
Abstract
Introduction
Hippocampal-avoidance whole-brain radiotherapy (HA-WBRT) effectively reduces neurocognitive decline in patients with brain metastases, but evidence from direct multi-platform comparisons remains limited. This study addresses the gap by comparing two mainstream radiotherapy systems for non-coplanar VMAT (NCVMAT) with flattening filter-free (FFF) and flattened (FF) beams.
Methods
A retrospective dosimetric cohort study was conducted on 22 consecutive patients. Four plan types were created: MC-NCVMAT (Elekta Infinity/Monaco) FFF/FF and UT-NCVMAT (UIH uRT-linac 506c/uRT-TPOIS) FFF/FF. Dosimetry, organ-at-risk (OAR) sparing, efficiency, and plan quality metric (PQM) were evaluated. Identical constraints were applied across platforms.
Results
UT-NCVMAT showed significantly better homogeneity, conformity, and OAR sparing than MC-NCVMAT. FFF beams outperformed FF in hippocampal protection. UT-NCVMAT reduced beam-on time and planning time by 44%. The 16-item PQM score was significantly higher in the UIH group. Post-hoc power analysis confirmed sample adequacy.
Conclusion
The UIH uRT-TPOIS system with NCVMAT FFF may offer superior dosimetry, efficiency, and clinical feasibility for HA-WBRT. The PQM model may serve as a reliable tool for standardized plan evaluation. Further multi-center validation is warranted.
Keywords
1. Introduction
Brain metastases (BM) frequently occur as a complication in advanced stages of cancer, with lung and breast cancers representing the most common primary origins. 1 Whole-brain radiotherapy (WBRT) continues to serve as a fundamental treatment approach for individuals presenting with multiple BM, offering palliative advantages and efficient management of symptoms. 2 Nonetheless, standard WBRT is linked to notable neurocognitive deterioration, largely because of injury to the hippocampus, which plays an essential role in memory formation and learning processes. 3 In response to this issue, hippocampal-avoidance WBRT(HA-WBRT) has arisen as an encouraging strategy, employing sophisticated radiation technologies to protect hippocampal functionality without compromising tumor control efficacy. Studies including RTOG 0933 and NRG CC001 have illustrated both the practicality and therapeutic value of HA-WBRT.4,5 As outlined in the American Society for Radiation Oncology (ASTRO) guidelines concerning suitable radiation therapy for brain metastases, WBRT is advised for patients who exhibit a favorable prognosis and present with brain metastases, yet are not suitable candidates for surgical intervention or stereotactic radiosurgery(SRS), should receive whole-brain radiotherapy. Whenever feasible, hippocampal avoidance techniques should be incorporated into the treatment plan. Additionally, the administration of Memantine is recommended as part of the therapeutic strategy. 6
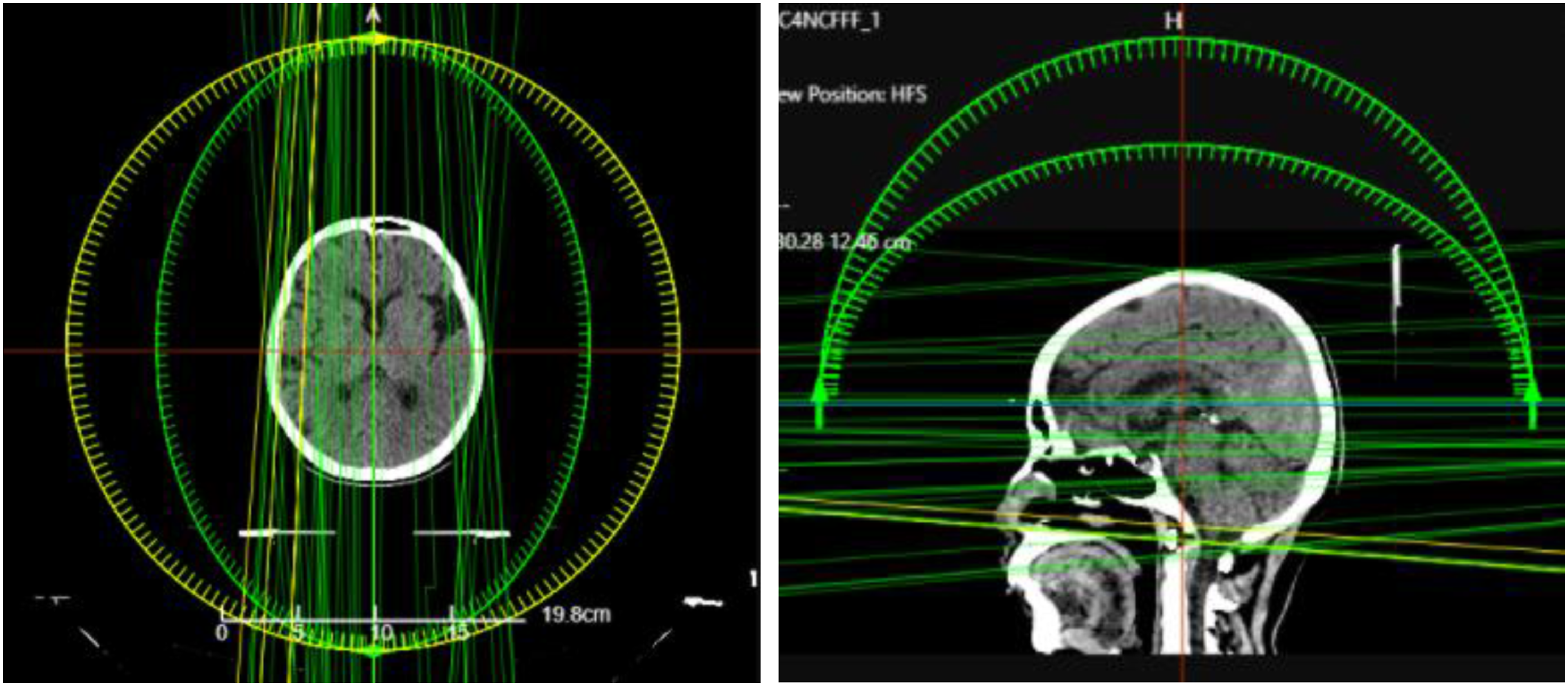
Recent progress in treatment planning systems(TPS) and linear accelerators(LINACs) has allowed for increasingly accurate dose administration. Widely implemented technologies such as volumetric-modulated arc therapy(VMAT), non-coplanar VMAT(NC-VMAT), and flattening filter-free(FFF) beams contribute to superior dose conformity, shorter treatment durations, and decreased integral radiation exposure to healthy tissues. Notable hardware and software differences exist between the two mainstream clinical platforms evaluated in this study. The Elekta Infinity LINACs system is equipped with 80 pairs of 0.5 cm fully central-focused Multi-Leaf Collimator(MLCs) and works with the Monaco TPS, which employs a Monte Carlo (MC)–based dose algorithm known for high precision in complex geometries, when used alongside the Monte Carlo(MC) - driven Monaco TPS, delivers reference-level precision in dose computation via sophisticated particle transport algorithms.7,8 Another innovative solution is the uRT-linac 506c radiotherapy system, which is a computed tomography-integrated LINACs platform(Figure 1) that works with its dedicated uRT-TPOIS TPS. The UIH uRT-linac 506c is an integrated CT–LINAC system equipped with a hybrid MLC configuration (0.5 cm central leaves + 1.0 cm peripheral leaves) and paired with the uRT-TPOIS TPS, which uses the Collapse Cone (CC) algorithm and supports proprietary uARC delivery.This system supports intensity-modulated radiation therapy(IMRT), uARC(VMAT), and non-coplanar radiotherapy(NC-RT). Initial research supports the clinical effectiveness of uRT-TPOIS across various tumor types,9-11 with Yang et al.
11
leading the way in its use for HA-WBRT via NC-VMAT planning with 6 MV beams FFF beams. Nevertheless, clinical application varies widely among different systems: commercial platforms (e.g., Elekta Monaco) and domestic options (e.g., United Imaging Healthcare’s uRT-TPOIS) exhibit differences in beam modeling techniques, optimization approaches, and the ability to deliver non-coplanar arcs, resulting in variations in both plan quality and treatment efficiency. Two state-of-the-art radiotherapy systems. (a) Elekta Infinity with Monaco TPS. (b) UIH uRT-linac 506c with uRT-TPOIS TPS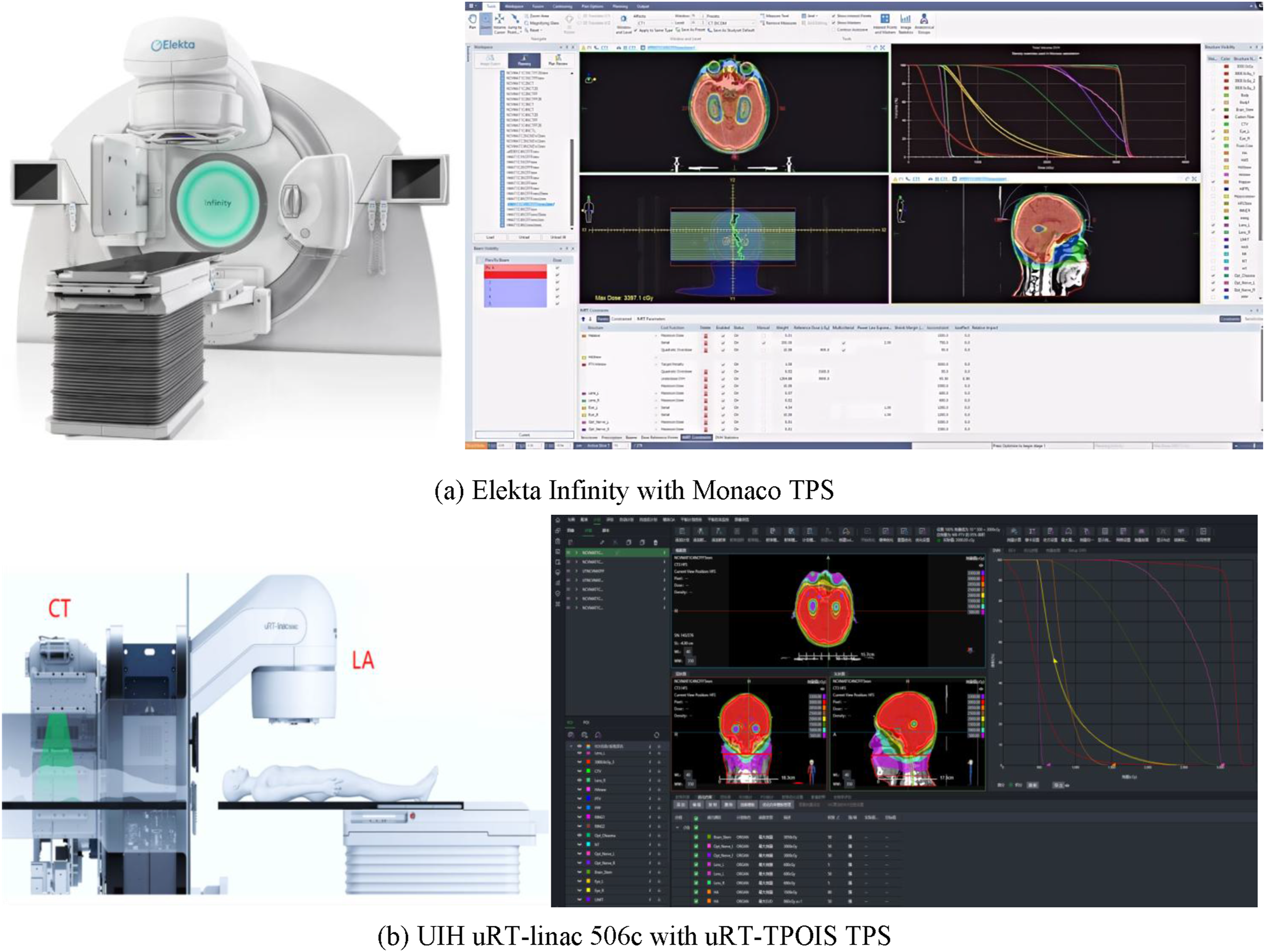
Although HA-WBRT is increasingly used clinically, several important questions remain to be further clarified: (1) How do different TPS–LINAC configurations compare in terms of dosimetric outcomes, particularly for critical structures such as the hippocampus, optic nerves, and lenses? (2)While FFF and FF beams have been compared in previous HA-WBRT studies (Ji et al., 2022), 12 it remains unclear whether such differences are consistent across different radiotherapy platforms or are system-dependent. (3) Can integrated evaluation tools such as the Plan Quality Metric (PQM) provide a consistent and standardized method for assessing HA-WBRT treatment plans? Resolving these issues is essential for refining clinical workflows and enhancing the quality and safety of patient care.
Accordingly, this study conducts a systematic comparison between the Elekta Infinity/Monaco platform and the UIH uRT-linac 506c/uRT-TPOIS platform for HA-WBRT. This research seeks to conduct a systematic comparison between two advanced radiotherapy platforms—Elekta Infinity equipped with Monaco TPS and UIH uRT-linac 506c integrated with uRT-TPOIS TPS—within the framework of HA-WBRT, as illustrated in Figure 1. Four distinct treatment plan configurations were assessed: NC-VMAT employing both FFF and FF beams across the two systems. We examined dosimetric outcomes, organ-at-risk sparing, plan complexity, and delivery efficiency to determine optimal clinical approaches. Furthermore, a novel PQM model was introduced to quantitatively evaluate plan quality, offering an evidence-based foundation for technology selection and standardization of treatment protocols.
2. Materials and Methods
2.1 Patient Selection and Structure Delineation
This retrospective study was approved by the institutional ethics committee. The requirement for written informed consent was waived due to the retrospective nature of the study. All procedures performed in this study were in accordance with the 1975 Helsinki Declaration, as revised in 2024. The reporting of this study conforms to STROBE guidelines, 13 which was shoued in appendix 3. All patient information was fully de-identified to protect privacy.
Twenty-two patients diagnosed with brain metastases from lung or breast cancer who received HA-WBRT
From 2023 to 2025 were enrolled in this retrospective dosimetric cohort study. All patients were treated with thermoplastic head mask immobilization in the supine position, as illustrated in Figure 2. Simulation images were obtained using computed tomography (CT) and magnetic resonance imaging (MRI), and were transferred to the RayStation 9A treatment planning system for image registration and structure delineation. Position fixation for radiotherapy in HA-WBRT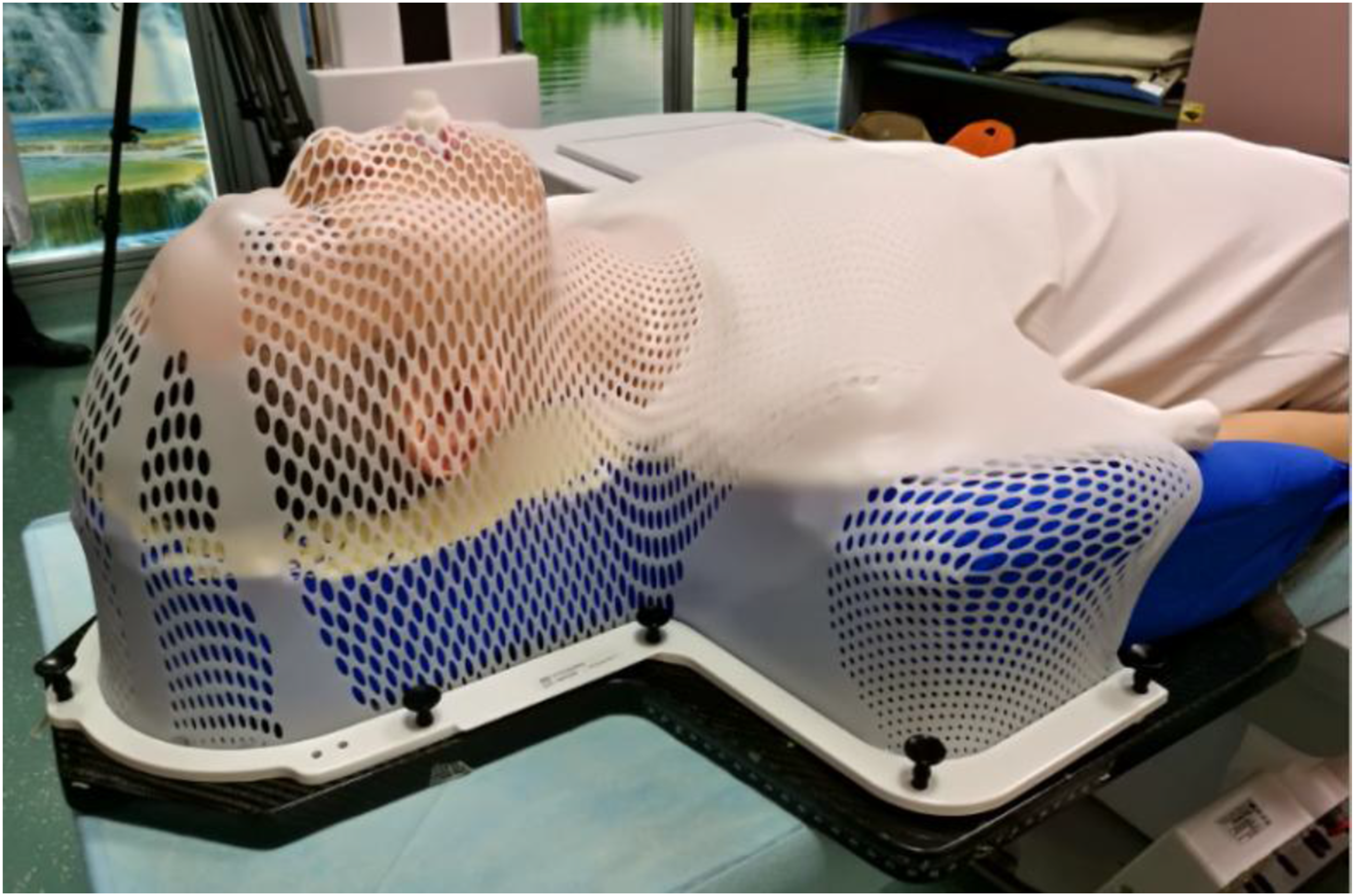
The hippocampus was outlined according to the RTOG 0933 reference atlas, utilizing axial T1-weighted magnetic resonance imaging sequences.
4
Additional organs at risk (OARs), such as the eyes, lens, optic nerves, optic chiasm, brainstem, and spinal cord, were automatically segmented via the OAR auto-segmentation tool integrated into the RayStation treatment planning system. Furthermore, the scalp and upper cervical regions were manually contoured by a radiation oncologist to assess scalp dosage and the extent of low-dose radiation exposure in the upper neck, as illustrated in Figure 3. A hippocampal planning risk volume (HP-PRV) was produced by uniformly expanding the hippocampus contour by 5 mm, in accordance with the RTOG 0933 protocol. The clinical target volume (CTV) included the whole brain. A planning target volume (PTV) was generated by applying a uniform 3 mm margin around the CTV. In the design of the HA-WBRT plan, the whole brain planning target volume (WB-PTV) was characterized as the PTV with the exclusion of the HP-PRV. All delineated target volumes and OAR contours were reviewed and adjusted by radiation oncologists possessing more than a decade of clinical experience, with subsequent verification conducted by senior radiation oncologists. The delineation of scalp and upper neck. (a) Scalp structure. (b) Upper neck structure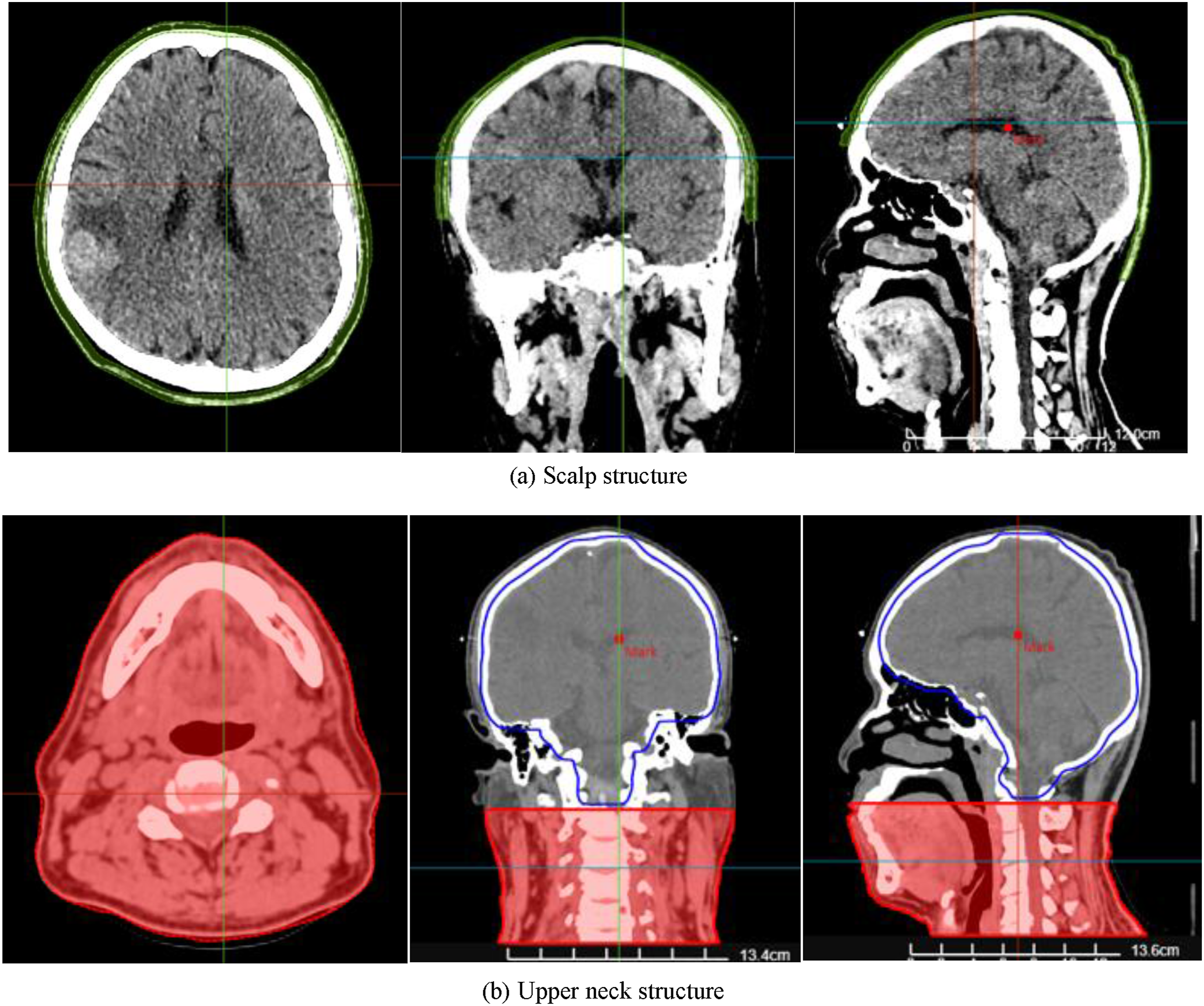
(The scalp was defined as the region with a thickness of 5 mm from the skin surface, located above the level of the foramen magnum, and the forehead area was adjusted accordingly, 14 the upper neck was defined as the anatomical region located inferior to the foramen magnum, serving as the transitional zone between the cranial base and the cervical spine.)
2.2 Treatment Planning
All CT images that included the target structures and OARs were imported into both the Monaco and uRT-TPOIS TPS. All treatment plans(NC-VMAT plans using FFF and FF modes for HA-WBRT) were redesigned by two independent senior medical physicists, each with over 10 years of clinical radiotherapy planning experience. One physicist was exclusively responsible for all Elekta/Monaco plans, and the other independently completed all UIH/uRT-TPOIS plans, with no cross-participation in each other’s planning work to avoid operational bias. Specifically, Monaco TPS version 5.40.4 (Elekta AB, Stockholm, Sweden) was employed to design plans for the Infinity linear accelerator (Elekta AB, Stockholm, Sweden), whereas uRT-TPOIS TPS version R001.4 (United Imaging Healthcare (UIH) Co., China) was applied for the uRT-linac 506c system (UIH Co., China). The UIH uRT-linac 506C employs a hybrid MLC configuration: 0.5 cm central 40 pairs + 1.0 cm peripheral 20 pairs. Dose calculation grid was uniformly set to 2.0 mm for both platforms. Identical dose constraints and optimization objectives were applied to both platforms to ensure fair comparison. The UT-NCVMAT plans use more arcs because uRT-TPOIS does not support round-trip arcs.
Patient-specific quality assurance (PSQA) for all reconstructed NC-VMAT plans was performed using the COMPASS system combined with an electronic portal imaging device (EPID). The EPID was used to acquire in-portal dose measurements, and the measured dose distribution was reconstructed within the COMPASS platform for subsequent comparison with the dose distribution calculated by each treatment planning system. Global gamma analysis was applied for dosimetric verification, adopting standard evaluation criteria of 3% dose difference/3 mm distance-to-agreement (3%/3 mm) with a low-dose threshold of 10%. A gamma passing rate greater than 95% was defined as the clinical acceptance threshold for plan deliverability.
Key Parameters of the Elekta Infinity and UIH uRT-Linac 506c
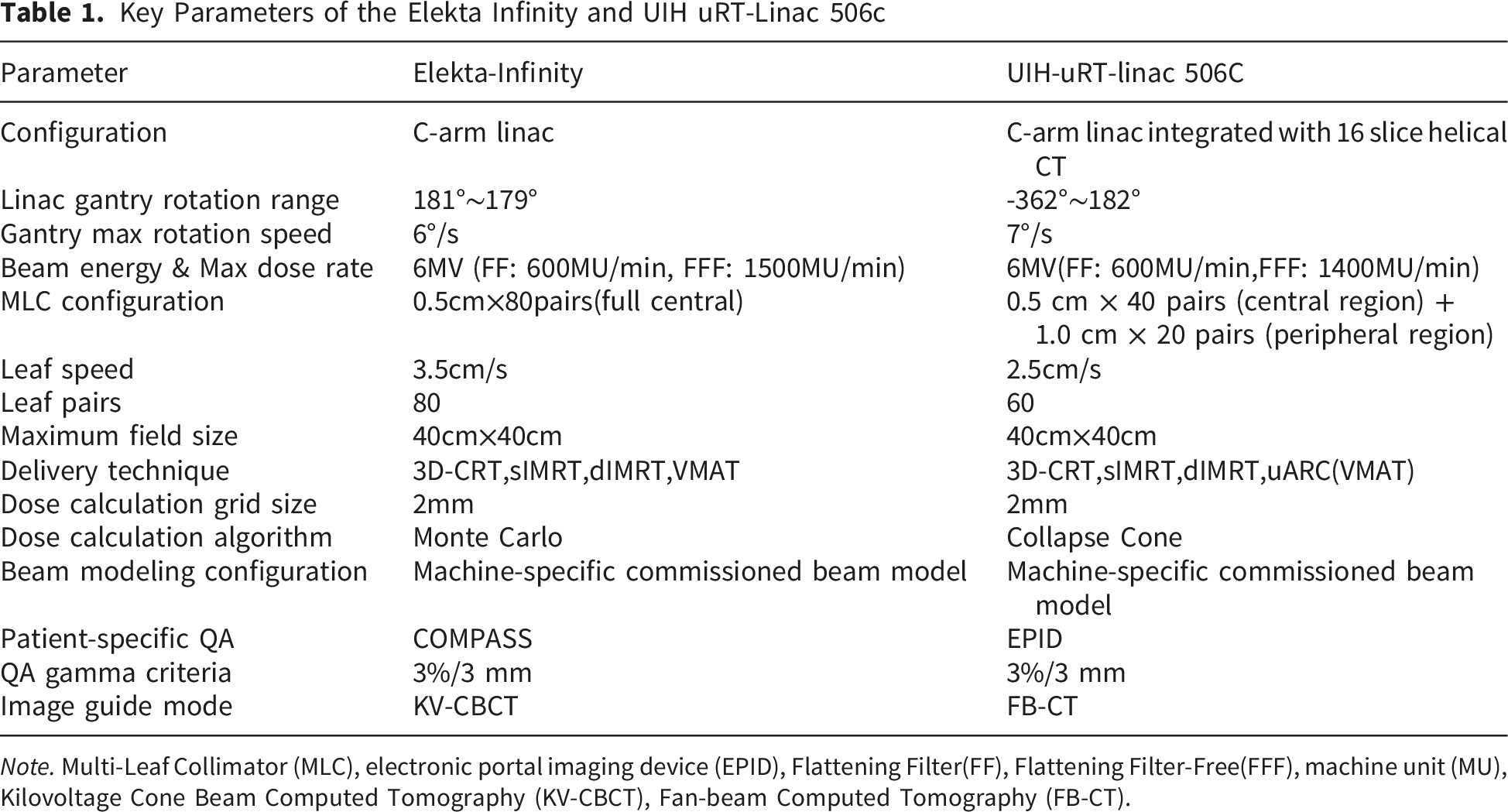
Note. Multi-Leaf Collimator (MLC), electronic portal imaging device (EPID), Flattening Filter(FF), Flattening Filter-Free(FFF), machine unit (MU), Kilovoltage Cone Beam Computed Tomography (KV-CBCT), Fan-beam Computed Tomography (FB-CT).
Dosimetric Compliance Criteria for Hippocampal Avoidance in RTOG 0933
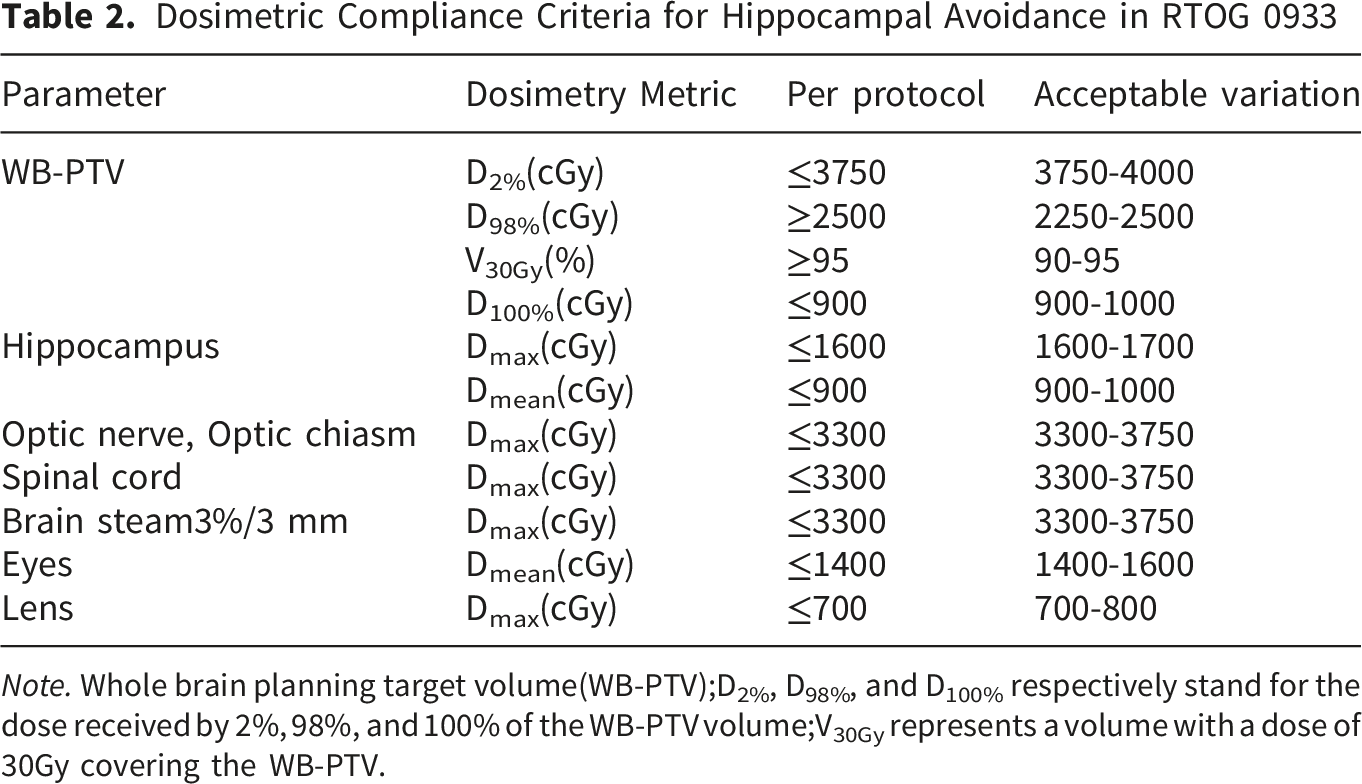
Note. Whole brain planning target volume(WB-PTV);D2%, D98%, and D100% respectively stand for the dose received by 2%, 98%, and 100% of the WB-PTV volume;V30Gy represents a volume with a dose of 30Gy covering the WB-PTV.
(1) NCVMAT Plans for Monaco
The beam configuration and all optimization parameters applied in the Monaco NCVMAT (MC-NCVMAT) plans were derived from two earlier investigations carried out by the author’s research group.16,17 Comprehensive details can be found in Appendix 1 of this work. The preliminary optimization objectives used during the first optimization cycle remained unaltered and were not customized for individual patients.
(2) NCVMAT Plans for uRT-TPOIS
UT-NCVMAT Beam Arrangements
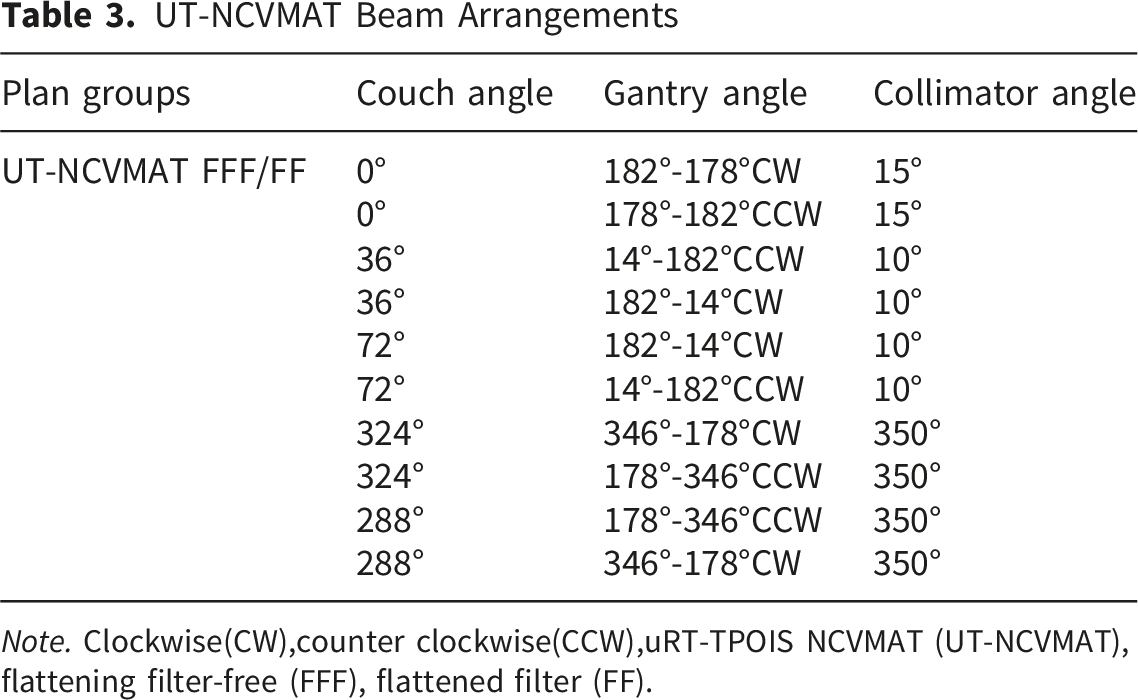
Note. Clockwise(CW),counter clockwise(CCW),uRT-TPOIS NCVMAT (UT-NCVMAT), flattening filter-free (FFF), flattened filter (FF).
UT-NCVMAT beam arrangements for uRT-linac 506C
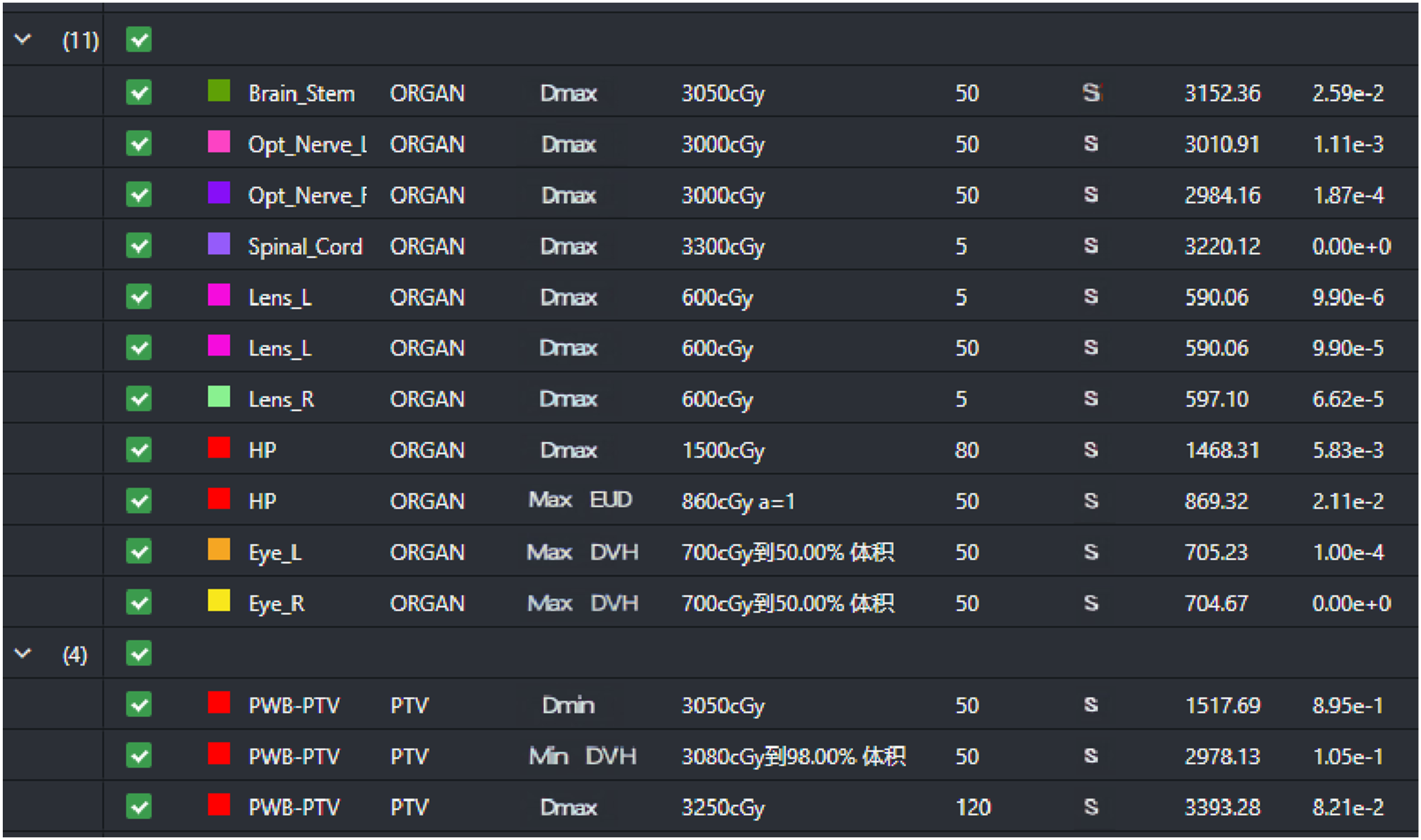
Initial optimization objectives for UT-NCVMAT
2.3 Plan Comparison
(1) Dosimetric Evaluation
Within the Monaco and uRT-TPOIS treatment planning systems, dose–volume histograms (DVHs) were produced for the target area, hippocampus, and additional organs at risk across four planning categories: MC-NCVMAT FFF, MC-NCVMAT FF, UT-NCVMAT FFF, and UT-NCVMAT FF. For every plan, the radiation doses encompassing 2%, 98%, and 50% of the target volume (D2%, D98%, and D50%) were assessed. The conformity index (CI), homogeneity index (HI), and gradient index (GI) were derived based on the formulas provided below.
TVpv denotes the portion of the target volume that obtains a dose no less than the prescribed dosage. PV indicates the entire tissue volume receiving a dose meeting or surpassing the prescription threshold, while TV corresponds to the gross target volume. The CI varies between 0 and 1, where values approaching 1 reflect superior dose conformity.
18

The D2%, D50%, and D98% correspond to the radiation doses absorbed by 2%, 50%, and 98% of the target volume, respectively. The Homogeneity Index (HI) indicates the uniformity of dose distribution across the target, where values nearer to 0 signify superior dose homogeneity.
19

V50% and V100% denote the volumes enclosed by the 50% and 100% prescription dose isolines, respectively. The Gradient Index (GI) quantifies the sharpness of dose decline beyond the target region; higher values reflect broader dispersion of the low-dose zone and consequently a less favorable plan quality. 20
For each treatment plan, the following parameters were assessed: the maximum doses to the hippocampus at volumes of 0 cc, 0.01 cc, and 0.03 cc (Dmax(0cc), Dmax(0.01cc), Dmax(0.03cc)), the dose covering 100% of the structure (D100%), and the mean dose (Dmean) to the hippocampus. Additionally, the maximum dose to 0.01 cc (Dmax(0.01cc)) was evaluated for the lens, optic nerve, optic chiasm, and scalp, while the Dmean was determined for the eyes and scalp. The relative volumes of the upper neck receiving 5 Gy, 10 Gy, 15 Gy, and 20 Gy were quantified as V5, V10, V15, and V20, respectively. Furthermore, beam-on time (BOT), machine units (MU), PQM, modulation complexity score (MCS), and modulation degree (MD) were employed to evaluate plan execution efficiency, overall quality, and complexity.
(2) Comprehensive Quantitative Evaluation of the Plan
The YINO tumor information management system (Yino v2.25, China) was utilized to perform a thorough and quantitative assessment of overall plan quality, integrating a dedicated plan evaluation module grounded in the PQM model. The MC-NCVMAT FFF, MC-NCVMAT FF, UT-NCVMAT FFF, and UT-NCVMAT FF plans were systematically imported into the YINO platform to acquire respective quantitative evaluation scores. In this investigation, the PQM evaluation framework comprised 16 items strictly derived from the complete dosimetric constraints of the RTOG 0933 protocol. Most previously reported PQM frameworks for HA-WBRT only included limited conventional target-related parameters while neglecting refined dose limits for multiple critical organs at risk. In contrast, the present 16-item PQM comprehensively integrates target coverage, dose homogeneity, conformity, and detailed dose endpoints for the hippocampus, optic nerve, lens, brain stem, and scalp. This design fully complies with RTOG 0933 specifications and better matches the clinical characteristics of hippocampal-sparing whole-brain radiotherapy. Compared with earlier simplified models, our PQM enables moreobjective, holistic, and standardized quantitative evaluation and cross-platform comparison, providing additional practical value for routine clinical plan assessment and quality control.
The Definition of PQM Evaluation Standard for HA-WBRT.
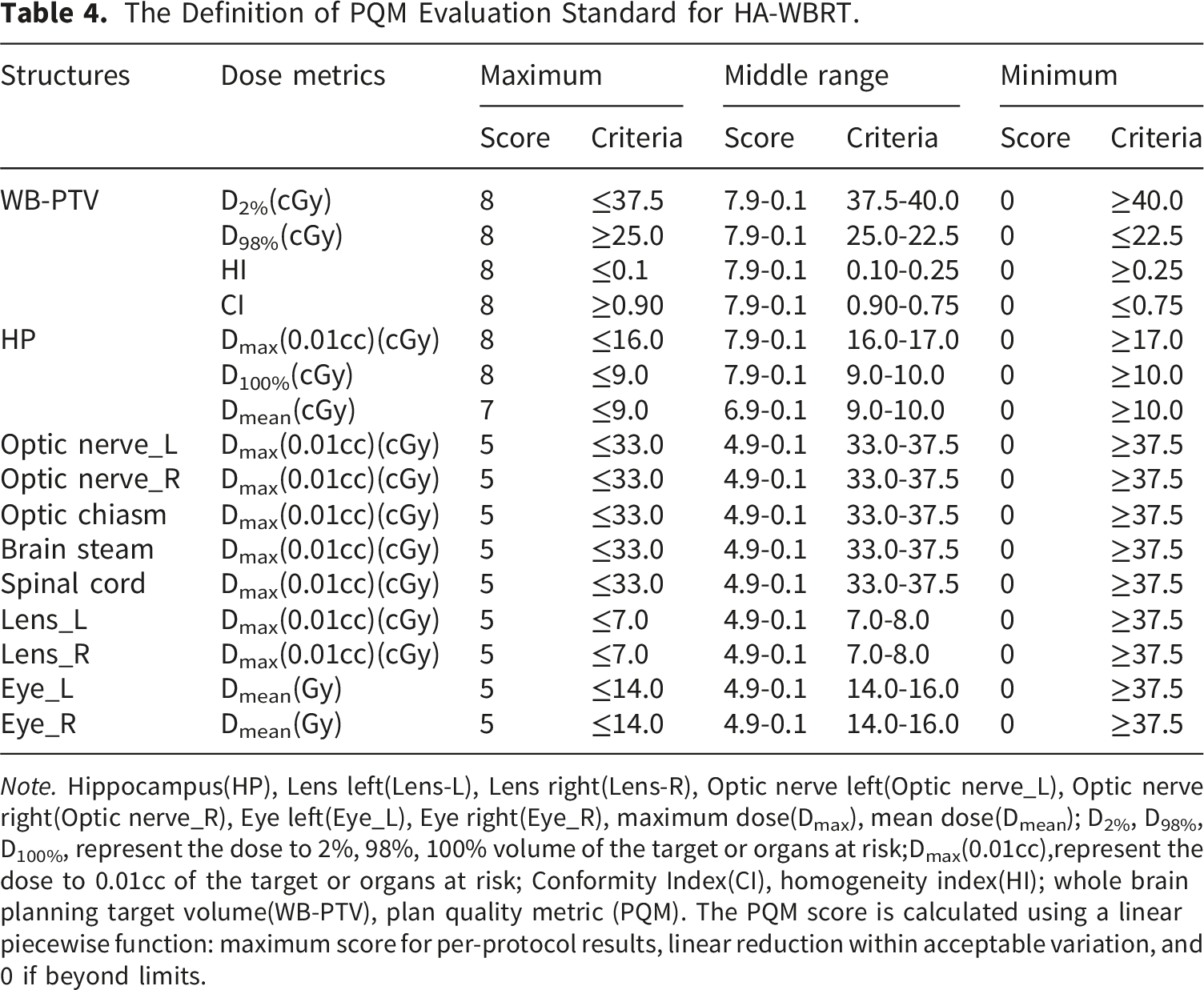
Note. Hippocampus(HP), Lens left(Lens-L), Lens right(Lens-R), Optic nerve left(Optic nerve_L), Optic nerve right(Optic nerve_R), Eye left(Eye_L), Eye right(Eye_R), maximum dose(Dmax), mean dose(Dmean); D2%, D98%, D100%, represent the dose to 2%, 98%, 100% volume of the target or organs at risk;Dmax(0.01cc),represent the dose to 0.01cc of the target or organs at risk; Conformity Index(CI), homogeneity index(HI); whole brain planning target volume(WB-PTV), plan quality metric (PQM). The PQM score is calculated using a linear piecewise function: maximum score for per-protocol results, linear reduction within acceptable variation, and 0 if beyond limits.
(3) Plan Complexity and Plan Execution Efficiency
Complexity indicators are crucial for assessing treatment plans. Drawing on the MCS-related studies by Masi et al. 21 and Huang et al, 22 we created a computational tool to measure plan complexity through MCS. This tool generates an MCS score on a scale from 0 to 1, where lower values reflect increased complexity. Further elaboration on this metric can be found in Appendix 2. Within the Monaco TPS, the MD offers an alternative complexity measure, accessible directly from the platform. It captures the extent of modulation present in the plan. For both IMRT and VMAT plans, MD values are generally equal to or greater than 1, and higher figures denote more intricate modulation. The modulation degree is computed over all beams or sequences using the formula 23 : Modulation Degree=Total MU/[Sum of (Segment Area×Segment MU)/Total Beam Area]. All plans were analyzed using the MCS tool, and MD values for the MC-NCVMAT treatment plans were directly exported from the Monaco TPS. MU and BOT were acquired from both the Monaco and uRT-TPOIS treatment planning systems.
There was an inherent difference in arc arrangement strategy between the two TPS platforms. The Monaco system supports round-trip arc delivery, which enables sufficient plan optimization with fewer arcs. In comparison, the current version of uRT-TPOIS does not support round-trip arc configuration and only allows unidirectional arcs. To maintain equivalent target coverage, hippocampal sparing level and overall plan quality consistent with Monaco NC-VMAT plans, more independent unidirectional arcs were applied for UT-NCVMAT planning. This setting is determined by the native functional characteristics of each TPS, and ensures a fair and comparable baseline for subsequent dosimetric analysis and PQM evaluation.
2.4 Statistical Analysis
All statistical evaluations were performed using IBM SPSS 22.0 (New York, NY), with a p-value below 0.05 deemed statistically significant. Normality of data was examined via the Shapiro-Wilk test. For data following a normal distribution, one-way ANOVA was employed to assess variations among the four groups. When significant differences were detected (p < 0.05), post hoc analyses were conducted to determine specific pairwise contrasts. Non-normally distributed data were analyzed using the Kruskal-Wallis test. Findings are expressed as mean ± standard deviation (x̄ ± SD) for normally distributed data and median (interquartile range) [M(Q1, Q3)] for non-normal data. A total of six pairwise comparisons were systematically performed among the four groups (MC-FFF vs MC-FF, UT-FFF vs UT-FF,MC-FFF vs UT-FFF, MC-FFF vs UT-FF, MC-FF vs UT-FFF, MC-FF vs UT-FF), utilizing either the independent samples t-test or the Mann-Whitney U test depending on data distribution characteristics.
3. Results
3.1 Patient Clinical Information
Summary of Patient Characteristics
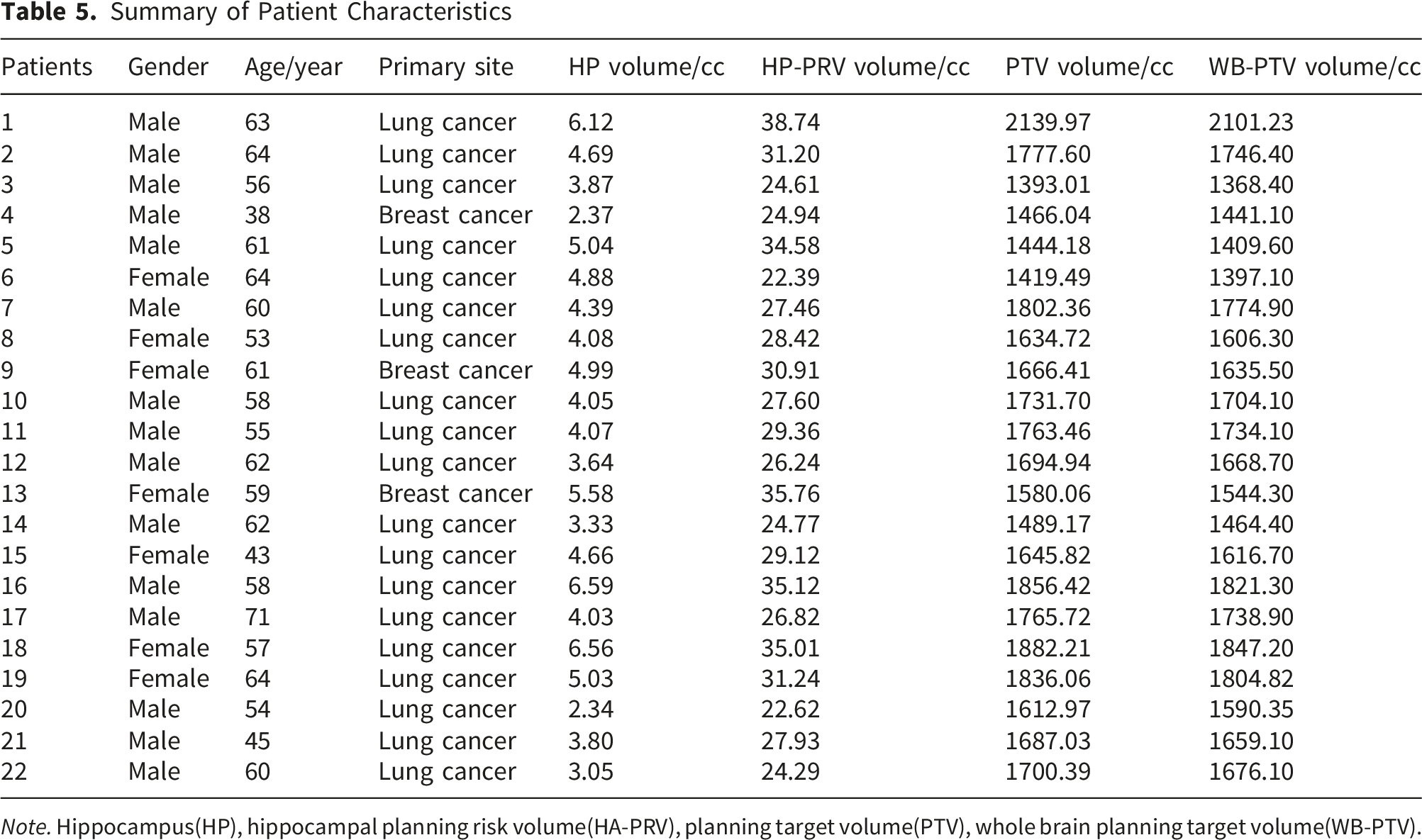
Note. Hippocampus(HP), hippocampal planning risk volume(HA-PRV), planning target volume(PTV), whole brain planning target volume(WB-PTV).
3.2 Assessment of Doses to Targets and OARs
A total of 88 plans were analyzed (four techniques per patient). All plans met predefined dosimetric criteria. Most parameters were within per-protocol thresholds; minor deviations remained within acceptable variation limits.
The average planning time was 25 minutes for UT-NCVMAT plans and 45 minutes for MC-NCVMAT plans, indicating higher efficiency with uRT-TPOIS. Dose distributions and DVHs are shown in Figure 6. Dosimetric endpoints are summarized in Table 6 and Figure 7. Group comparisons were performed using ANOVA or nonparametric tests, with post-hoc pairwise testing as appropriate. Dosimetric comparison among four HA-WBRT plan groups. (a) Axial isodose distributions for MC-NCVMAT FF and MC-NCVMAT FFF plans. (b) Dose–volume histogram (DVH) curves for MC-NCVMAT plans (solid = FFF; dashed = FF). (c) Axial isodose distributions for UT-NCVMAT FF and UT-NCVMAT FFF plans. (d) Dose–volume histogram (DVH) curves for UT-NCVMAT plans (solid = FFF; dashed = FF) Average Dosimetric Values and Comparison Under 4 Groups Note. WB-PTV(WPTV),hippocampus(HP),Optic nerve Left(OptL),Optic nerve Right(OptR),Optic chiasm(Opsm),Brain steam (BS),Spinal cord(SC),Lens Left(LensL),Lens Right(LensR),Eye Left(EyeL),Eye Right(EyeR).*p<0.05 represents statistically significant difference between the four groups. If there is a statistically significant difference between groups, post hoc tests will be conducted to compare the differences among each group:† represents statistically significant difference with MC-NCVMAT FF, ‡ represents statistically significant difference with UT-NCVMAT FFF, £ represents statistically significant difference with UT-NCVMAT FF. Dmax represents the maximum dose to 0cc, Dmax✦represents the maximum dose to 0.01cc, Dmax✫represents the maximum dose to 0.03cc. The median dosimetric results among the four groups
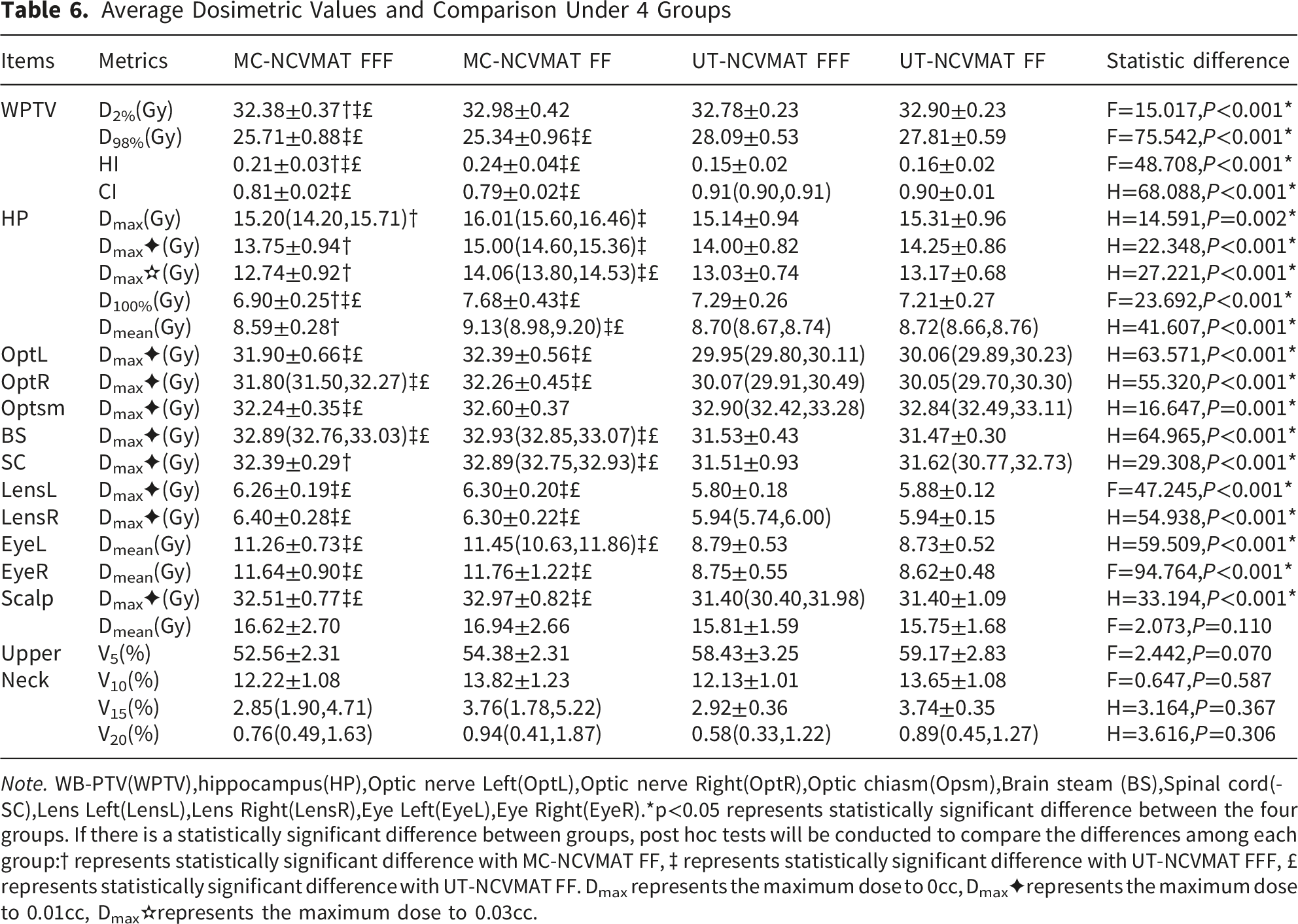
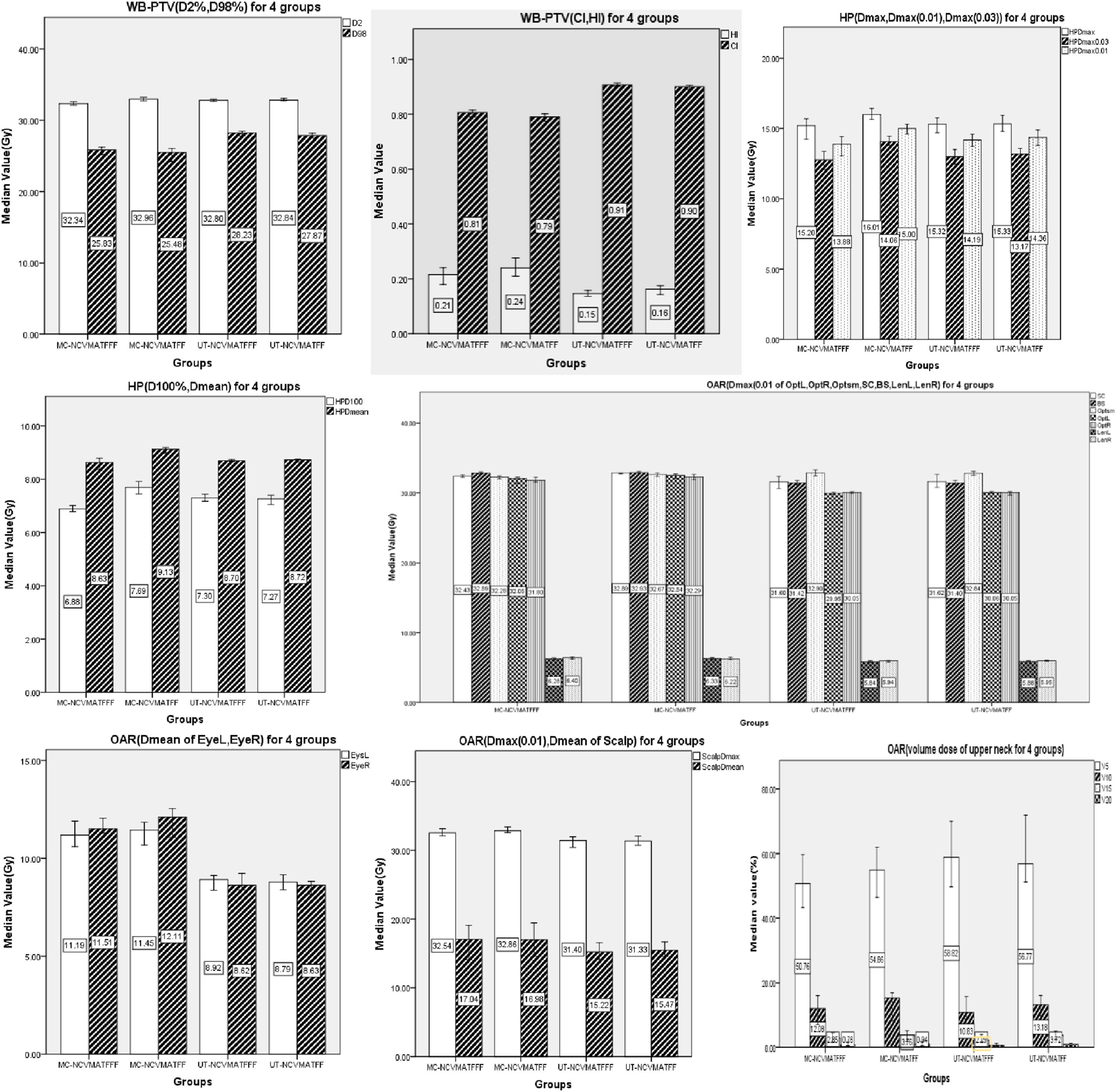
Significant differences were observed in nearly all parameters (all P<0.001) except scalp Dmean and upper-neck V5–V20 (all P>0.05). MC-NCVMAT FFF achieved significantly lower WB-PTV D2% than the other three groups (all P<0.001). UT-NCVMAT plans (both FFF and FF) showed significantly better WB-PTV D98%, HI, and CI than MC-NCVMAT plans (all P<0.001). MC-NCVMAT FFF also exhibited superior HI compared with MC-NCVMAT FF (P<0.001).
Both FFF plans (MC-NCVMAT FFF and UT-NCVMAT FFF) provided significantly better HP sparing (Dmax, Dmax(0.01cc), Dmax(0.03cc), D100%, Dmean) than MC-NCVMAT FF (all P<0.05). UT-NCVMAT FF also showed improved HP Dmax(0.03cc), D100%, and Dmean relative to MC-NCVMAT FF (all P<0.01).
UT-NCVMAT plans (FFF and FF) yielded significantly lower Dmax(0.01cc) for bilateral optic nerves, brainstem, lenses, and scalp, as well as lower eye Dmean, compared with MC-NCVMAT plans (all P<0.01). MC-NCVMAT FFF showed lower optic chiasm Dmax(0.01cc) than UT-NCVMAT plans (P<0.01). For spinal cord, UT-NCVMAT plans and MC-NCVMAT FFF provided lower Dmax(0.01cc) than MC-NCVMAT FF (all P<0.05). No significant differences were observed in upper-neck volume doses.
The Pairwise Difference for the 4 Types of Treatments in the Related P Values of Dosimetric Metric
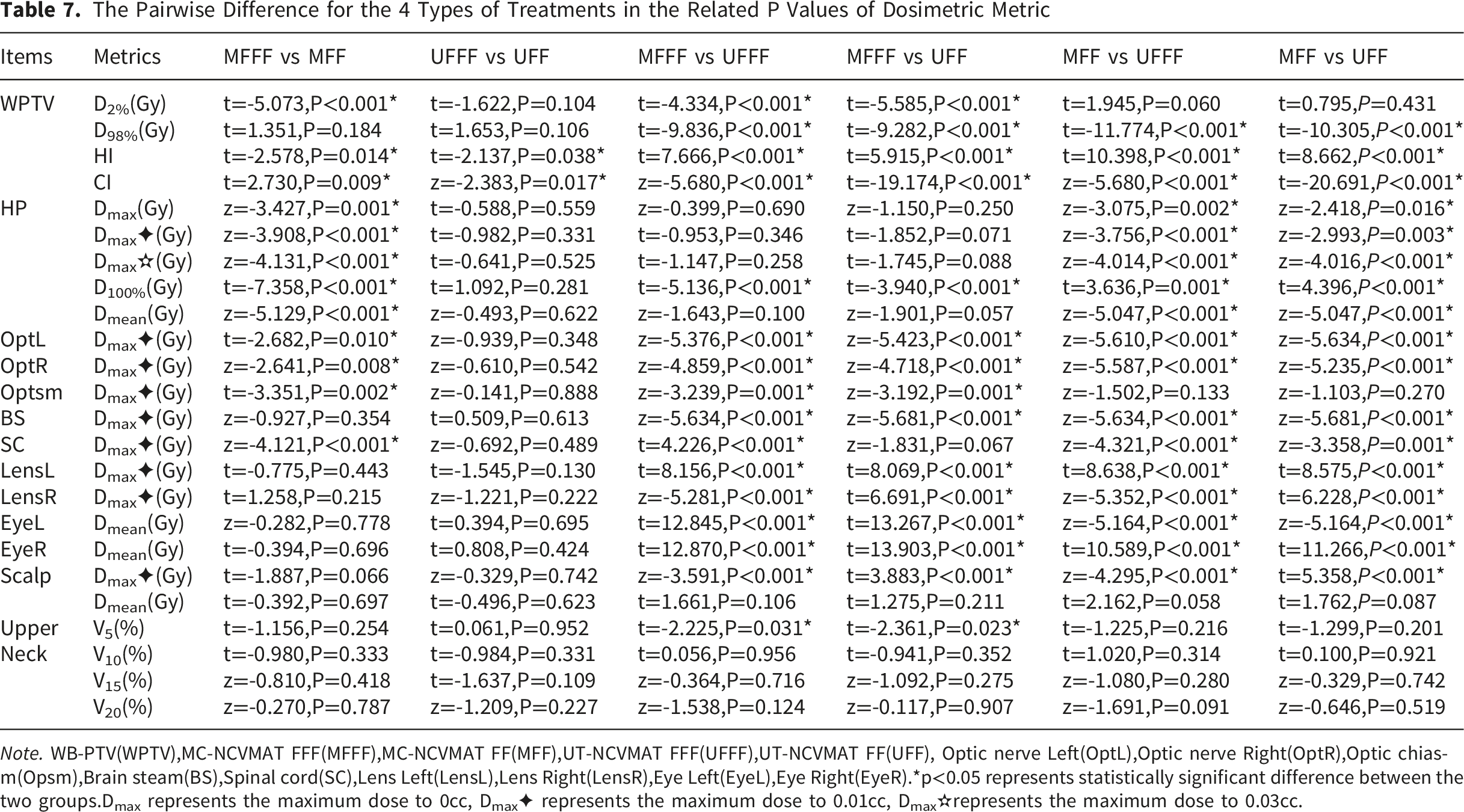
Note. WB-PTV(WPTV),MC-NCVMAT FFF(MFFF),MC-NCVMAT FF(MFF),UT-NCVMAT FFF(UFFF),UT-NCVMAT FF(UFF), Optic nerve Left(OptL),Optic nerve Right(OptR),Optic chiasm(Opsm),Brain steam(BS),Spinal cord(SC),Lens Left(LensL),Lens Right(LensR),Eye Left(EyeL),Eye Right(EyeR).*p<0.05 represents statistically significant difference between the two groups.Dmax represents the maximum dose to 0cc, Dmax✦ represents the maximum dose to 0.01cc, Dmax✫represents the maximum dose to 0.03cc.
MC-NCVMAT FFF was superior to MC-NCVMAT FF in multiple target, HP, and OAR metrics (all P<0.05).
UT-NCVMAT FFF was only significantly better than UT-NCVMAT FF in WB-PTV HI and CI (P<0.05).
MC-NCVMAT FFF achieved lower WB-PTV D2% and higher HP D100% but poorer HI, CI, D98%, and OAR sparing than UT-NCVMAT plans (all P<0.001).
Both UT-NCVMAT techniques were dosimetrically superior to MC-NCVMAT FF for most endpoints (all P<0.05).
All plans were normalized to a prescription dose of 30 Gy in 10 fractions. Color scale represents radiation dose in cGy.
3.3 Evaluation of MU, BOT, PQM, MCS, GI, and MD
Plan quality metrics are shown in Figure 8 and Table 8. All parameters differed significantly among groups (all P<0.001). MC-NCVMAT FFF had the highest MU, followed by MC-NCVMAT FF, UT-NCVMAT FF, and UT-NCVMAT FFF (all P<0.001). The median plan quality results among the four groups Plan Quality Comparison of 4 Group Plans Note. Machine unit(MU), beam on time(BOT), plan quality metric (PQM), modulation complexity score (MCS), gradient index(GI), modulation degree(MD).*p<0.05 represents statistically significant difference between the four groups. If there is a statistically significant difference between groups, post hoc tests will be conducted to compare the differences among each group:† represents statistically significant difference with MC-VMAT FF, ‡ represents statistically significant difference with UT-VMAT FFF, £ represents statistically significant difference with UT-VMAT FF.“/” there is no relevant data available.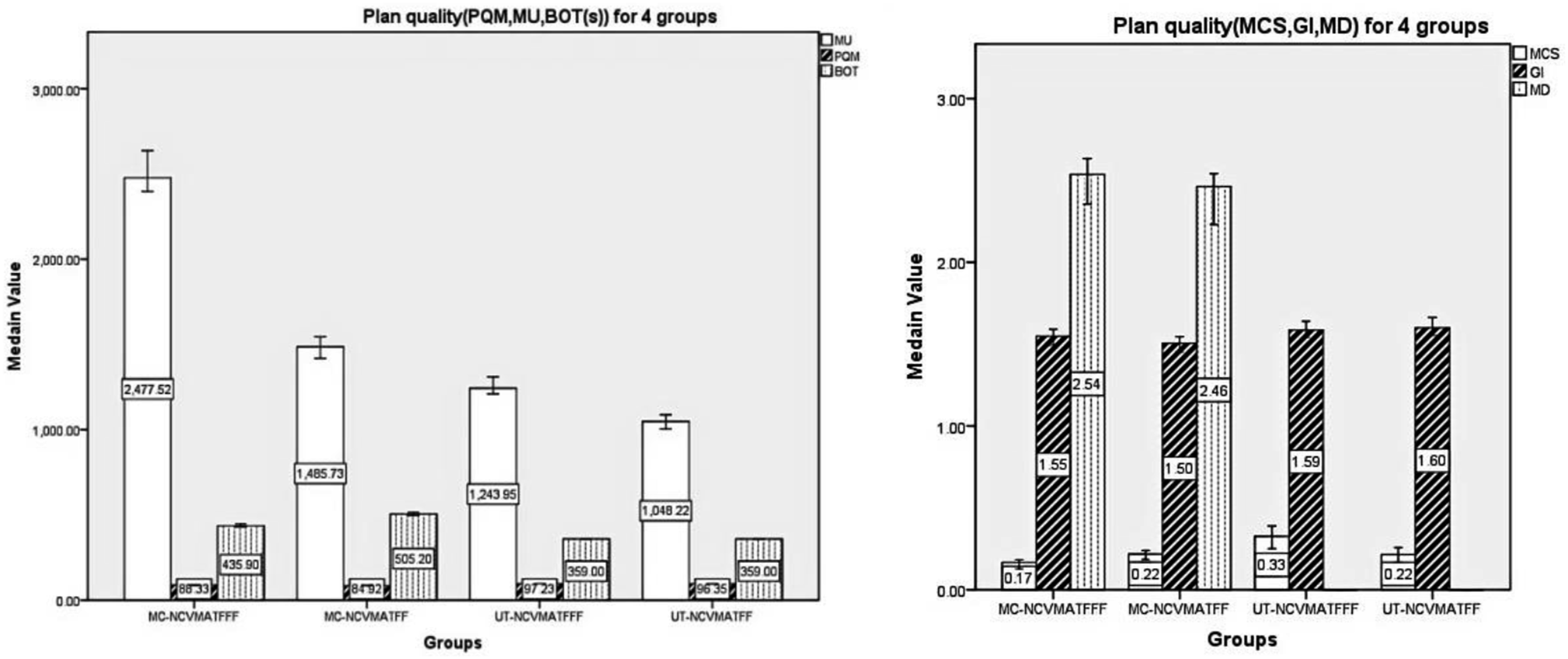
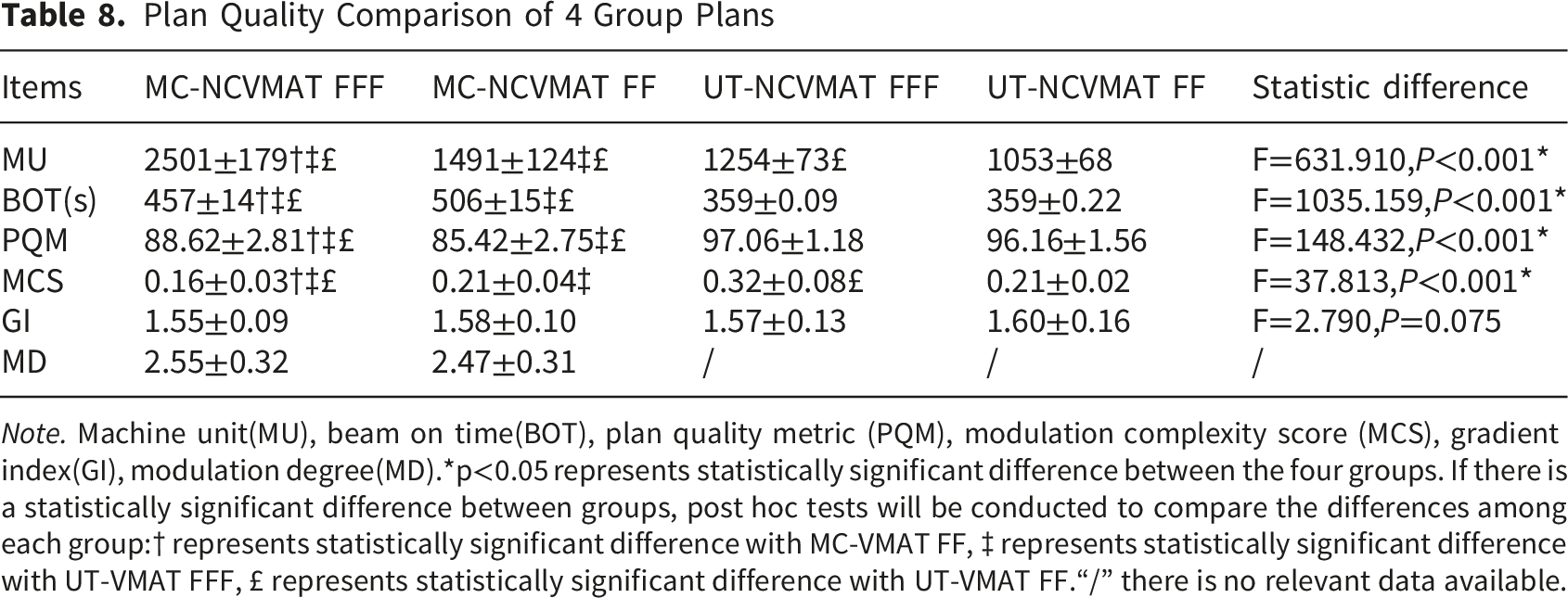
BOT was longest in MC-NCVMAT FF, followed by MC-NCVMAT FFF, while UT-NCVMAT plans showed similarly short BOT (all P<0.05). PQM was significantly higher in UT-NCVMAT plans than in MC-NCVMAT plans (all P<0.001); MC-NCVMAT FFF also had higher PQM than MC-NCVMAT FF (P<0.001).
MCS was lowest in MC-NCVMAT FFF, intermediate in MC-NCVMAT FF and UT-NCVMAT FF, and highest in UT-NCVMAT FFF (all P<0.001). GI showed no significant differences among groups (P>0.05). MD was only available in Monaco plans and showed no significant difference (P=0.599).
The Pairwise Difference for the 4 Types of Treatments in the Related P Values of Plan Quality
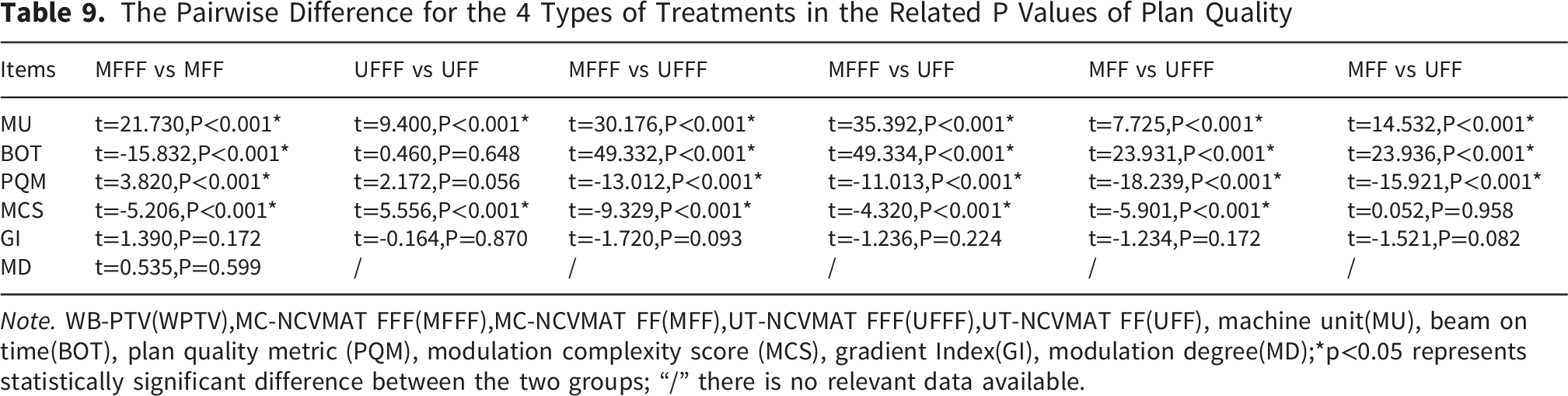
Note. WB-PTV(WPTV),MC-NCVMAT FFF(MFFF),MC-NCVMAT FF(MFF),UT-NCVMAT FFF(UFFF),UT-NCVMAT FF(UFF), machine unit(MU), beam on time(BOT), plan quality metric (PQM), modulation complexity score (MCS), gradient Index(GI), modulation degree(MD);*p<0.05 represents statistically significant difference between the two groups; “/” there is no relevant data available.
Patient-specific QA was performed for all plans. The average gamma passing rate (3%/3 mm, 10% threshold) was 98.2±1.1% for MC-NCVMAT plans and 98.7±0.8% for UT-NCVMAT plans, with all plans above 95%. These results confirm excellent delivery accuracy and support the reliability of cross-platform dosimetric comparisons.
In addition, patient-specific quality assurance was performed for all reconstructed HA-WBRT plans in this study. The average gamma passing rate was 98.2 ± 1.1% for MC-NCVMAT plans and 98.7 ± 0.8% for UT-NCVMAT plans, with all plans achieving a passing rate greater than 95%. The consistently high gamma passing rates across all groups further validate the delivery accuracy and clinical deliverability of the optimized plans, confirming the reliability of the dosimetric comparison results between the two platforms.
4. Discussions
4.1 Summary of the Study
Radiotherapy inevitably inflicts some harm on healthy tissues while focusing on tumor eradication. In recent years, the treatment philosophy has shifted from “survival-focused care' to “optimal survival”. 24 As radiation technology continues to advance, greater possibilities have arisen for maintaining the functionality of normal organs during treatment. The challenge of leveraging both traditional and innovative radiotherapy systems to realize “optimal survival' for individuals with cancer remains a central concern within clinical and physics investigations in this domain. Safeguarding hippocampal integrity is especially vital, given its profound influence on cognitive performance, memory retention, and the overall quality of life among oncology patients.
This investigation utilized a combination of retrospective and prospective research approaches. A total of twenty-two radiotherapy cases treated with HA-WBRT were randomly chosen. Drawing on two distinct radiotherapy platforms (uRT-TPOIS paired with uRT-linac 506c, and Monaco integrated with Infinity), and taking cues from the HyperArc radiotherapy method as well as earlier studies by the research team, four distinct radiotherapy strategies were formulated: MC-NCVMAT FFF, MC-NCVMAT FF, UT-NCVMAT FFF, and UT-NCVMAT FF. This process yielded a cumulative total of 88 distinct treatment plans. Each plan underwent thorough assessment using a variety of dosimetric metrics and plan quality indices, with the goal of determining the optimal HA-WBRT planning technique and confirming the clinical efficacy of the novel radiotherapy system.
The findings revealed that UT-NCVMAT FFF/FF delivered enhanced outcomes in target homogeneity (reduced HI), conformity (elevated CI), and organ-at-risk sparing (notably decreased Dmax(0.01cc) for the optic nerves, brainstem, and lens), alongside improved plan efficiency (reduced MU, shorter BOT, and higher PQM scores). Conversely, MC-NCVMAT FFF exhibited superior high-dose target coverage (better D2%) and diminished hippocampal dose exposure (lower D100%). Importantly, differences observed between FF and FFF modes among treatment planning systems highlighted the substantial impact of TPS-specific features and beam setup (with or without flattening filter) on both dose distribution and delivery performance in HA-WBRT. These results provide empirical justification for the clinical adoption of HA-WBRT methodologies, facilitating the refinement of treatment strategies to optimally reconcile tumor management with normal tissue preservation.
Clinical Feasibility of Five-Couch-Angle Non-coplanar VMAT
Although five non-coplanar couch angles are used in the NCVMAT plans, this configuration is clinically feasible and widely accepted in routine practice. Couch angles are preconfigured before treatment, and modern image-guided radiotherapy (IGRT) allows for rapid, accurate patient positioning. The small increase in setup time is acceptable and partially offset by shorter beam on times, especially with FFF beams. While simpler beam arrangements can provide satisfactory dose distributions, the multi-angle non-coplanar approach yields superior target homogeneity and organ-at-risk sparing, which is critical for protecting neurocognitive and visual function in HA-WBRT. Multiple published studies have validated the safety and practicality of 4–6 non-coplanar arcs for brain radiotherapy, supporting the clinical suitability of this technique.
Dosimetric Result Overview
It is noteworthy that statistical significance does not always equate to clinical meaningfulness. In this study, several dosimetric parameters presented statistically significant differences between the two platforms. For hippocampal dose parameters, the reduced dose achieved by the optimized plans not only reached statistical difference but also satisfied the dose-sparing requirements specified in RTOG 0933. This degree of hippocampal dose reduction is clinically meaningful, as it helps lower radiation damage to neural stem cells and potentially reduces the risk of post-radiation neurocognitive impairment and memory deterioration. By contrast, the statistically significant differences observed in other organs at risk, including the optic nerve, lens and brain stem, were small in absolute dose variation and remained far below clinically relevant tolerance thresholds. Such differences are statistically detectable but considered clinically negligible for routine clinical application.
4.2 Comparison With Relevant Research Literature
Literature Review on HA-WBRT Based on Linear accelerators(2015-2025)
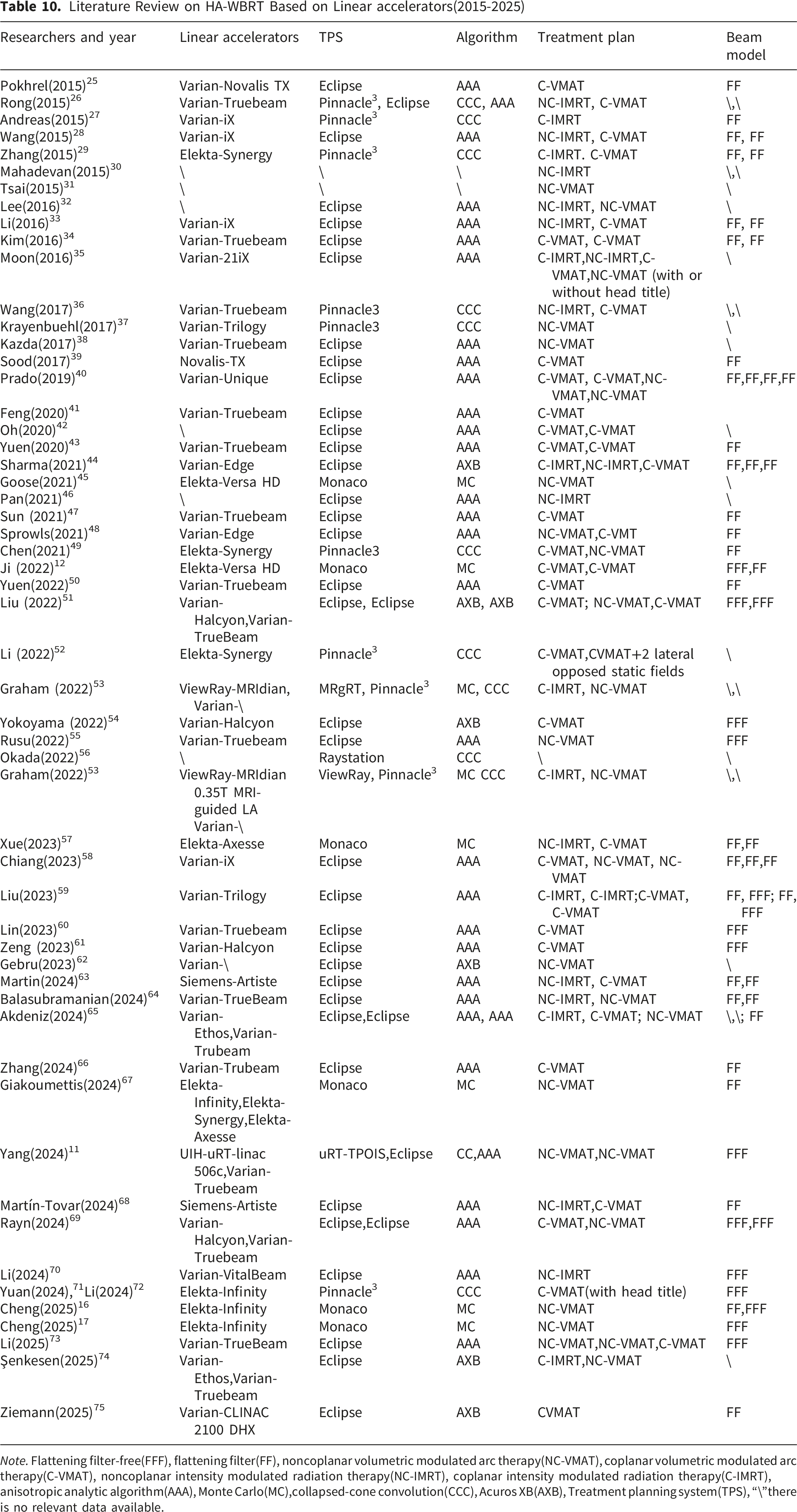
Note. Flattening filter-free(FFF), flattening filter(FF), noncoplanar volumetric modulated arc therapy(NC-VMAT), coplanar volumetric modulated arc therapy(C-VMAT), noncoplanar intensity modulated radiation therapy(NC-IMRT), coplanar intensity modulated radiation therapy(C-IMRT), anisotropic analytic algorithm(AAA), Monte Carlo(MC),collapsed-cone convolution(CCC), Acuros XB(AXB), Treatment planning system(TPS), “\”there is no relevant data available.
Comparison of Dosimetry With Related Studies Reported in the Literature (2020–2025) (Mean Values)
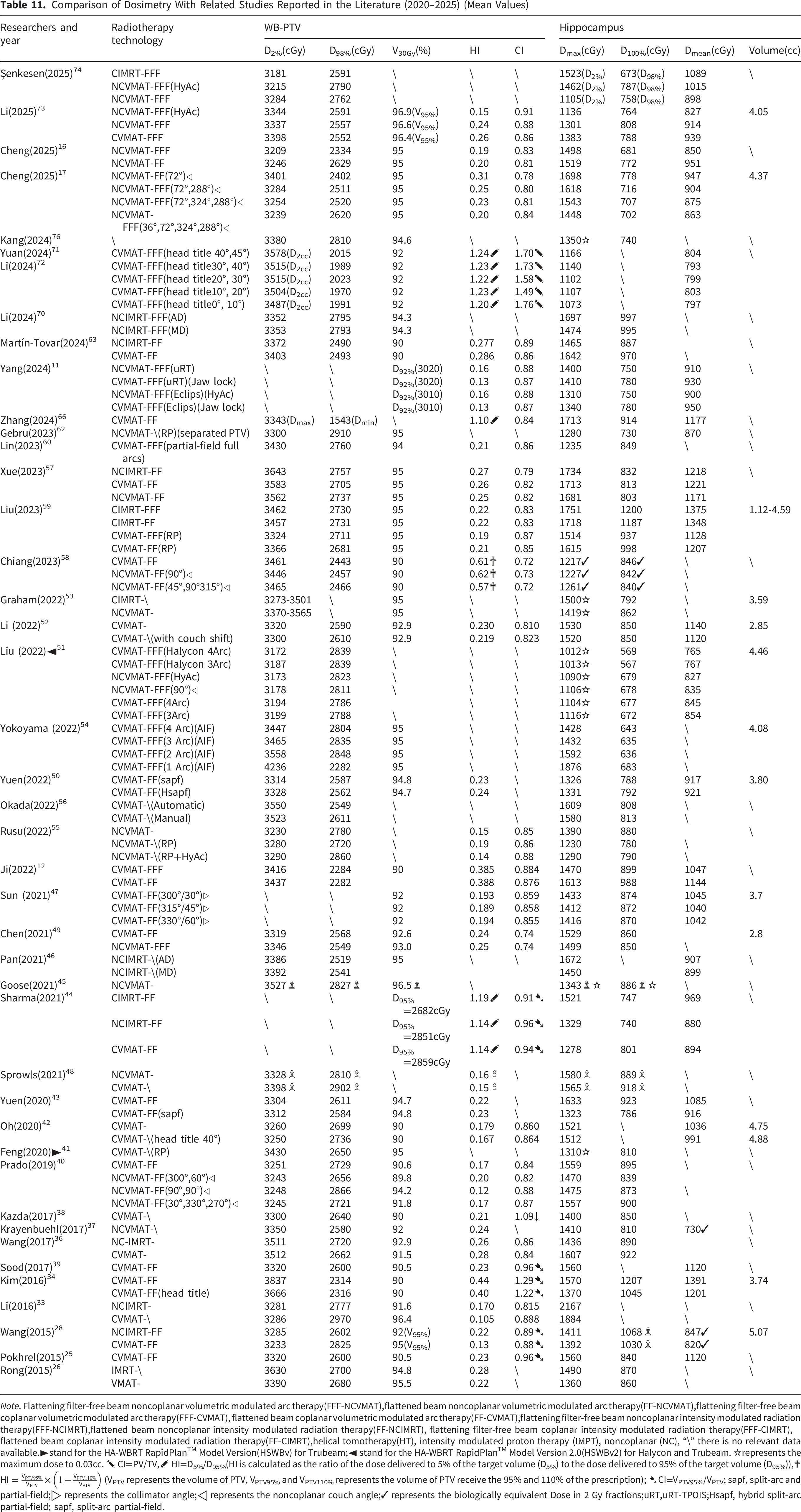
Note. Flattening filter-free beam noncoplanar volumetric modulated arc therapy(FFF-NCVMAT),flattened beam noncoplanar volumetric modulated arc therapy(FF-NCVMAT),flattening filter-free beam coplanar volumetric modulated arc therapy(FFF-CVMAT), flattened beam coplanar volumetric modulated arc therapy(FF-CVMAT),flattening filter-free beam noncoplanar intensity modulated radiation therapy(FFF-NCIMRT),flattened beam noncoplanar intensity modulated radiation therapy(FF-NCIMRT), flattening filter-free beam coplanar intensity modulated radiation therapy(FFF-CIMRT), flattened beam coplanar intensity modulated radiation therapy(FF-CIMRT),helical tomotherapy(HT), intensity modulated proton therapy (IMPT), noncoplanar (NC), “\” there is no relevant data available.►stand for the HA-WBRT RapidPlanTM Model Version(HSWBv) for Trubeam;◄ stand for the HA-WBRT RapidPlanTM Model Version 2.0(HSWBv2) for Halycon and Trubeam. ✫represents the maximum dose to 0.03cc. ✎ CI=PV/TV,✐ HI=D5%/D95%(HI is calculated as the ratio of the dose delivered to 5% of the target volume (D5%) to the dose delivered to 95% of the target volume (D95%)),✟
4.2.1 Hippocampus Delineation
Accurate and consistent hippocampal delineation is fundamental and indispensable for clinically reliable HA-WBRT. In this study, all hippocampal contours were strictly generated in accordance with the RTOG 0933 contouring atlas using T1-weighted MRI sequences registered to planning CT.4,77 All contours were independently reviewed and adjusted by senior radiation oncologists to ensure uniformity across all patients.
Standardized hippocampal delineation is directly critical to the core results of this study because it eliminates interobserver contour variability as a confounding factor. This ensures that the observed differences in hippocampal dose metrics (Dmax, Dmean, D100%, D40%) among the four plan groups truly reflect dosimetric advantages of different platforms and beam modes, rather than contouring inconsistencies. 78
Previous studies have demonstrated that variable hippocampal contouring can significantly alter dose evaluation, 79 and multiple automated or deep learning–based segmentation methods have been proposed to improve consistency and efficiency.41,70,80,81 Nevertheless, rigorous manual annotation and review remain essential for ensuring accuracy in clinical trials and comparative studies.
The strict, consistent, and protocol-adherent hippocampal delineation applied in this study provides a methodologically robust foundation for all subsequent comparative dosimetric analyses.
4.2.2 Comparison of FFF vs. FF and NCVMAT vs. CVMAT in HA-WBRT
This investigation assessed NCVMAT FFF and NCVMAT FF across two radiotherapy platforms (Monaco and uRT-TPOIS), uncovering system-dependent differences while consistently highlighting the enhanced performance of NCVMAT FFF in HA-WBRT. Relative to MC-NCVMAT FF, the MC-NCVMAT FFF approach exhibited notable improvements in target coverage and hippocampal sparing, lower maximum doses to additional organs at risk, and elevated PQM scores, reflecting an overall superior treatment plan. Although MU were higher, MC-NCVMAT FFF achieved a reduction in BOT, thereby boosting delivery efficiency. Conversely, MCS and MD suggested greater plan intricacy. These outcomes are consistent with earlier work, even with an increased cohort size from 15 to 22 participants. 7
A review of the literature (Table 10) reveals that there are relatively few studies on NCVMAT FFF/FF, with the majority of research concentrating on CVMAT-FFF/FF and comparisons between NCVMAT and CVMAT in the context of HA-WBRT. Ji et al. (2020) 12 conducted a comparison of CVMAT-FFF and CVMAT-FF using the Monaco-Versa HD system, which highlighted the benefits of FFF beams, although their results showed lower target coverage (90%) and less favorable dosimetric metrics (e.g., PTV D98%: 2284 vs. 2571 cGy, hippocampal Dmax: 1470 vs. 1375 cGy) when compared to our MC-NCVMAT FFF cohort. In a similar vein, Liu et al. (2023) 59 documented enhanced target conformity (CI: 0.87 vs. 0.81) and homogeneity (HI: 0.19 vs. 0.21) with CVMAT-FFF implemented on the Eclipse-Trilogy system, though this came with elevated hippocampal doses (Dmean: 1128 vs. 859 cGy) that surpassed the thresholds set by RTOG 0933. These findings corroborate the dosimetric advantages of FFF beams relative to FF beams in HA-WBRT. Mishra et al. 82 and Rajadurai et al. 83 likewise noted that FFF-based RapidArc/VMAT techniques resulted in better organ-at-risk sparing while maintaining plan quality in cases of oropharyngeal cancer, as also observed by Domgouo et al. 84 observed a 57% decrease in BOT for smaller targets (48.9 cc) when using FFF beams. In the present investigation, even with a substantially larger whole-body planning target volume (mean 1652 cc), FFF-based MC-NCVMAT achieved an approximate 10% reduction in BOT. Meanwhile, UT-NCVMAT FFF maintained comparable BOT levels despite a 17% increase in MU. These outcomes affirm the benefits of FFF techniques in treatments involving larger target volumes.
In the comparison between NCVMAT and CVMAT, initial research conducted by Moon et al. (2016) 35 using the Eclipse-21iX system indicated that NCVMAT offered advantages when head tilt was not applied, although their methodology did not fully comply with RTOG 0933 guidelines. Subsequent work by Parado et al. (2019) 40 on the Eclipse-Unique platform verified the dosimetric superiority of NCVMAT with FF, particularly at a 90° noncoplanar couch angle. Sprowls et al. (2021) 48 further illustrated that HyperArc-NCVMAT FF (on Eclipse-Edge) resulted in a reduction of OAR doses and a decrease in maximum target dose by 1.3 Gy. Chen et al. (2021) 49 observed limited benefits of NCVMAT FF on the Pinnacle3-Synergy system, except for lens protection, but noted lower target coverage (93%) and less favorable dosimetric outcomes (e.g., PTV D2%: 3346 vs. 3238 cGy, hippocampal Dmax: 1499 vs. 1375 cGy) relative to the findings in our investigation. Liu et al. (2022) 51 introduced the HSWBv2 model employing HyperArc-NCVMAT FFF (Eclipse-Halycon/TrueBeam), which led to enhanced hippocampal sparing (Dmax: 1090 vs. 1274 cGy) and improved target coverage (D98%: 2823 vs. 2571 cGy), despite ongoing challenges in clinical implementation.
Chiang et al. (2023) 58 proposed the use of three C-arcs CVMAT FFF for HA-WBRT, citing comparable dosimetric outcomes across NCVMAT setups, though they observed reduced target coverage (90%) and conformity (CI: 0.72). In a similar vein, Yang et al. (2024) 11 demonstrated that HyperArc-NCVMAT FFF and CVMAT FFF (on Eclipse-TrueBeam) with jaw-lock segmentation performed similarly, albeit with target coverage at 92% and a higher hippocampal D100% (750 cGy compared to 690 cGy). More recently, Li (2025) 73 documented enhanced dosimetric results using HyperArc-NCVMAT FFF (Eclipse-TrueBeam/Halcyon), achieving 97% target coverage and a hippocampal Dmax of 1136 cGy. Taken together, these findings indicate that NCVMAT outperforms CVMAT in the context of HA-WBRT.
The quantity of noncoplanar arcs plays a crucial role in determining plan quality. Previous work from our group (2025) 7 demonstrated that NCVMAT plans using 4 noncoplanar arcs surpassed those with 1–3 arcs in satisfying the “Per protocol” requirements of the RTOG 0933 guidelines, aligning with the findings of Liu et al. (2022) 51 using a 3-arc HyperArc model. Although Xue et al. (2023) 57 reached 95% target coverage with a single NC-arc NCVMAT approach, their results indicated less favorable dosimetric outcomes—for instance, higher PTV D2% (3562 cGy vs. 3238 cGy) and elevated hippocampal Dmean (1171 cGy vs. 859 cGy). In a comparative analysis of delivery platforms, Yang et al. (2024) 11 evaluated 3 NC-arc FFF-NCVMAT plans between the uRT-TPOIS-uRT-linac 506c and Eclipse-TrueBeam systems, reporting similar dosimetric performance alongside reduced delivery times on the uRT-TPOIS system. Expanding on these observations, our research reveals that UT-NCVMAT exhibited superior performance over MC-NCVMAT in terms of target homogeneity and conformity indices, enhanced organ-at-risk protection (reflected through reduced Dmax and Dmean values), higher plan quality metric scores, and improved efficiency—evidenced by shorter beam-on times and reduced planning duration (25 minutes compared to 45 minutes).
In conclusion, NCVMAT FFF consistently exhibits enhanced dosimetric outcomes, improved organ-at-risk sparing, and greater treatment efficiency in HA-WBRT when compared to both NCVMAT FF and CVMAT methods across various platforms. The selection of treatment planning systems, beam models (FFF/FF), and noncoplanar arrangements plays a critical role in determining results, underscoring the importance of tailored optimization for each system to achieve an optimal balance between tumor management and preservation of healthy tissues.
4.2.3 The Dose for Scalp and Upper Neck
The evaluation of scalp and upper neck radiation exposure is essential in HA-WBRT, as it may be linked to alopecia caused by radiation and chronic tissue damage. Emerging research suggests that FFF beams result in reduced out-of-field and skin doses relative to FF beams. According to Yang et al, 85 the depth at which maximum dose occurs in the percent depth dose (PDD) curve was 1.58 cm for 6MV FFF beams and 1.39 cm for FF beams, with FFF beams showing lower peripheral doses that diminish as field size increases. In a study by Athiyaman et al, 86 out-of-field measurements for 6MV beams from Truebeam accelerators revealed that FFF beams administered only 64% of the dose delivered by FF beams, and this difference became more pronounced with larger field sizes. Additionally, an investigation into skin dosimetry for FFF photon beams indicated that while FFF beams lead to elevated skin doses in small fields, FF beams produce higher skin doses in large fields. 87
Despite its clinical significance, a standardized consensus regarding scalp dose limitations in HA-WBRT has yet to be established. Witek and colleagues 88 pioneered the exploration of scalp preservation in HA-WBRT, conducting a comparative analysis between hippocampus-sparing (HP-Sparing) and combined hippocampus-scalp sparing (HP&Scalp Sparing) cohorts. The HP&Scalp Sparing approach resulted in lower maximum scalp dose (2930 cGy compared to 3480 cGy) and mean scalp dose (980 cGy versus 1540 cGy), though it came at the expense of reduced hippocampal safeguarding (maximum dose: 1510 cGy vs. 1450 cGy) and less optimal target coverage (90%). According to Mahadevan et al, 30 maintaining scalp Dmax below 3295 cGy and Dmean under 1634 cGy supported hair regrowth when employing 11-field NCIMRT with FF beams, and documented typical hair regrowth at a mean scalp dose of 1486 cGy. Takaoka et al. 89 conducted a comparison between helical tomotherapy (HT) and intensity-modulated proton therapy (IMPT), revealing that IMPT markedly decreased scalp V10 (37.1% relative to 90.5%) and V20 (6.6% compared to 56.7%) while adhering to predefined thresholds (V10 <80%, V20 <50%). In their assessment of HyperArc, NCVMAT, and CVMAT methodologies, Li et al. 73 reported the mean scalp radiation doses were recorded as 1799 cGy, 1779 cGy, and 1890 cGy, respectively, with HyperArc resulting in the greatest dosage exposure to the upper neck (Dmean, V5-V20). According to Yu et al, 14 scalp dose limitations were established in accordance with the European Particle Therapy Network consensus, advising V30 <15% and Dmean <17 Gy. Meanwhile, Torizuka et al. 90 determined that an EQD2 threshold of 1990cGy for 50% of the scalp volume (EQD2 50%) serves as a predictor for severe permanent alopecia.
In this investigation, scalp and upper neck dosages were assessed across four distinct planning cohorts. Among the MC-NCVMAT FFF/FF and UT-NCVMAT FFF/FF subsets, dose-related metrics were found to be similar. Nonetheless, UT-NCVMAT FFF/FF plans exhibited improved scalp Dmax (3140 cGy) and Dmean (1581 cGy), in addition to lower V10, V15, and V20 values in the upper neck region, underscoring the dosimetric benefits offered by the uRT-TPOIS/uRT-linac 506c platform. It is worth noting that no substantial variations were detected between FFF and FF modes in either treatment planning system group, which may be attributed to the lack of specific scalp and neck constraints within the optimization parameters. These outcomes align with the suggestion by Li et al. 73 to incorporate “as low as reasonably achievable' (ALARA) scalp dose goals during treatment planning optimization. Drawing from the accumulated data, this research advocates for scalp dose thresholds of Dmax(0.03cc) <3200 cGy and Dmean <1600 cGy to optimally reconcile treatment effectiveness and potential adverse effects.
4.2.4 Hippocampal Dose Constraints for Neuroprotection
The hippocampus exhibits notable vulnerability to radiation, and even minimal exposure levels can result in damage to its tissue, subsequently contributing to cognitive impairments. Implementing stringent dose limitations for the hippocampus is essential to preserve its functionality. However, given its deep-seated position within the brain, overly restrictive dose reductions may compromise target coverage and potentially undermine tumor control outcomes. Thus, identifying appropriate dose constraints for the hippocampus holds substantial importance for safeguarding hippocampal integrity, ensuring effective tumor management, and optimizing the design of radiotherapy plans.
Dosimetric Criteria for HA-WBRT in NRG CC001 Trail
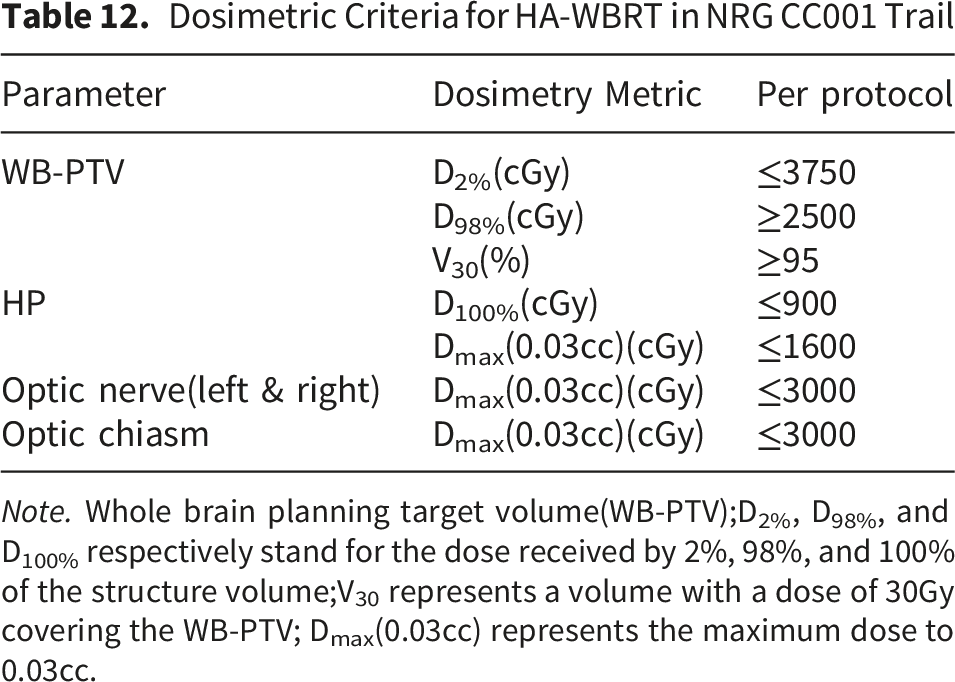
Note. Whole brain planning target volume(WB-PTV);D2%, D98%, and D100% respectively stand for the dose received by 2%, 98%, and 100% of the structure volume;V30 represents a volume with a dose of 30Gy covering the WB-PTV; Dmax(0.03cc) represents the maximum dose to 0.03cc.
Extensively utilized in clinical practice, Dye et al. 93 proposed hippocampal dose limitations of D100% ≤ 9 Gy and Dmax≤16 Gy. Their research revealed that elevated radiation doses to the D100% region of the hippocampus correlated with more significant reductions in Hopkins Verbal Learning Test delayed recall (HVLT-DR) scores. Redmond et al. 94 demonstrated a pronounced dose-response association linking the maximum dose delivered to the bilateral hippocampus and the decline in verbal memory function, suggesting that more rigorous dose restrictions could yield improved outcomes. Within the prospective randomized HIPPORAD trial, 95 the applied hippocampal constraints included D98% ≤ 9 Gy, D2% ≤ 17 Gy, and Dmean ≤ 10 Gy. Clinical assessments indicated that the rate of hippocampal atrophy in the HA-WBRT cohort was nearly threefold lower compared to the standard WBRT group (3.1% versus 8.5%).
The Hippocampal Dose Comparisons (D40% and Dmax) in This Study
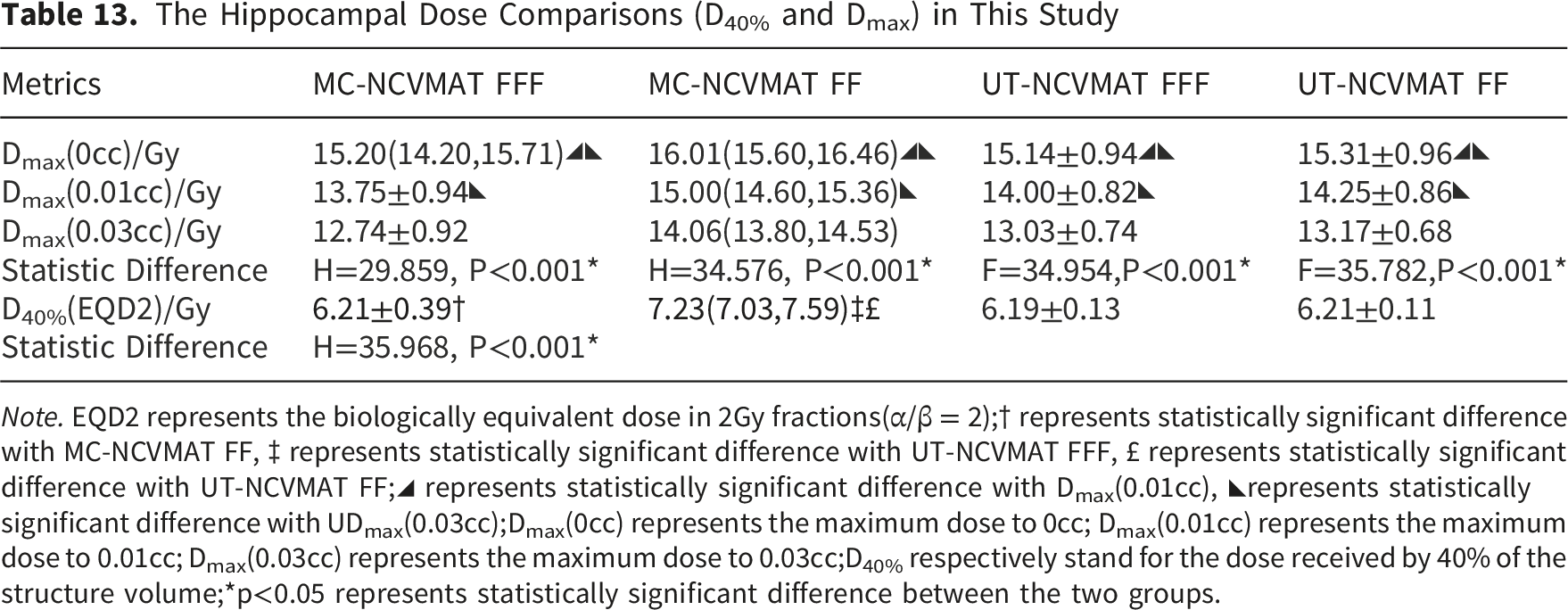
Note. EQD2 represents the biologically equivalent dose in 2Gy fractions(α/β = 2);† represents statistically significant difference with MC-NCVMAT FF, ‡ represents statistically significant difference with UT-NCVMAT FFF, £ represents statistically significant difference with UT-NCVMAT FF;◢ represents statistically significant difference with Dmax(0.01cc), ◣represents statistically significant difference with UDmax(0.03cc);Dmax(0cc) represents the maximum dose to 0cc; Dmax(0.01cc) represents the maximum dose to 0.01cc; Dmax(0.03cc) represents the maximum dose to 0.03cc;D40% respectively stand for the dose received by 40% of the structure volume;*p<0.05 represents statistically significant difference between the two groups.
The investigation revealed that merely five articles explicitly indicated Dmax(0.03cc) as the evaluation method for the hippocampal maximum dose, while the majority employed Dmax(0cc). In summary, this research proposes the following per protocol dose constraints for the hippocampus: D100% ≤ 900cGy, Dmean ≤ 900cGy, Dmax(0.03cc) ≤ 1600cGy, and D40% ≤ 730cGy (EQD2). These criteria may contribute to harmonizing hippocampal dose limitations with target coverage, though additional clinical studies are required for further validation.
In the context of HP-PRV, the majority of HA-WBRT investigations employ a 5 mm margin, though a smaller proportion apply a 7 mm expansion.75,95,96 This preference stems from several studies that have documented a minimal occurrence of brain metastases in proximity to the hippocampus. According to the RTOG0933 trial, 4 just 4.4% of 272 individuals diagnosed with brain metastases exhibited lesions situated within 5–10 mm of the hippocampus, reinforcing the viability of using a narrow margin to preserve tumor control outcomes. With respect to dose limitations for HP-PRV, available evidence is sparse. Initial guidelines from Gondi et al. 97 suggested maintaining Dmax below 30 Gy and V20 under 20% for this region. Nevertheless, the 2020 NRG CCOO1 clinical study 5 clearly indicated that “no particular dose criteria for HP-PRV' are advised, given that this area functions as a transitional dose zone where rigorous constraints could unintentionally elevate the likelihood of tumor recurrence. Such uncertainty underscores the importance of additional research to optimize the trade-off between hippocampal sparing and treatment effectiveness.
4.2.5 Comprehensive Evaluation of HA-WBRT Treatment Plan Quality
The evaluation of HA-WBRT treatment plans necessitates a multidimensional approach that encompasses dosimetric precision, preservation of healthy tissues, and operational efficiency. Traditional assessment methods, which depend exclusively on adherence to RTOG/NRG guidelines, fall short in capturing the subtleties of plan quality. This limitation is evident from the inconsistent clinical results observed even when fundamental dose criteria are satisfied. To address this gap, our research proposes an innovative composite evaluation framework that includes conformity to the target, uniformity of dose distribution, sharpness of dose fall-off, intricacy of the plan, and practical efficiency, thereby establishing a measurable foundation to support clinical choices.
(1) Target Conformity and Homogeneity
CI and HI serve as essential indicators for evaluating dose distribution within the target. Patel et al. 98 carried out a comprehensive analysis tracing the development of CI, HI, and GI, examining the importance of each metric and variations among different computational techniques. Drawing on their findings, this study computed the CI was calculated as (TVprescription)2/(TV×PV), where TVprescription denotes the target volume receiving at least 95% of the prescribed dose. This formulation enforces more rigorous dose coverage criteria than other indices like PV/TV or TVprescription/TV, as adopted in previous HA-WBRT investigations.25,28,34,39,44 Outcomes revealed that UT-NCVMAT FFF plans attained the best CI values (0.91±0.02), markedly surpassing those of MC-NCVMAT FF (0.91±0.02, P<0.001), which reflects enhanced conformity to the WB-PTV. Regarding the HI, expressed as (D2%−D98%)/D50%, UT-NCVMAT FFF demonstrated the smallest value (0.15±0.02), suggesting a more even dose distribution relative to MC-NCVMAT FF (0.21±0.03, P<0.001). These outcomes are consistent with reports that noncoplanar arc arrangements mitigate hot and cold spots through refined beam angle optimization in relation to intracranial structures.58,69,73
(2) Gradient Index and Organ-At-Risk Protection
The gradient index (GI), which measures the dose reduction outside the target region (V50%/V100%), did not exhibit significant variation across the four planning groups (range: 1.55–1.60, P = 0.075). In the HA-WBRT research by Li et al., 74 GI values derived from HyperArc and NCVMAT methods were 1.61 and 1.63, respectively, aligning closely with the outcomes of the present investigation. This points toward a technical stabilization in dose fall-off performance for extensive targets like the whole brain. Nonetheless, UT-NCVMAT FFF displayed enhanced protection of organs at risk, achieving reductions in Dmax(0.01cc) of 6.2–10.3% for the bilateral optic nerves, 4.1% for the brainstem, and 7.4% for the lens relative to MC-NCVMAT FFF (all P < 0.001). Of particular note, the hippocampal Dmax(0.03cc) under UT-NCVMAT FFF (13.03 ± 0.74 Gy) was markedly lower than with MC-NCVMAT FF (14.06 ± 0.82 Gy, P = 0.004), reinforcing the value of volume-based metrics (0.03cc) in hippocampal sparing evaluation, especially since Dmax(0cc) tends to overestimate dose by 16–18% due to localized dose spikes at the voxel level.
(3) Plan Complexity and Delivery Efficiency
MCS and MD were employed to measure the complexity of treatment plans. MCS, derived from a weighted combination of leaf sequence variability and aperture area variability, was found to be lowest in MC-NCVMAT FFF (0.16±0.03), suggesting greater complexity relative to UT-NCVMAT FFF (0.32±0.08, P<0.001). This resulted in extended BOT for MC-NCVMAT FFF (457±14 s) compared to UT-NCVMAT FFF (359±0.09 s, P<0.001), even though target coverage remained comparable. The SPO algorithm in the uRT-TPOIS system helped lower complexity by refining segment shapes, with UT-NCVMAT plans using 38% fewer MU than MC-NCVMAT FFF (1254±73 vs. 2501±179 MU, P<0.001), thereby reducing risks associated with secondary cancers from radiation scatter.
(4) PQM for Composite Assessment
Traditional evaluation of HA-WBRT plans relies primarily on independent dosimetric parameters, which makes standardized comparison difficult. To address this limitation, we adopted a Plan Quality Metric (PQM) system based on the RTOG 0933 protocol, incorporating 16 clinically relevant items including target coverage, homogeneity, conformity, and maximum/mean doses for the hippocampus, optic nerves, lens, and other organs at risk. The PQM score provides a comprehensive, quantitative, and observer-independent measurement of overall plan quality and clinical compliance.99,100
A higher PQM score indicates better adherence to clinical constraints, fewer dose violations, more uniform target dose distribution, and more effective organ-at-risk protection.99,100 This scoring system offers an objective tool for comparing plans across different platforms and reduces inter-observer variability in clinical plan evaluation. In the present study, UT-NCVMAT plans (both FFF and FF) achieved significantly higher PQM scores (97.06±1.18 and 96.16±1.56) than MC-NCVMAT plans.
The clinical significance of this finding is substantial. Higher PQM scores confirm that the UIH uRT-linac 506c/uRT-TPOIS platform generates more clinically robust and protocol-compliant HA-WBRT plans, with better target homogeneity, fewer high-dose regions, and superior protection of the hippocampus, optic nerves, and lens. These advantages are directly associated with a lower risk of neurocognitive impairment and ocular toxicity, which are critical endpoints in HA-WBRT.4-6 Furthermore, the PQM system can serve as a standardized, automated assessment tool to improve consistency and efficiency in clinical practice, supporting high-quality plan delivery across institutions.69,99,100
4.2.6 Template Development for HA-WBRT
The uniform structure of target volumes and OARs in HA-WBRT renders it particularly well-suited for template-driven automated planning. This approach enhances consistency across treatment plans, alleviates the burden on medical physicists, and supports broader integration into clinical practice. Recent progress in machine learning–based planning has led to the creation of tailored models for HA-WBRT. As an example, the RapidPlan™ Version 2.0 model (HSWBv2) was developed to emphasize hippocampal protection without compromising target coverage, adhering to the constraints outlined in the NRG-CC001 protocol. 101 Utilizing an iterative training methodology, this model fine-tunes parameters to reduce hippocampal dosage while improving target conformity and dose homogeneity, leading to superior dosimetric outcomes relative to manually generated plans. The HSWBv2 model offers a tailored framework for HA-WBRT within the Eclipse/Trubeam radiotherapy platform. Nonetheless, since its introduction in 2022, there have been limited reports on its practical clinical implementation in HA-WBRT settings.
For the Monaco/Infinity radiotherapy system, a planning template based on earlier institutional research70,71 was implemented in this study. It employed predefined beam configurations (such as a 1-beam-2-arcs setup) along with specific optimization parameters (including a 2 mm calculation grid and the Monte Carlo algorithm). This standardized approach ensured uniform plan quality across all 22 patients, with each plan satisfying the RTOG 0933 “per protocol” requirements automatically, without the need for manual refinement. Regarding the uRT-TPOIS/uRT-linac 506c radiotherapy system, a tailored template was constructed using previously published beam arrangements, 11 integrating adjusted collimator angles and couch positions. Following initial testing on 5 patient cases, the template was extended to the full cohort of 22 patients. It proved highly efficient, cutting plan generation time to 25 minutes per plan—compared to 45 minutes with Monaco—while also achieving improved organ-at-risk sparing. These templates enhance workflow efficiency by formalizing optimal beam angles, dose constraints, and optimization goals, thereby minimizing variability among planners and guaranteeing.
Despite its advantages, HA-WBRT continues to be underused. A survey conducted in the United States regarding the clinical implementation of HA-WBRT revealed that merely 35% of radiation oncologists would contemplate using hippocampal-sparing radiotherapy for select patients in favorable health. 102 A major obstacle is the perceived challenge of complying with strict dose limitations. Template-driven automated planning tackles this issue by: (1) Ensuring Quality Standardization—templates guarantee uniform compliance with dosimetric guidelines (for instance, maintaining hippocampal Dmax below 16Gy), thereby lowering the likelihood of inadequate treatment plans. (2) Diminishing Reliance on Expertise—automated systems lessen the dependence on advanced physics expertise, broadening the availability of HA-WBRT to facilities with constrained resources. (3) Enhancing Efficiency—by cutting down planning duration from several hours to just minutes, templates facilitate seamless incorporation into demanding clinical routines.
Future initiatives should prioritize the validation of templates across multiple institutions, the incorporation of real-time adaptive planning techniques, and the advancement of artificial intelligence-based contouring systems to enhance automation within the treatment planning workflow. Such progress will be essential for increasing the uptake of hippocampal avoidance whole-brain radiotherapy and for achieving better neurocognitive results in individuals diagnosed with brain metastases.
4.3 The Clinical Implications
Advantages
This study has several notable strengths. First, we systematically compared two representative clinical platforms for HA-WBRT: Elekta Infinity/Monaco and UIH uRT-linac 506c/uRT-TPOIS. Both systems were evaluated using identical NC-VMAT techniques with FFF and FF beams, supporting reliable cross-platform comparisons. Second, we developed standardized non-coplanar VMAT planning templates for both systems, which can improve plan consistency and reduce the workload for medical physicists. Third, we introduced a combined evaluation framework including PQM, MCS, and BOT, enabling objective and standardized plan quality assessment. Fourth, we proposed clinically applicable dose constraints for the hippocampus and scalp to better balance tumor control and normal tissue protection. Finally, Results are generalizable to centers using similar radiotherapy platforms and HA-WBRT protocols.
Limitations
Several limitations should be acknowledged. First, this was a single-center dosimetric study with 22 patients, most of whom had lung cancer metastases, which may limit generalizability. Second, clinical outcomes such as neurocognitive function and survival were not analyzed. Third, the UTNCVMAT plan used 10 noncoplanar arcs, which may increase setup complexity and time. Fourth, the two systems used different dose calculation algorithms (Monte Carlo vs. Collapse Cone), which may introduce minor dosimetric differences, it should be acknowledged that Monaco utilizes the high-precision Monte Carlo algorithm, while uRT-TPOIS adopts the widely used Collapse Cone convolution algorithm. Inherent discrepancies between the two dose calculation algorithms may bring minor systematic deviations to absolute dosimetric results. All plans in this study were calculated using the default clinical algorithm of each treatment planning system in accordance with routine clinical practice. The primary conclusion of this work focuses on the relative dosimetric performance of FFF and FF modes under the same platform rather than direct cross-algorithm absolute dose comparison. This algorithm difference has been recognized as an inherent limitation of the present study.
Limitations related to treatment setup efficiency: The non-coplanar VMAT technique employed five couch angles, which may slightly increase patient setup time compared with coplanar or simplified non-coplanar plans. Although this configuration is clinically feasible and widely used, future studies may explore optimized beam configurations with fewer couch angles to further improve efficiency while preserving dosimetric quality.
Future Directions
Future research directions include: (1) developing and validating AI-based auto-segmentation tools to improve the accuracy and consistency of hippocampal delineation; (2) exploring reduced margins for HP-PRV to further enhance hippocampal sparing; (3) simplifying non-coplanar beam arrangements to improve efficiency while maintaining plan quality; (4) validating the proposed planning templates across multiple centers; and (5) performing prospective clinical trials to correlate dosimetric parameters with longterm neurocognitive outcomes.
5 Conclusions
This study compared the dosimetric and clinical performance of two radiotherapy platforms for HA-WBRT using NCVMAT with FFF and FF beams. The UIH uRT-linac 506c/uRT-TPOIS system may provide significantly improved target homogeneity, conformity, and OAR sparing compared with the Elekta Infinity/Monaco system. FFF beams may offer advantages over FF beams in hippocampal protection and plan efficiency. The 16-item PQM model may enable standardized and objective plan evaluation.
The UT-NCVMAT FFF technique may represent a practical and efficient option for clinical implementation, especially in settings seeking high-quality HA-WBRT with reduced planning workload. Limitations include the single-center design and relatively small sample size. Future multi-center studies and long-term neurocognitive follow-up may help verify these findings.
Supplemental Material
Supplemental Material - A Comprehensive Dosimetric and Plan Quality Evaluation of Non-coplanar VMAT With Flattening Filter-free Versus Flattened Beams for Hippocampal-Avoidance Whole-Brain Radiotherapy: A Multi-Platform Study on Elekta Infinity and UIH uRT-Linac Systems
Supplemental Material for A Comprehensive Dosimetric and Plan Quality Evaluation of Non-coplanar VMAT With Flattening Filter-free Versus Flattened Beams for Hippocampal-Avoidance Whole-Brain Radiotherapy: A Multi-Platform Study on Elekta Infinity and UIH uRT-Linac Systems by Xiao-long Cheng, Lu Zhang, Long Sun, Wen-liang Yu in Technology in Cancer Research & Treatment
Footnotes
Acknowledgements
We thank the medical staff, physicists, and technicians involved in patient care and data collection, as well as all patients and their families for their participation. Gratitude is also extended to Elekta AB and United Imaging Healthcare for technical support, and to the reviewers and editorial team for their valuable input.
Ethical Considerations
Ethical review and informed consent were involved. The ethical guidelines of the Helsinki Declaration were followed, and the study was approved by the Institutional Review Board of Zhejiang Provincial Cancer Hospital (IRB-2025-489(IIT)). Written informed consent was obtained from all patients prior to treatment.
Authors Contributions
Wen-liang Yu conceived of the presented idea. Xiao-long Cheng designed radiotherapy plans. Lu Zhang and Long Sun collected the planning data of all patients in this study. Xiao-long Cheng took the lead in writing the manuscript. All authors provided critical feed-back and helped shape the research, analysis, and manuscript.
Funding
This work was supported by the Zhejiang Provincial Natural Science Foundation of China (LGF22H160050) and the Zhejiang Medicine and Health Science and Technology Plan Project (2025KY715).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated and analyzed during this study are included in this published article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.