
Abstract
Introduction
Severe bone marrow suppression (BMS) is a frequent and dose-limiting toxicity in esophageal cancer treated with chemoradiotherapy. A simple pre-treatment tool is needed to identify high-risk patients.
Methods
In this single-center retrospective cohort study, we analyzed 404 patients receiving radiotherapy or chemoradiotherapy between February 2022 and July 2025. Severe BMS, defined per CTCAE v5.0, was predicted using variables selected by LASSO and multivariable logistic regression to construct a nomogram. Model performance was evaluated by discrimination (AUC/C-index), calibration, and decision-curve analysis in training and test cohorts.
Results
Among 404 patients, 143 developed severe BMS (35.4%). Multivariable analysis identified sex, age, N stage, Pre-ALB, creatinine, and platelet count as independent predictors. Given their clinical relevance, radiotherapy regimen and overall treatment approach were retained in the final model. In this dataset, the nomogram showed strong discrimination, with an AUC of 0.972 (95% CI, 0.941–0.988) in the training set and 0.956 (95% CI, 0.932–0.983) in the internal test set. Calibration was close to the observed risk, with mean absolute errors of 0.011 in the training cohort and 0.037 in the testing cohort; the Hosmer–Lemeshow test showed no significant evidence of poor fit in either cohort (training cohort, P=0.512; testing cohort, P=0.738). Decision-curve analysis suggested potential net benefit within the internal validation framework across threshold probabilities of 0.10–0.80 in the training set and 0.10–0.70 in the testing set.
Conclusion
We developed and internally validated a nomogram based on routine clinical and laboratory measures to estimate the risk of severe BMS before radiotherapy or chemoradiotherapy in esophageal cancer. This tool may help identify patients at higher risk before treatment and may support risk stratification, closer monitoring, and supportive care planning. Prospective, multicenter studies are warranted to further evaluate the generalizability of these findings.
Introduction
Esophageal cancer arises from the esophageal epithelium and is classified mainly as esophageal squamous cell carcinoma (ESCC) or esophageal adenocarcinoma (EAC). 1 In 2020, an estimated 600,000 new cases and more than 500,000 deaths occurred worldwide. 2 China bears roughly half of the global incidence and mortality, with ESCC accounting for about 90% of cases; national rates far exceed the global average, posing a major public health challenge.3,4 Because early symptoms are nonspecific, most patients present with locally advanced or metastatic disease, limiting surgical options. Consequently, radiotherapy or concurrent chemoradiotherapy (CCRT) is recommended as standard care for locally advanced disease in major guidelines. 5 Treatment, however, commonly leads to toxicity, with bone marrow suppression being both frequent and clinically important. 6 Thoracic irradiation exposes substantial active marrow, and cytotoxic chemotherapy further suppresses hematopoiesis; together, these effects markedly increase the risk of severe marrow suppression. Such toxicity can force treatment interruptions or dose reductions, compromise tumor control, and elevate the risks of infection, bleeding, and hospitalization, adversely affecting survival and quality of life.7,8
Most studies of CCRT for esophageal cancer emphasize radiation esophagitis, radiation pneumonitis, or cardiotoxicity, while hematologic toxicity has received less attention. Prior reports suggest that low serum albumin—reflecting poor nutritional reserve—raises the risk of marrow suppression,9,10 and that lymphopenia and more intensive regimens are additional independent risk factors.11,12 Yet many of these studies rely on small samples or univariable analyses and lack rigorously developed and validated risk models. Although dosimetric models have provided valuable mechanistic insights into radiation-related marrow injury, their routine clinical use may be limited by the need for marrow contouring, dose-volume histogram extraction, radiotherapy plan export, and specialized post-planning calculations. These requirements reduce their feasibility for rapid pretreatment risk assessment, especially when clinicians and nursing teams need a simple tool based on routinely available data. In particular, large cohort data from Chinese populations on predicting severe marrow suppression during CCRT remain scarce. This gap makes it difficult for clinicians and nursing teams to identify high-risk patients before treatment and to plan tailored management, limiting adherence strategies, resource allocation, and complication prevention.
To address this practical unmet need, our study introduces four advances: (1) the first large-scale, systematically developed model to predict severe marrow suppression in a high-incidence region of central China; (2) incorporation of renal function (creatinine) into the predictor set, filling a gap in evidence linking kidney function to hematologic toxicity; (3) integration of multidimensional indicators—nutritional status, hematopoietic reserve, tumor burden, and treatment factors—into a comprehensive risk framework; and (4) a user-friendly nomogram for pre-treatment risk estimation based on routinely available clinical data. Our goal is to develop an internally validated risk-estimation tool that may help identify patients at higher risk before treatment and may support closer monitoring and supportive-care planning, pending external validation.
Methods
This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cohort studies. 13
Patient Selection
This single-center retrospective cohort study consecutively screened all patients with esophageal cancer treated with radiotherapy or concurrent chemoradiotherapy in the Department of Radiation Oncology, First Affiliated Hospital of Zhengzhou University, from February 2022 to July 2025. All eligible patients who met the predefined inclusion and exclusion criteria were included in the analysis. Eligibility criteria were: (1) histologic or cytologic confirmation of esophageal cancer (squamous cell carcinoma, adenocarcinoma, or other subtypes) according to the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Esophageal and Esophagogastric Junction Cancers (Version 2.2026) 14 and the ESMO Clinical Practice Guidelines 15 ; (2) clinical staging per the 8th edition AJCC/UICC TNM system 16 ; (3) age ≥18 years with no prior radiotherapy, chemotherapy, targeted therapy, or immunotherapy; and (4) complete clinical records. Exclusion criteria were: (1) Barthel Index <60; (2) completion of <50% of the planned radiotherapy dose; (3) concurrent hematologic diseases; (4) severe cardiac, hepatic, renal dysfunction, or psychiatric disorders; and (5) missing clinical or follow-up data.
Hematologic data were retrieved from the electronic medical record. Baseline (pre-treatment) measures included serum albumin (ALB), hemoglobin (Hb), white blood cell count (WBC), platelet count (PLT), and creatinine (Cr). During treatment, weekly laboratory monitoring was summarized across the full radiotherapy course (weeks 1–6), including WBC, neutrophils (NEU), Hb, and PLT. For patients who discontinued early due to disease progression, adverse events, or other reasons, data were collected up to the time treatment stopped. All included cases had complete baseline data and at least one set of on-treatment hematologic measurements.
We identified 1,247 patients treated in our department between February 2022 and July 2025. After applying exclusions—Barthel Index <60 (n=89), <50% of planned radiotherapy delivered (n=156), hematologic disease (n=78), severe cardiac/hepatic/renal dysfunction or psychiatric disorders (n=298), and missing clinical or follow-up data (n=222), 404 patients met all criteria and were included in the analysis. The selection process is shown in Figure 1. Flowchart of patient selection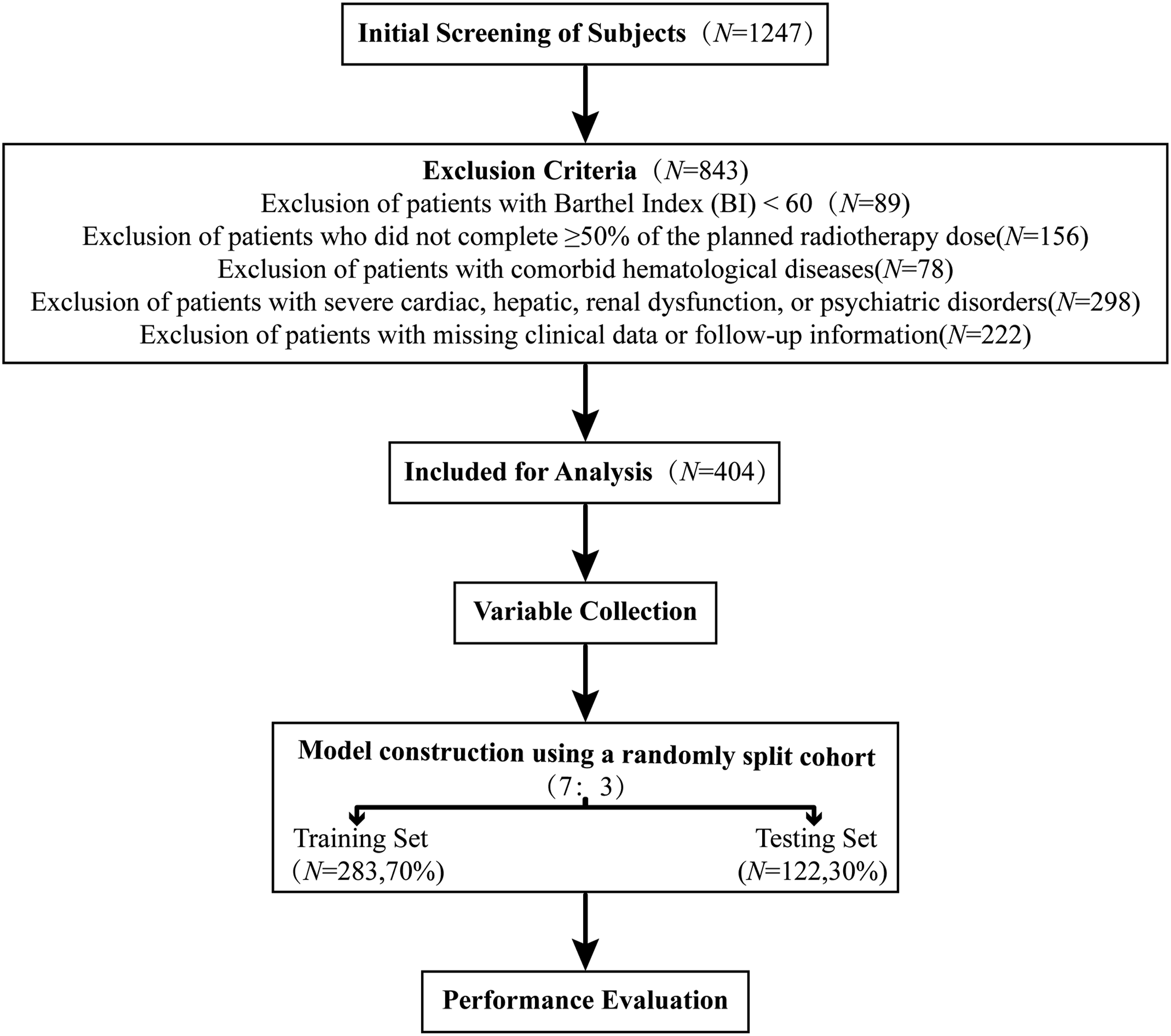
Sample Size Estimation
To ensure adequate events for model development, we estimated the required sample size using the rule of at least 10 outcome events per predictor in multivariable logistic regression. Assuming 5–7 predictors, we targeted ≥50 events of severe bone marrow suppression. With an anticipated incidence of ∼25%, 17 the minimum cohort size was ∼200 patients. Allowing for ∼20% loss to follow-up or attrition, 18 we aimed to enroll ≥250 patients. We ultimately included 404 patients, meeting and exceeding the requirement.
Ethical Approval
This retrospective study was approved by the Ethics Committee of First Affiliated Hospital of Zhengzhou University (Approval No. 2025-KY-1517-002; approval date: October 25, 2025). The study was conducted in accordance with the Declaration of Helsinki, as revised in 2024. Given the retrospective design, all patient details were de-identified before data extraction and analysis, and no information that could reveal the identity of any individual was retained in the study dataset. The study used de-identified data from the hospital’s electronic medical record system; therefore, the requirement for written informed consent was waived by the Ethics Committee.
Data Collection
We developed a standardized case report form based on literature review and expert input, reviewed by two senior radiation oncologists and two oncology nursing experts to ensure completeness and rigor.
19
Clinical data were obtained from the electronic medical record, laboratory information system, and radiotherapy treatment records. Two trained researchers independently extracted and cross-checked all variables; discrepancies were resolved by a third investigator. Key variables are summarized below. 1) Demographics and general characteristics: age, sex, body mass index, smoking and alcohol history, and comorbidities (hypertension, diabetes, coronary heart disease) collected from admission records. 2) Tumor characteristics: histology (e.g., squamous cell carcinoma, adenocarcinoma) confirmed by pathology reports; TNM stage assigned per AJCC 8th edition by two independent radiologists using CT, MRI, or PET-CT. 3) Laboratory measures: complete blood count—WBC, neutrophils (NEU), hemoglobin (Hb), and platelets (PLT)—measured with an automated hematology analyzer (Mindray BC-6800Plus). Samples were fasting peripheral venous blood obtained within one week before treatment and then weekly during weeks 1–6 of radiotherapy. Serum albumin (ALB), creatinine (Cr), carcinoembryonic antigen (CEA), and creatine kinase (CK) were assessed using a fully automated biochemical analyzer (cobas 6000 series, Roche). These biochemical tests were completed within one week before treatment initiation. 4) Radiotherapy: patients received 3D-CRT or IMRT using a linear accelerator (Varian, USA) with 6-MV X-rays. Target delineation followed ICRU recommendations and national guidelines for esophageal cancer. Regimens were categorized as: (a) PGTV-only irradiation—limited to gross disease for patients with severe comorbidity, poor performance, or palliative intent; typical dose 50–60 Gy in 25–30 fractions (2.0–2.4 Gy/fraction). (b) PTV-only irradiation—conventional fields expanded from CTV to PTV; typical dose 40–50 Gy in 20–25 fractions (1.8–2.0 Gy/fraction) to cover potential subclinical disease. (c) Simultaneous integrated boost (PGTV+PTV, SIB)—standard PTV dosing with an additional boost to PGTV; typical prescriptions PGTV 60–66 Gy in 28–30 fractions (2.0–2.2 Gy/fraction) and PTV 50–54 Gy in 28–30 fractions (1.8 Gy/fraction). All parameters were exported from the radiation oncology electronic system and manually verified. 5) Systemic therapy categories were defined according to the NCCN Guidelines for Esophageal and Esophagogastric Junction Cancers (Version 2.2026) and related clinical guidelines, and were further specified as follows: first-line treatment mainly included platinum-based fluoropyrimidine regimens, with PD-1 inhibitor added when clinically indicated; second-line treatment mainly included PD-1 inhibitor monotherapy or other guideline-recommended salvage systemic regimens selected according to prior treatment history and biomarker status; and no systemic therapy referred to patients treated with radiotherapy alone without concurrent chemotherapy or immunotherapy. Data were exported from departmental records and verified. 6) Assessment of bone marrow suppression: hematologic toxicity was graded per CTCAE v5.0; grades 3–4 defined severe suppression
20
and were classified as the primary outcome. In this study, severe bone marrow suppression operationally comprised severe leukopenia, severe anemia, and/or severe thrombocytopenia during treatment. The assessment window was the first 6 weeks after treatment initiation (acute phase). CBCs were obtained weekly at weeks 1–6. An event was recorded if any on-treatment value met criteria for severe toxicity (WBC < 2.0×109/L, or Hb < 80 g/L, or PLT < 50×109/L). These components are clinically important because they may increase the risks of infection, bleeding, treatment interruption, and the need for supportive interventions. The analysis focused on treatment-related acute toxicity and did not include late or chronic marrow dysfunction.
Statistical Analysis
All analyses were performed in R (version 4.4.1, R Foundation for Statistical Computing, Vienna, Austria). The 404 patients were randomly split 7:3 into a training set (n=282) and a testing set (n=122), following Harrell’s recommendations for prediction model validation 21 to ensure adequate data for model building and a sufficiently large test set for reliable evaluation. For continuous variables, normality was assessed with the Shapiro–Wilk test; normally distributed data were compared with independent-samples t tests, and non-normal data with the Mann–Whitney U test. Categorical variables were compared using the χ2 test or Fisher’s exact test when expected counts were <5. For model development, candidate predictors were selected using least absolute shrinkage and selection operator (LASSO) with 10-fold cross-validation, choosing the λ that minimized mean squared error. Multivariable logistic regression was then fitted. Variance inflation factors (VIFs) were calculated to assess collinearity, and variables with VIF >10 were removed. Radiotherapy regimen and systemic treatment were retained in the final model despite P>0.05 because of strong biological plausibility and clinical relevance. A nomogram was constructed from the final model. Discrimination was evaluated using Harrell’s concordance index (C-index) and the area under the ROC curve (AUC); calibration was assessed using bootstrap calibration curves based on 1,000 resamples, mean absolute error, and the Hosmer–Lemeshow goodness-of-fit test; and potential net benefit across threshold probabilities was assessed using decision-curve analysis. For the Hosmer–Lemeshow test, patients were grouped by deciles of predicted risk, and P>0.05 was considered to indicate no significant evidence of poor fit. Missing data were handled with mean imputation when <5% and multiple imputation when 5–20%. All tests were two-sided, with P<0.05 considered statistically significant. All P-values were reported to three decimal places, except that values less than 0.001 were reported as P<0.001.
Results
Baseline Characteristics
Baseline Characteristics of Esophageal Cancer Patients by Severe Myelosuppression Status
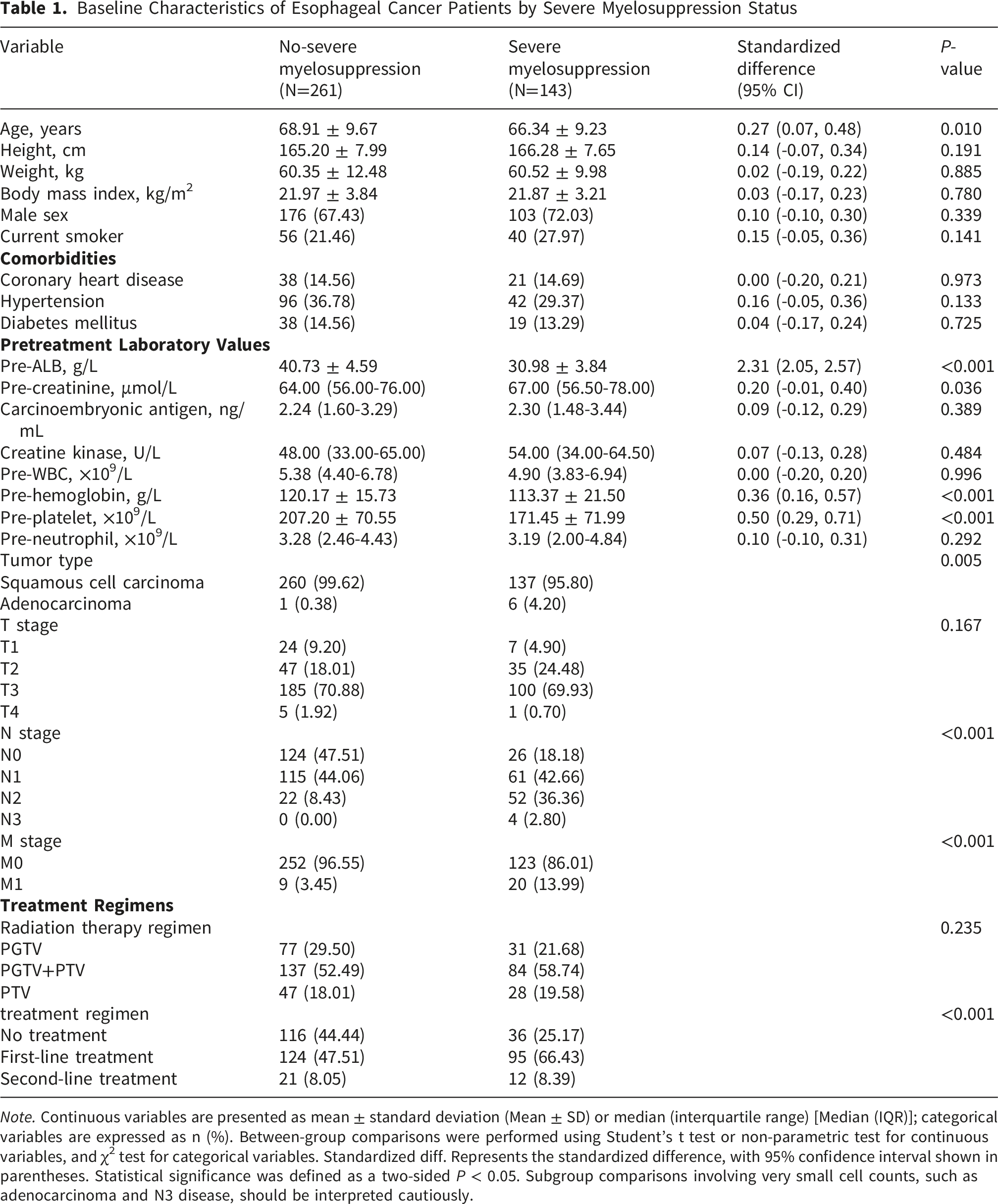
Note. Continuous variables are presented as mean ± standard deviation (Mean ± SD) or median (interquartile range) [Median (IQR)]; categorical variables are expressed as n (%). Between-group comparisons were performed using Student’s t test or non-parametric test for continuous variables, and χ2 test for categorical variables. Standardized diff. Represents the standardized difference, with 95% confidence interval shown in parentheses. Statistical significance was defined as a two-sided P < 0.05. Subgroup comparisons involving very small cell counts, such as adenocarcinoma and N3 disease, should be interpreted cautiously.
LASSO Selection and Multivariable Logistic Analysis
In the training set, candidate predictors were filtered using LASSO. Figure 2A shows coefficient shrinkage across values of the penalty parameter λ. As shown in Figure 2B, model deviance was minimized at λ_min; using the “1-SE” rule produced a more parsimonious set. To balance performance and simplicity, we proceeded with variables at λ_min (λ=6.47×10−4). We then assessed multicollinearity and excluded any variable with VIF>10 before fitting the multivariable logistic model. LASSO regression analysis for variable selection. (A): LASSO coefficient profiles of candidate predictors; (B): Tenfold cross-validation curve for selecting the optimal penalty parameter (λ)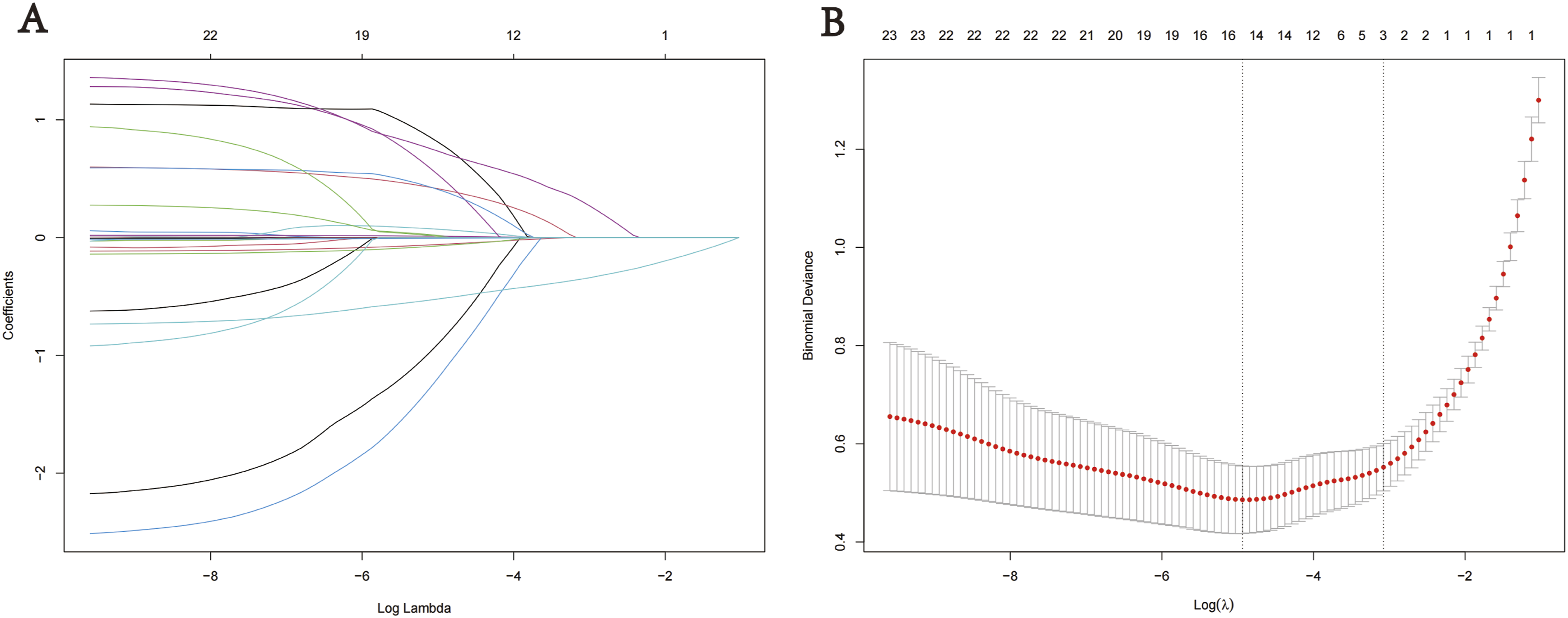
Results of Multivariable Logistic Regression Analysis
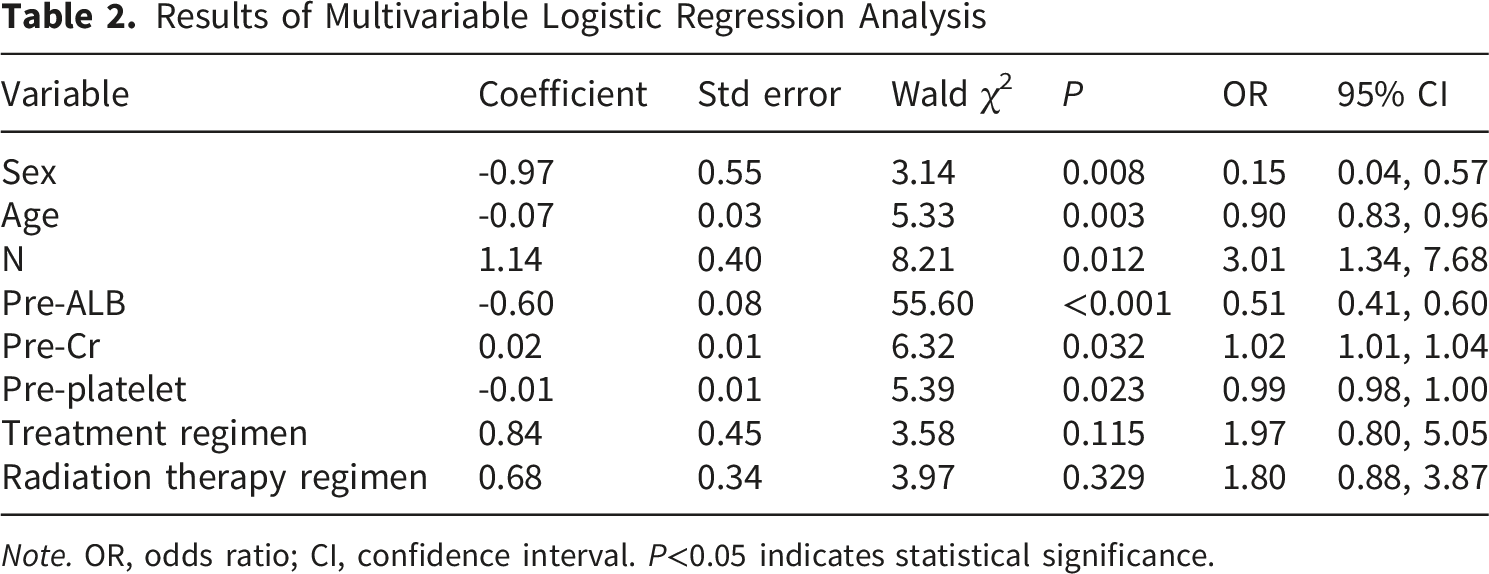
Note. OR, odds ratio; CI, confidence interval. P<0.05 indicates statistical significance.
Comparison of Model Variables Between Training and Test Cohorts After Chemoradiotherapy
Baseline Characteristics of Patients Stratified by Training and Testing Set Group
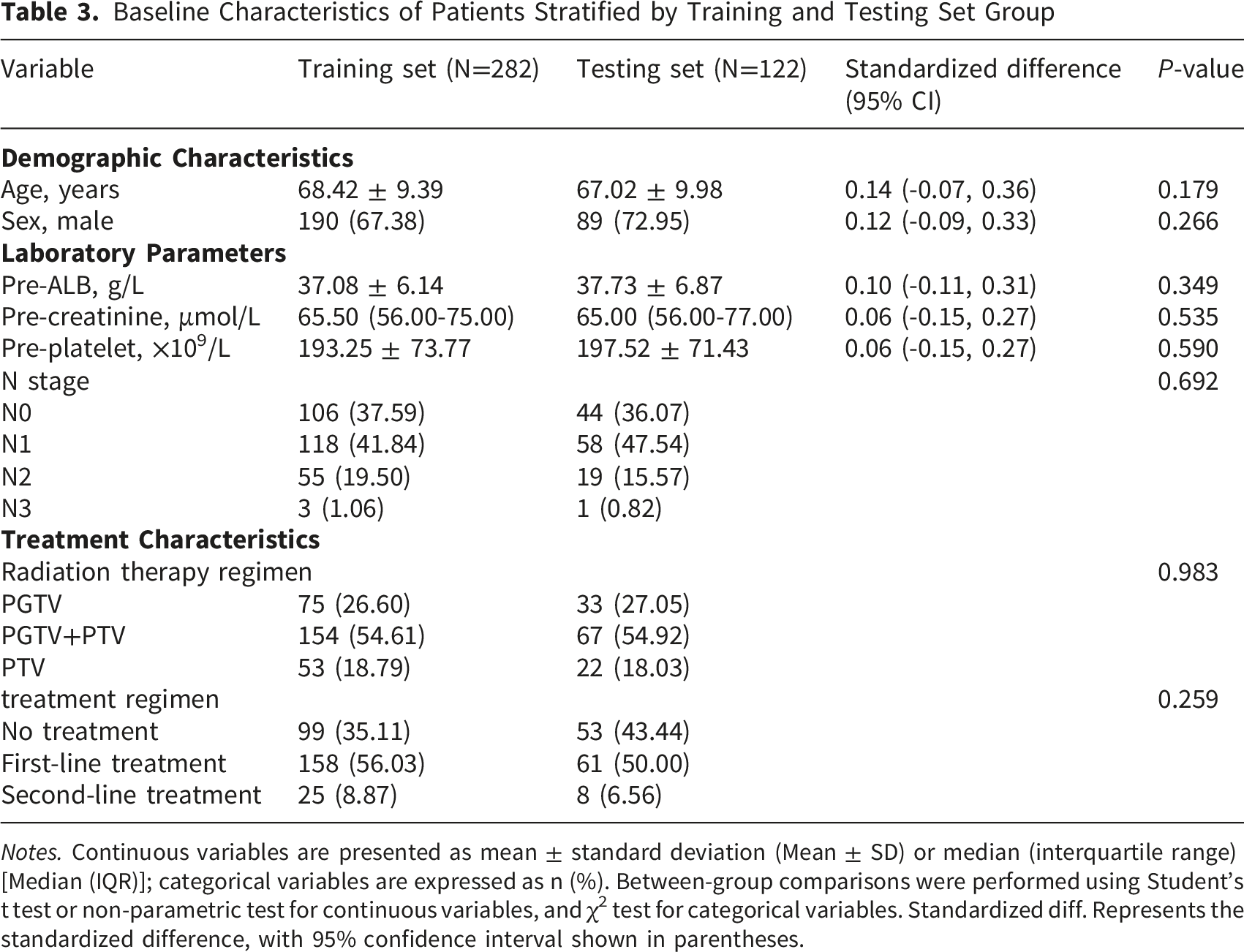
Notes. Continuous variables are presented as mean ± standard deviation (Mean ± SD) or median (interquartile range) [Median (IQR)]; categorical variables are expressed as n (%). Between-group comparisons were performed using Student’s t test or non-parametric test for continuous variables, and χ2 test for categorical variables. Standardized diff. Represents the standardized difference, with 95% confidence interval shown in parentheses.
Risk Model Development and Nomogram
Based on the multivariable logistic regression, we built a model to predict severe bone marrow suppression after radiotherapy or chemoradiotherapy and translated it into a nomogram (Figure 3). The nomogram incorporates eight predictors: sex, age, N stage, Pre-ALB, baseline creatinine, baseline platelet count, radiotherapy regimen, and systemic treatment category. To use it, locate the patient’s value on each predictor axis, draw a vertical line to the top “Points” scale to assign a score, and sum the scores to obtain a total (theoretical range 0–140). Map the total score to the “Linear Predictor” scale and then to the bottom axis, “Risk of severe myelosuppression,” to read the predicted probability (approximately 0.05–0.90). This provides an accessible estimate of individualized pre-treatment risk within the study cohort. Nomogram for predicting the risk of severe myelosuppression in patients with esophageal cancer undergoing (chemo)radiotherapy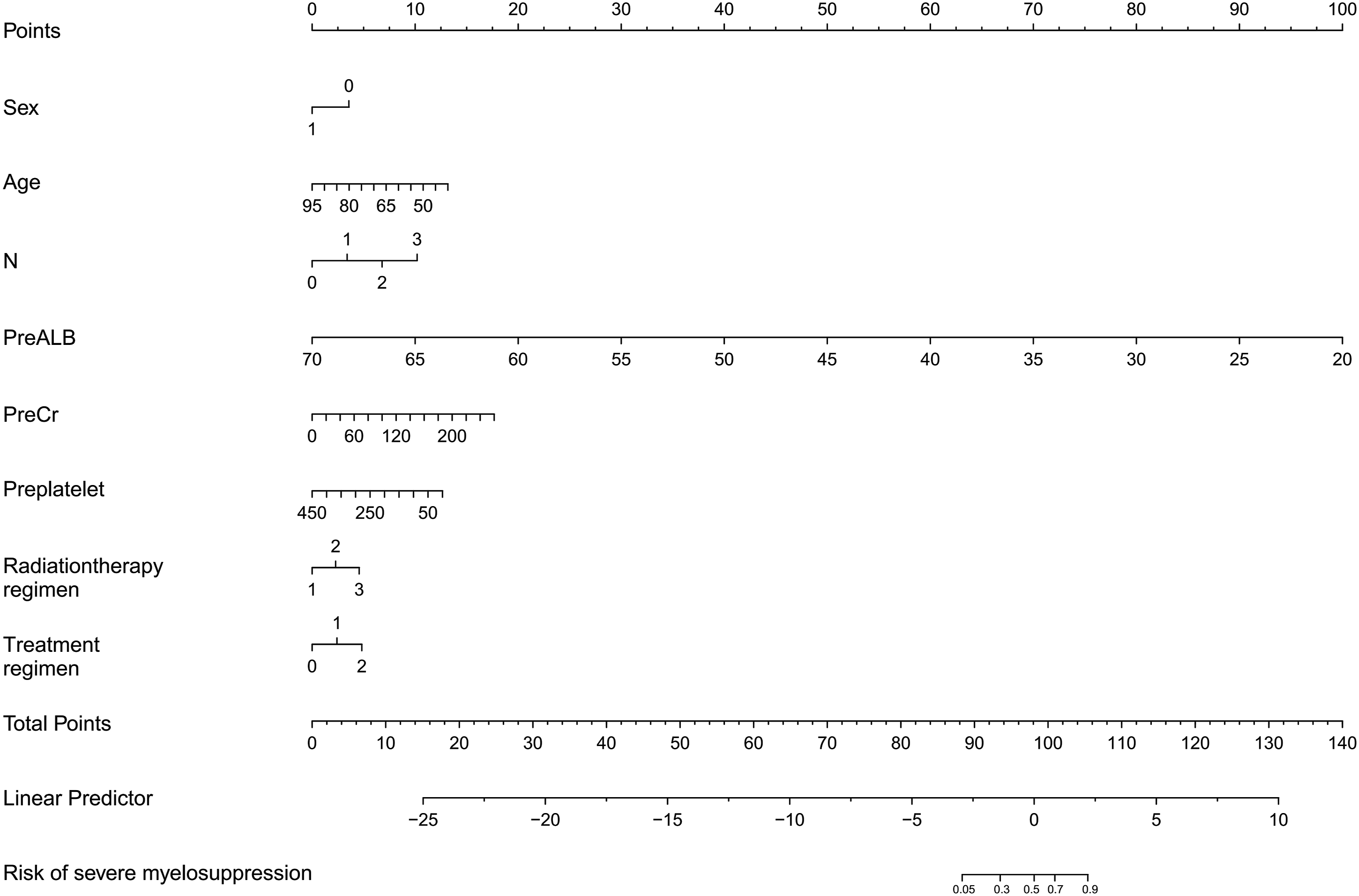
Model Validation and Performance
We undertook internal validation to assess model performance. ROC analyses showed strong discrimination in the present dataset: AUC 0.972 (95% CI, 0.941–0.988) in the training set (Figure 4A) and 0.956 (95% CI, 0.932–0.983) in the test set (Figure 4B), both well above the conventional threshold of 0.70. Among single predictors, Pre-ALB performed best (training AUC=0.953; test AUC=0.942), followed by N stage (training AUC=0.721; test AUC=0.705); other variables had more limited standalone discrimination. Calibration with 1,000 bootstrap resamples demonstrated close agreement between predicted and observed risks, with mean absolute errors of 0.011 in the training cohort (Figure 4C) and 0.037 in the testing cohort (Figure 4D). The Hosmer–Lemeshow goodness-of-fit test showed no significant evidence of poor fit in either cohort (training cohort, P=0.512; testing cohort, P=0.738), further supporting the calibration performance of the model. Decision-curve analysis suggested potential net benefit within the internal validation framework: in the training set, the model yielded greater net benefit than “treat all” or “treat none” across threshold probabilities of 0.10–0.80, approaching 1.0 (Figure 4E); in the test set, net benefit remained high (∼0.8) across thresholds of 0.10–0.70 (Figure 4F). Overall, the model showed strong discrimination and favorable calibration in the present cohort, supporting further external validation before broader clinical use. Performance evaluation of the predictive model. (A)–(B): ROC curves for the training and testing cohorts; (C)–(D): Calibration curves with bootstrap correction (1,000 resamples) in the training and testing cohorts. (E)–(F): Decision curve analysis (DCA) showing net benefit across different threshold probabilities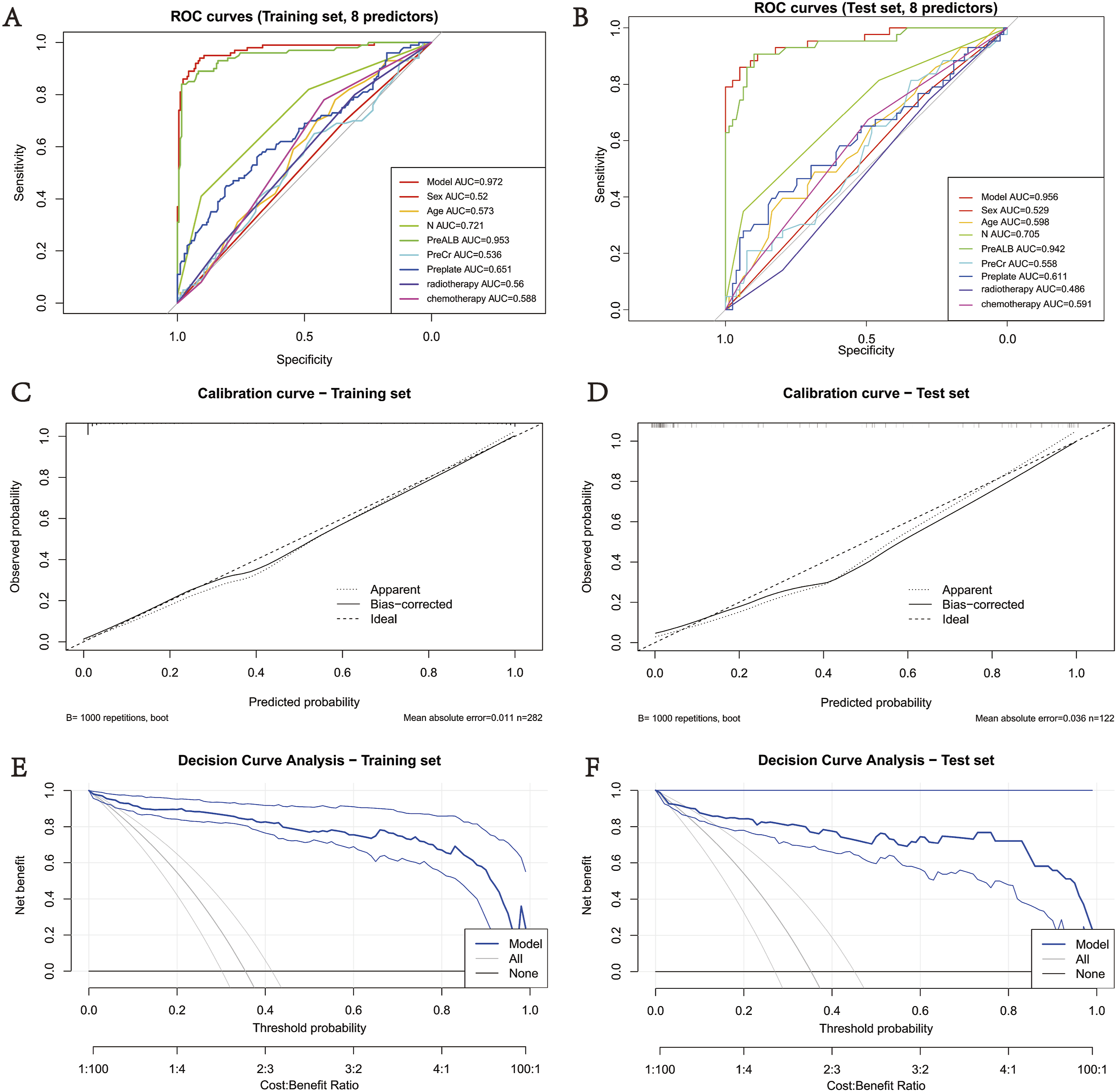
Discussion
Esophageal cancer is a common and lethal gastrointestinal malignancy worldwide. For locally advanced disease, concurrent chemoradiotherapy remains a principal nonsurgical option.22,23 Bone marrow suppression is the most frequent and consequential toxicity of this approach: it can prompt treatment interruption or dose reduction, diminish efficacy, and increase the risks of infection, bleeding, and hospitalization, with adverse effects on survival and quality of life.24,25 Using data from 404 patients treated with radiotherapy or concurrent chemoradiotherapy, we developed and validated a nomogram to predict severe bone marrow suppression. The model incorporates eight routinely available variables—sex, age, N stage, baseline ALB, Cr, PLT, radiotherapy regimen, and systemic treatment. Sex, age, N stage, ALB, Cr, and PLT emerged as independent predictors. In the present dataset, the model showed strong discrimination and favorable calibration in the training and internal test sets, and decision-curve analysis suggested potential net benefit across selected threshold probabilities.
Our findings align with, and extend, prior research on hematologic toxicity in esophageal cancer treated with CCRT. Earlier work has focused on dosimetric factors, particularly the association between thoracic vertebral bone marrow (TVBM) irradiation and acute marrow suppression. For example, Zhang et al. 26 linked higher TVBM dose to grade ≥3 hematologic toxicity and recommended treating marrow as an organ at risk during planning; similarly, Fabian et al 27 demonstrated a dose–response relationship between TVBM exposure and toxicity in lung cancer CCRT, underscoring the value of marrow contouring. Although our model does not include marrow dose metrics, it achieves high discrimination using readily available variables—baseline ALB and PLT, tumor stage, and treatment factors—offering a practical alternative when detailed dosimetry is unavailable. Related tools include a pre-treatment nomogram by van Rossum PSN et al that predicts grade 4 lymphopenia during CRT using staging and tumor length, 28 and more recent nomograms for radiation-associated thrombocytopenia. By combining nutritional/hematopoietic indices (ALB, PLT) with treatment strategy, our model attained a higher AUC, highlighting modifiable, non-dosimetric. These factors may help generate hypotheses for risk-adapted monitoring and supportive-care planning, which should be evaluated in future prospective studies.
Baseline ALB was the strongest predictor, underscoring the role of nutritional status in marrow toxicity. This accords with a meta-analysis in gastrointestinal cancers reporting higher rates of hematologic toxicity during CCRT among patients with hypoalbuminemia. 9 Low ALB may reflect poor reserves that impair hematopoietic recovery and exacerbate chemotherapy-related marrow injury. 6 Lower baseline PLT was also an independent risk factor, echoing findings by Cui et al., 11 who incorporated PLT into a radiomics–hematology nomogram for survival in locally advanced esophageal cancer. Including PLT helps flag patients with limited marrow reserve and may support pre-emptive measures such as granulocyte colony-stimulating factor (G-CSF). For risk management and nursing practice, these findings may help identify patients who could be considered for closer monitoring and supportive-care assessment.
Several nonintuitive associations also emerged. Younger patients had a higher risk of marrow suppression, in contrast to findings in SCLC by Li et al., 29 who reported greater toxicity in older adults. Treatment intensity may explain this discrepancy: younger patients often receive more aggressive regimens that increase marrow burden, whereas older patients with comorbidities are more likely to receive de-escalated therapy. 10 We also observed a higher risk of severe marrow suppression in women than in men, consistent with reports of greater chemotherapy toxicity among female patients.30,31 Potential mechanisms include differences in drug metabolism, hematopoietic reserve, and hormonal milieu; these warrant further study. Finally, N stage was a key contributor in our model. More advanced nodal disease reflects greater tumor burden and typically necessitates more complex or intensive treatment, increasing the likelihood of hematologic toxicity. However, estimates for the N3 subgroup should be interpreted cautiously because only a small number of patients had N3 disease. This pattern echoes observations in cervical and gastric cancer treated with chemoradiotherapy.32,33 For nursing practice, these findings support proactive risk management in high-risk patients—early education on signs of infection or bleeding, risk-adapted education and monitoring strategies should be further evaluated before being used for resource allocation or staffing decisions.
A notable innovation of this study is the inclusion of creatinine, a renal function marker, as an independent predictor—an uncommon feature in esophageal cancer research. Hua et al. 34 likewise identified creatinine as an independent risk factor for grade ≥3 adverse events in older Chinese patients receiving chemotherapy. Our findings suggest that renal impairment may heighten marrow suppression by altering drug metabolism and clearance. Clinically, renal status should be assessed before initiating therapy, with dose adjustments or marrow-protective measures considered for patients with dysfunction. Although radiotherapy regimen and systemic treatment were not statistically significant in multivariable analysis, we retained them based on clinical rationale and expert consensus. 35 Their nonsignificant P-values in this dataset should not be interpreted as evidence of no clinical relevance, because treatment-related effects may be influenced by sample distribution, collinearity with other predictors, and heterogeneity in treatment exposure. Both variables directly reflect treatment intensity, marrow exposure, and the overall burden of therapy, all of which are closely related to the risk of hematologic toxicity. Therefore, retaining these treatment-related variables improves the clinical interpretability of the model and may enhance its relevance for pretreatment risk stratification within the current dataset, particularly when the model is intended to support pretreatment risk stratification rather than to identify only statistically independent factors. 36
The model may have potential translational value as a pre-treatment risk-estimation tool, but its use should remain exploratory until external validation is completed. Before treatment, the nomogram may help identify patients at higher estimated risk of severe bone marrow suppression who may warrant closer hematologic monitoring, nutritional assessment, and supportive-care planning. However, it should not be used alone to determine chemotherapy dosing, radiotherapy fractionation, or other treatment modifications; such decisions should continue to be based on established clinical guidelines and multidisciplinary judgment. A risk-adapted monitoring framework could be explored in future prospective studies, including standard monitoring for lower-risk patients and more intensive hematologic surveillance and symptom screening for patients with higher estimated risk. Similarly, supportive measures such as nutritional counseling, infection-prevention education, and timely clinical review may be considered as part of individualized supportive-care planning rather than as protocolized interventions mandated by the model. Future work should include prospective external validation in independent multicenter cohorts, assessment of clinical impact, and integration with clinical decision-support systems before broader implementation.
Compared with prior studies, our model offers several advantages. The nomogram by van Rossum et al predicted grade-4 lymphopenia during CCRT with reasonable discrimination (C-index = 0.76) but targeted a single hematologic endpoint and was derived mainly from Western populations. The dosimetric model by Zhang et al clarifies mechanisms of marrow suppression from a physics perspective but requires complex calculations that limit routine use. In contrast, our model: (1) relies on routine clinical variables and needs no additional testing or complex computation; (2) is the first to be developed and validated in a Chinese cohort; (3) addresses multiple hematologic toxicities rather than a single metric; and (4) incorporates renal function, an under-recognized yet important predictor. This study has several limitations. First, as a single-center retrospective observational study, it can identify associations but cannot establish causal relationships, and residual confounding may remain despite multivariable adjustment. Second, potential selection and information bias cannot be fully excluded, and as a provincial referral center, our case mix may be skewed toward more advanced disease, which may limit generalizability. Third, some subgroups, such as adenocarcinoma and N3 disease, contained only a small number of patients, which may have reduced statistical power and limited the stability of subgroup-specific estimates. Therefore, findings related to these underrepresented subgroups should be interpreted cautiously and require confirmation in larger multicenter cohorts. Fourth, the model relied on pre-treatment static variables and did not incorporate dynamic on-treatment changes. Finally, although the model showed strong discrimination and favorable internal calibration, overfitting cannot be fully excluded in a single-center retrospective dataset with high apparent performance. Therefore, the nomogram should currently be regarded as a pre-treatment risk-estimation tool rather than a clinical decision-making standard. The current model should therefore be regarded as internally validated only. External prospective validation is still lacking, and independent multicenter cohorts are needed to confirm model robustness and generalizability. In addition, genetic polymorphisms, drug-metabolizing enzyme activity, and the impact of specific supportive nursing interventions were not assessed.
Conclusion
Using a large retrospective cohort from central China, we developed and validated a model to predict the risk of severe bone marrow suppression during radiotherapy or concurrent chemoradiotherapy in patients with esophageal cancer. The model showed favorable apparent performance, including strong discrimination, acceptable calibration, and potential net benefit, in the training and internal validation cohorts. These findings should be interpreted as dataset-specific model performance rather than evidence of proven real-world effectiveness. It may help clinicians and oncology nurses identify patients at higher risk before treatment and may inform risk stratification and supportive care planning; however, the findings should be interpreted cautiously until externally validated. Further evaluation in broader, multicenter populations is warranted.
Supplemental Material
Supplemental Material - Developing and Validating a Risk Model for Severe Bone Marrow Suppression in Esophageal Cancer Treated With Radiotherapy or Chemoradiotherapy: A Retrospective Cohort Study
Supplemental Material for Developing and Validating a Risk Model for Severe Bone Marrow Suppression in Esophageal Cancer Treated With Radiotherapy or Chemoradiotherapy: A Retrospective Cohort Study by Linlin Guo, Qian Zhang, Mengmei Zhang, Xiaohang Zhong, Yadong Song, Yongcheng Fu, Zhaorui Wang, Haozhe Zhang, Youfu He, and Chao Li in Technology in Cancer Research & Treatment.
Footnotes
Acknowledgements
We thank the participants for their contributions to this study. Generative artificial intelligence tools were used solely for language editing, grammar correction, and sentence polishing during manuscript preparation. They were not used to generate scientific content, analyze or interpret data, create or modify figures/tables, or draw conclusions. All scientific content was independently completed and approved by the authors.
Ethical Considerations
This retrospective study was approved by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University (Approval No. 2025-KY-1517-002; approval date: October 25, 2025).
Consent to Participate
Because this retrospective study used de-identified data from the hospital’s electronic medical record system, the requirement for written informed consent was waived by the Ethics Committee.
Author contributions
Conceptualization: CL and YH. Funding acquisition: YH and ZW. Project administration: CL. Supervision: CL. Validation: LG, QZ, and ZW. Visualization: LG, QZ, MZ, XZ, HZ, YS, and YH. Writing-original draft: LG and QZ. Writing-review and editing: CL and YH. All authors contributed to the article and approved the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (No. 82260084) and the 2024 Zhengzhou Medical and Health Technology Innovation Guidance Program Project (2024YLZDJH292).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.