
Abstract
Medication adherence and regimen responsibility (RR) have important implications for adolescents with hemodialysis-dependent end-stage renal disease (ESRD). This case study assesses the preliminary efficacy of a cognitive-behavioral intervention to promote medication adherence and RR in two African American adolescents. Two patients and their mothers participated. Intervention modules addressed adherence barriers. Using a case-series design, weekly parent–adolescent reports of medication adherence and RR were collected. The female participant’s selective nonadherence improved during treatment. Mother and daughter were high in RR throughout the study. The male participant’s adherence initially decreased following his mother’s reduced involvement in treatment. His adherence improved by the end of treatment, and coincided with his mother’s reassumption of RR. Improvements were maintained through follow-up for both patients. This case study provides preliminary support for using a cognitive-behavioral protocol to improve medication adherence in adolescents with hemodialysis-dependent ESRD.
1 Theoretical and Research Basis for Treatment
End-stage renal disease (ESRD), the final stage of chronic kidney disease, is an incurable condition in which both kidneys function at <15%. Approximately 7,330 pediatric patients, ages 0 to 19 years, are affected (U.S. Renal Data System, 2011). Primary treatments include dialysis and kidney transplantation. Clinic-based hemodialysis (HD), the focus of this case study, requires patients to attend multi-hour sessions three times a week. In addition, patients follow dietary and fluid intake restrictions and take multiple prescribed medications (Denhaerynck et al., 2007). This case study addresses medication adherence, the degree to which patients’ medication taking coincides with health care providers’ recommendations (World Health Organization, 2003).
As disease severity increases, patients with ESRD will likely be considered for kidney transplantation, the optimal treatment for ESRD. Medication adherence is particularly important at this treatment stage: Transplantation is associated with better survival rates and quality of life, yet about 12% of adolescent kidney transplant failures are due to medication nonadherence, four times the rate for adults (Rianthavorn & Ettenger, 2005). Adherence history may be considered in determining transplant eligibility (Fung & Shaw, 2008). Patients on clinic-based HD also may have more adherence difficulties. Alternatives to clinic-based HD, home-based HD and peritoneal dialysis, require responsibility to independently manage treatment and are less suitable for nonadherent patients (Heaf, 2004). Adolescents on clinic-based HD with histories of nonadherence may be at risk of posttransplant nonadherence and subsequent health problems. Intervention to improve medication adherence before transplantation is required may reduce obstacles to receiving a transplant and enhance long-term health outcomes (Zelikovsky, Schast, Palmer, & Meyers, 2008).
Adolescence is a problematic period for adherence due in part to transitioning regimen responsibility (RR) from parents to adolescents (Pai & Ostendorf, 2011). RR refers to the degree to which family members and the patient are involved in condition management (Greenley, Doughty, Stephens, & Kugathasan, 2010), and, for this case study, specifically refers to medication management. Older adolescence is associated with less parent monitoring (Gilleland, Amaral, Mee, & Blount, 2012), even though adolescents are less adherent than younger children (Fredericks et al., 2010). In adolescent transplant recipients, adolescents whose parents were mostly in charge of monitoring medication taking had better adherence than adolescents who independently managed medication taking (Zelikovsky et al., 2008). In pediatric patients with diabetes, parent–adolescent perception of shared RR was associated with following doctor’s recommendations (Helgeson, Reynolds, Siminerio, Escobar, & Becker, 2008). Because sustained parental RR and shared parent–adolescent RR seem to be associated with better medical adherence, intervention to support appropriately allocated parent–adolescent RR is warranted.
Only one study promoting adherence in adolescent patients on HD was found: a token reinforcement system, which effectively improved dietary restriction adherence (Magrab & Papadopoulou, 1977). However, there is a rich history of adherence-promoting interventions for pediatric patients with diabetes, asthma, and other commonly occurring illnesses. Behavioral, educational, and multicomponent interventions are most effective for improving pediatric adherence (Graves, Roberts, Rapoff, & Boyer, 2010; Kahana, Drotar, & Frazier, 2008). For adults on HD, a systematic review (Sharp, Wild, & Gumley, 2005) reported that most adherence interventions used behavioral methods with education, cognitive therapy, and social support, and recommended multicomponent cognitive-behavioral interventions for renal populations.
The Health Belief Model (HBM; Janz & Becker, 1984) provides a framework to understand patients’ nonadherence. The HBM posits that adherence is a function of patients’ perceived susceptibility and severity of illness, as well as perceived benefits, barriers, and cues to adhere. “Perceived barriers” are considered the most powerful predictor of patients’ engagement in various health practices (Janz & Becker, 1984). In pediatric renal transplant recipients, barriers are associated with lower adherence (Zelikovsky et al., 2008). Barrier identification can contribute to intervention development, enabling clinicians to tailor interventions by problem solving to overcome patients’ obstacles to adherence (Rapoff, 2010). This case study used the HBM’s perceived barriers component to conceptualize adherence and guide treatment development.
This case study documents an intervention developed to improve medication adherence and support RR in adolescents with HD-dependent ESRD. The case-series design facilitated description of the feasibility, preliminary efficacy, and outcomes of this innovative intervention for a rare condition (Drotar, 2011). The design allowed consideration of practical issues and idiosyncratic patient factors to refine the protocol. This manualized, multicomponent, family-based intervention conceptualized adherence through the HBM’s “perceived barriers” component and incorporated cognitive-behavioral principles and recommended practices for promoting adherence in pediatric and renal populations. The intervention was implemented during clinic-based HD sessions with two African American adolescents and their parents. The parent component was included to enhance parental support and monitoring of medication taking. It was hypothesized that the intervention would (a) increase adolescent medication adherence, (b) increase adolescent RR, and (c) support shared RR between parents and adolescents.
2 Case Introduction
Adolescent patients and their parents were recruited from the dialysis unit of a children’s hospital. Any adolescent receiving clinic-based HD at the unit was eligible to participate. Exclusion criteria included low parent-reported child cognitive ability, non-English primary language, and parent unavailability to be involved with the intervention. Two patients enrolled and completed the intervention. Prior to participation, adolescent assent, parent informed consent, and a waiver of authorization for protected health information were obtained from participants. The participating university’s Institutional Review Board approved the study.
Jane was a 16-year, 6-month-old African American female receiving clinic-based HD for systemic lupus erythematosus, which led to lupus nephritis. She was homeschooled and completing ninth-grade level work. Jane’s 36-year-old mother was separated, had some college education, and was unable to work due to Jane’s health. Jane had two siblings, an aunt, and an uncle living at home. Her health insurance required a small (<25%) prescription drug co-pay.
Jack was a 14-year, 11-month-old African American male receiving clinic-based HD for focal segmental glomerulosclerosis (FSGS). His 35-year-old single mother worked part-time and had a professional degree. Jack was an only child, but had a grandparent living at home. He was in ninth grade at a public school, attended twice a week due to his HD schedule, and was reportedly failing his classes. A year earlier, Jack was in an automobile accident in which a friend died. He was in counseling at the time of enrollment but reportedly did not talk during his sessions. Jack’s insurance provided full prescription drug coverage.
3 Presenting Complaints
Jane and her mother reported Jane’s inconsistent medication taking as their main concern at recruitment. Jane and her mother demonstrated a good understanding of the medication regimen and its purpose. Because Jane still struggled to achieve total adherence, she and her mother were interested in learning skills and strategies to support complete medication taking.
Jack and his mother reported near-perfect adherence at recruitment. However, both agreed that his high adherence was due to his mother’s assumption of almost total RR and Jack’s assumption of little to no RR. Jack’s mother wanted him to assume more responsibility for taking his medications. Considering the relationship between greater adolescent RR and lower medication adherence (Pai & Ostendorf, 2011), it was important to support a transition of RR that would not compromise Jack’s adherence. Jack’s mother also reported difficulty managing Jack’s negativistic and oppositional behavior, which was a source of family conflict and appeared to be partly linked to Jack’s need to take medications.
4 History
Jane was diagnosed with systemic lupus erythematosus leading to lupus nephritis 8 years prior to enrollment. Complications from lupus led to both kidneys being removed. She was also diagnosed with a seizure disorder and high blood pressure. Jane was prescribed medications for lupus, ESRD, seizures, and high blood pressure (Table 1). She began her current clinic-based HD regimen 3 months prior to enrollment. Previously, at a different hospital, Jane was on peritoneal dialysis for 3.5 years, followed by 1 year of clinic-based HD.
Jane’s Medication Regimen
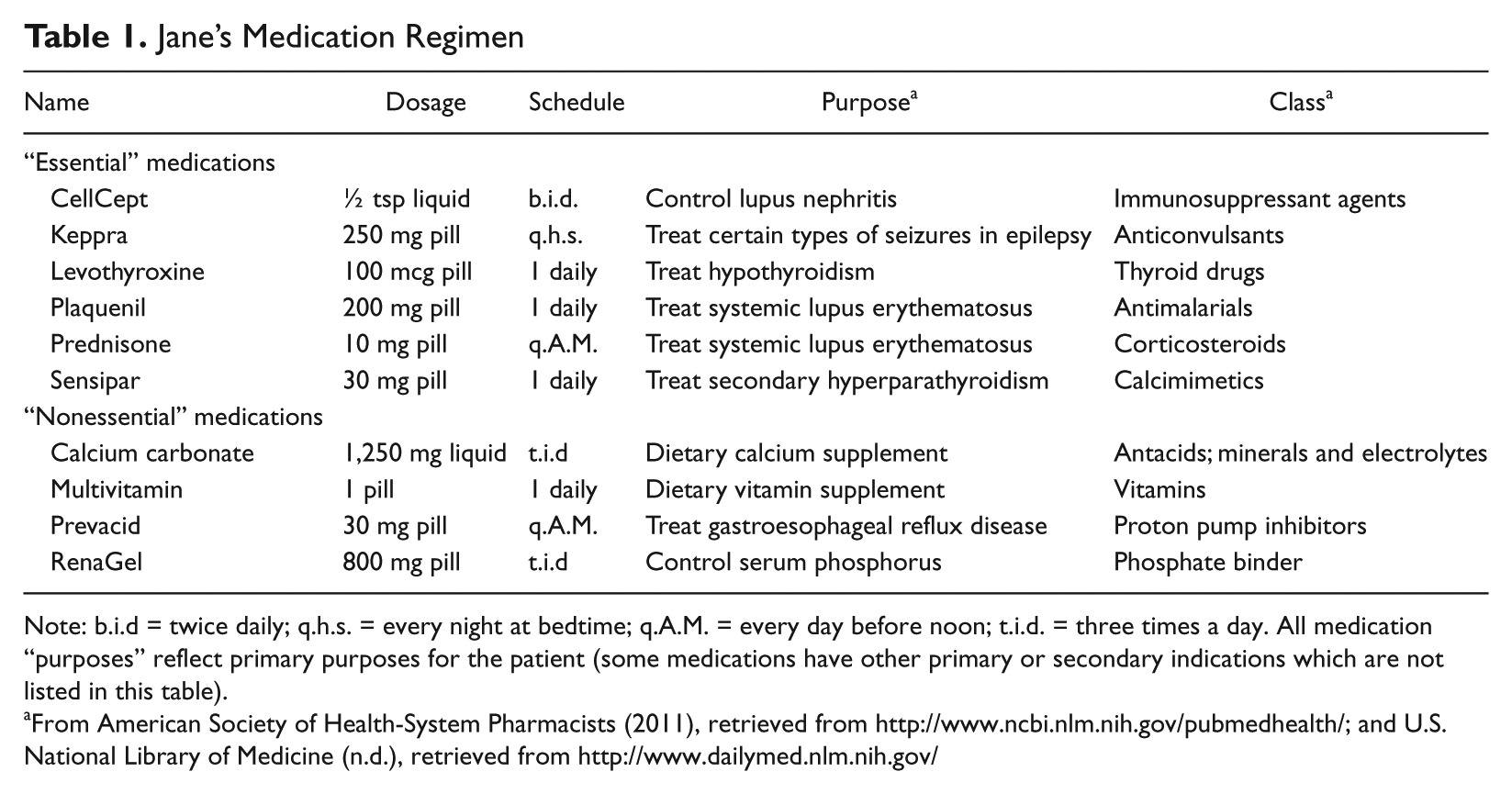
Note: b.i.d = twice daily; q.h.s. = every night at bedtime; q.A.M. = every day before noon; t.i.d. = three times a day. All medication “purposes” reflect primary purposes for the patient (some medications have other primary or secondary indications which are not listed in this table).
From American Society of Health-System Pharmacists (2011), retrieved from http://www.ncbi.nlm.nih.gov/pubmedhealth/; and U.S. National Library of Medicine (n.d.), retrieved from http://www.dailymed.nlm.nih.gov/
Jack was diagnosed with FSGS 8 years prior to enrollment and was diagnosed with hypertension and attention-deficit/hyperactivity disorder (ADHD). He was prescribed medications for FSGS, ESRD, hypertension, and ADHD (Table 2). Jack began his current clinic-based HD regimen 1.5 months prior to enrollment, with no previous dialysis history. His mother received dialysis for FSGS and his grandmother and grandfather also had the condition. Jack reported believing that his FSGS was hereditary and expressed resentment toward his family for his condition and need to take medications.
Jack’s Medication Regimen
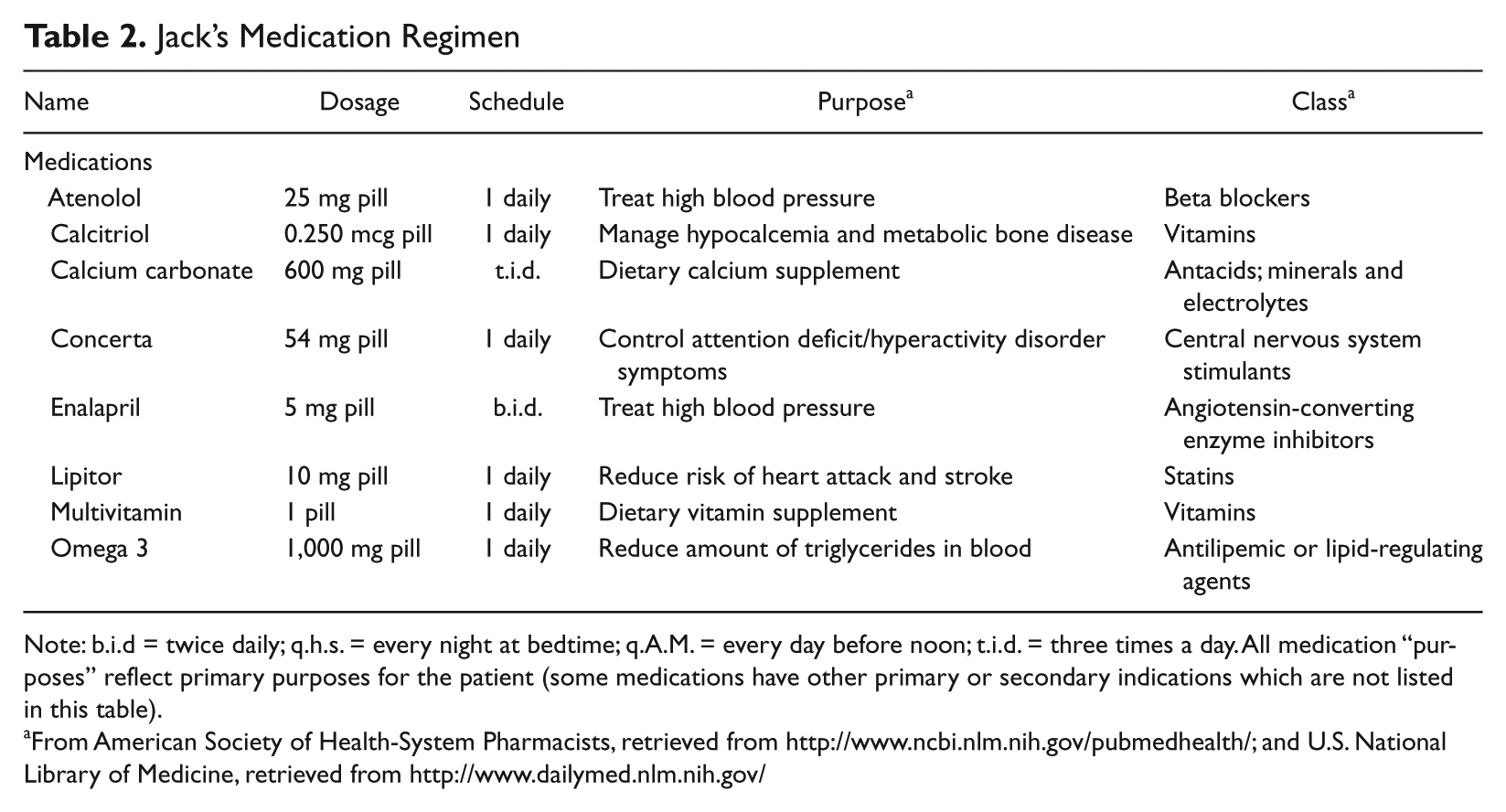
Note: b.i.d = twice daily; q.h.s. = every night at bedtime; q.A.M. = every day before noon; t.i.d. = three times a day. All medication “purposes” reflect primary purposes for the patient (some medications have other primary or secondary indications which are not listed in this table).
From American Society of Health-System Pharmacists, retrieved from http://www.ncbi.nlm.nih.gov/pubmedhealth/; and U.S. National Library of Medicine, retrieved from http://www.dailymed.nlm.nih.gov/
5 Assessment
Measures
Demographic information
Parents completed a demographic and medical information questionnaire. Medical and psychiatric diagnoses were confirmed via medical chart review.
Medical Adherence Measure (MAM)
The MAM (Zelikovsky & Schast, 2008) is a semistructured interview assessing adherence in four modules: medication, diet, exercise, and clinic attendance. For this case study, only the self-reported medication adherence domain, which is within the medication adherence module, was administered. Adolescents and parents completed weekly self-reports of adolescents’ adherence to all prescribed medications at the beginning of each baseline, intervention, and follow-up session. Weekly adherence was reported separately by each prescribed medication. Overall weekly medication adherence percentages were computed by dividing the sum of all doses taken that week by the sum of all doses prescribed that week and multiplying by 100. A previous study with adolescent transplant recipients indicated good internal consistency for parent and adolescent report (Cronbach’s α = .88 and .84, respectively; Simons & Blount, 2007).
Family Responsibility Questionnaire (FRQ)
The FRQ was adapted from eight questions on the Inflammatory Bowel Disease-Family Responsibility Questionnaire (IBD-FRQ; Greenley et al., 2010). The IBD-FRQ assesses RR in adolescents with IBD and their parents (Cronbach’s αs = .80 for youth, maternal, and paternal report; Greenley et al., 2010). Parent and adolescent provided weekly ratings of their own perceived RR and RR assumed by the other (e.g., adolescent rated self- and parent RR; parent rated self- and adolescent RR) at the beginning of each baseline, intervention, and follow-up session. Examples of question items included, “How involved is each person in knowing the names and dosages of [adolescent’s] medications?” Each question was rated on a scale from 1 (not involved at all) to 9 (involved all the time). Weekly mean scores were computed for each adolescent- and parent-report by summing the ratings of the eight questionnaire items and dividing by 8.
Illness Management Survey (IMS)
The IMS (Logan, Zelikovsky, Labay, & Spergel, 2003) is a 27-item self-report inventory that was used during the baseline phase to aid in identifying barriers to adherence that would be targeted during intervention. Questions are answered on a 5-point Likert-type scale. The IMS was originally developed for adolescent asthma patients. The initial evaluation study reported good internal consistency (Cronbach’s α = .88; Logan et al., 2003).
6 Case Conceptualization
Both patients’ issues with adherence were conceptualized through the HBM’s “perceived barriers” component, an empirically supported predictor of medication adherence behavior (Janz & Becker, 1984). Barriers were defined as issues, such as forgetting, being away from home, or refusing to take the medication (Zelikovsky et al., 2008), which were obstacles to medication taking and contributed to medication nonadherence. By providing skills and knowledge necessary to remove barriers, it was hypothesized that medication adherence would improve. Conceptualizing adherence as being influenced by each patient’s perceived barriers to medication taking allowed the interventionist to flexibly address a variety of barriers to adherence as they emerged during treatment.
RR is an important component of medication adherence and was targeted as a modifiable factor that positively influenced adherence behavior. Guided by previous RR and adherence research (Helgeson et al., 2008; Pai & Ostendorf, 2011), adherence was conceptualized as being dependent on higher parental involvement, as well as patients sharing RR with parents. Integrating RR into the adherence conceptualization, lower RR was viewed as a barrier that was fundamentally linked to adherence behavior. It was hypothesized that providing knowledge about the influence of RR on adherence and teaching problem-solving skills to foster optimally allocated RR would promote high parent and shared parent–adolescent RR to support adherence.
Within this conceptualization, intervention to increase patients’ adherence behaviors involved providing knowledge and skills to remove adherence barriers. As such, treatment was also developed around the perceived barriers framework (Rapoff, 2010) to target a broad range of modifiable factors that would be amenable to intervention. Based on empirically supported treatment for enhancing pediatric medical adherence and recommended practices for enhancing renal patients’ adherence, treatment selection was multicomponent and included educational, behavioral, and cognitive components (Graves et al., 2010; Kahana et al., 2008; Sharp et al., 2005). The educational component was included to address low medication and disease knowledge as a modifiable adherence barrier (Simons & Blount, 2007) that would provide the foundation for subsequent modules. Problem-solving, organizational, and coping skills components were included as skills to remove behavioral barriers to adherence. Cognitive restructuring was included to remove cognitive adherence barriers, such as having thoughts that medications are not effective.
7 Course of Treatment and Assessment of Progress
Intervention
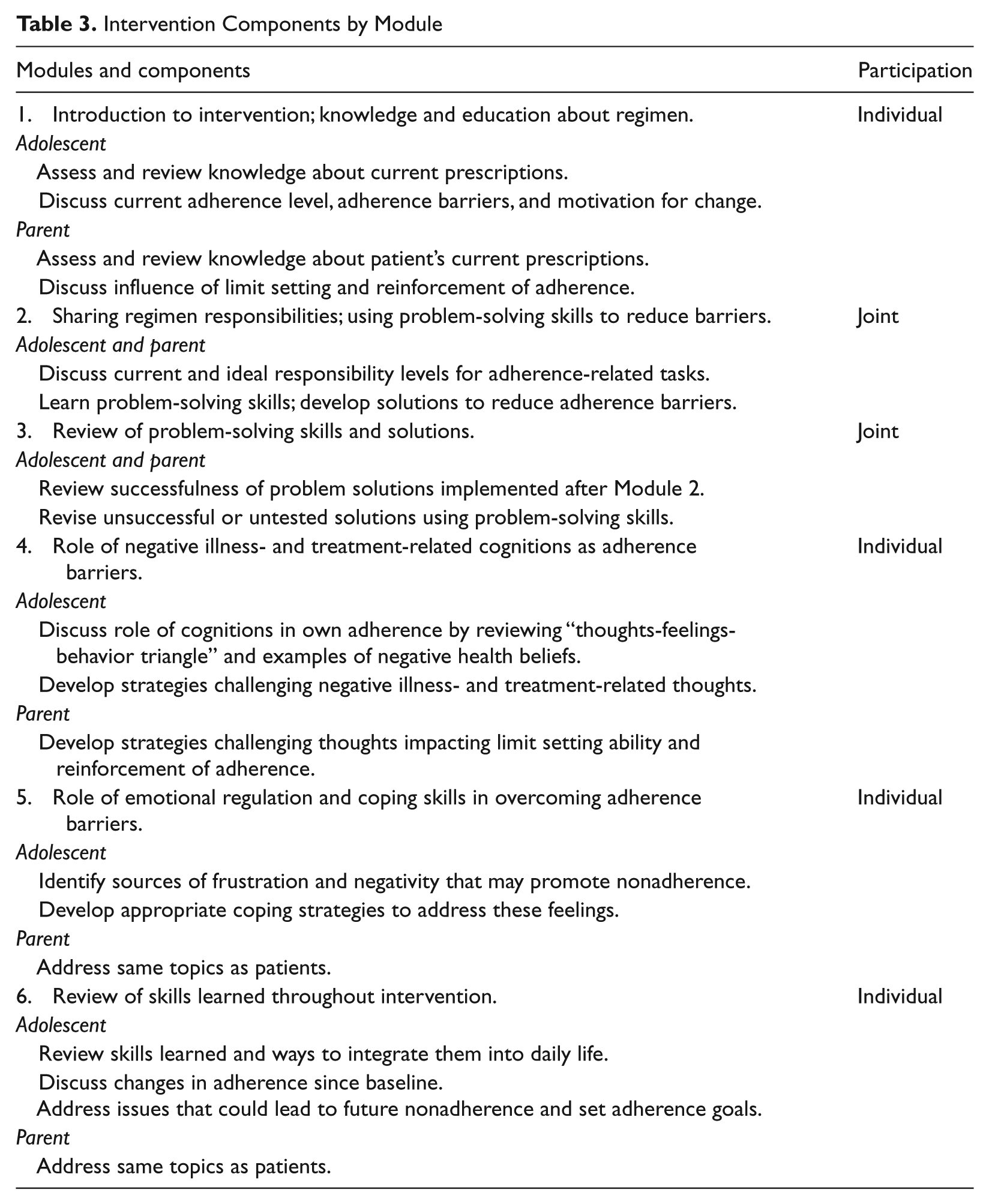
The intervention consisted of six modules (Table 3) designed to identify and address knowledge, behavioral, and cognitive barriers to medication adherence. Modules were manualized to standardize content and limited to six for clinical practicality. Specific RR issues and adherence barriers addressed were based on patient input and baseline IMS, FRQ, and MAM assessment. Adolescents completed one module per week individually during HD sessions. Modules 1, 4, 5, and 6 were completed individually with the patient and interventionist. Modules 2 and 3, which addressed sharing RR, determining ideally allocated parent–adolescent RR levels, and using problem-solving skills to reduce barriers, were completed jointly with adolescents, parents, and the interventionist. The jointly completed modules required more communication and cooperation between parent and adolescent, particularly in determining allocation of RR, and benefited from the interventionist’s facilitation. For adolescent-only modules, parents received session summaries to foster support and monitoring of adherence. A quiz was given after each session to assess knowledge of skills before progressing to the next module. The intervention was completed in a minimum of 6 weeks. Modules could be repeated if quiz scores were low or if the interventionist (an advanced graduate student) determined a need. Sessions began with a review of skills, issues applying skills, and the medication regimen.
Intervention Components by Module
Procedure
All data collection and intervention sessions occurred during patients’ multihour HD appointments. Participants completed the IMS once during baseline. Participants completed the MAM and FRQ to establish adherence and RR rates over 4 to 5 baseline sessions and at the beginning of each intervention session. Including data collection, intervention sessions lasted 60 to 90 minutes.
Analysis
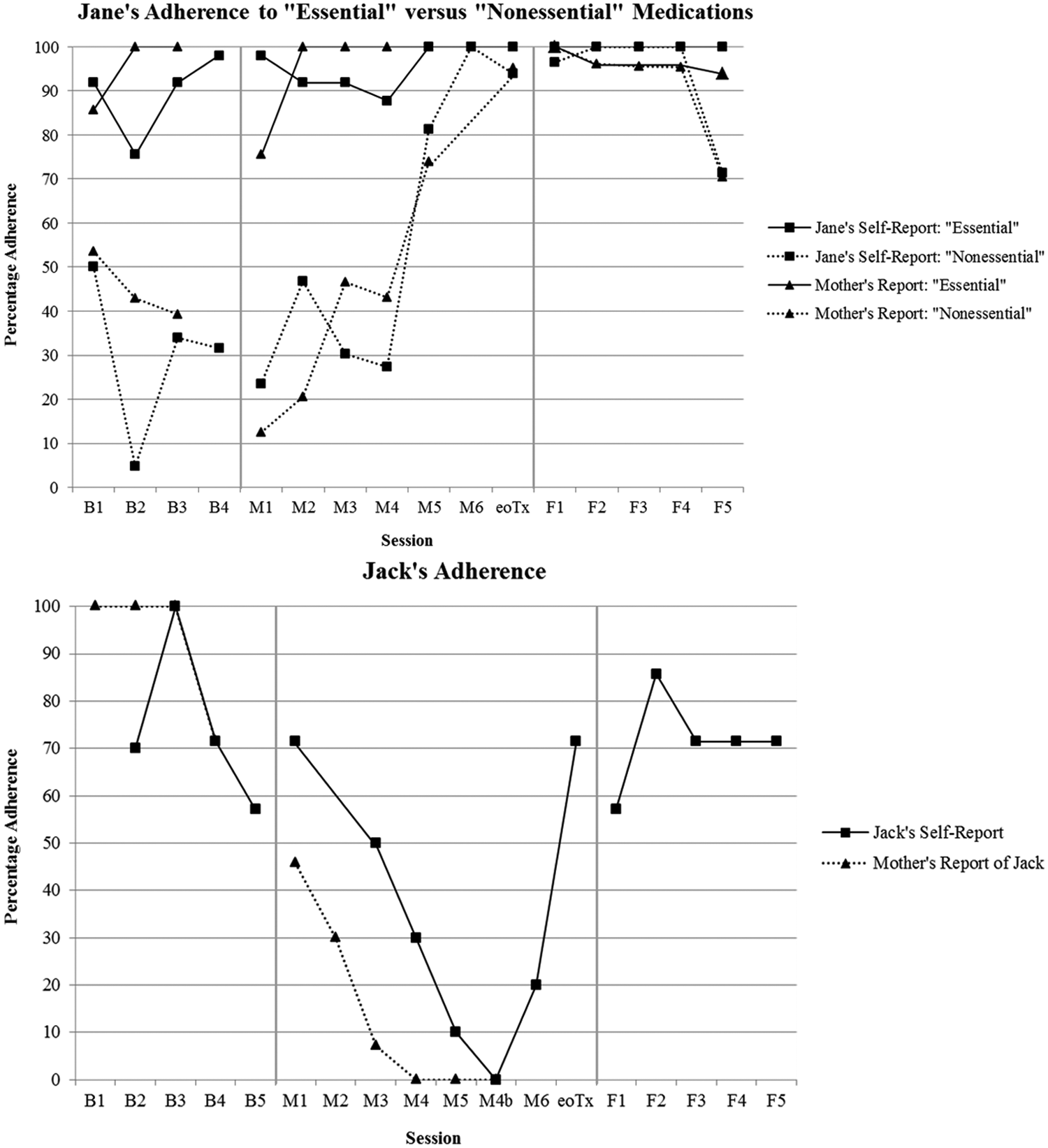
Weekly mean adolescent and parent report of adherence and RR data were plotted on line graphs to visually present and identify trends (Figures 1 and 2). Ranges are also presented in text for both dependent variables.
Changes in participants’ weekly mean percentages of adherence over time by patient- and parent report
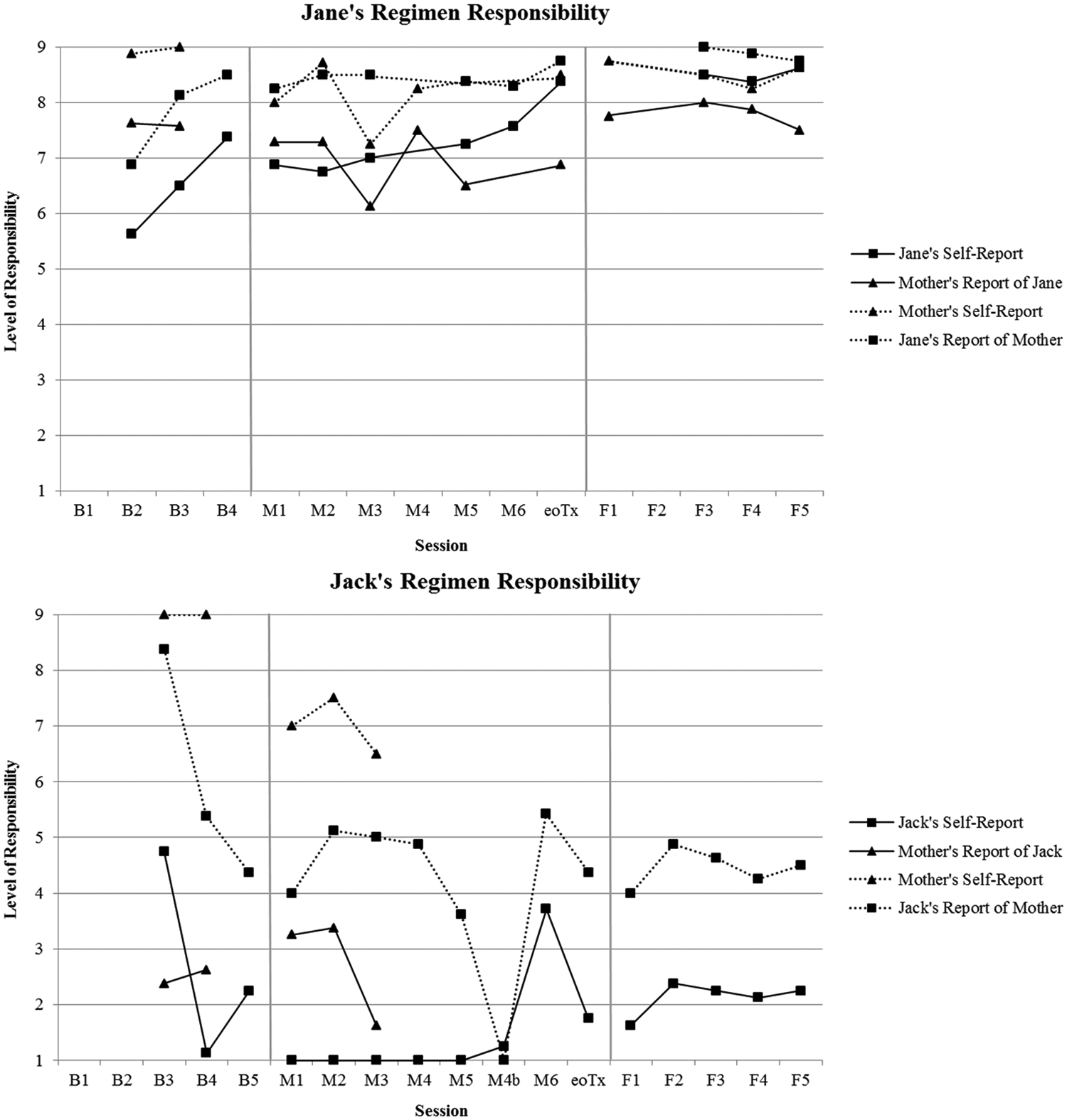
Changes in regimen responsibility weekly mean ratings over time by self-report and report of the other (adolescent or parent)
Jane’s Adherence ( Figure 1 )
Baseline revealed that Jane’s “inconsistent” medication taking reflected selective nonadherence to some of her 10 prescribed medications. Over four baseline sessions, Jane was typically adherent to six medications, including anti-epileptics, lupus medications, and immunosuppressants (self-report: adherence M = 89.29%, range = 75.51%-97.96%; parent report: adherence M = 95.24%, range = 85.71%-100%); she was mostly nonadherent to four medications, including vitamins and phosphate binders (self-report: adherence M = 30.07%, range = 4.88%-50.00%; parent report: adherence M = 45.24%, range = 39.29%-53.57%). Jane accurately described the purpose of each of the 10 medications but reported viewing those to which she was nonadherent as “nonessential” to her immediate health. The term nonessential refers to the four medications that Jane thought were unnecessary to take consistently (Table 1). Jane’s mother reported awareness of her nonadherence but had difficulty enforcing adherence. She reported feeling guilty making Jane take medications that she did not want to take.
During the treatment phase, Jane’s adherence to “nonessential” medications remained low from Module 1 until Module 4, which targeted illness- and treatment-related cognitions as adherence barriers (self-report for Modules 1-4: adherence M = 31.95%, range = 23.53%- 46.81%; parent report: adherence M = 30.71%, range = 12.50%-46.67%). Jane challenged her thoughts about some medications being “nonessential” by thinking about the long-term usefulness and purpose of each medication. Another cognitive barrier was Jane’s frustration with taking so many medications and desire to control things she felt were medically “nonessential.” To address this barrier, Jane developed alternative adherence-promoting thoughts, such as “I have control over my life. My kidney disease doesn’t have control.” Jane’s mother’s guilt and lenient enforcement of total medication adherence was also targeted. She was emotional when discussing how she allowed nonadherence despite understanding the regimen’s importance. Previous thoughts included, “Jane is so frustrated, and I feel guilty making her take them [medications Jane believed were nonessential].” Alternative adherence-promoting thoughts included, “She has to have them [her medications].”
After Module 4 and through the end of treatment, Jane’s adherence to “nonessential” medications increased to near-perfect levels (self-report for Module 5 to end of treatment: adherence M = 91.71%, range = 81.25%-100%; parent-report: adherence M = 84.56%, range = 73.91%-95.24%). Her adherence to “essential” medications improved to perfect levels.
Jack’s Adherence ( Figure 1 )
Baseline data confirmed Jack’s refusal to assume age-appropriate RR and volitional nonadherence (“I just don’t want to take them [my medications]”). Jack and his mother reported perfect to near-perfect adherence to his eight prescribed medications in the first three baseline sessions (self-report: adherence M = 85.00%, range = 70.00%-100%; parent-report: adherence M = 100%, range = 100%), though his adherence was due to his mother’s assumption of near total RR. Jack’s mother reported increasing frustration with Jack’s lack of RR and, at the end of baseline, reduced involvement in his care. Her reduced involvement coincided with markedly decreased adherence rates from initial baseline levels.
During treatment phase, Jack was minimally engaged with the interventionist, but passed knowledge-based quizzes and progressed through the modules. However, his adherence worsened from Module 1 to Module 5 (self-report: adherence M = 40.36%, range = 10%-71.43%; parent-report: adherence M = 16.60%, range = 0%-45.86%) at which point he had the opportunity to repeat any of Modules 3 to 5. He chose to repeat Module 4 targeting cognitive barriers to adherence. Jack appeared to be resistant, but more effectively challenged negative thoughts. His mother withdrew from the study after Module 5 (she was absent for Modules 4-5 and provided adherence data via telephone), reporting that she was “tired of discussing Jack’s issues” and frustrated by his nonadherence despite her assistance. She permitted Jack to finish the study. Jack agreed to finish but not repeat any other modules. When asked what he learned from the intervention, Jack identified the cognitive model’s “thoughts-feelings-behavior triangle” presented in Module 4.
Self- and parent-reports of Jack’s adherence were highly correlated until Jack’s mother withdrew from the study (r = .87; p = .005), providing support for the validity of Jack’s self-reported adherence for the study’s remainder. Jack’s adherence decreased from Modules 1 to 5, but improved from 0% before repeating Module 4 to 71.43% at the end of treatment. Jack’s adherence at the end of treatment was relatively consistent with his self-reported adherence at baseline, when his mother was clearly supervising all medication taking. Improved adherence toward the end of treatment coincided with Jack’s reports of his mother’s resumed supervision for medication-taking. It is unclear from outcome measures whether maternal frustration had significantly subsided, but Jack reported that he and his mother were communicating more at this point.
Jane’s RR ( Figure 2 )
Jane and her mother assumed high RR levels during baseline and treatment. FRQ scores reflected being involved “a lot of the time” to “all the time.” In Modules 2 and 3, Jane and her mother worked with the interventionist to determine ideal RR levels for adherence tasks. Jane and her mother each reported who was currently responsible for specific adherence-related tasks. In discussion with the interventionist, they identified areas of discrepancy and clarified who would be responsible for those tasks. After a review about RR levels that should best support medication adherence in adolescents, Jane’s mother identified a need to maintain some responsibility for monitoring Jane’s adherence but encourage Jane to be responsible for her own care. Jane and her mother determined their own ideal RR levels and developed a plan to maintain these distributions by specifying who would take primary responsibility for completing various adherence-related tasks. During problem-solving training, they generated options to improve Jane’s adherence and developed a system for managing RR. Jane’s self-reported RR increased from “involved a lot of the time” at Module 1 to “involved all the time” by the end of treatment. Her mother remained “involved all the time” through the end of treatment.
Jack’s RR ( Figure 2 )
Jack occasionally reported RR scores reflective of being “involved a little of the time” or “some of the time” during baseline and treatment, but reported being “not at all involved” for most of the study. Working with Jack and his mother in Module 2 revealed significant family conflict regarding Jack’s RR. When the interventionist attempted to facilitate clarification of how RR was allocated between Jack and his mother, Jack reported that he assumed no RR besides attending HD sessions. His mother wanted him to become 50% to 100% responsible for his regimen but Jack stated that he would not assume any additional RR in the future. In Module 3, Jack stated that he had not tried any strategies from Module 2 and was unmotivated to change.
Jack’s mother reportedly attempted to facilitate change between Modules 2 and 3, but was unsuccessful due to Jack’s oppositionality and refusal to assume more RR. She reported being “involved a lot of the time” or “all the time” until she stopped actively participating in the intervention. There were no maternal RR reports after she withdrew. Concurrent parent–adolescent RR reports were not significantly correlated, suggesting discrepant perceptions of respective RR. Jack’s report indicated that he had lower RR than his mother, his mother’s RR decreased as the intervention progressed, and his RR was already decreasing before his mother’s withdrawal. Before withdrawing, Jack’s mother confirmed his lack of adherence, his low RR, and her decreased RR via telephone. Jack reported an increase in his and his mother’s RR after repeating Module 4. RR and adherence improvements coincided.
8 Complicating Factors
Although this case study is a notable step in addressing medication adherence and related RR issues in adolescents with HD-dependent ESRD, there were complicating factors and limitations. The intervention was implemented in an AB case-series design, so it was not possible to determine whether changes were due to the intervention or to isolate the most effective treatment component. Follow-up began 2 weeks after treatment ended, lasted 5 weeks, and indicated that adherence gains were maintained. A longer follow-up would have provided additional support for observed changes (Kahana et al., 2008).
Jack’s case was complicated by his negativistic behavior, maternal frustration, ADHD, school difficulties, reactions to a friend’s death, and resentment over his ESRD and medical regimen. These factors likely interfered with his motivation to meet intervention goals. Jack’s ADHD was uncontrolled as his medication adherence decreased. Other psychosocial issues were left to be addressed by his outside therapist. There was no attempt to coordinate care but this is an important treatment issue to consider when implementing future adherence interventions.
9 Access and Barriers to Care
Implementing the intervention during regularly scheduled HD sessions was time-efficient and eliminated the need to attend additional appointments to receive services. This intervention model provided greater access to care for families who may have been unable to attend additional sessions due to economically driven barriers such as transportation difficulties or child care costs. Participants may have been more receptive to discussing personal health care issues in a familiar setting where they already received care. However, the family-based intervention was not feasible for patients whose parents did not attend HD sessions due to work or other schedule constraints.
Although not directly measured, material costs were minimal as the intervention modules mainly involved discussion between the patient, parent, and interventionist. Medical costs were not actively assessed as a barrier to medication adherence, and patients and parents did not mention them as interfering with medical care. Still, medical costs may have interfered in medication adherence for both patients and may be significant adherence barriers for other patients and families. Supporting medication adherence and RR in pediatric patients with chronic illnesses could reduce health care utilization due to nonadherence and save medical costs for patients and the health care system.
10 Follow-Up
A 5-week follow-up phase began 2 weeks after the intervention ended, during which participants completed the MAM and FRQ weekly.
Maintenance of Medication Adherence Gains
Jane’s improvements in “nonessential” medication adherence were maintained during follow-up (self-report: adherence M = 93.57%, range = 71.43%-100%; parent report: adherence M = 91.54%, range = 70.45%-100%). Jane and her mother reported a slight drop in nonessential medication adherence in the final follow-up session, but attributed this to an insurance issue preventing timely prescription refill rather than Jane’s refusal to take the medication.
Jack’s improvements in medication adherence after repeating Module 4 were generally maintained during follow-up (self-report: adherence M = 71.43%, range = 57.14%-85.71%) and were relatively consistent with his self-reported adherence levels at baseline. His self-reported weekly medication adherence mean plateaued after the third follow-up session.
Maintenance of RR Gains
Jane remained “involved a lot of the time” to “involved all the time” with managing her medication taking during follow-up. Her mother remained “involved all the time” with managing Jane’s medication taking during follow-up.
Improvements in Jack’s report of his mother’s RR toward the end-of-treatment were maintained during follow-up when Jack rated his mother as “involved some of the time” with managing his medication taking. Jack’s self-reported RR remained low during follow-up but was higher than during Modules 1 to 5.
11 Treatment Implications of the Case
Practical aspects of this intervention include efficient delivery during regularly scheduled HD sessions, following a manualized plan, and tailoring modules based on patient input and issues emerging during treatment. The conceptual framework based on the HBM’s perceived barriers component allowed for flexible application to patients’ unique adherence and RR issues.
The intervention was conducted with two African American adolescents, which we consider to be a unique contribution of this case study. Most adherence interventions have included primarily White participants (Kahana et al., 2008). The intervention model was designed to be applicable to any pediatric patients from diverse backgrounds with the shared experience of attending HD sessions to treat ESRD. By conducting individualized assessments, the interventionist can tailor the modules to address individual barriers endorsed by patients facing a variety of adherence-related challenges. Some patients’ barriers may be closely tied to socioeconomic status (e.g., cost of medications, lack of health insurance), whereas other patients’ barriers may relate to organizational difficulties (e.g., forgetting dosage schedule, missing clinic appointments, failing to refill prescriptions on time).
Jane’s improvement in adherence to “nonessential” medications and Jack’s improvement in adherence by the end of treatment partially met the hypothesis that adolescents would demonstrate increased adherence after treatment. The findings are encouraging for using cognitive-behavioral adherence interventions with adolescents on HD, pretransplantation. Addressing medication adherence issues before transplantation could improve adolescents’ eligibility for receiving a transplant and improve posttransplant adherence and health outcomes.
Jane’s adherence to “nonessential” medications improved after completing Module 4 and Jack’s adherence also improved after repeating this module. For Jane, challenging thoughts about “nonessential medications” may have altered her perception of their long-term value, thereby facilitating change. Similarly, Jane’s mother challenged thoughts associated with adherence-related guilt, likely resulting in a shift of her perceived parental role and empowering her to support total adherence for Jane.
Jack identified the “thoughts-feelings-behavior triangle” as information learned from the intervention. Acquiring cognitive skills may have increased Jack’s motivation to adhere, which, coinciding with Jack’s report of his mother’s reassumption of RR, may have contributed to his improved adherence after Module 4. Given Jack’s resistance to participating in his medical treatment and the intervention, however, it is unclear how the specific cognitive-behavioral skills taught in the intervention may have helped Jack become more adherent to his medications toward the end of treatment and during follow-up. The skills covered in the intervention may have enhanced Jack’s awareness of his mother’s important role in his treatment and reduced his resistance to her supervision. Outcome assessments used in this case study do not specifically document these processes.
Although there is supporting evidence that Module 4 contained the most active treatment components, small sample size precludes a definite conclusion and requires further evaluation. Still, clinicians may wish to elicit patients’ cognitions about their medication regimens or diagnoses as barriers to medication adherence, in addition to targeting behavioral- and knowledge-based barriers. Decisions to partially or completely not adhere are often based on perceived treatment burden or beliefs about health and medications (Graves, Adams, Bender, Simon, & Portnoy, 2007). Believing that some medications are less efficacious than others, inaccurately assessing nonadherence costs, and having less treatment burden by taking fewer medications might outweigh potential nonadherence-related medical complications for many adolescents. Jane’s case specifically demonstrated how targeting cognitive adherence barriers could help facilitate behavioral change.
There was less evidence that adolescents would demonstrate increased self- and parent-reported RR and shared RR with parents after treatment. Jane and her mother shared high RR before enrolling, which remained stable throughout the study. Jack’s RR remained low and his mother’s RR decreased until she withdrew from the study. Jane’s improved adherence and Jack’s improved adherence after his mother reportedly reassumed RR suggest that this intervention may be most successful when parents already have or are willing to consistently use high levels of RR.
Issues related to adolescent and parent expectations for RR warrant clinical assessment. For example, Jack’s mother had difficulty coping with his low RR and defiance, which likely reflected his developmental maturity level and other complicating factors. She may have benefited from learning behavioral management and emotion regulation strategies. Screening for family conflict related to expectations for RR is also warranted. Family conflict may have fueled disagreement about appropriate RR levels for Jack, reflected by Jack’s and his mother’s discrepant reports of parent–patient RR. In adolescent renal transplant recipients, greater parent–patient discrepancy on respective reports of total patient treatment responsibility was associated with poorer oral medication adherence (Pai et al., 2010). Clinicians may wish to address parent–adolescent disagreement on their respective expectations regarding RR with the goal of both parties assuming high responsibility for adherence. In addition, in cases like Jack’s where there is a host of complicating factors, it may be more appropriate to first address other issues that would likely impede the adolescent’s ability to assume more RR. Once those issues are adequately addressed, the clinician may consider working with the family to modify RR.
12 Recommendations to Clinicians and Students
This case study provides initial support for the feasibility and efficacy of addressing adherence and RR issues in adolescents with ESRD pretransplant, during regularly scheduled clinic-based HD sessions, and using a multicomponent cognitive-behavioral treatment protocol. Clinicians should consider issues emerging during this intervention’s implementation (e.g., cognitively driven selective nonadherence, family conflict related to expectations for allocation of parent–adolescent RR, and complicating psychosocial factors) when attempting to promote adherence and appropriately allocated RR in pediatric patients on HD for ESRD. Clinicians may also use the perceived barriers framework described in this case study when conceptualizing patients’ issues with medication adherence. Cognitive adherence barriers may be useful to examine, as they were primary issues for both patients in this case study and may enhance behavioral and educational strategies to promote adherence.
The intervention described in this case study may have use with other adolescent patients with chronic health conditions who are prescribed complex medication regimens and are attempting to assume more RR. Health care providers may utilize in-clinic opportunities to provide education and cognitive-behavioral skills training to adolescents and parents that are tailored to help patients overcome specific adherence barriers. Future research should attempt to demonstrate the potential long-term impact of this intervention on patients’ health statuses and measure medical cost reductions that may be associated with improved medication adherence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by an award from the Graduate School at the University of Georgia to the first author.