
Abstract
This case study describes an older adult war veteran who served during World War II (WWII) and later developed disruptive behaviors related to psychosomatic symptoms, dementia, and his war-related fear of dying. While in the service, he developed lifelong gastrointestinal problems and was subsequently diagnosed with undifferentiated somatization disorder (USD). USD is a mental illness characterized by medically unexplained physical symptoms originating from psychological or emotional distress. The geropsychology team who worked with the veteran postulated the association of WWII experiences to his somatic symptoms; however, this veteran never received treatment for posttraumatic stress disorder (PTSD), and only a couple of notes in his computerized medical record referenced his wartime experiences. A stepwise approach to care was necessitated to identify a successful, individualized treatment. Phase I of treatment was aimed to reduce attachment anxiety and related behavioral disturbances when the veteran moved into the nursing home. In Phase II, cognitive behavioral therapy and acceptance and commitment therapy were used to help the veteran cope with somatic symptoms. In Phase III, Montessori-based interventions were used to minimize distress associated with dementia-related cognitive impairment and associated war-related somatization and fear of dying. We contemplate the possibility that the veteran’s presentation is a variant of PTSD that has not been described in the literature. We hope that you find this case study to be not the story of someone enduring a life of chronic mental and physical illnesses, but instead our discoveries about the man who persevered with courage and dignity.
1 Theoretical and Research Basis for Treatment
Throughout history, military veterans have presented with unique clusters of physical symptoms with vague psychiatric comorbidity, an earlier example being shell shock that was a disorder characterized by medically unexplained symptoms as well as clusters of trauma-related psychiatric symptoms (Jones & Wessely, 2005; Moore & Reger, 2007). Making a correct diagnosis, although challenging, is key to selecting and implementing effective treatment. Posttraumatic stress disorder (PTSD) seems to be the most obvious disorder to consider after a soldier has served in combat. Yet, only an estimated 31% of war veterans meet diagnostic criteria for full-blown PTSD (http://www.ptsd.va.gov/professional/pages/epidemiological-facts-ptsd.asp). PTSD is diagnosed when an individual experiences intense fear, helplessness, or horror in reaction to a potentially life-threatening traumatic event (American Psychiatric Association, 2000). In addition, the individual must experience intrusive thoughts, avoidance/emotional numbing, and hyperarousal for at least 1 month.
Persons with PTSD may experience difficulties with sleep and concentration, as well as stress related to family relationships such as extreme dependency on loved ones (American Psychiatric Association, 2000; Mikulincer, Shaver, & Horesh, 2006). In their attempt to suppress stressful thoughts and emotions related to the traumatic event, people with PTSD may develop symptoms of depression, anxiety, and somatization (Tull, Gratz, & Roemer, 2004). Research demonstrates that older veterans with PTSD typically experience physical symptoms, such as pain or sleep disruption, rather than the usual psychological symptoms of intrusive recollections, emotional numbing, and hyperarousal that younger veterans report (Owens, Baker, Kasckow, Ciesla, & Mohamed, 2005). Somatic or psychosomatic symptoms are bodily symptoms originating from psychological or emotional distress. These symptoms frequently occur in the cardiovascular, neurological, and gastrointestinal systems, as these systems are highly involved in the bodily stress response (Chrousos, 2009; Jones & Wessely, 2005; Mayer, Craske, & Naliboff, 2001; Ommeren et al., 2002). Chronic, excessive, or unexplained pain is the most commonly reported symptom of the somatic presentations (Jakupcak et al., 2006).
According to the Diagnostic and Statistical Manual of Mental Health Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000), the diagnostic category of somatoform disorders includes clusters of common physical symptoms suggestive of medical conditions; however, the symptom clusters are not fully explained by any known medical or psychiatric conditions. To meet diagnostic criteria for a somatoform disorder, somatic symptoms must cause clinically significant functional impairment or distress (American Psychiatric Association, 2000). Undifferentiated somatization disorder (USD) falls within the somatoform disorders diagnostic category and is characterized by having at least one unexplained physical symptom, such as gastrointestinal or genitourinary problems, loss of appetite, chronic pain, excessive fatigue, impaired coordination, or localized weakness, lasting at least 6 months, and not intentionally produced or feigned (American Psychiatric Association, 2000). A complicating factor in diagnosing and treating USD is that many of the symptoms are the same as those frequently identified as stress-related physical illnesses (e.g., headaches and gastrointestinal disorders; American Psychiatric Association, 2000; Chrousos, 2009). Similarly, the presentation of USD mirrors the presentation of the psychosomatic symptoms of PTSD. In 1989, White and Faustman reported that 42% of male veterans requesting inpatient treatment for PTSD also had several co-occurring medical problems, with 25% of these veterans experiencing musculoskeletal or pain conditions. PTSD symptom severity has been linked to veterans’ endorsements of somatic symptoms (Jakupcak et al., 2006); therefore, the stronger the experience is of PTSD, the more likely the veteran is to voice related somatic issues.
PTSD appears to be underdiagnosed in older adult veterans, including many veterans who participated in World War II (WWII), Korea, and Vietnam. Estimates predict that more than 1 million older adult veterans currently experience chronic PTSD symptoms (Snell & Padin-Rivera, 1997). When older veterans present for treatment of PTSD, their symptoms may be overlooked, as these veterans generally demonstrate somatic symptoms of PTSD rather than emotional symptoms (Owens et al., 2005); therefore, they may receive treatments that are ineffective or invasive. In addition, with older adults, medical conditions, such as diabetes mellitus or renal failure, can mask or complicate the presence of PTSD-related psychosomatic symptoms (Owens et al, 2005).
Research shows that older veterans with PTSD are at an increased risk of developing dementia (Yaffe et al., 2010). Dementia is a generic term for more than 50 specific brain disorders that are characterized by memory impairment and at least one other cognitive disturbance, such as aphasia, apraxia, agnosia, or disruption in executive functioning (American Psychiatric Association, 2000). With dementia, patients can demonstrate a wide range of cognitive and behavioral disturbances, such as sleep problems, aggression, restlessness, repetitive questioning, paranoia, delusions, and fear of abandonment (Desai & Grossberg, 2001; Kitwood, 1997). In addition, patients with dementia may experience sundowning, which is a period of increased agitation, pacing, and disorientation that typically occurs in the afternoon or early evening (Bachman & Rabins, 2006). Depression and anxiety can predate the onset of dementia but they also commonly co-occur with dementia which can exacerbate the cognitive and functional impairments already inherent to the disease (Desai & Grossberg, 2001). Persons who had controlled anxieties in their younger years may show increased anxiety or agitation as their cognitive ability to suppress anxious thoughts and emotions declines (Kitwood, 1997).
Selecting an appropriate therapeutic approach for working with persons with long-standing mental illnesses and cognitive impairment can be quite a challenge, even for seasoned professionals; moreover, navigating this challenge is necessary for producing a successful outcome. Fortunately, several empirically supported psychotherapies are available for treatment of PTSD and USD as individual or unique disorders; however, little to no literature is available to the clinician for treating the disorders in combination. Nevertheless, clinicians are grappling with when to use which treatment for which disorder in which patient. The goal is to match or modify intervention tools with the symptom cluster, values, needs, environment, and capabilities of the patient to offer maximum benefit and wellness.
Therapies focusing on thoughts, feelings, and behaviors, known as cognitive behavioral therapy (CBT), are recommended for psychological treatment of somatoform disorders and PTSD (Kroenke & Swindle, 2000; Lautenbacher & Rollman, 1997; E. Waller & Scheidt, 2006). One specific goal of CBT for persons with a somatoform disorder is to minimize the impact that anxious, psychosomatic thoughts have on their lives by helping them identify emotions and express them in a nonsomatic manner (Kroenke & Swindle, 2000; Lautenbacher & Rollman, 1997). Relaxation training and deep breathing are frequently used in CBT to help patients reduce maladaptive thoughts and become less reactive to physical stimuli (e.g., itching, pain, or numbness). Manualized CBT therapies available for PTSD treatment within the VA include prolonged exposure and cognitive processing therapy. The goals of CBT for treating PTSD are similar to the goals of treating USD, minimize the impact of the dysfunctional thoughts and reduce the physical reactivity to the stimuli by repeated, but safe, exposure to the noxious stimuli. CBT is used effectively in geriatric dementia patients with modifications and adjustments for memory deficiencies.
Acceptance and commitment therapy (ACT) is a type of behavior therapy that became available to psychotherapists in the 1990s and 2000s (Hayes, Strosahl, & Wilson, 2003). It focuses on reducing psychological inflexibility and increasing acceptance of negative affect through the use of metaphor and exploring the individual’s personal sense of values (Luoma, Hayes, & Walser, 2007). One ACT technique that is used to break the cycle of psychological inflexibility is creative hopelessness. Creative hopelessness involves helping the patient to recognize the futility of past attempts to reduce or control negative affect. Through creative hopelessness, the patient begins to develop a willingness to try novel ways of coping. In addition, the person refocuses his or her life to attain meaningful goals consistent with life values. Although several ACT manuals have been written for treatment of anxiety, PTSD, depression, and anger, chronic pain is the only somatoform disorder for which ACT treatment manuals have been developed (Dahl, Wilson, Luciano, & Hayes, 2005). Literature could not be located for using ACT successfully in older adult patients; however, there is no reason to conclude that ACT could not be used effectively once accommodations had been implemented, as other similar techniques have been incorporated into treatment as needed.
Montessori-based intervention is a care approach that has been abstracted from early childhood education and adapted for older adults with dementia who have language impairment. Montessori-based techniques have shown promising effects for improving the overall quality of life for older persons, particularly people with dementia who have receptive and/or expressive aphasia (Camp, Cohen-Mansfield, & Capezuti, 2002; Hopper et al., 2005). These techniques work for this population because they utilize parts of the brain responsible for procedural memory, which generally remains intact until end-stage dementia. Montessori-based methods reduce disruptive behaviors while highlighting the older adult’s retained strengths through engagement in meaningful activities that minimize the use of spoken language during engagement (Camp, 2006). Montessori-based methods include memory bingo, spaced retrieval, and task breakdown. Spaced-retrieval emphasizes deconstructing information into manageable pieces that the person with dementia can process and retrieve (Hopper et al., 2005). The simplified information is then rehearsed with the older adult to assist with the storage of information in the person’s procedural memory. Another method that was designed to improve quality of life in persons with dementia is a memory book (Bourgeois, 1992, 2007). Memory books are external memory aids that were developed to enhance conversations with persons with dementia. They serve as external cues for meaningful information, much like having an external hard drive for a computer. The use of Montessori-based methods and memory books are concordant with the recommendation to provide individualized treatment for persons with Alzheimer’s and other dementias (American Psychiatric Association, 1997) and the VA’s goals of veteran and family centered care.
2 Case Introduction
David Adler, whose name and personal health information have been changed to protect his privacy, was a Caucasian male in his 90s who lived at a VA nursing home. His medical history was significant for multiple physical disorders, and he carried psychiatric diagnoses of USD, anxiety, depression, and dementia. Psychiatric medications included clonazepam, citalopram, mirtazapine, and lorazepam used as needed (i.e., PRN).
The purpose of this case study is to highlight the process of finding empirically based psychological treatment for a patient with complex medical conditions, multiple psychiatric diagnoses, and moderate dementia. This case study emphasizes the creative approach to treatment that was required to develop a successful program for one older patient in a nursing home.
3 Presenting Complaints
Mr. Adler lived in the nursing home for approximately 3 months before he was referred to geropsychology for evaluation and treatment of “feelings of depression and lack of energy.” Typically, geropsychology staff is not consulted until behaviors become unmanageable for nursing staff, and Mr. Adler started demonstrating excessive disruptive behaviors related to anxieties of being separated from his wife. He frequently called his wife and demanded that she take him home. In addition, he became agitated and angry when his wife left the nursing home after her weekly visits. A geropsychological assessment was completed using our standard clinical interview, mental status screening, and depression screening. Initially, interventions were designed to reduce the immediate short-term levels of distress for the veteran, the spouse, and the nursing staff. Next, longer-term therapeutic goals were established.
Over time, as the interventions offered by the geropsychology staff appeared to diminish Mr. Adler’s agitation related to separation from his wife, we began to observe that he increasingly became distressed about his misinterpreted physical symptoms. Mr. Adler’s physical concerns were related to high blood pressure, muscle weakness, malaise, and locking knee joints. Although Mr. Adler was aware that he lived in a nursing home with attending physicians, psychologists, and a large nursing staff, including nurse practitioners, RNs, LPNs, and certified nursing assistants readily available to meet his needs, he regularly demanded to be transported by ambulance to the nearest hospital for medical interventions because he thought he was dying. However, when he presented to the nurses’ station to request emergency medical attention, he did not exhibit any observable or abnormal physical symptoms. For example, on several occasions, he walked approximately 100 feet to the nurses’ station only to tell the nurses that his legs were locked and he could not walk. His agitated behaviors usually started between 3:00 p.m. and 4:00 p.m. as would be expected with dementia-related sundowning, and these symptoms would continue until he fell asleep or a PRN dose of lorazepam was administered. On each occasion Mr. Adler voiced concerns, nursing staff followed several steps: (a) discussing his concerns and examining his symptoms, (b) assessing his vital signs, (c) determining whether acute treatment was needed, (d) providing comfort and emotional support, (e) administering PRN medication, (f) contacting the on-call doctor if needed, and (g) documenting the event and responses in the chart. These examinations, although seemingly brief, took 30 to 60 min of nursing time daily. From a psychological perspective, performing these exams reinforced the veteran’s misperception of his symptoms as being medical and not psychological, making it more likely that the veteran was going to present this way again in the future. However, these examinations could not be avoided because these symptoms must be taken seriously in patients, like Mr. Adler, who are at risk of acute exacerbations of serious medical problems. Managing the delicate balance between performing appropriate examinations without reinforcing disruptive behaviors is not an easy one.
4 History
Mr. Adler was an American soldier during WWII who came from a poor farming community in the South. His only access to higher education was via the G.I. Bill, and he availed himself of this opportunity after WWII. He attended a major university and received a bachelor’s and a master’s degree. After graduation, he started a career as a defense contractor. He retired when he was in his late 50s, likely due to his mental and physical health problems. When Mr. Adler was in his 80s, he had at least one stroke, and, thereafter, his cognitive abilities noticeably declined, which caused him to become increasingly agitated and anxious about his health. Moreover, he became more dependent on his wife to care for him, a characteristic that may have been present years leading up to the stroke due to his lifelong somatic symptoms and continued search for a successful medical treatment. Mr. Adler continued to live with his wife until she was in her 90s and could no longer take care of him on her own. The veteran was placed on a secure dementia unit due to his tendency to become lost when wandering but after several months, he was transferred to an open, skilled care nursing unit because the dementia unit underwent reconstruction. He exhibited few adjustment problems with the transfer to the open unit. He continued to wander some days but could generally be found on the nearby hospice unit seated in a quiet corner chair reading a newspaper.
Mrs. Adler described meeting her husband in the late 1950s and marrying him 2 years later. This marriage was his second and her first. They spoke reverently about their marriage and it was easy to observe the profound love they had for one another. Mrs. Adler noted that she became aware of her husband’s “nervousness” and “minor medical problems” in the early 1960s after they had been married a few years. The Adlers always believed that his symptoms were war related; therefore, they sought treatment for him through the VA. Yet, even after seeking treatment for more than 40 years, Mr. Adler did not have a diagnosis of PTSD or any other stress-related disorder, such as adjustment disorder. By the time he was being treated for dementia in the late 1990s, his diagnosis of USD was 100% service connected, meaning that his psychiatric condition was quite long-standing and likely caused or exacerbated by his service in the military.
VA psychological reports written almost 20 years ago at a distant VA provided strong confirmatory support for our budding case conceptualization of Mr. Adler’s chronic somatic symptoms as stemming from his experiences during WWII. The first psychologist evaluated Mr. Adler as part of the “Fitness and Nutrition Clinic” which likely reinforced Mr. Adler’s misperceptions of his digestive symptoms as being a medical issue and not a psychological one. While there, Mr. Adler described his digestive problems as beginning in 1942, though he did not demonstrate any insight into the connection of his symptoms and war deployment. Psychiatric diagnoses of dysthymia and USD were assigned, but the psychologist did not link Mr. Adler’s symptoms to wartime service. However, 1 year later, a second psychologist was consulted to rule out PTSD in Mr. Adler who was already service connected for “neurotic stomach disorder.” The second psychologist suspected that Mr. Adler’s combat experience was linked to his symptoms, and she noted a moderate elevation of a PTSD scale on Mr. Adler’s Minnesota Multiphasic Personality Inventory–2 (MMPI-2) profile. The second psychological report contains the only available account of Mr. Adler’s combat experiences found within his extensive online VA medical record. These combat experiences included having served under enemy fire for approximately 3 to 6 months and being in imminent danger more than 50 times. In addition, up to 25% of the men in his unit were reported as wounded, killed in action, or missing in action, and Mr. Adler indicated that he saw someone hit by incoming or outgoing fire up to 12 times. He received a diagnosis of “probable” PTSD, chronic. Despite this psychologist’s concern about Mr. Adler’s symptoms stemming from PTSD, the diagnosis was never explored further, perhaps because Mr. Adler held very strong opinions about psychology being a waste of time. His long-held belief about psychology was so powerful that his wife advised us not identify ourselves as psychology staff; however, we were not able to ethically comply with Mrs. Adler’s recommendation. We are required to and did provide Mr. Adler with that information as part of ensuring that informed consent was obtained.
5 Assessment
During the 10 years prior to Mr. Adler’s move into the VA nursing home, he received primary care services at our local VA and completed mood and mental status screening exams almost annually. The available data for these screening exams illustrated Mr. Adler’s slow, gradual decline in cognition and mood. However, even though his depression screenings typically fell in the mild to moderate depressive range, he frequently reported that he was not depressed when directly asked.
Saint Louis University Mental Status Examination (SLUMS)
The SLUMS is a brief mental status screening tool that is used to assess possible cognitive impairment and identify cognitive changes over time. In comparison with the Folstein Mini-Mental State Exam, the SLUMS has better predictive ability of mild cognitive impairment and is similarly capable of detecting dementia (Tariq, Tumosa, Chibnall, Perry, & Morley, 2006). The SLUMS adjusts for level of education unlike other cognitive screening measures. Lower scores indicate more severe cognitive impairment.
Geriatric Depression Scale (GDS)
The GDS is a self-report scale that was specifically developed to measure depression in adults aged 65 and older (Brink et al., 1982). Both GDS forms have been validated and have adequate predictive ability in older adults in the community and in nursing homes (Sheikh & Yesavage, 1986; Yesavage et al., 1982). Concurrent validity was confirmed with comparisons to other well-established depression measures (Yesavage et al., 1982). Higher scores on the GDS indicate greater severity of depression.
Geropsychology began working with Mr. Adler several months after he moved into the nursing home. He was administered the SLUMS and obtained a score of 14 out of 30, which fell in the dementia range for his level of education. Related to orientation, he was unable to identify the day of the week. He missed several of the numeric items requiring intact attention which was particularly problematic given his background, educational attainment, and career in business. He remembered four out of five items on a delayed recall task. He performed poorly on the contextual learning task, indicating that he would have difficulty recalling material read in the newspaper or comprehending more than one or two bits of information shared at a time. He demonstrated mild fluency problems on the timed word-generating task. His visuospatial abilities were mildly impaired as evidenced by his difficulties with the clock-drawing task on the SLUMS. In addition, the clock-drawing task revealed mild impairment in executive functioning suggesting that judgment and decision making would be compromised. Based on our clinical interview, Mr. Adler was a very bright man before developing vascular dementia, and this intellect was evident in his retention of a very large vocabulary. His vocabulary, however, was misleading to staff, who believed that he did not have substantial cognitive impairment because he was able to have extensive conversations when initiated by others.
On the GDS long form, Mr. Adler obtained a score of 8 out of 30, which placed him in the “normal 0 to 9” range of scores. He endorsed the following: preferring to stay home at night, feeling as if he has more problems with memory than most, having trouble concentrating, avoiding social gatherings, not finding life very exciting, not feeling full of energy, having problems with decision making, and his mind not being as clear as it used to be. These symptoms are characteristic of people with depression. Although Mr. Adler’s results did not meet the cutoff score for the “mild depressive” range, it is likely that he experienced depression that was not captured by the GDS due to his cognitive impairment as well as his restricted psychological mindedness.
Interestingly, many of the symptoms that he endorsed could also represent symptoms of PTSD. For example, not finding life to be very exciting and avoiding social gatherings could be seen as the PTSD symptoms of avoidance and emotional numbing. Similarly, Mr. Adler’s endorsement of having trouble with concentration could be interpreted as PTSD hyperarousal symptoms.
6 Case Conceptualization
Mr. Adler’s primary symptoms targeted for treatment by geropsychology were anxieties related to separation from his wife, USD-related health issues, and dementia. During our therapy sessions, Mr. Adler never gave details about his war experience, even when questioned directly, making it difficult to confirm whether his anxieties were connected to his combat experiences. Although he did not have a formal diagnosis of PTSD, we postulated the association of his WWII experiences to his somatic symptoms. Research indicates that troops who served in the danger zone are at very high risk of developing stress reactions, including excessive health care worries as well as physical illnesses, such as gastrointestinal disorders, back pain, poor stamina, and headaches (Hobfoll et al., 1991; Shnurr, Spiro, & Paris, 2000). In addition, research demonstrates that PTSD and war-related stress can result in extreme dependency and attachment to family members (e.g., attachment anxiety; Mikulincer et al., 2006). The stress reactions and attachment anxiety were prominent features of Mr. Adler’s presentation, and we carried an understanding of the theoretical ties between war-related stress and lifelong anxieties (i.e., attachment and health) in our case conceptualization throughout treatment. We became aware of the previously described documentation in Mr. Adler’s electronic medical records from 20 years ago which revealed that another VA psychologist suspected that Mr. Adler’s somatic symptoms, including the gastrointestinal disorders for which he persistently sought medical rather than psychological treatment, were a direct result of combat exposure. Yet, because Mr. Adler did not receive effective treatment for his somatic war-related symptoms, his symptoms never dissipated, he became increasingly aware of his own internal sensations and symptoms, and he likely experienced much unnecessary suffering during the course of his lifetime.
Mr. Adler’s clinical presentation changed as he grew older. His initial concerns appeared to relate to his gastrointestinal symptoms; however, when he was in his 70s, he was treated for several episodes of transient ischemic attacks and a stroke that required rehabilitation to regain the ability to read and ambulate. Afterwards, Mr. Adler began to focus excessively on his blood pressure, and he frequently feared that he was having another stroke. Eventually, he became obsessed with these fears and developed a fear of dying, which only became apparent in the middle stages of therapy. This fear of dying is often seen in veterans with unresolved issues surrounding their combat experiences or other actions that were taken during military duty.
To summarize, we believed that many of Mr. Adler’s physical symptoms were best conceptualized as psychological, and, as such, could not be effectively treated medically. He likely had a genetic predisposition for manifestation of somatic symptoms that combined with the prevailing soldier mentality to reject any symptoms characteristic of mental illnesses; after all, WWII soldiers were heroes, and mental illness signified vulnerability, a point of weakness. Indeed, many military careers have been abruptly terminated by the stigma of having mental illness, rightly or wrongly (Dingfelder, 2009; Hoge et al., 2002). Even if a member of the military had been able to avoid the stigma of mental illness or psychiatric treatment, war-related psychological brain changes may be permanent to some extent, as many members of the military and their families can affirm.
Mr. Adler’s war-related stress followed a trajectory that began with the start of gastrointestinal symptoms during the war in 1942. His wife took notice of his chronic physical symptoms early in the course of their marriage, and she became skilled at managing his environment to minimize the impact that stress would have on him (e.g., asking psychology staff not to identify themselves as psychologists). During the Vietnam War era, although Mr. Adler was not in the Army, listening to news about Vietnam likely triggered intrusive memories of his own combat experiences, heightened his somatic symptoms, and resulted in an exacerbation of his gastrointestinal disturbances. Then, after his stroke in the late 1990s, he became increasingly anxious in general, and, more specifically, became obsessed with his vital signs with the unspoken goal of ameliorating his renewed fear of death. He also endorsed several symptoms of depression that were likely connected to his war-related stress, persistent somatic symptoms, and health-related anxieties. As a result of the ischemic events and stroke, Mr. Adler developed vascular dementia that further damaged his brain that was already overtaxed by trauma and mental illness, limiting his ability to process his deepest fears. His anxiety developed into agitation, and his USD-related somatic fears resulted in his daily demands to be treated in an acute care facility. Due to his cognitive impairment, Mr. Adler did not recall making the same demands the previous day with the same results. In addition, the aphasia stemming from his moderate dementia made it difficult for him to express his concerns to nursing staff.
7 Course of Treatment and Assessment of Progress
The treatment focus throughout the therapy was to decrease Mr. Alder’s symptoms of anxiety. Therapy occurred in three phases, and each phase was based on a different approach to treatment for anxiety. In the first phase of the therapy, the aim was to decrease the observed anxiety and depressed mood Mr. Adler experienced from living apart from his wife. The aim of the second phase of the therapy was to decrease his USD-related anxieties concerning his health. The focus of the last phase of the therapy was to decrease his anxiety and agitation related to his dementia and memory loss.
Therapy Phase I
The initial geropsychological evaluation, which included behavioral analysis of antecedents and consequences, revealed that Mr. Adler experienced symptoms of depressed mood and anxiety. His anxiety symptoms were multifaceted and difficult to isolate; however, we were able to determine that he faced specific fears about death and dying as well as attachment anxiety, a stress symptom that is common in persons with war-related stress and dementia (Kitwood, 1997; Mikulincer et al., 2006). In addition, his wife experienced considerable distress about placing her husband in the nursing home, perhaps related to Mr. Adler’s attachment anxiety. Therefore, many sessions during the first phase of therapy addressed Mr. Adler’s complex presentation of anxiety and depression as well as his wife’s concerns. Specific issues addressed in therapy included the following: (a) Mr. Adler’s repeated telephone calls aimed at persuading his wife to pick him up, (b) his fear that his wife would leave him permanently, (c) education for the spouse about the natural course of dementia, (d) assistance with creating a pleasant visiting experience for the couple by planning birthday and anniversary parties, and (e) collaboration with nursing staff to coordinate the timing of visits so that Mr. Adler would be engaged in an activity or mealtime when it was time for his wife to leave after her visits.
Approximately 6 months into working with Mr. Adler and his wife, Mrs. Adler voiced her appreciation for the improvements in her husband’s mood, agitation, and anxiety. As indicated by the geropsychology and nursing chart notes, the specific behaviors that were targeted in psychotherapy, such as not calling his wife and demanding to go home, had improved significantly. Mr. Adler was observed to have more pleasant visits with his wife in the nursing home, and he displayed less agitation when his wife left after their weekly visits.
Therapy Phase II
After improving Mr. Adler’s disruptive behaviors related to attachment anxiety, we began to notice increased distress related to somatic symptoms. Thus, the second phase of therapy was designed to address Mr. Adler’s agitated, fearful USD-related behaviors that became problematic for his personal health as well as the provision of health care. Individual psychotherapy was used to address Mr. Adler’s fearfulness and his anxious responses to his symptoms. One major challenge of treating people with USD is the entrenched belief that all symptoms have medical explanations that require medical rather than psychological treatments. Due to the nature of Mr. Adler’s concerns and the possibility for grave consequences if his symptoms were incorrectly overlooked, complete sets of “distressed” vital signs were obtained each time that Mr. Adler reported he was dying or whenever he requested emergency medical attention. His vital signs never appeared to be unstable or out of a normal range. A random sample of 20 “routine” vital signs were collected from his electronic medical records and summarized for comparison with his “distressed” vital signs; however, no differences were found. A comparison of scores is shown in Figure 1.
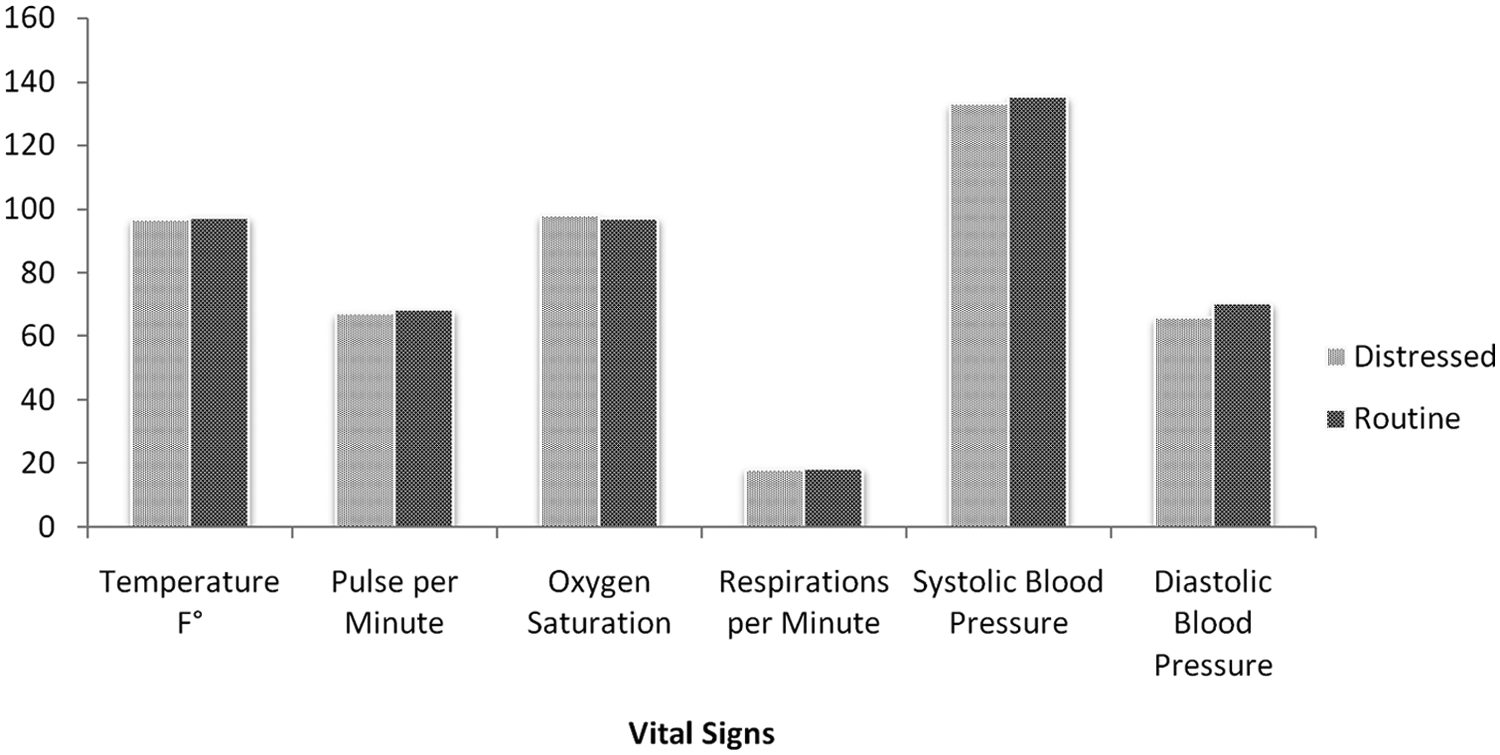
Comparison of routine and distressed vitals
During this phase of treatment, we used CBT to address Mr. Adler’s somatic symptoms. To accommodate his cognitive impairments, we provided therapy at a slower than usual pace, repeated information, provided written materials with large font as well as other visual cues. We provided psycho-education about the role that psychological factors play in bodily functioning by highlighting the associations between thoughts, emotions, behaviors, and physiologic responses. Still, Mr. Adler did not find psychology to be relevant to his stomach problems, blood pressure, malaise, or weakness. His vital signs, “distressed” and “routine,” were presented to him to provide well-established medical data to illustrate the stability of his bodily functions. He responded positively to this information when it was presented, and, at times, his agitation would decrease to the point of not needing a PRN medication for his anxiety. Yet, the nursing staff indicated that Mr. Adler never benefitted from having this information shared with him when they provided him with the information. On the occasions that he was calmed during the CBT, we would engage him in a relaxation training exercise. We offered this exercise as treatment for his medical symptoms (e.g., blood pressure) rather than his anxiety because of his past rejections of psychological treatment. During each relaxation session, Mr. Adler participated fully and appeared very relaxed. However, he did not report any improvements in mood or muscle tension on the 0 to 10 subjective units of distress scale. In addition, he would immediately return to his baseline cognitions about needing to be hospitalized.
After several weeks of psychotherapy using CBT, Mr. Adler continued to demonstrate significant levels of distress as evidenced by almost daily reports that he was dying. We realized that, not only was Mr. Adler not psychologically minded as we had been told by him and his wife, he was also not in a place of readiness to accept that any psychological factors played a role in his symptoms. In addition, with his cognitive impairments, it was unlikely that he was going to master the skills to independently challenge his own cognitions in a way that was going to cause the necessary change needed to significantly reduce his distress. Because of his severe distress, the geropsychology team did not want to postpone trying another treatment option. Thus, after several weeks of trials and partial failures with CBT, we transitioned to using ACT.
We began ACT interventions by talking with Mr. Adler about his life values, which was initiated by using a modified ACT Valued Living Questionnaire (Wilson & Murrell, 2004). Mr. Adler rated the importance of 10 life domains on a 10-point Likert-type scale. He rated family, marriage, and work as 9 out of 10, and he rated parenting, friends, recreation/fun, and spirituality as 8 out of 10. Mr. Adler rated health-related domains of physical self-care, diet, and exercise and sleep as 7 out of 10. Even though his ratings on the health-related domains were relatively high, they were discordant with his daily distress regarding his health as it was expected that these life domains would be rated much higher than they were.
A turning point in treatment occurred during a therapy session in which Mr. Adler was able to experience creative hopelessness, a central concept in ACT. He approached the geropsychologist (B.D.) one day stating, “This isn’t the right place for me,” and expressed his desire to go home. The geropsychologist used this as an opportunity to foster creative hopelessness, and she administered the SLUMS to Mr. Adler, providing immediate feedback. The assessment and feedback session allowed him to recognize his own cognitive deficits, something he did not have insight into moments before. Without prompting, he stated that, despite his wish to go home, he realized he needed to stay in the nursing home because the staff could provide the care that he needed. He showed compassion and concern for his wife as he stated that he knew she could no longer provide for his physical care. Emotional support was provided as he grieved and finally allowed himself to experience sadness related to his dementia. At the end of the session, he appeared calm and made no other requests to be discharged from the nursing home. Unfortunately, this insight did not diminish his demands to be treated acutely in the intensive care unit at the local hospital or his perception that he was dying.
We found that exploring values with Mr. Adler was beneficial to building rapport; however, due to his cognitive impairment, he was not able to benefit fully from the independent growth process inherent to values-based approaches. Therefore, no homework could be assigned and he could not reflect on our conversations outside of the therapy sessions. The geropsychology staff began to reinterpret Mr. Adler’s disruptive behaviors as an expression of distress related to his dementia as it was becoming clear to us that his cognitive impairment was complicating all of our approaches to treat the psychosomatic symptoms.
Therapy Phase III
The third phase of therapy was designed to treat the agitation and behavior disruption that was caused by Mr. Adler’s dementia and memory loss. He appeared distressed by his general confusion, and he expressed fears about having another stroke. We conceptualized his agitation as sundowning. During one episode of agitation, we talked to him for a couple of hours about his diagnosis of dementia. Education was provided about the symptoms of dementia, memory loss, and sundowning. This confirmation of a medical cause for his confusion and agitation symptoms appeared to be the validation that he needed to calm his anxieties. Mr. Adler was welcoming of a medical explanation as would be expected given his lifelong somatic focus from USD. In addition, he seemed to benefit from understanding that his symptoms were dementia specific rather than heart disease or stroke. He appeared less threatened by the knowledge that he was not actively dying, and with this, we surmised that possible PTSD-related sensations were ameliorated. Direct care staff received brief training on how to remind Mr. Adler that his symptoms were dementia related rather than heart attack or stroke related, and several of them became skilled at using this intervention to prevent emotional distress and behavioral disruption.
As the focus of therapy shifted from treating Mr. Adler’s USD to treating his dementia, we initially engaged in peer consultation with another geropsychologist (M.H.) to discuss other possible treatment options. She suggested that we consider implementing a memory book. This book would serve as an external memory source for providing comfort to Mr. Adler when geropsychology staff could not be present. We knew his reading skills were sufficiently preserved and that reading was enjoyable for him. Therefore, we concluded that a memory book would be a feasible intervention. During the next few therapy sessions, we helped Mr. Adler personalize a binder (i.e., Montessori-type memory book) bearing his name and a meaningful picture. When educational material about dementia was shared with Mr. Adler, we placed the information in his memory book for him to review. Interestingly, when he was not distressed, he spoke very highly of the care he was receiving in the VA, and he had very kind words to say about the way the nursing staff cared for him. We wanted him to have access to this information when he became distressed; therefore, during therapy sessions in which Mr. Adler was not agitated, we asked him to describe his thoughts about his health and the care he received at the facility. As expected, Mr. Adler talked about the excellent care provided at this facility and stated that he had absolutely no fears or concerns about his health. We typed his comments and placed them in his memory book so he could read it on his own to find comfort.
Nursing notes revealed that some direct care staff were implementing the psycho-education techniques they were trained to use for this phase of treatment. During documented periods of agitation, the direct care staff would talk with Mr. Adler about his dementia-related symptoms rather than automatically administering a PRN medication. As shown in Figure 2, Mr. Adler’s use of lorazepam PRN dropped from an average of 1.18 mg daily to 0.37 mg daily as a result of this intervention. The dementia unit Mr. Adler lived on when he first moved to the nursing home was complete from reconstruction, and he was transferred back to that unit a few weeks after the third phase of therapy was initiated. He took his memory book with him when he transferred, and the direct care staff on his new unit adopted the intervention strategies with success.
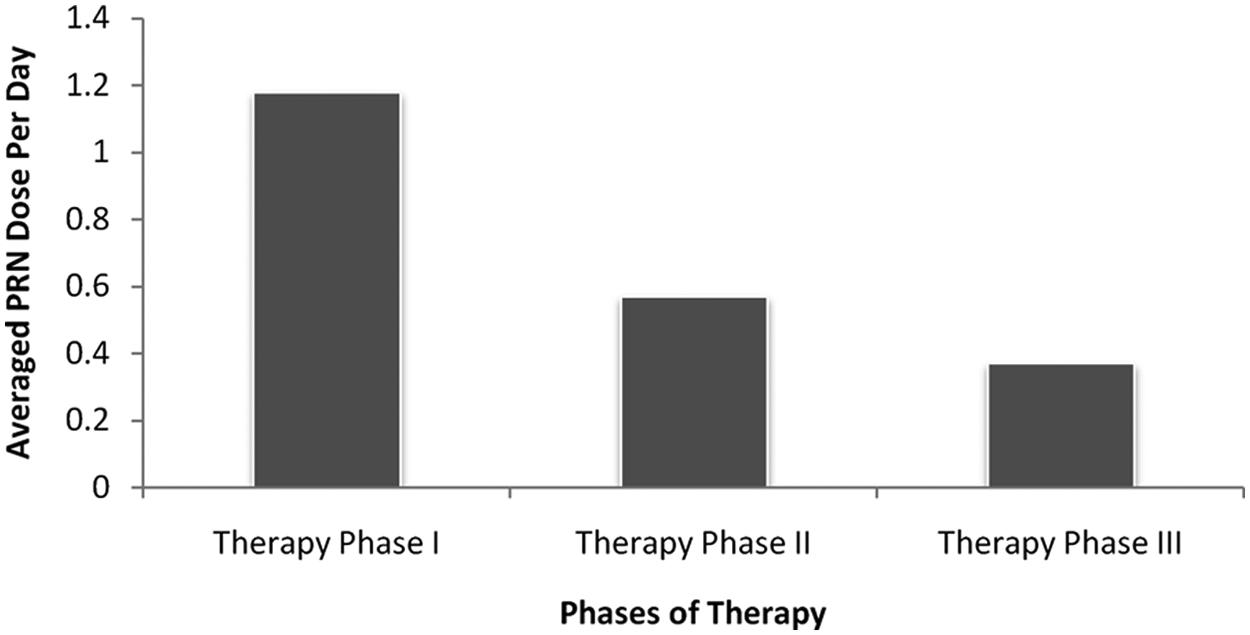
Averaged PRN administration during treatment
8 Complicating Factors
Providing care to nursing home residents almost always entails some complicating factors. Nursing home residents are by definition significantly impaired given that residents are required to have two skilled care needs, such as toileting, feeding, bathing, dressing, and ambulation. Having any type of mental illness further complicates treatment. Furthermore, it seems that military service in and of itself causes health complications that can last a lifetime. Bedard and Deschênes (2006) studied the long-term impact of military duty on the health of WWII veterans and found that veterans are 5% more likely to be disabled than are nonveterans by their mid 50s. They also document that mortality is higher in age groups with higher WWII participation due to vascular disease and lung cancer.
Mr. Adler had a long list of health problems in addition to his mental health diagnoses. Because he frequently endorsed somatic symptoms, it was necessary to assess observable symptoms of stroke or transient ischemic attack (e.g., expressive aphasia, coordination problems, and weakness in extremities) before starting each therapy session. The informal physical evaluations took approximately 10 minutes each, and medical emergencies were ruled out at every session. These assessments took a significant amount of time and not infrequently precluded the geropsychology team from actually working with the patient on some days.
Another challenge throughout working with Mr. Adler was the role of the psychology staff in treating patients on the unit. When geropsychology started working on the units approximately 4 years ago, many staff members had never worked with a psychologist before, nor were the direct care staff trained in providing mental health interventions. Through staff training at shift report and hallway consultations, geropsychology has been gradually integrating psychological treatment into the care of nursing home residents. Regarding this case, we observed discrepancies within observational symptom measures that were completed by direct care staff in spite of the training they had been provided for completing them. For example, the direct care staff member described Mr. Adler as having severe worry about physical health on one measure, but she did not endorse signs of anxiety or physical complaints on another measure. Due to these types of inconsistencies, we elected to omit observational measures from this report.
Mrs. Adler remained actively involved in her husband’s care in the nursing home. Her priority was ensuring that his needs were met. She noted that Mr. Adler needed treatment relative to his anxiety about physical symptoms, but she did not think he would not respond favorably to psychological treatment. Indeed, it was evident that he preferred to talk about medical rather than psychological treatment. Therefore, even though we were met with initial resistance from Mr. and Mrs. Adler, geropsychology services proved to be of benefit for both over the course of treatment.
9 Access and Barriers to Care
Veterans’ hospitals have been referenced as providing the best health care in the United States (D. Waller, 2006). The first component of stellar care is the access providers have to veterans’ computerized medical records, which includes physical exams, lab tests, and all chart notes (e.g., psychological reports). This information is available to VA staff regardless of which VA hospital provided the services. Despite the accessibility of patient information via the computerized medical record, health care providers who treated Mr. Adler prior to his nursing home admission did not incorporate findings from previous psychological assessments into their case conceptualization or approach to care, nor were the findings transferred from one VA to another. The lack of awareness of the original psychologists’ reports and subsequent non-utilization data may have led to years without treatment for USD and without regard for the influence of combat and military experiences on Mr. Adler’s quality of life.
The unfortunate event regarding documentation that happened with this case is much less likely to occur in the current climate of VA health care. First, the VA now provides a seamless transition of care from one venue to another. Outside medical records are quickly scanned into the computerized record so that information is available in a timely manner. Second, the VA is committed to providing veteran-centric, interdisciplinary care to every veteran, which will make it more difficult to overlook details related to care. Each veteran now has a team of dedicated providers rather than being seen by whichever provider is available at that date and time. When therapeutic bonds and trust are established between patient and provider, better care becomes a reality. Third, for decades, the stigma associated with mental illness has been a barrier to care for people with mental illness. Fortunately, this problem seems to have diminished in recent years due to the Department of Defense and the VA working together as leaders in the field with the goal of reducing this stigma. Veterans now have greater access to empirically based interventions.
10 Follow-up
Mr. Adler was administered a SLUMS and GDS at 1 month post-treatment. He obtained a score of 15 out of 30 on the SLUMS, which is 1 point above his baseline assessment and 5 points above a mid-treatment assessment. Furthermore, his score on the GDS long form was 5 out of 30, which is a 3-point reduction in depressive symptoms compared with his baseline measure. The improvements observed in Mr. Adler’s cognitive and mood screenings are thought to be a direct result of the dementia-specific interventions used to improve orientation to symptoms, diagnoses, and other meaningful information. In addition, the reduction in PRN lorazepam administrations likely decreased loss of orientation, a side effect that can occur with the use of lorazepam. Several direct care staff provided informal, verbal reports about Mr. Adler’s behaviors, and they noted that he infrequently expressed worry about his health and rarely asked to be transferred to the hospital. We completed behavioral observations on several occasions at follow-up, and Mr. Adler always appeared calm and free from distress as evidenced by his affect and speech content. Overall, his anxiousness and somatic symptoms decreased significantly and his quality of life improved. Mrs. Adler reported the same observations during her visits.
11 Treatment Implications of the Case
This case introduces the complexities of working with an older adult with multiple medical and psychiatric diagnoses. At the start of the treatment, geropsychology took a traditional psychological approach to reduce Mr. Adler’s anxieties and fears about his physical issues. However, Mr. Adler had an inherent medical bias toward his care because of mental illness causing him to overfocus on somatic problems, and he remained disinterested or unmotivated to talk about the psychological component of his physical symptoms. For him, a medical explanation for his symptoms proved to be the best treatment approach. His agitation dissipated when he received news that he had dementia and that sundowning was the cause of his discomfort. Because Mr. Adler had dementia, a memory book was used to provide an external memory source for important information so that he could seek reassurance and comfort independently.
Mr. Adler’s symptom cluster and medical history was complex, but we were fortunate to have access to his computerized medical record, his spouse, and nursing staff to develop a timeline of symptom occurrence. We believe his war experiences contributed to the start of his somatic symptoms. Furthermore, we have wondered whether he had a variant of PTSD that has not been fully described in the research and clinical literature. Still, we have not fully resolved this question to our satisfaction, and we continue to explore the idea of a somatic variant of PTSD. We hope that future research in war veterans will investigate the somatic presentations so that a clear differentiation exists between somatic-based PTSD and USD.
12 Recommendations to Clinicians and Students
Reviewing the literature in search of successful therapies for specific mental illnesses is pertinent in establishing an empirically based treatment plan. The American Psychological Association (2004) and American Psychiatric Association (1997) developed guidelines specific to working with older adults, and they provide an overview of empirically supported treatments. In general, most validated therapies are efficacious for older adults, but adjustments for treatment delivery may need to be made based on the older adult’s physical, cognitive, and sensory abilities. In addition, due to the complexities of comorbidities and treatment, psychologists should should collaborate with interdisciplinary treatment teams and consult with colleagues as needed to develop a comprehensive, successful treatment plan.
Footnotes
Acknowledgements
We would like to thank Michelle M. Hilgeman for her peer consultation regarding the use of Montessori-based techniques. We would also like to acknowledge Yuriy Ustinov for his assistance with minor statistical procedures and sharing his knowledge of computers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is the result of work supported in part with resources from and the use of facilities at the Tuscaloosa VA Medical Center.