
Abstract
Introduction
A subgroup of pancreatic cancer with unstable genome, such as BRCA mutation, may be more sensitive to platinum-based chemotherapy. How to define the patients with homologous recombination deficiency (HRD) status other than BRCA mutation has been a clinical challenge and interest.
Methods
In this retrospective cohort study, we collected NGS data of 163 pancreatic cancer patients from July 2020 to April 2024. HRD score was calculated by 3DMed-HRD algorithm. The median of HRD score of our study population was used as potential cut-off value to determine HRD status. Cox regression was used to evaluate association of HRD status, platinum-based chemotherapy and overall survival (OS). Kaplan–Meier method with log-rank test was performed to analyze OS among different subgroups.
Results
Among the 163 patients, the HRD score ranged from 0 to 76. The mean value was 10.48. The median was 6. With a criterion of HRD ≥6 and/or germline Homologous Recombination Repair (HRR) mutation, a total of 89 patients were considered to be HRD+. HRD+ status was associated with a poor prognosis (HR: 1.46, 95%CI:1.01-2.11, p=0.04). Platinum-based all-time usage would reduce the hazard of death by 34% (HR: 0.66, 95%CI: 0.45-0.97, p=0.03). Among the HRD+ subjects, the initiation of platinum-based chemotherapy might be associated with a longer overall survival (OS: 19.92 vs 15.38, Log-Rank test, p=0.09).
Conclusion
HRD score could be a potential indicator for genome unstable pancreatic cancer patients who would benefit from platinum derivatives. Future study with better design and larger population size would help to determine a proper threshold for clinical application.
Keywords
Introduction
Pancreatic cancer is one of the most lethal cancers. The major pathologic type is pancreatic ductal adenocarcinomas (PDACs) (>90%). 1 Without an effective early screening, only 15-20% of the PDACs present as surgically resectable cases. 2 Thus chemotherapy, whether neoadjuvant or adjuvant, remains a crucial part of the comprehensive treatment of PDAC. With the new chemo regimen NALIRIFOX prolonging the overall survival of metastatic PDAC, 3 and poly ADP ribose polymerase (PARP) inhibitor targeting germline BRCA1/2 mutated PDAC, 4 the latest overall five-year survival rate reported by the Surveillance, Epidemiology and End Results (SEER) Program reached 11%.1,5 However, the low overall survival rate still makes it the third leading cause of cancer-related death in the United States.5-7
Next generation sequencing (NGS) enables scientists to analyze PDAC on a biomolecular level. A subgroup of PDAC with unstable genome was categorized by Waddel, et al in 2015.
8
This subgroup contains defects in DNA damage response (DDR) genes, which causes homologous recombination deficiency (HRD).
8
HRD status potentially defines sensitivity to DNA-damaging agents.9,10 Germline BRCA1/2 mutation is one of the mechanisms causing HRD status, other mechanisms are promoter methylation, other Homologous Recombination Repair (HRR) mutation and other undefined factors (Figure 1). The concept of ‘BRCAness’ was formed to describe the cellular deficiencies that phenocopy those occurring in BRCA1 and BRCA2 deficient cancer cells, as they might share the same sensitivity to targeted treatment such as PARP1/2 inhibitors and platinum derivatives.11,12 Many studies reported platinum-based chemotherapy associated with better prognosis in PDAC with germline BRCA or HRR mutation.10,13 Furthermore, POLO study revealed that PARP inhibitor prolonged progression-free survival (PFS) of germline BRCA mutated patients.
4
Thus, NCCN guideline updated a recommendation of NGS for newly diagnosed PDAC.
14
Relations of BRAC mutation, HRR mutation and HRD status. Abbreviation: HRR, Homologous Recombination Repair; HRD homologous recombination deficiency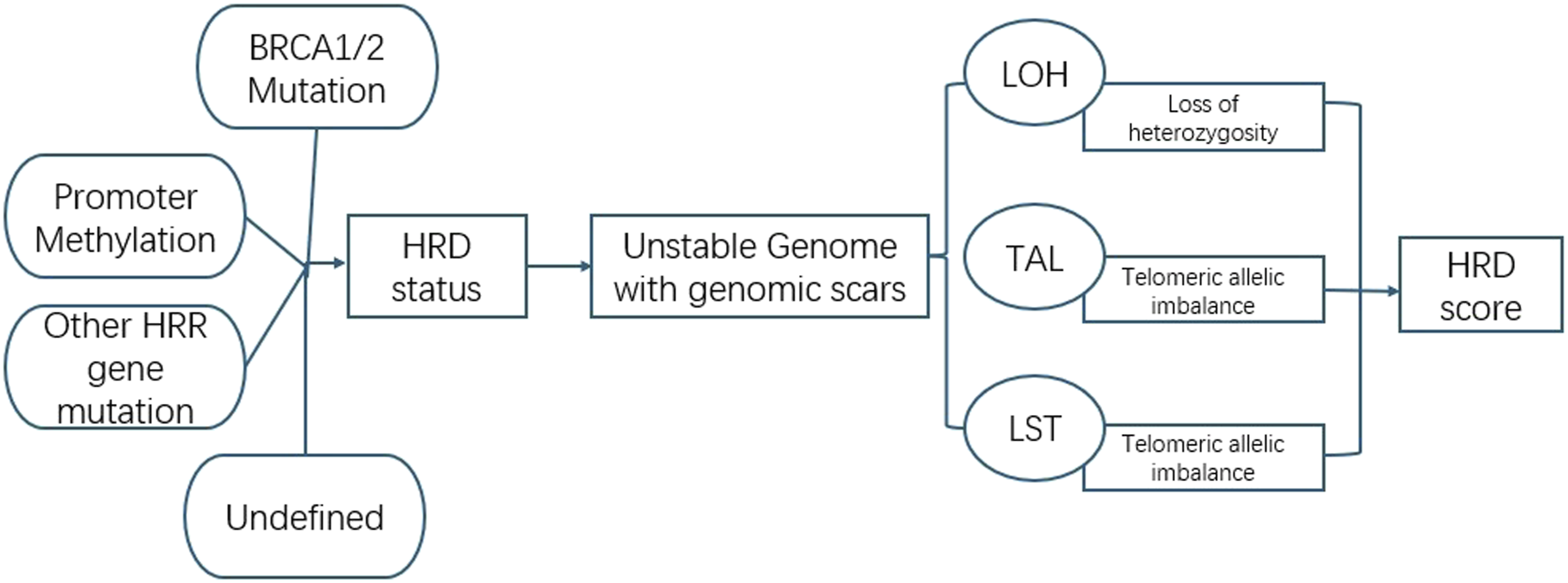
The frequency of germline pathogenic variation in patients with pancreatic cancer is about 9%. 15 The reported frequency of germline BRCA1/2 mutation is 3% in sporadic PDAC, and the number is 5%-10% in familiar PDAC. 16 Since BRCA mutation is not the only event that leads to HRD status (Figure 1), merely checking mutation through sequencing cannot identify all HRD subgroups suitable for targeted treatment. How to expand the platinum-based chemotherapy benefit population has always been a clinical interest and challenge. HRD score is a system calculating tumor genomic instability score (GIS) which includes loss of heterozygosity (LOH), telomeric allelic imbalance (TAI) and large-scale state transitions (LST). 17 In ovarian cancer, nearly 50% patients present with HRD status. Half of the HRD+ cases are due to BRCA mutation. 18 However, report on HRD score application in PDAC is scarce and none published in Chinese population. The criteria for HRD+ varies among different studies, limiting its clinical application. Furthermore, in real world clinic practice, platinum-based chemotherapy and other regimens are often used for the same patient, given the fact that regimens for PDAC is limited. Thus, we conducted this retrospective study to focus on the HRD score in PDAC, aiming to get a scope of the HRD status in PDAC and investigate its value in guidance on chemotherapy regimen selection. This study may help to answer the question: whether and who will benefit from neo/adjuvant treatment with platinum derivatives.
Method
Study Design and Population
This retrospective cohort study initially screened 204 patients with malignant pancreatic tumor who underwent NGS at the Department of Pancreatic Surgery, Huashan University, between July 2020 and April 2024. Inclusion criteria were: (1) Pathological diagnosed malignant pancreatic tumor of epithelial origin; (2) Underwent NGS; (3) Underwent chemotherapy. Exclusion criteria were: (1) No HRD score due to unsuccessful genotyping (2) did not finish least one cycle of chemotherapy of any regimen (3) no follow-up information. After applying these criteria, 163 patients were included in the final analysis (Figure 2). Clinical information including sex, age at diagnosis, tumor stage at diagnosis, family history, secondary tumor history, surgery and chemotherapy information was collected from electronic chart review data. All subjects were followed till death or August 31th, 2025. Patients without death were censored at that point. Survival status was confirmed by electronic chart data or remote phone follow-up. The IRB of Huashan Hospital approved this study (2020-015-1 for approval of recruiting participants for previous cohort, 2026-981 for approval using data from previous cohort for current study). Living patients or their proxies were informed that the de-identified information was used for this study during follow-up phone calls. A written consent was not mandatory for this study. The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2024. The reporting of this study conforms to the STROBE guidelines.
19
Flow chart of enrollment of study subjects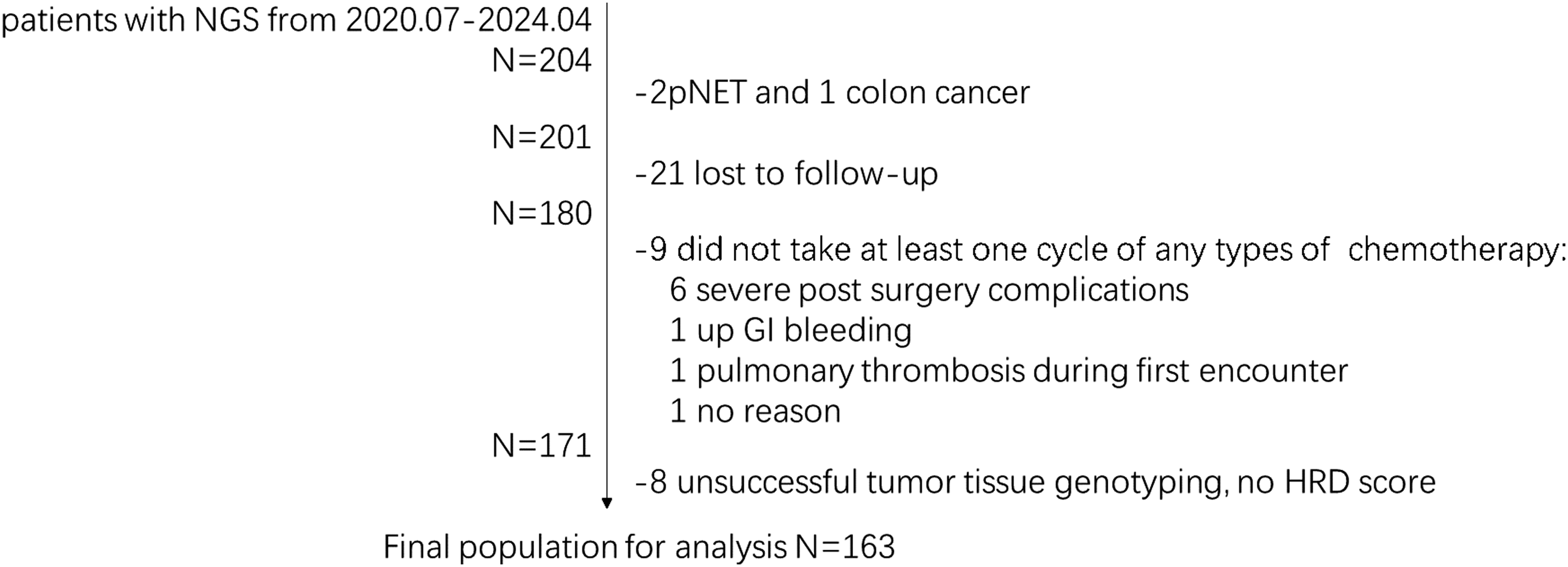
NGS and HRD Score
Tumor tissues and blood samples were required for both germline and somatic tests. Samples for NGS test were acquired from surgery or endoscopy-guided fine needle aspiration (EUS-FNA). Quality check(QC) standard for sample was set to be tumor cells over 20% of overall tissue cells by pathological evaluation. Sample failed QC would proceed with blood test only for possible germline mutation,20,21 leading to no report on somatic mutation or HRD score (Figure 2). All NGSs were performed by 3D Medicines Inc., using an Illumina NovaSeq 6000 platform and 100 bp paired-end read sequencing. For pancreatic tumor, a panel targeting 733 cancer-related genes was used (See details in supplement material). Repetitive elements from intronic baits were filtered out basing on the annotation of UCSC Genome RepeatMasker.
HRD score was calculated using a 3DMed-HRD algorithm aim for the estimation of genomic scar left by unstable genome events. The 3DMed-HRD algorithm is derived from the only FDA approved HRD test kit by MyChoice CDx, Myriad Genetics, Inc. 22 The algorithm is based on over 10,000 single-nucleotide polymorphisms distributed across human genome, which are included in the panel used for pancreatic tumor. HRD was evaluated by the sum of heterozygosity (LOH), telomeric allelic imbalance (TAI) and large-scale state transition (LST), adjusted by tumor ploidy and purity. The 3DMed-HRD algorithm has been validated in Chinese breast cancer and ovarian cancer population. 23
Statistical Analysis
Nominal variables (sex, family history, biopsy method) were described by percentage. Age at diagnosis was sorted into age groups with five-year range (<45, 45-54, 55-64, 64-74, ≥75). 24 Tumor stage at diagnosis was categorized into Ia, Ib, IIa, IIb, III and IV. HRD score was checked for its distribution. Given that there is no generally accepted threshold of HRD score among PDAC population, the median of the HRD score from our study population was used for further analysis in this study. 25 The HRD+ status was defined as holding germline HRR pathway mutation and/or a HRD score over threshold. Chi-square test or Fisher exact test was used for comparison of categorical and nominal data. For all variables, missing values were categorized as a separate group. Survival analysis was performed using Kaplan Meier Curve with long rank test. Cox regression model was to estimate hazard ratios (HRs) and 95% confidence intervals (CIs). Multivariable cox regression model was adjusted for age (<45, 45-54, 55-64, 64-74, ≥75), sex, tumor stage at the time of diagnosis (Stage IV, non-stage IV) and radical surgery (yes or no). All statistical analyses were performed using SAS Version 9.4 (SAS Inc., Cary, NC). 26
Results
Basic Information of Study Population
Basic Information of Study Population
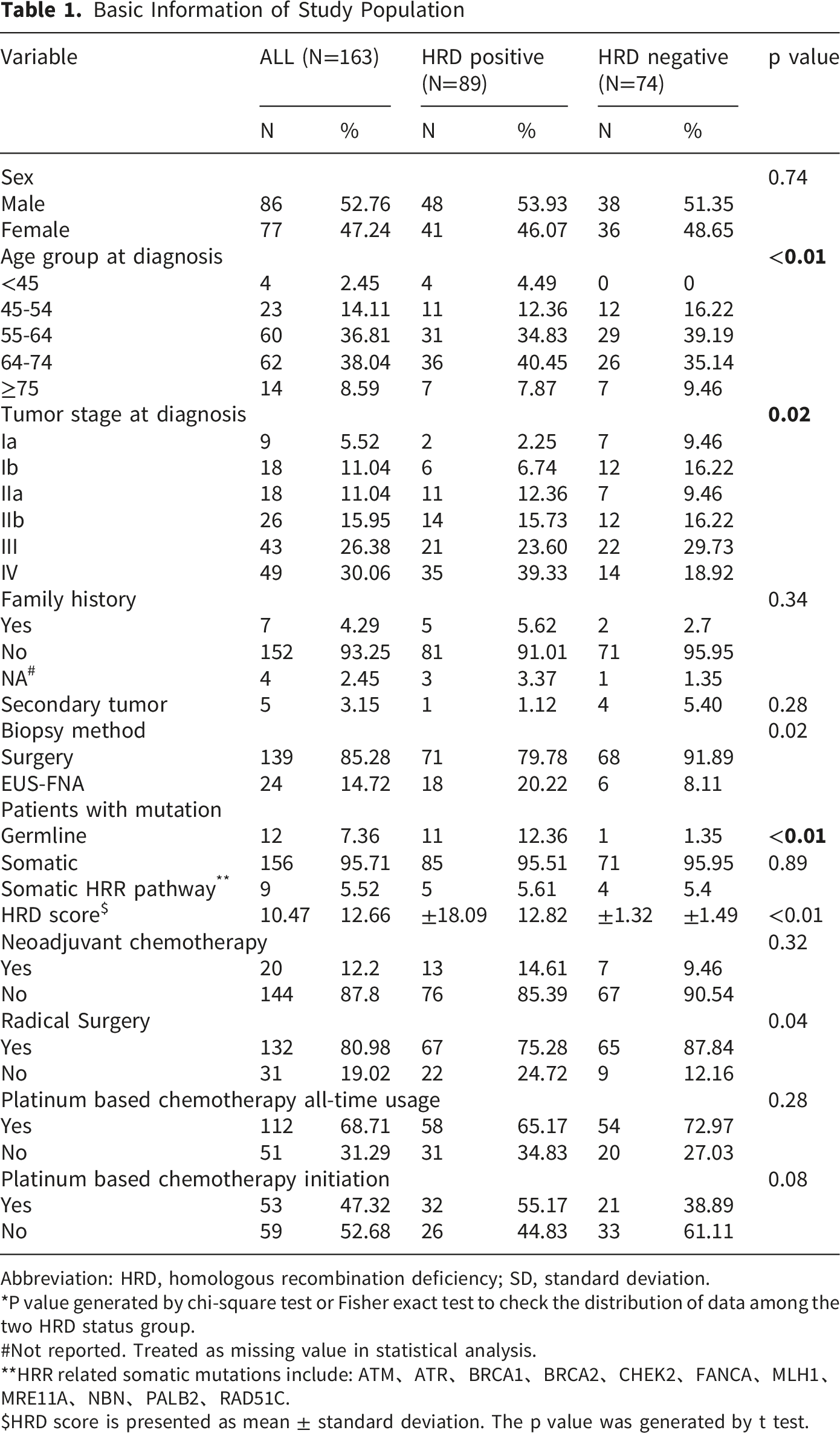
Abbreviation: HRD, homologous recombination deficiency; SD, standard deviation.
*P value generated by chi-square test or Fisher exact test to check the distribution of data among the two HRD status group.
#Not reported. Treated as missing value in statistical analysis.
**HRR related somatic mutations include: ATM、ATR、BRCA1、BRCA2、CHEK2、FANCA、MLH1、MRE11A、NBN、PALB2、RAD51C.
$HRD score is presented as mean ± standard deviation. The p value was generated by t test.
Germline and Somatic Mutation
Among the study population, germline mutation was detected in 12 patients. The germline mutation rate in our population was 8.78%, with BRCA2 being the leading germline mutation, reported in 4 (2.44%) patients. Other germline mutations detected were as followed: PALB2(n = 2), ATR (n = 1), BARD1 (n = 1), BRIP1 (n = 1), EPCAM 1(n = 1), SLX4 (n = 1), TSC1(n = 1).
Somatic mutations were detected in 156 patients, with the most prevalent being KRAS mutations (n = 150, 92.02%). TP53 (n = 113, 69.33%) was the second common somatic mutation. The other leading somatic mutations were CDKN2A(n = 59), SMAD4(n = 32), CDKN2B(n = 23), ARID1A (n = 17), STK11(n = 6), ACVR2A(n = 5), and ATM(n = 4).
HRD Status, Platinum-Based Chemotherapy Usage and Overall Survival Time
Among the 163 patients, the HRD score ranged from 0 to 76. The mean value was 10.48. The median and 75th percentile were 6 and 17. Twenty-six was the 90th percentile of HRD score of our population. The distribution of HRD score of our study population was showed in Figure 3. Basic information of HRD status subgroups is also presented in Table 1. Eleven patients were reported to carry germline HRR mutation and a HRD over 6. One case was found with germline HRR mutation only, while the other 78 cases showed a score over 6 without any germline mutation. Thus, with a threshold of 6, 89 patients were defined as HRD+. Patients of HRD positive status were found be more likely in stage IV at diagnosis (Table 1). Distribution of HRD score in study population. Abbreviation: HRD homologous recombination deficiency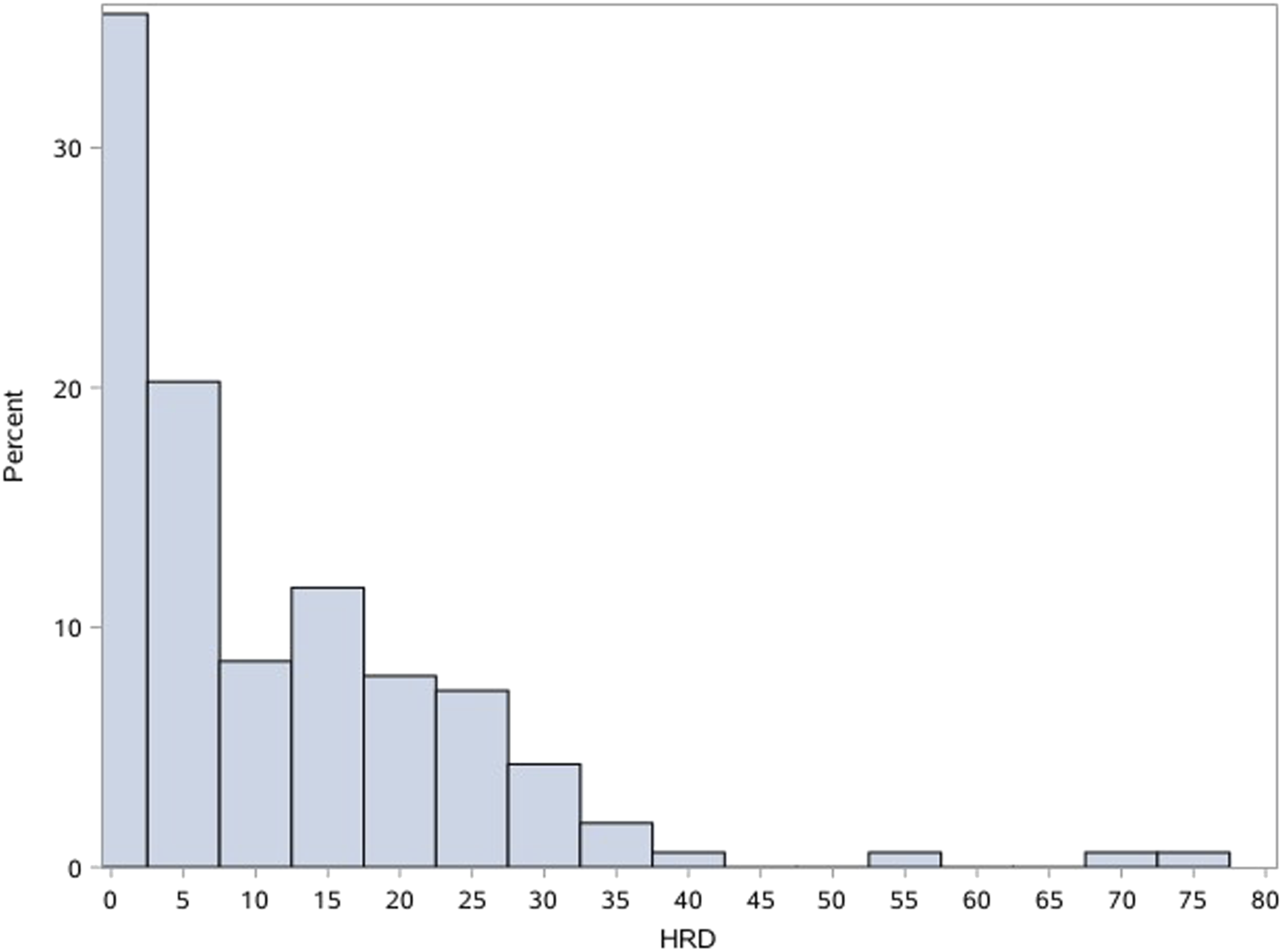
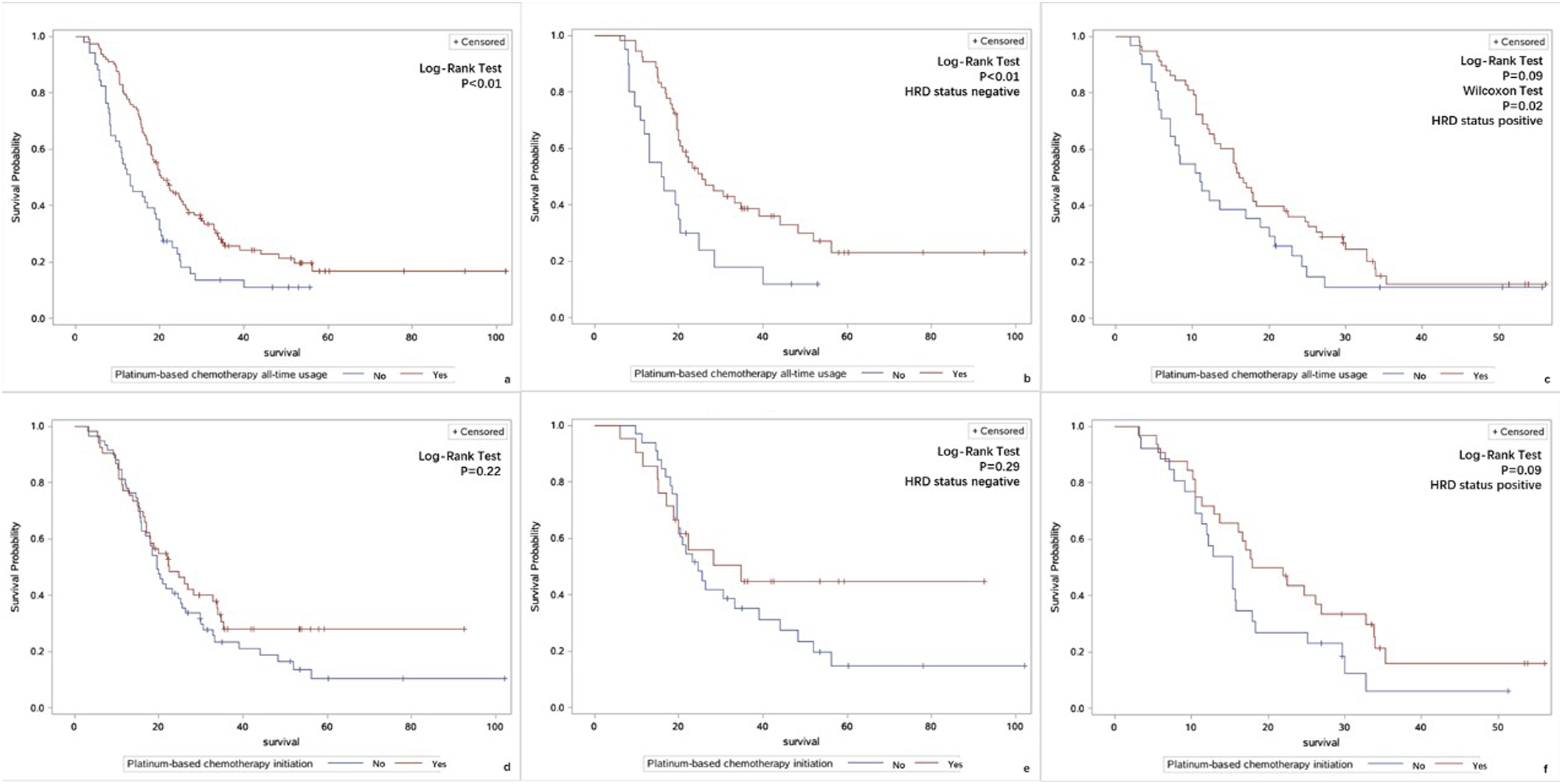
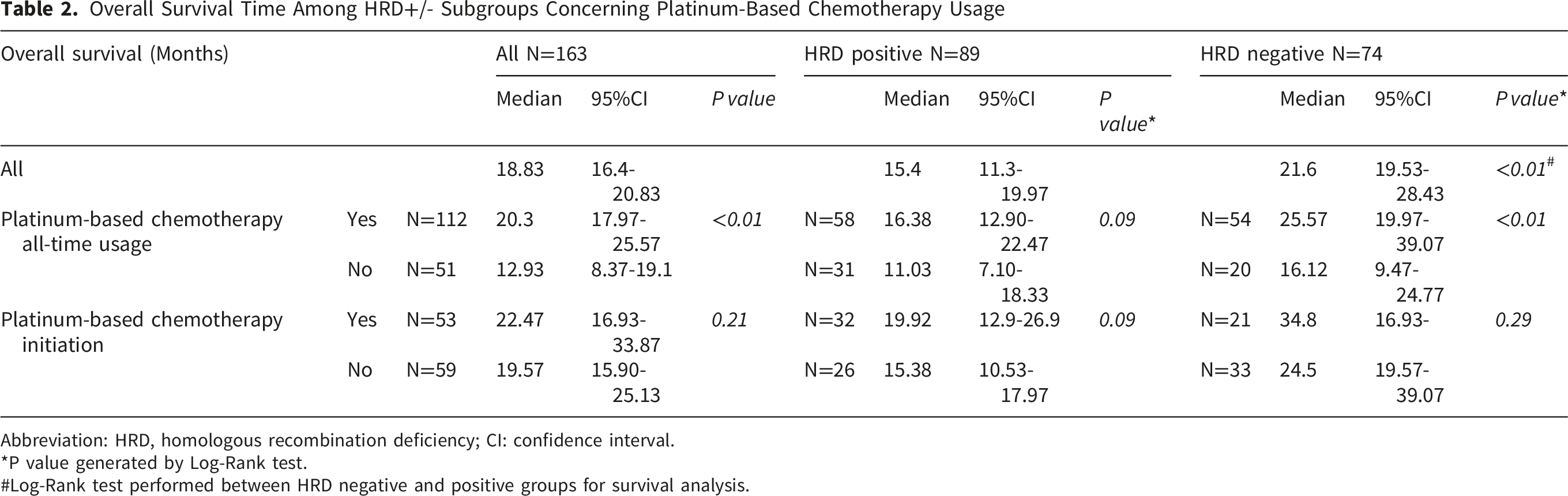
A total of 112 patients used platinum-based regimen during treatment. Fifty-three out of those 112 patients started with platinum-based regimen. The percentage of patients used platinum-based chemotherapy was similar in HRD positive and negative group (68.71% vs 65.17%,p = 0.28). The median OS for HRD positive and negative subgroup of our study was 15.4 months (95%CI: 11.3-19.97) and 21.6 months (95%CI: 19.53-28.43) respectively (p < 0.01, long-rank test) (Figure 4). All-time platinum-based chemotherapy usage was found to be associated with better survival (Log-Rank test, p < 0.01. Figure 5A) compared with no platinum-based chemotherapy usage. This founding was consistent among the group with a negative HRD status (Log-Rank test, p < 0.01. Figure 5B). Among the HRD+ subgroup the trend was also observed (Log-Rank test, p = 0.09. Figure 5C). HRD+ patients were more likely to initiate chemotherapy with platinum-based regimens (55.17% vs 38.89%, p=0.08. Figure 5D). The initiation of platinum-based chemotherapy, compared with latter usage, was not related to a better survival among HRD negative group (Figure 5E). But a trend was observed among the HRD+ group (19.92m, 95%CI: 12.9-26.9 vs 15.38m, 95%CI: 10.53-17.97, Log-Rank test p = 0.09, Figure 5F). Detailed OS information is showed in Table 2. Kaplan-Merie curve of study population stratified by HRD status. Abbreviation: HRD homologous recombination deficiency (A) Kaplan-Merie curve of study population stratified by all-time platinum-based chemotherapy usage. (B) Kaplan-Meier curve of study population with negative HRD status and stratified by all-time platinum-based chemotherapy usage c. Kaplan-Meier curve of study population with positive HRD status and stratified by all-time platinum-based chemotherapy usage. (D) Kaplan-Merie curve of study population stratified by platinum-based chemotherapy initiation. (E) Kaplan-Merie curve of study population with negative HRD status stratified by platinum-based chemotherapy initiation. (F) Kaplan-Merie curve of study population with positive HRD status stratified by platinum-based chemotherapy initiation. Abbreviation: HRR, Homologous Recombination Repair; HRD homologous recombination deficiency Overall Survival Time Among HRD+/- Subgroups Concerning Platinum-Based Chemotherapy Usage Abbreviation: HRD, homologous recombination deficiency; CI: confidence interval. *P value generated by Log-Rank test. #Log-Rank test performed between HRD negative and positive groups for survival analysis.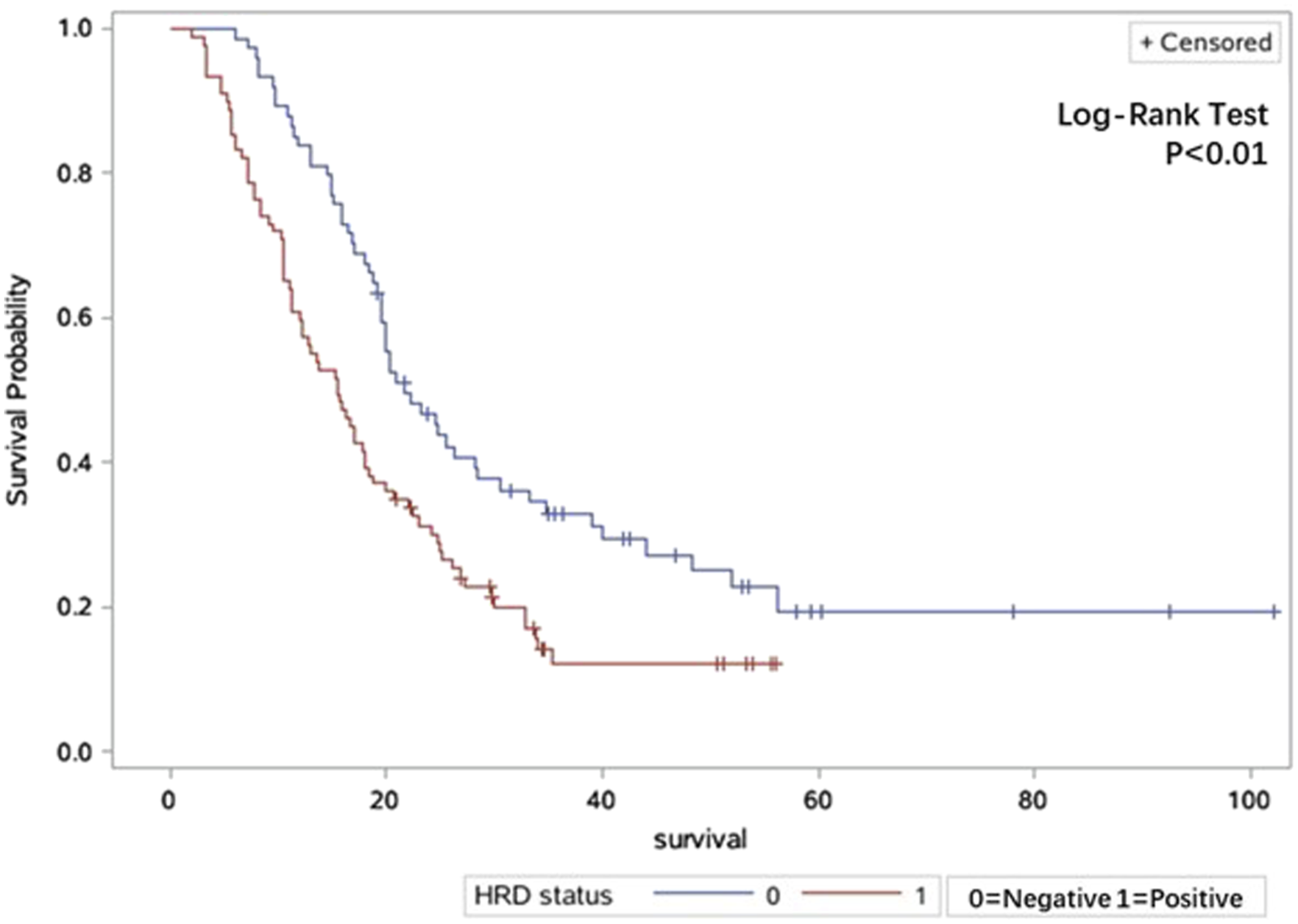
Association Between Factors of Clinical Interest With Overall Survival
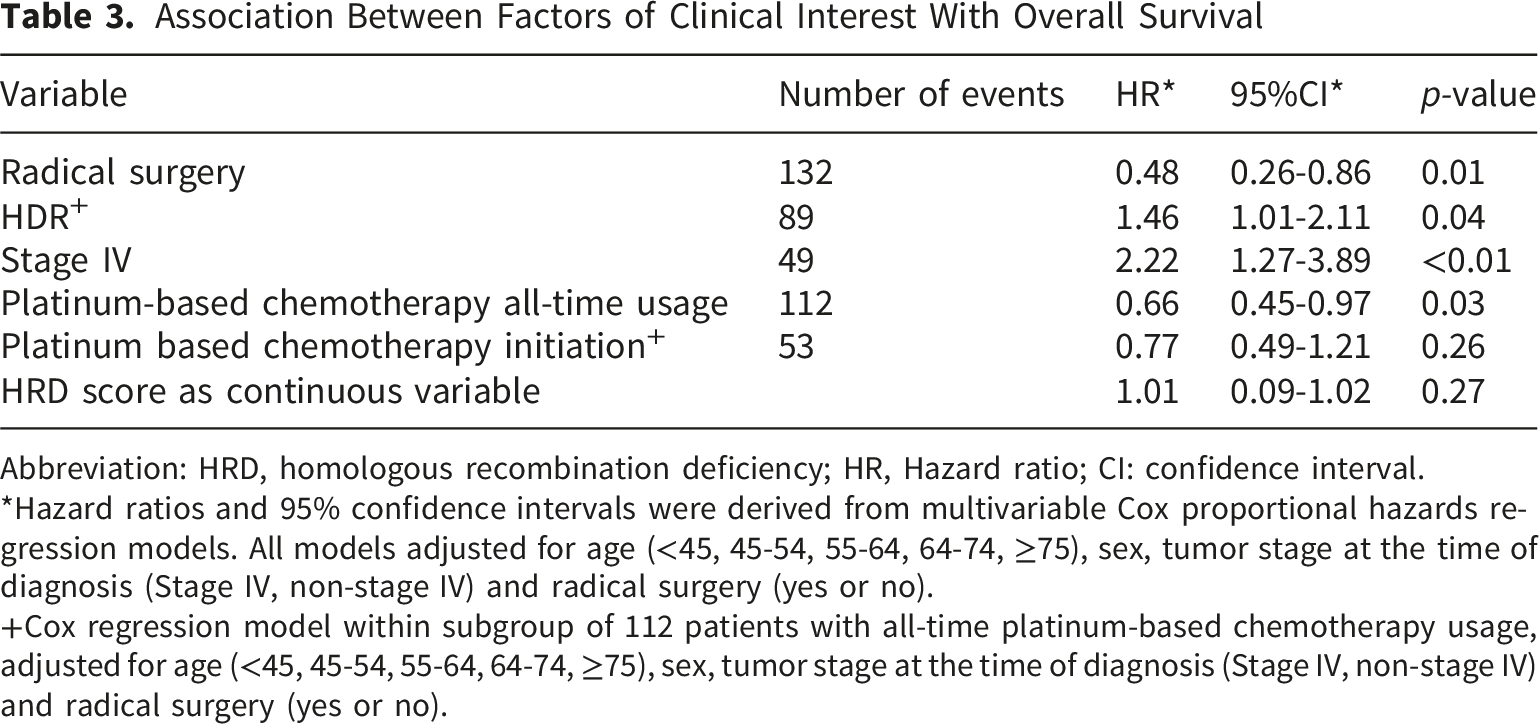
Abbreviation: HRD, homologous recombination deficiency; HR, Hazard ratio; CI: confidence interval.
*Hazard ratios and 95% confidence intervals were derived from multivariable Cox proportional hazards regression models. All models adjusted for age (<45, 45-54, 55-64, 64-74, ≥75), sex, tumor stage at the time of diagnosis (Stage IV, non-stage IV) and radical surgery (yes or no).
+Cox regression model within subgroup of 112 patients with all-time platinum-based chemotherapy usage, adjusted for age (<45, 45-54, 55-64, 64-74, ≥75), sex, tumor stage at the time of diagnosis (Stage IV, non-stage IV) and radical surgery (yes or no).
Discussion
Pancreatic cancer is projected to be the second leading causes of cancer-related death by 2030, causing huge medical and economic burden.27,28 Surgery remains the only possible treatment for long-term survival. 15 One of the reason for its poor prognosis is that precision medicine in pancreatic cancer is relatively lagged behind compared with other cancers. 29 KRAS, the most prevalent somatic mutation in PDAC, remained undruggable for over two decades.30,31 Recently, clinical trials on KRAS g12C, g12D (HRS-4642, GFH375, RMC-9805, etc.) or pan-RAS inhibitor (RMC-6236, GFH276) has emerged. 32 Other new attempts including antibody-drug conjugate (ADC) targeting CLDN18.2,33,34 inhibitor of ubiquitin-specific protease 7, 35 and immune checkpoint inhibitor. 36 Despite these progresses in the development of innovative therapies, chemotherapy remains the cornerstone of the comprehensive treatment of pancreatic cancer. 37 Thus, finding novel specific biomarker indicating chemotherapy sensitivity has always been of clinical interest.38-40 Defining HRD status is one of them. 41
To our knowledge, this is the first study focusing on the application of HRD score in Chinese pancreatic cancer population. With a population of 163 patients, we get a first glance on the HRD score distribution among Chinese pancreatic cancer population. With a threshold of median HRD score, our study revealed that HRD+ status is more likely associated with patients with advanced stage. The usage of platinum-based chemotherapy usage was similar between the HRD positive and negative groups. All time usage of platinum-based chemotherapy decreased the hazard of death. The initiation of platinum-based chemotherapy seemed to be irrelevant of overall survival.
Previous study includes Kondo et al who reported patients with HRR mutation responded better to oxaliplatin-based chemotherapy. 13 However, their sample size of 28 might introduce selection bias to study. Shahda et al, 25 conducted a retrospective study using the Myriad kit. With a population of 78 and a median of 18 as cut-off value, they failed to found out HRD score associated with better overall survival among patients treated with FOLFIRINOX. Chen et la, used a novel algorithm to define HRD Signature (HRDsig), and found HRDsig predictive of FOLFIRNOX chemotherapy benefit with doubled OS relative to gemcitabine and paclitaxel (GP). 42 However, the algorithm and criteria for HRDsig was not described in detail. Thus, indication from previous study that could be applied to real clinical use is scarce. The threshold of 30 is recommended for ovarian cancer. 22 It would not be appropriate to directly apply the same threshold for pancreatic cancer. First reason is the distribution of the data. We can see from Figure 2 that there were a large portion of patients with a HRD score between 10 and 30. Second reason is that carcinogenesis involves many different molecular mechanisms that may weigh differently in different cancer type. Thus, the appropriate cut-off value may vary among different cancer types.
Unlike Shahda et al, 25 we retrospectively enrolled patients of all tumor stages at the time of diagnosis. With the different inclusion criteria and a different sample size, our median value of HRD score differ. With a cut-off value of 6 and/or HRR germline mutation, we classified 89 subjects to be HRD+. HRD positive subjects were found to have a less OS compared with HRD negative subjects. This may be due to a higher percent of stage IV patients among the HRD+ population. Similar findings were reported by Yadav et al among PDAC patients with HRR germline mutation. 43 The trend was statical significant after adjusting for radial surgery treatment and tumor stage, indicating a more progressive tumor behavior of subgroup with HRD. Chemotherapy with platinum derivatives was found to be associated with a better OS among whole study population (cox regression and Log-Rank test) and HRD negative subgroups. The trend was also observed among HRD+ population. However, the initiation of chemotherapy with platinum derivatives was not related to OS. Only a trend of better survival was observed among HRD+ population. A total of 68% of our study subjects received platinum-based chemotherapy, while half of them started with platinum derivatives. Thus, the OS benefit observed with platinum-based regimen all-time usage may be related to a continuance of treatment and better physical fitness to receive intensive regimens. The potential OS benefit we observed among HRD+ subgroup with platinum-based regimen initiation did not reach statical significance. Sample size is considered to be one possible explanation. An exact threshold to determine HRD+ population for targeted therapy may need further investigation with more data of a larger sample size.
One of our limitations is a relatively small sample size. Our study showed that the overall germline mutation frequency was 8.33%. This is similar to the frequency from previous study.15,16,44,45 The rate of germline BRCA and PALB2 mutation, and the most frequent mutated somatic genes all accorded to previous studies.16,46,47 This means our population could be considered representative. The actual impact of a small sample size may be on the event number needed for survival analysis and insufficient cases for subgroup analysis concerning tumor stages or HRD score in more details. With more event, the trend we observed that patients with HRD+ would benefit more from platinum-based initiation may reach statical significance. Another major fallback is the lack of disease progression information necessary for progression-free survival (PFS) analysis. Due to the difficulty in collecting detailed disease progression information in a retrospective study, we didn’t include PFS in the final analysis. Thirdly, survival time is not a binary variable but a time-dependent one. Thus, AUC curve could not be applied to our data for a cut-off value. Future direction would be on both longitudinal and horizontal level. Prospective study with a large population is granted. If we wish to set-up a cut-off value by the traditional AUC curve, an outcome reflecting treatment response on the molecular level may be better than the overall survival time. Novel approach such as artificial intelligence assisted algorithm may be another direction that worth trying.
Conclusion
HRD score may have the potential to indicating genomic unstable pancreatic cancer patients other than those who carries germline HRR mutation. Among our study population, a positive HRD status was found to be associated with advanced disease stage, while the usage of platinum-based chemotherapy was associated with better outcome. Future study with better design and larger population size is needed for the determination of a proper threshold for clinical application.
Supplemental Material
Supplemental Material - HRD Score: A Promising Biomarker for Genomic Instability Evaluation for Targeted Treatments Among Pancreatic Cancer Patients
Supplemental material for HRD Score: A Promising Biomarker for Genomic Instability Evaluation for Targeted Treatments Among Pancreatic Cancer Patients by Xiaoyi Wang, Qingyun Zhang, Yecheng Xu, Wenteng Miao, Bai’an Tao, Chen Jin and Deliang Fu in Technology in Cancer Research & Treatment.
Footnotes
Acknowledgements
The authors declare that the views expressed in the submitted articles are those of the authors and do not represent the official position of the organisations or funders.
Ethical Considerations
The IRB of Huashan Hosptial, Fudan University approved this study.
Author Contributions
Conceptualization, Xiaoyi Wang; methodology, Xiaoyi Wang, Qingyun Zhang, Wenteng Miao; software, Xiaoyi Wang, Bai’an Tao; validation, Xiaoyi Wang, Qingyun Zhang; formal analysis, Xiaoyi Wang; resources, Xiaoyi Wang, Qingyun Zhang; data curation, Wenteng Miao, Xiaoyi Wang, Bai’an Tao, Yecheng Xu; writing—original draft preparation, Xiaoyi Wang; writing—review and editing, Xiaoyi Wang, Chen Jin, Deliang Fu; visualization, Xiaoyi Wang, Bai’an Tao; supervision, Deliang Fu, Chen Jin; project administration, Xiaoyi Wang, Deliang Fu; funding acquisition, Xiaoyi Wang. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Shanghai Municipal Health Commission project (202240380): Study on AI assisted Genetic Risk Score based pancreatic adenocarcinoma risk prediction model.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.