
Abstract
Although the traditional emphasis on overt symptomatology leads readily to diagnosis, such categorization typically assumes a pathological process within the individual that may at best be managed or modified. Conceptualization of symptoms in terms of adaptive and functional considerations may facilitate and broaden options for treatment, potentially improving outcome. This case study provides an example of treatment of schizotypal personality disorder using such an approach. Psychotherapy and medication were directed toward alleviating symptoms of anxiety and depression producing functional impairment in memory, and development of interpersonal skills to increase prospects for reinforcement in interaction with others was implemented to decrease the need for fantasy as a means of obtaining such gratification. Psychotherapy focused on selectively reinforcing positive self-statements, social skills training, and anxiety reduction. Serendipitous peer modeling also facilitated therapeutic efforts. The anxiolytic buspirone, the serotonin-selective reuptake inhibitor citalopram, and the stimulants dextroamphetamine and amphetamine, and methylphenidate were effective in pharmacologic management. This treatment approach was found to be beneficial not only in terms of self-report and peer appraisal but also in results of psychological assessment, including a neuropsychological screening measure.
Keywords
1 Theoretical and Research Basis for Treatment
Schizotypal personality disorder is characterized by impaired interpersonal functioning and oddities in thought and behavior. The resemblance of the latter to symptomatology in the schizophrenic disorders may warrant consideration of treatment with antipsychotics. Another conceptualization that might suggest an alternate emphasis on manifestations of Axis II psychopathology is that proposed by Millon (Davis, 1999), which regards personality functioning as essentially functioning as an immune system mitigating the development of Axis I pathology. However, such a perspective does not preclude the possibility of an interactive relationship between Axis I and Axis II pathology, with symptoms in the former exacerbating ineffective adaptive efforts in the latter in a cyclic manner. Such a relationship provides the possibility that effective alleviation of Axis I symptoms may result in reduction of Axis II symptomatology. The following case study provides an example of the efficacy of this approach. The presenting problem of memory lapses appeared to be due to preoccupation with fantasies. Although this could have been regarded as manifestations of thought disorganization/disorder, warranting use of antipsychotic medication to control symptoms, consideration of the functional utility of fantasy preoccupation as a means of reducing anxiety suggested that decreasing anxiety would likely diminish such preoccupation and memory lapses.
2 Case Introduction
Symptoms of schizotypal personality disorder include odd beliefs, fantasies, or preoccupations. The disorder is often treated with antipsychotics. However, the clinical presentation and occupational situation of the subject of this case study warranted an alternative treatment approach. First of all, the patient had overwhelming anxiety that was the foundation of his interpersonal oddities and elaborate fantasy life. Second, the case subject was in the military, where antipsychotic use is considered incompatible with military service and requires immediate discharge. Finally, the subject of the case showed potential to derive benefit from cognitive and behavioral approaches. The details of his presentation, assessment, treatment, and outcomes are provided, followed by implications for clinicians.
3 Presenting Complaints
William F. was a 21-year-old single Caucasian male with 2 years’ time in service, who had deployed to Iraq with his unit as a combat infantryman. He was referred by his Commander to the Camp Liberty Combat Stress Clinic for memory lapses. Although his duty performance was otherwise rated as “good,” these lapses resulted in periods of inattentiveness and lack of awareness of surroundings of sufficient concern to warrant taking his weapon as a safety measure.
William stated that he began to have what others would describe as odd thinking when he was in basic training. William also reported recurrent episodes of losing track of time for intervals of approximately 5 min, which started when he was assigned to Korea approximately 1 year ago. The gaps in time, which were getting longer in duration and becoming more frequent, typically entailed ego syntonic fantasy experiences and a sense of loss of volitional control. William gave an example of walking to an unspecified location, in the presence of an unspecified individual, where he could feel his feet move but could not recall making the turns to get to his destination and experienced no visual indications of movement. He would lapse into a fantasy during this time, and when the fantasy ended, he had the sensation of someone “changing the channel.” In another example, during the course of a conversation about baseball, he lapsed into a fantasy, in a “figurative, fictional” setting, where “perhaps” he was a baseball player. When he would laugh in amusement or make reference to the fantasy, people around him would indicate that they did not know what he was talking about. William commented that he would have no “recreation” (i.e., recollection) of how he departed from his interaction with others. He described a sensation of being “sucked into it,” feeling that he had no control over entering into a fantasy, and commented that he did not hear as well when it was occurring. He stated, “I didn’t know I was in it till I was in it.” He apparently regarded these experiences as unique and interesting, and compared them to “an alcoholic beverage that sneaks up on you.” William explained further that he felt like he was two separate people; in contrast to his usual sense of himself as an introvert, the part of him that participated in the fantasy was more of an extrovert. He compared himself to the “subconscious of someone who’s trapped.” He described one of his fantasies as feeling as though “someone had injected speed into my membrane.” Sometimes he would “rewind himself,” to replay a fantasy scenario over and over again.
Although at least some of his fantasies were self-enhancing, William described his actual role in society as “comic relief.” In this capacity, he served as a laughing stock, affording others the opportunity to compare themselves to him and concluding that they were not that bad off after all. He lacked close friends or confidants in his unit as well as prior to joining the military.
4 History
William expressed unwillingness to talk about his mother but described her as a person who habitually smoked marijuana and “lived for the party,” and he felt that he was a hindrance to her social life. His own social functioning was extremely limited. He had only one friend and did not engage in social activities or dating. William felt as though he was never taken care of. In his late teens, he was thrown out of the house and was rendered homeless. He recalled fighting over food with other homeless people and often felt threatened. He briefly lived with his sister and later his brother, and recalled that these arrangements were strained because he did not know how to do basic household tasks. He enlisted in the military and went on full-time active duty in response to his brother’s suggestion that he join the army. While in Korea, his first duty station, he experienced the initial onset of the fantasies. This brought him into mental health treatment for the first time, though he only went a few times because he “didn’t like the way it was going.” While in Korea, he attended the University of Maryland at an extension campus and studied psychology, attaining a C-minus average.
5 Assessment
Mental Status Exam
On mental status exam, William was noted to be alert, fully oriented, and attentive to the interviewer. He slouched in his chair but made good eye contact. His speech was pressured, digressive, and idiosyncratic. Thought processes were notable for looseness of associations. Suicidality and homicidality were absent. His mood was anxious, and his affect was constricted. Insight, judgment, and impulse control were intact.
William endorsed some depressive symptoms, reporting that he no longer enjoyed researching things on the computer or drawing, previously two of his favorite pastimes. He reported persistent low mood as well as frequent anxiety, feeling on edge, and concentrating poorly. His sleep was poor, with initial and middle insomnia. He denied manic symptoms. He denied that his experiences were that of depersonalization or derealization, in that he was not having out-of-body experiences and he did not experience the world as strange or unreal. Rather, he was able to feel his body going through the motions of going form one place to another. He had a strong awareness of lapsing into a fantasy and maintained a sense of connectedness with it, and he had memory of the fantasy. However, he experienced the fantasy as real, thus likening it more to a psychotic than a dissociative experience. He denied any substance-use disorder symptoms, indicating that he never drank alcohol or used street drugs at all.
Initial Testing
In view of the presenting problem of memory lapses, neuropsychological screening and cognitive testing were deemed warranted as well as personality testing to aid in differential diagnosis. The following measures were administered:
Wechsler Abbreviated Scale of Intelligence (WASI; Figure 1)
• Repeatable Battery for the Assessment of Neuropsychological Status (RBANS; Figure 2)
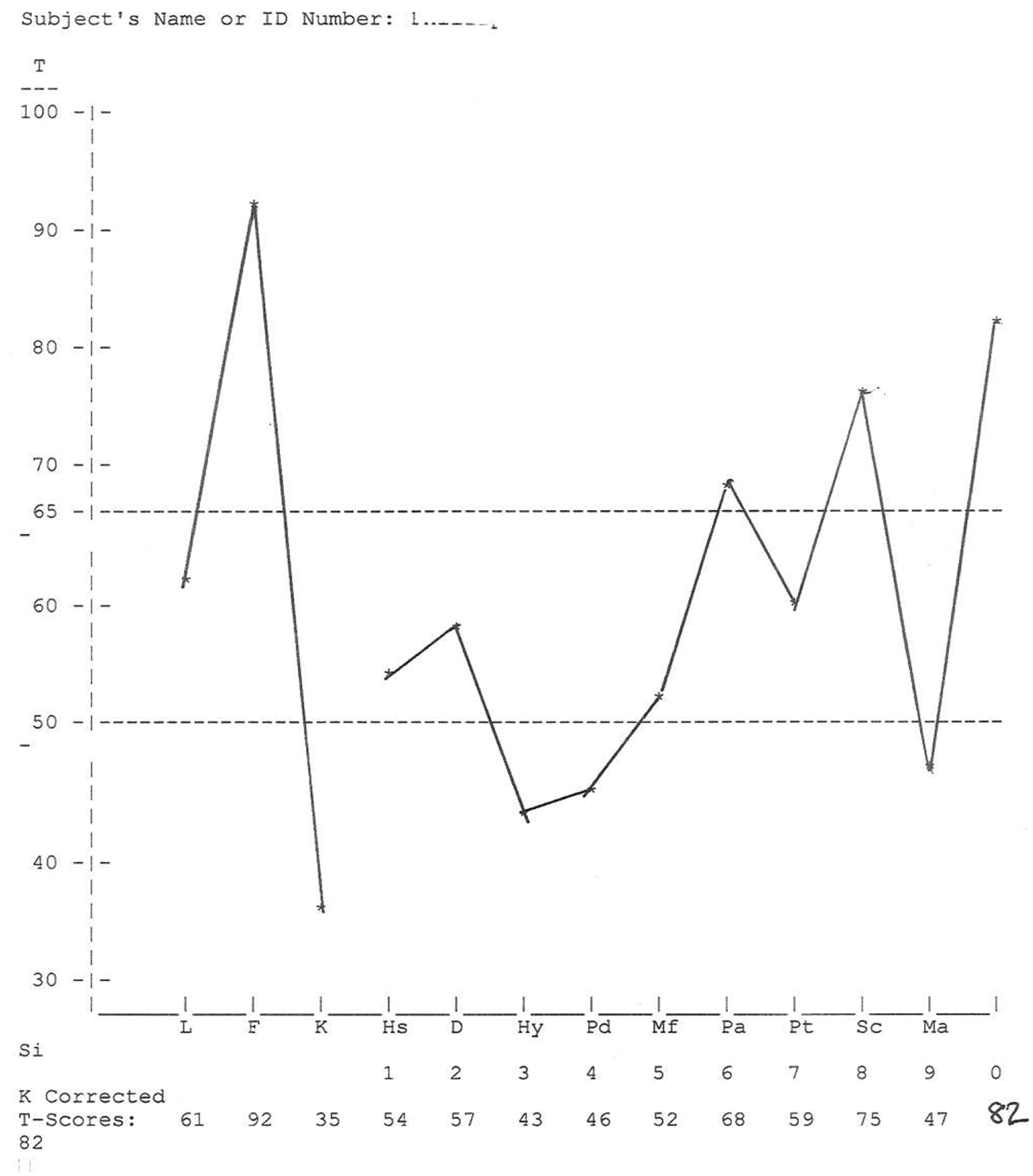
Minnesota Multiphasic Personality Inventory–Second Edition (MMPI-2; Figure 3)
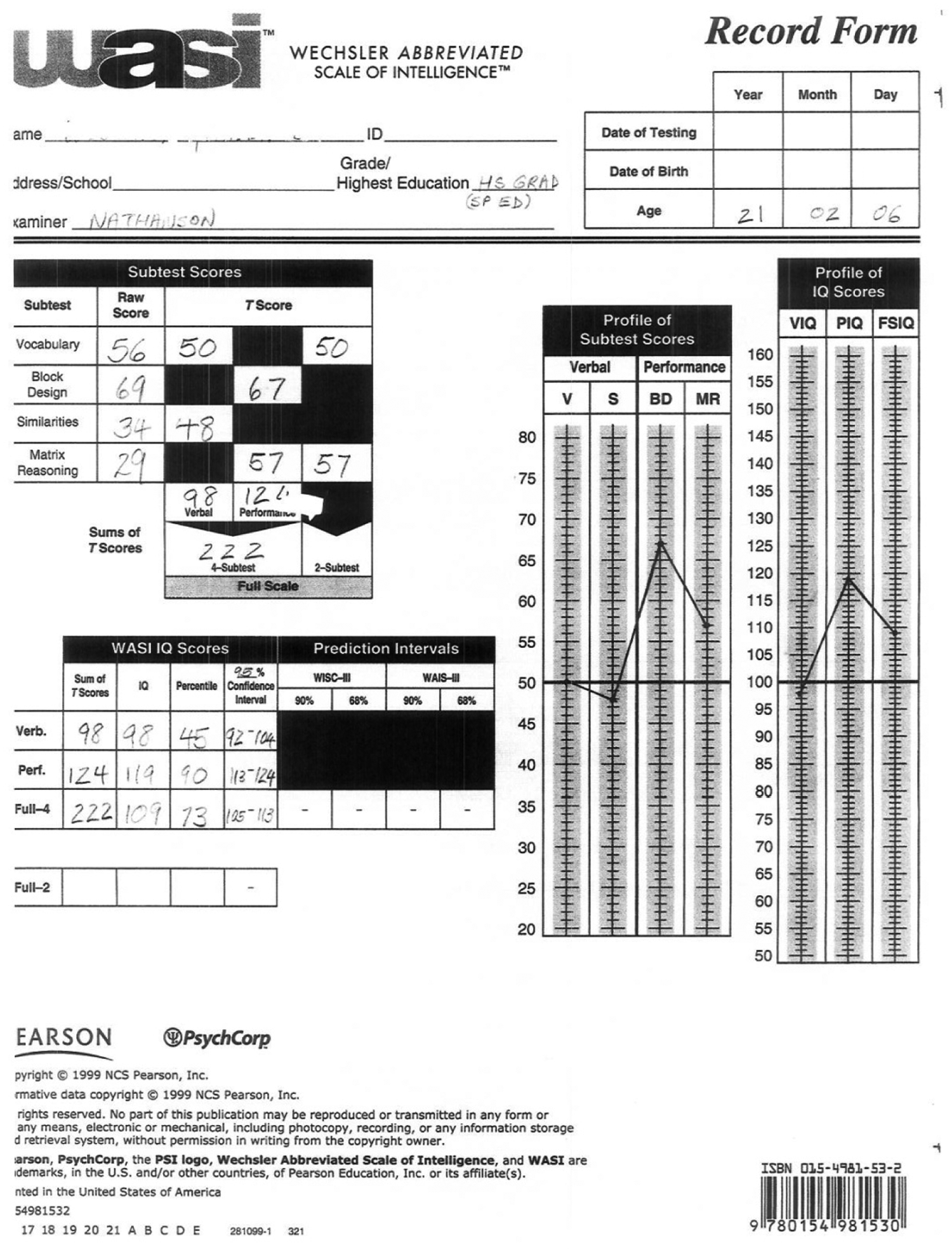
WASI
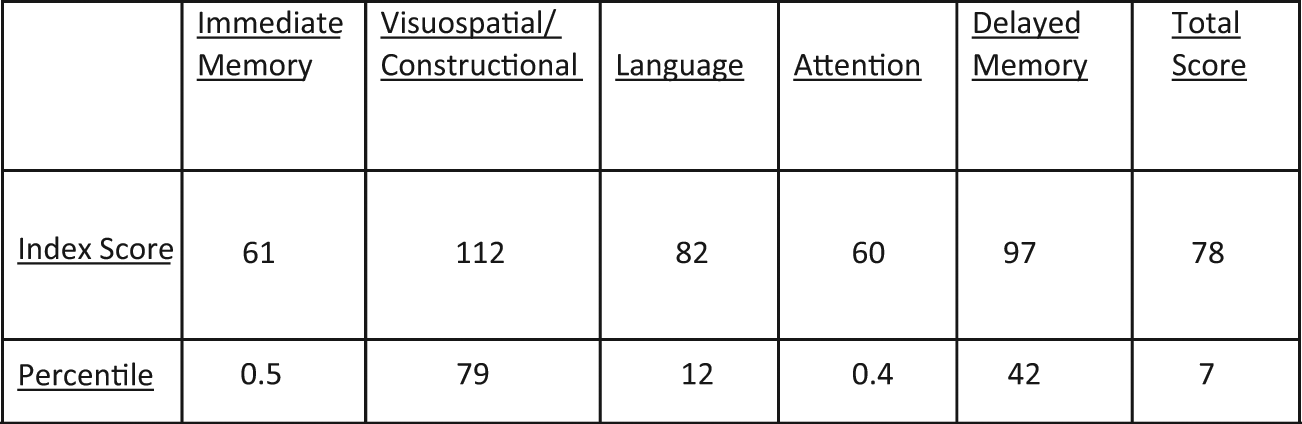
RBANS, initial administration
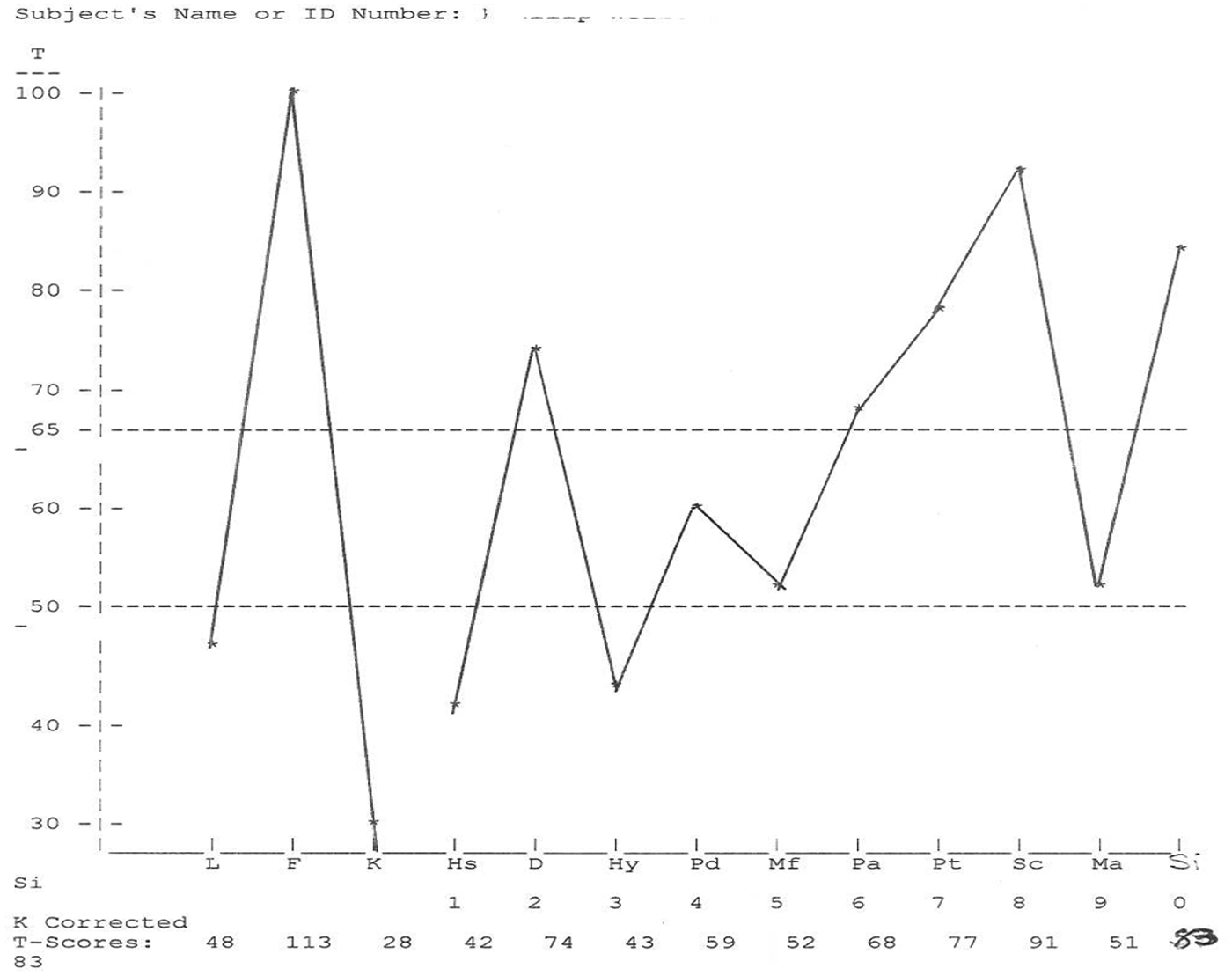
MMPI-2, initial administration
William put forth good effort and appeared motivated to do well. Brief assessment of intellectual functioning indicated that verbal IQ was in the average range and performance IQ was at the upper limit of the high average range. RBANS scores reflect significant impairment in immediate (short-term) memory. William’s score in delayed memory was substantially higher than his score in immediate memory. In view of WASI scores, MMPI-2 scores, clinical presentation, and self-report, the most probable explanation of the preceding finding is anxiety-based impairment.
William’s MMPI-2 profile was invalid due to his endorsement of an inordinate level of items associated with unusual or pathological attributes. This is considered likely due to acute distress, rather than intentional misrepresentation. Although validity considerations preclude conventional interpretation of the clinical profile, tentative qualitative inferences may still be derived from test scores. Individuals with similar profiles typically express fear that they are “going crazy” and are apt to manifest significant symptoms of anxiety and depression. Marked discomfort in social situations, as well as interpersonal alienation, wariness, and mistrust, are also reflected.
Findings are suggestive of deficits in social skills and knowledge of social conventions. Doubt and uncertainty regarding capabilities for meeting situational demands are likely characteristic. It is felt that supportive measures directed toward anxiety management and development of skills for social interaction and elicitation of needed support may be beneficial.
Although psychometric and clinical interview data reflected interpersonal deficits and relative strength in nonverbal problem-solving skills characteristic of a pervasive developmental disorder such as Asperger’s, William’s marked cognitive slippage, that is, malapropisms and oddities of expression and perception, was consistent with an impression of thought disorder. He did not report auditory or visual hallucinations but did note frequent perceptual alterations and bizarre fantasies. His belief that his purpose in life was comic relief for others is suggestive of ideas of reference. His interpersonal functioning reflected an absence of intimate relationships, wariness/mistrust of others, and excessive anxiety in social settings. His affect was constricted, and his behavior was often eccentric or peculiar. The aforementioned is consistent with a diagnostic impression of schizotypal personality disorder.
Although William did not meet the requisite number of behavioral criteria to warrant the diagnosis of a depressive or anxiety disorder, these symptoms were considered a sufficiently significant source of distress and functional impairment to make them important initial foci of treatment.
6 Case Conceptualization
As indicated above, William’s clinical presentation when initially seen reflected significant dysfunctionality in thinking, perception, and reality testing, and marked deficits in interpersonal skills. However, his ability to meet the demands of the military for more than 2 years, including a prior overseas deployment, suggested a greater coping capacity than expected with such symptomatology. It was noted that William’s fantasies and distortions could be understood as sources of reinforcement and means of compensating for feelings of inadequacy and social ineptitude. His persisting anxiety and depression were regarded as indications of the limited efficacy of these measures, and a potential motivation for acquisition of alternate adaptive measures. Improving skills to increase the likelihood of external reinforcement from social and work environments was accordingly regarded as the most promising approach to decrease anxiety and reliance on dysfunctional distortions to alleviate distress.
7 Course of Treatment and Assessment of Progress
Initial Safety Measures
Due to William’s memory lapses, his weapon was taken from him, and he was assigned a noncommissioned officer escort as safety measures. The escort remained with him at all times, and William came to regard him as a buddy or big brother.
Psychotherapy
William was seen at the Combat Stress Control Clinic for psychotherapy, skills training, and medication management 6 days a week for 3 weeks and met with the therapist and often the behavioral health technician on those occasions. Subsequent follow-up was provided once very 2 to 3 weeks for the remainder of his 12-month tour of duty.
The initial objective of William’s psychotherapeutic treatment was to provide him with a containing and validating environment to express cognitions that fostered and maintained his low self-esteem. William would often speak of how he refrained from setting goals in his life because he knew he would not meet them. He thought of himself as a “knucklehead.” He felt that if he stayed in the army, he would not succeed as a leader and that if he became a civilian, he would be homeless once again. He stated that in an infantry unit, he felt as though he was a “pet,” a creature that was cared for but would do things on command. He reported that he refrained from seeking any intimate relationships because it would lead to a marriage that would end in divorce, which was “a Hell I don’t want to be part of.” William was given the opportunity to voice his innermost thoughts with acceptance from the therapist, who took a person-centered approach, rather than challenged William’s distorted cognitions. The therapist positively reinforced statements that were self-affirming, grounded, or optimistic. The therapist’s interest, acceptance, and validation were potent reinforcers for William.
The other primary goal of William’s psychotherapy sessions was reduction of anxiety. As this symptom was most prominent in his interaction with others, a key objective was to increase his comfort and efficacy in interpersonal situations. The methods used to accomplish this were as follows:
Selective reinforcement: While providing an accepting holding environment in which William was able to freely and openly speak about thoughts and feelings he had rarely expressed previously, the therapist responded with increased attentiveness and approbation when he talked about himself in positive or hopeful terms, and demonstrated disinterest or changed the subject when he referred to himself in a disparaging manner.
Social skills training: The therapist and behavioral health technician provided direct instruction in such aspects of interaction as eye contact, conversational pauses, and appropriate questioning.
Anxiety management: The therapist instructed William in using self-talk to decrease anxious responding.
A behavioral therapy technician conducted exercises with William that involved concentration and memory following the sessions with the therapist. Part of the corrective emotional experience came from William’s interactions with the noncommissioned officer escort assigned to accompany him as a safety measure due to his memory lapses. The therapist met with the patient and the buddy several times during the 3-week period, to gain an observer’s perspective on William’s progress in therapy and response to medication. The therapist also provided the buddy with guidance on an interaction style that would foster William’s independence and interpersonal skill.
Medication
Psychopharmacologic therapy with William commenced with risperidone 1 mg b.i.d. and lorazepam 1 mg b.i.d., both ordered for a 3-day period, to defuse his tremendous anxiety. His thinking was clearer and less disorganized in initial follow-up sessions, but he was quite drowsy, so the lorazepam dose was halved. Definitive therapy for anxiety with buspirone, 5 mg t.i.d., was begun several days later and gradually uptitrated to 15 mg t.i.d. For his depressive symptoms, as well as the anxiety, William was treated with citalopram, initially at 10 mg daily to minimize side effects, with an increase to 20 mg daily after 4 days. The buspirone and citalopram were quite well tolerated. William’s self-report reflected attenuation in his anxiety, decreasing from a rating of 7 to an eventual 1 to 2 on a scale of 1 to 10, with 10 being the most severe. William also reported a decrease and eventual cessation of the memory lapses, and remained free of these throughout follow-up. After William’s anxiety and depression were treated, a problem of inattention became more noticeable. Even though he no longer had the memory lapses, William noted that it was very difficult to concentrate now that he was fully aware of his surroundings. Further exploration revealed that William had problems with inattentiveness in school, well before the memory lapses. A trial of extended release dextroamphetamine and amphetamine 20 mg was decided on. When William was first prescribed this medication, he took it later in the morning and noticed its stimulant effects late into the evening. He did note a beneficial effect on his attention span and was able to look things up on the Internet that interested him. His escort noted a much more dramatic change, remarking that William initiated conversations, voiced opinions, and was less forgetful and more attentive. He described the effect of the medication as having “brought him back to Earth.” The stimulant was changed to methylphenidate in hopes of alleviating any nighttime overstimulation, and this was a beneficial switch.
Posttreatment Testing
The MMPI-2 and the RBANS (Figure 4) were readministered to determine whether these measures would also provide indications of improved functioning.
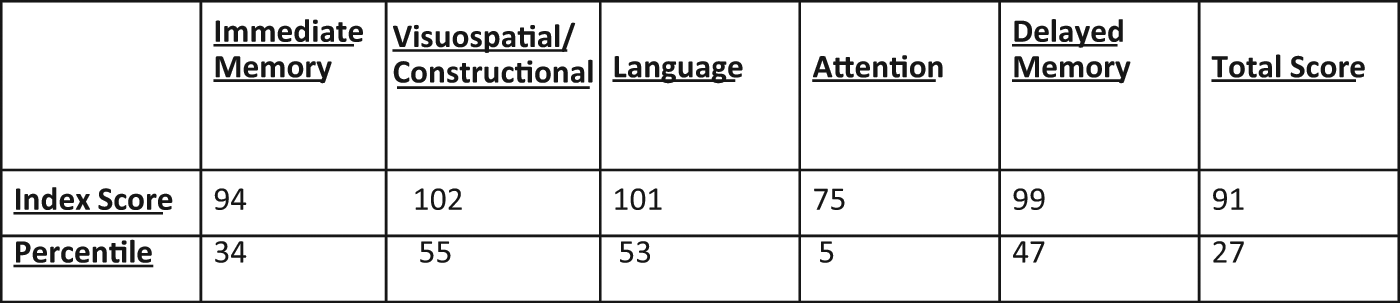
RBANS, posttreatment administration
William’s MMPI-2 profile (Figure 5), although still not within valid limits, reflected substantial changes, most notably in scales most associated with subjective distress. The largest decrease was on Scale F, infrequently endorsed items regarding unusual behaviors and experiences (−21T), which was followed by Scale 7, anxiety/obsessiveness (−18T); Scale 2, depressive symptoms (−17T); Scale 8, dyscontrol, alienation, and bizarre sensory experiences (−16T); and Scale 4, authority/family problems, rebelliousness, and nonconformity (−13T). Although indices reflecting continued oddities of experience, alienation, dyscontrol, and persecutory thoughts remained clinically elevated, all the aforementioned changes are indicative of improved adjustment/functioning. The sole exception was a score increase on Scale 1, concern with somatic functioning (+12T). The reason for this finding is a matter of conjecture, but one possible explanation might be discomfort in response to heightened awareness of bodily sensations when no longer distracted/preoccupied by symptoms of anxiety, depression, or active fantasies. Score increases noted on Scale L, naïve defensiveness (+13T), and, to a lesser degree, on Scale K, more sophisticated defensiveness (+7T), are seen as indications of increased ability and motivation to present in a socially approved manner.
MMPI-2, posttreatment testing
Marked changes were also evident in William’s scores on the RBANS Form B. Most notably, his immediate memory index score increased 30 points, from the 0.5th to the 34th percentile. Although this was still slightly (5 points) lower than his delayed memory score, there was no longer a significant disparity between these measures. The concurrence of improved memory functioning with reduction in psychometric and clinical indications of anxiety is seen as support for the previously posited role of anxiety as a significant factor in memory impairment. Increases were also noted in language (19 points, from the 12th to the 53rd percentile) and attention (15 points, from the 0.4th to the 5th percentile) index scores, though the latter was still an area of significant deficiency relative to his age peers. William performed more poorly when retested in visuospatial/constructional performance (a 10-point index score decrease, from the 79th to the 55th percentile); this appeared to be due to haste and carelessness in his figure copying.
It is noteworthy that William’s posttreatment testing not only indicated improvement in self-reported symptoms and subjective distress but also in performance in such cognitive functions as short-term memory, semantic fluency, and attention.
8 Follow-Up
About a week after William returned to his own base, we received a call from a medic in his unit, reporting some late evening wakefulness and increased energy. It was established that William was having trouble with the self-administration of his medication and was taking the methylphenidate late in the day. We advised the unit medic of the appropriate regimen, and William reported to the aid station 3 times daily to take his medication. This ameliorated the nighttime wakefulness. The goal was a transition to William taking his medications independently.
At his first follow-up appointment, William reported that he was much more attentive at work and concentrating better. He had begun playing an interactive computer game in which several computers from the soldiers in his unit were networked, and the soldiers would have conversations after the games themselves. William remarked that this was a good transition for him to full-fledged social interaction. William missed his second follow-up appointment; however, a phone conversation with his Commander revealed that he was functioning well. He was prompt to pick up his medications. He was noted to have “come out of his shell” and “have more life in his face,” watching movies with his peers, approaching people, and interacting to a degree that was never observed before he came into treatment.
9 Treatment Implications of the Case
Initial evaluation noted that William’s cognitive slippage was consistent with a possible diagnosis of a thought disorder, which could warrant consideration of treatment with antipsychotics. Such a diagnosis would render him ineligible to meet medical standards to remain in the military, as would the use of antipsychotic medication. An alternate approach was to conceptualize the presenting problem of loss of time and situational awareness as due to overwhelming anxiety and depression. William’s characteristic use of internal fantasy was similarly regarded in terms of its functional significance and viewed as an adaptive effort to obtain gratification and reinforcement that he was not otherwise able to see as attainable. The treatment approach was accordingly directed to address his symptoms on a functional level by reducing anxiety and depression, and improving his ability to obtain reinforcement from the environment (externally) rather than via fantasy (internally). Once the anxiety and depression were treated and the memory lapses abated, it was then possible to see a residual disorder of attention and concentration that was not initially apparent.
The effectiveness of the treatment argues for the potential utility of attempting to address symptoms functionally or adaptively, rather than regarding them as manifestations of relatively unmodifiable psychopathology. Alleviating the symptoms of anxiety and depression not only proved beneficial in addressing indications of thought disorder as well but also made possible the recognition of another previously unidentified problem, the attention deficit, which required a separate approach. We were also able to avoid the long-term use of antipsychotic medications that would necessitate discharge from the military.
Recognition and acknowledgment of William’s own traits that increased the likelihood of a positive outcome are also warranted. Qualities that make individuals with schizotypal personality disorder more likely to benefit from analytically oriented psychotherapy have been identified (Stone, 1985a). These qualities, which would seem to predispose one to successful outcomes in more directive therapies as well, are likeableness, high motivation, psychological-mindedness, genuine concern, good moral sense, self-discipline, and low impulsivity. William certainly possessed several of these qualities.
Some individuals with schizotypal personality disorder have social skills deficits similar to individuals with schizophrenia, as reflected in such research findings as poor performance on social role-play tasks and decreased ability to label positive emotions compared with negative ones (Stone, 1985b). Group therapy and behavioral interventions may serve as effective means of modifying socially alienating mannerisms and increasing social skills (Waldeck & Miller, 2000); in addition to the therapy William received in the clinic, his escort was instrumental in modeling socially appropriate behavior. These two soldiers spent all their time together for the nearly 3 weeks that William came for daily intervention at the clinic, and often, William’s escort would provide input about William to the treatment team. In contrast to hospitalization, where nurses and aides administer medications, ensure safety, and conduct psychoeducation, William’s escort was more of a peer. The escort played an integral part in William’s acquiring more normative social skills.
The approach to William’s pharmacotherapy was symptom based and used medications that would allow William’s continued service in the military. Buspirone is an agonist at the 5HT1A serotonin receptor subtype, as are the atypical antipsychotics, where it has an effect on anxiety, mood, and memory. There is not much precedent for the use of buspirone in the treatment of schizotypal personality disorder. A case report of an adolescent with social phobia and mixed personality disorder (Cluster A type) with predominantly schizotypal features describes its successful use (Zwier & Rao, 1994). Pergolide, a dopamine agonist, was shown in a double-blind, placebo-controlled trial to improve visuospatial working memory, executive functioning, and verbal learning and memory in patients with schizotypal personality disorder (McClure et al., 2010). Given that dopamine agonists in this experiment provided benefit for the cognitive abnormalities of schizotypal personality disorders, it seems natural that dextroamphetamine and amphetamine and methylphenidate, dopamine, and norepinephrine reuptake inhibitors would have a positive effect on our schizotypal patient’s deficits.
The similarities between schizotypal personality disorder and schizophrenia-related disorders phenomenologically and biologically provide the rationale for testing the efficacy of neuroleptics in schizotypal personality disorder (Herpertz et al., 2007). A trial of the dopamine (D2) and serotonin (5HT2A) receptor blocker, olanzapine, has shown benefit in the psychosis and depression associated with schizotypal personality disorder (Keshavan, Shad, Soloff, & Schooler, 2004). However, significant weight gain was observed. One trial demonstrated that risperidone reduced positive and negative symptoms of schizotypal personality disorder but did not alleviate depression (Koenigsberg et al., 2003). As previously mentioned, the use of these medications or any of the medications or any other antipsychotic would have meant discharge from military service. Furthermore, by regarding William’s fantasies and ideas of reference as adaptive efforts; alleviating the anxiety and depression and resulting functional impairment with citalopram, buspirone, and psychotherapy; and using the therapeutic relationship and peer modeling to promote development of behaviors that increased the likelihood of reinforcement and social interaction, it was possible to essentially eliminate signs of thought disorder.
This case provides an example of the potential utility of conceptualization of psychiatric symptoms in terms of functional and adaptive considerations in planning and implementing treatment efforts. Regarding the presenting problem of memory lapses as related to pervasive anxiety and frequent immersion in fantasy led to the formulation of a treatment approach focused on reduction of anxiety and development of social skills ultimately resulting in marked reduction in distress, and significantly improved interpersonal and cognitive functioning. In this case, the use of atypical antipsychotics was avoided through the use of medicating the underlying distress with citalopram and buspirone, and an attentional disorder became evident that responded nicely to stimulants.
10 Recommendations to Clinicians and Students
Although diagnostic determination based on observable behavior facilitates categorization, such classification does not provide a basis for understanding the functions behaviors may serve for the individual, which may vary substantially, despite meeting criteria for the same diagnosis. It is therefore advisable to assess the likely reinforcement value of problematic behavior patterns to formulate a treatment strategy where alternate, more adaptive means of attaining comparable objectives may be developed. The role of medication in such an approach is primarily to facilitate such relearning by decreasing the anxiety that would be apt to interfere with change efforts, rather than directly altering oddities in thinking.
The current study also illustrates the importance of considering the ecological context of the individual, particularly with regard to capitalizing on and incorporating opportunities for modeling and peer support in promoting behavioral change.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.