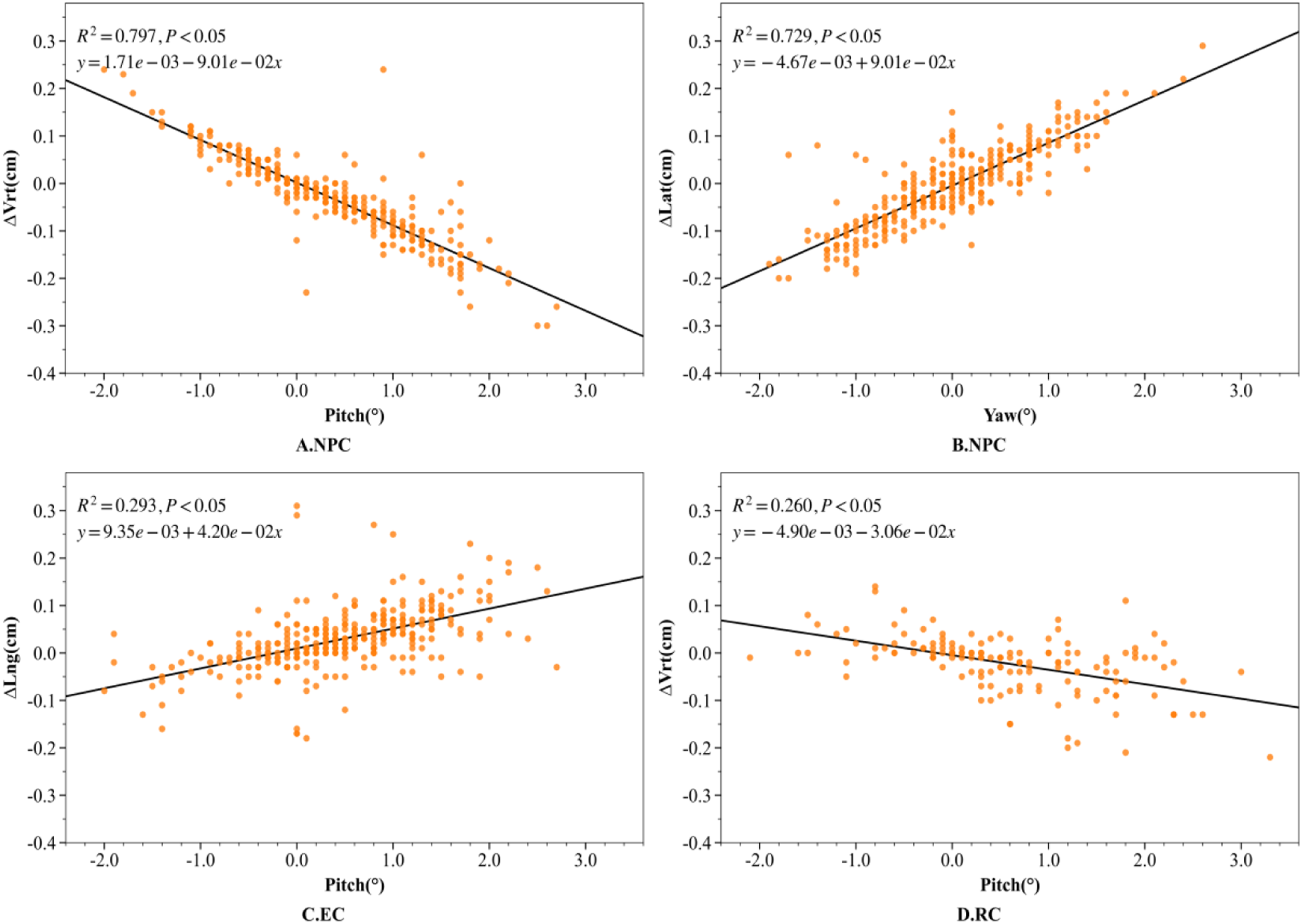
Discussion
This study conducted an in-depth analysis of rotational and linear setup errors for NPC, EC, and RC using both 3DoF and 6DoF CBCT-guided image registrations. The results first revealed distinct site-specific patterns and a coupling phenomenon between rotational errors and residual translational deviations.
Quantitative analysis demonstrated a highly significant negative correlation between rotational and translational errors in NPC (Pitch vs. ΔVrt, r = −0.893), which lends robust support to the “lever-arm effect” hypothesis proposed by Gutfeld et al. 25 Consistent with the findings of Graff P et al in head and neck radiotherapy, 26 the data suggests that rigid-body registration algorithms may misinterpret rotations as translational shifts when the anatomical center of rotation deviates from the treatment isocenter. Consequently, neglecting rotational corrections in a 3DoF protocol does not constitute a valid approximation but instead introduces substantial geometric inaccuracies. In contrast, the weak correlation observed in the EC cohort aligns with the principles of CBCT soft-tissue registration outlined by Sonke et al, 27 wherein pronounced non-rigid deformations and respiratory motion artifacts in the thorax attenuate simple geometric relationships. Although the pattern of pelvic tilt in the RC group corresponded to that reported by White et al, 28 the clinically relevant vertical displacements induced by even minor Pitch rotations underscore the inherent limitations of rigid-body algorithms in semi-rigid anatomical regions.
This geometric coupling carries direct dosimetric implications. As highlighted by Graff P et al 26 and Delishaj et al 29 uncorrected rotations can displace dose gradients relative to organs at risk (OARs). Thus, while a 3DoF correction may appear to improve image registration indices, it may inadvertently introduce a “shearing misalignment” of the target volume.
Although 6DoF correction represents the ideal solution, the findings demonstrate that in the widely used 3DoF mode, disregarding rotational errors results in significant deviations in translational correction values.
Among all sites, NPC exhibited the most pronounced rotational-translational coupling, particularly the negative correlation between Pitch and ΔVrt (r = −0.893) and the positive correlation between Yaw and ΔLat (r = 0.826). Mechanistically, this is attributed to the rigid nature of the skull base and cervical spine. Specifically, the pivot offset—defined as the distance between the actual rotation axis (often near the cervical fulcrum or foramen magnum) and the isocenter—compels the rigid algorithm to generate a fictitious vertical displacement to fit the bony landmarks when a Pitch error occurs. If only 3DoF correction is applied, this mathematical compensation results in a physical displacement of the target away from the planned position, potentially shifting high-dose regions into critical structures such as the brainstem or optic chiasm.
Unlike NPC, registration in EC and RC is significantly confounded by non-rigid deformation. In the RC group, the correlation between Pitch and ΔVrt reflects pelvic tilt driven by variations in bladder or rectal filling, which is frequently misinterpreted by algorithms as vertical shifts. Conversely, the correlation in the EC group is weaker (r= 0.397) because thoracic non-rigidity, respiratory motion artifacts, and mediastinal deformation attenuate the propagation of errors in a linear manner. Therefore, predicting error propagation based solely on geometric models is less reliable for EC patients compared to NPC or RC cases.
These findings challenge the conventional assumption that 3DoF translation can partially compensate for rotation, suggesting instead that when rotation exceeds a certain threshold (e.g., 1.5 ∘), pure translational correction may introduce systematic geometric errors.
In light of the strong geometric correlations observed, we propose a ‘Stratified Hybrid Correction Strategy’ for institutions with 3DoF correction capabilities only. This strategy is employed when CBCT-derived rotational errors, notably pitch or yaw, exceed 1.5-2°. The following protocols are recommended for tolerance: NPC: Priority is given to manually adjusting cervical lordosis, mandibular tilt, and thoracic posture to correct pitch, while couch rotation is used to rectify yaw deviations. EC: Pitch magnitude is mitigated through respiratory motion management and strict adherence to dietary protocols. RC: Setup optimisation focuses on reproducing bladder and rectal filling, ensuring pelvic alignment and promoting patient muscular relaxation.
The rationale is to suppress rotation below the tolerance threshold, thereby severing the error propagation pathway to translational shifts, prior to executing residual linear corrections. This strategy circumvents target misalignment caused by algorithmic compensation for uncorrected rotations.
Image-guided correction with 3D and 6D couches improves patient setup accuracy in radiotherapy, supporting the view of Anagnostopoulos et al 2 that high-precision spatial mapping is essential for clinical 3D printing. Mulita et al3,30 also showed that accurate spatial calibration allows multimodal imaging, such as positron emission tomography/computed tomography (PET/CT), to optimize treatment planning and target delineation. Therefore, correcting setup errors is fundamental for integrating advanced imaging, modeling, and precise radiotherapy.
This study has certain constraints. Firstly, the analysis relied solely on rigid registration algorithms, disregarding elastic (deformable) variations, which constitutes a key limitation, as rigid registration cannot account for anatomical deformations such as tumor shrinkage, organ motion, or positioning changes. In regions subject to significant non-rigid changes, this may result in residual alignment errors and suboptimal dose delivery. Therefore, future studies should incorporate deformable registration techniques to better address anatomical variability and improve clinical accuracy. Secondly, the scope was confined to geometric positional discrepancies. Future investigations should incorporate Monte Carlo dose reconstruction to quantify the precise dosimetric consequences of residual rotational errors and guide the refinement of setup optimisation protocols. The study has a relatively small sample size, which may affect the generalizability and statistical power of the results. Future studies with larger cohorts are needed to confirm and extend the findings.
Conclusion
Rotational errors may induce site-specific coupling with translational shifts through the lever-arm effect. Therefore, in non-6DoF environments, it may be beneficial to establish anatomically stratified error management protocols with defined rotational thresholds. Prioritizing rotational correction before translation when errors exceed these limits could help minimize coupled errors. This approach has the potential to enhance geometric accuracy and patient safety, and may provide practical guidance for clinical radiotherapy positioning.
Footnotes
Acknowledgment
This work was supported by the corresponding author and other authors. At the same time, sincerely thank for their guidance and help on this article.
Ethical Considerations
This study was approved by the Ethics Committee of Beijing Cancer Hospital (also known as Peking University Cancer Hospital & Institute, and Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing)), e.g., with approval number 2020KT12 on March 10, 2020. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from all participants included in the study.
Author Contribution
All authors approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Beijing Natural Science Foundation (No. 1202009), Sichuan Provincial Science and Technology Achievement Transfer and Transformation Guidance Program (No. 24ZHSF0072), Sichuan Provincial Key Research and Development Program (No. 25QYCX0359), and the Deyang Science and Technology Plan Project (No. 2023SZZ094).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Generative AI and Large Language Models
The content of this paper was authored by the authors. Gemini was used for refining the language and expression, and ChatGPT was employed for grammar correction.