
Abstract
Little empirical information is established about synthetic marijuana, including the treatment of related disorders. Similar to organic marijuana, chronic synthetic use can lead to a variety of functional impairments, including diminished academic and workplace productivity and performance. Many traditional approaches emphasize treating co-occurring disorders separately, but the present case examines concurrent treatment for Diagnostic and Statistical Manual of Mental Disorders (4th ed., DSM-IV) Synthetic Marijuana Dependence and Generalized Anxiety Disorder by using Motivational Interviewing (MI) and Relapse Prevention (RP) in conjunction with an adapted form of Dialectical Behavior Therapy (DBT). A model for treatment and its potential effects are discussed.
Keywords
1 Theoretical and Research Basis for Treatment
Of all illicit (i.e., illegal) substances, cannabis is the most commonly used in the United States (42% lifetime use in individuals 12 or older; Substance Abuse and Mental Health Services Administration [SAMHSA], 2011). Cannabis is the third most common substance reported (18% of admissions, after alcohol and opiates) for which patients seek a substance use intervention (SAMHSA, Center for Behavioral Health Statistics and Quality, 2011). Conservative estimates indicate that at least one half of the individuals with a substance use disorder have also been diagnosed with another mental health disorder (Wu et al., 2013).
The legality of marijuana, and by extension its risks and benefits, are hotly debated in light of shifting social views and political policy. Upon review of the extant literature, it becomes clear that marijuana is neither the malevolent gateway to destruction nor the completely harmless cure-all proponents on either side of the legalization spectrum espouse. Rather, the truth about marijuana lies somewhere in between (Earleywine, 2002).
Chronic cannabis use can lead to a variety of functional impairments, including diminished academic and workplace productivity and performance. Cognitive deficits related to memory and attention while under the influence and/or using regularly are detected. These cognitive impairments are no longer observed following 25 days of abstinence in adults (Schreiner & Dunn, 2012); however, there are studies that suggest that individuals who use cannabis during adolescence may experience cognitive impairment into adulthood (Meier et al., 2012; Raver, Haughwout, & Keller, 2013; Zalesky et al., 2012).
In addition, legal problems due to the possession of cannabis can extend into other arenas of one’s life such as their ability to acquire federal financial aid for education or one’s ability to secure gainful employment. Unlike other illicit and licit substances, many of the most impactful consequences are observed as a result of the legality of the substance.
Synthetic Marijuana
A diagnosis of Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV, American Psychiatric Association [APA], 1994) Cannabis Dependence is appropriate for cases in which criteria are satisfied with a chemically similar, synthetic compound. Despite widespread availability and use, synthetic marijuana herbal blends are largely unfamiliar to both professionals and laypeople alike. Synthetic marijuana is commonly referred to and sold as K2 or Spice. It consists of plant matter that is sprayed with chemical grade synthetic cannabinoids, which are typically smoked. The packages are labeled as incense and are clearly marked “not for human consumption.” These marijuana alternatives can be purchased in gas stations and head shops. Although laws have been implemented in many states to ban the substances, companies simply reconfigure the chemical structure and re-release a new blend.
Because of the ease of access and large Internet sales presence, it is difficult to estimate the demographics of those who use synthetic cannabis. Individuals who may be motivated to avoid drug detection or legal consequences, such as military personnel, individuals on legal probation, or those participating in substance use treatment programs, are the most frequently reported demographic (Rosenbaum, Carreiro, & Babu, 2012). To date, some urine-based detection tests have been developed, but they have been plagued by inaccuracies and have not been demonstrated to be reliable due to frequently changing chemical formulations.
Although there is little objective empirical information, anecdotal reports about psychotic episodes, seizures, paranoia, delusions, anxiety, and agitation have proliferated (e.g., see Hurst, Loeffler, & McLay, 2011; Müller et al., 2010; Tofighi & Lee, 2012). Commonly described physical side effects include tachycardia, diaphoresis, conjunctival injection, and xerostomia.
2 Case Introduction
Amelia was a 28-year-old married Caucasian female. She was a U.S. Navy veteran and was a non-degree seeking student at a large public university. Amelia was referred by the Alcohol and Other Drug Office (AOD) on campus to address co-occurring anxiety symptoms.
3 Presenting Complaints
Amelia reported smoking synthetic marijuana (Spice) up to 40 times per day, with a typical pattern of 20 to 30 times daily. Amelia reported that she was experiencing impairment across several domains of functioning. She also indicated that she was experiencing symptoms associated with depression and anxiety.
4 History
Amelia experienced a tumultuous childhood marked by multiple intra-state moves. Amelia’s parents ended their relationship when Amelia was 8 due to her father’s chronic substance use (primarily cocaine and marijuana). She has developed a strong relationship with her mother, brother, and other extended family members, but continues to work on her relationship with her father.
She described two romantic relationships as emotionally, physically, and sexually abusive that occurred during her teenage years. Amelia reported that she did not graduate from high school due to chronic truancy; however, she earned her General Education Development (GED) and completed a bachelor of arts degree in English. After graduation, she joined the Navy to “see the world” but was never deployed.
Amelia was taking Celexa (20 mg daily) for 6 months prior to assessment for the treatment of depression and anxiety, which she began experiencing while in the Navy in her early twenties. Amelia reported that while she felt the medication had helped in the past, she returned to pre-medicated symptom levels at the time of the assessment.
Amelia saw a counselor at age 12 for behavioral problems (i.e., drinking alcohol, skipping school, smoking cigarettes, etc.), but stated that she was disinterested in treatment and did not make treatment gains. At age 14, she cut herself, called police, and reported that she was trying to kill herself after a fight with her parents. As a result, she spent 2 weeks in an inpatient facility. Amelia denied actual suicidal intent, but explained that the event was in response to extreme stress and a “cry for help.” At age 17, she saw a counselor for 6 months who she reported inspired her and encouraged her. She reported temporary attenuation of depressive symptoms subsequent to seeing this therapist, but terminated treatment because she moved to another state. At age 27, she saw a counselor for 5 months who treated her with Eye Movement Desensitization and Reprocessing Therapy and Cognitive Therapy, but she reported experiencing minimal gains, and thus terminated the treatment. At age 28, she presented to the AOD at her university on a voluntary basis.
5 Assessment
Functioning
Amelia lived with her husband. She was enrolled full-time as a non-degree seeking student to fulfill prerequisites for a graduate program and worked part-time as a waitress. She was struggling to pass her classes as a direct result of her substance use.
She reported that her marriage was plagued by difficulties related to differing communication styles and perceived problematic familial relationships. She indicated that her husband disapproved of the frequency of her substance use and that he would often “punish” her with verbal tirades; thus, her continued use was adding stress to their marriage.
It was determined that Amelia was in the preparation stage of change (i.e., recognizing that a change was necessitated and making plans to do so yet not engaging in any change behaviors). Antecedents and consequences of her substance use were discussed at length. It was concluded that Amelia was most likely to use when feeling strong emotions of any kind (i.e., both positive and negative) and experiencing high levels of stress. She also reported using it to help her sleep and cope with boredom.
Personality Assessment Inventory (PAI)
The PAI (Morey, 1991) is a 344-item self-administered inventory of adult personality designed to assess various constructs related to psychological functioning. Specifically, the PAI contains 4 validity scales, 11 clinical scales, 5 treatment scales, and 2 interpersonal scales. A T score of 50 (standard deviation = 10) reflects a normal level of functioning, and a T score of 70 or above (two standard deviations above the mean) indicates a clinically significant elevation on the relevant scale. Results revealed that validity scales were within normal limits, indicating that Amelia responded to the questionnaire in an honest and open manner and paid attention to the items. Results revealed mild-to-moderate elevations on the primary clinical scale for anxiety (T = 66), anxiety-related disorders (T = 66), and borderline (T = 69); a moderate elevation on depression (T = 71); and a severe elevation on drug problems (T = 92). The PAI suggested that Amelia’s level of motivation for treatment was comparable with that of adults who are being seen in a therapeutic setting.
Cannabis Use Disorder Identification Test (CUDIT)
CUDIT (Adamson & Sellman, 2003) is a 10-item multiple-choice self-report inventory designed to assess the risk level of cannabis use and the likelihood of the presence of a cannabis-related substance use disorder over the last 6 months. Amelia’s score of 25 corresponds with a Very High Risk level. It is noteworthy that because Amelia’s presenting complaint concerned synthetic marijuana, she was asked to respond with both synthetic and non-synthetic forms in mind.
Alcohol Use Disorder Identification Test (AUDIT)
AUDIT (Babor, de la Fuente, Saunders, & Grant, 1992) is a 10-item multiple-choice self-report inventory designed to assess the risk level of alcohol use and the likelihood of the presence of an alcohol-related use disorder over the last year. Amelia’s score of 8 corresponds with a Low-to-Moderate Risk level, but further discussion revealed that her score was slightly elevated due to behaviors that occurred approximately 6 months prior to assessment (i.e., blackouts, unable to stop once started, and guilt).
Beck Depression Inventory–II (BDI-II)
BDI-II (Beck, Steer, & Brown, 1996) is a 21-item multiple-choice self-report inventory designed to assess for the severity of common symptoms of depression over the past 2 weeks. Amelia’s score of 29 on the BDI-II corresponds with a severe level of depressive symptoms. Amelia endorsed passive suicidal ideation, but denied intent, plan, and/or means.
Beck Anxiety Inventory (BAI)
BAI (Beck & Steer, 1993) is a 21-item multiple-choice self-report inventory designed to assess for the severity of common symptoms of anxiety over the past week. Amelia’s score of 29 corresponds with a severe level of anxiety.
Structured Clinical Interview for the DSM-IV (SCID)
SCID (First, Spitzer, Gibbon, & Williams, 1996) surveys for symptoms related to major DSM-IV disorders. Amelia endorsed symptoms related to anxiety, depression, and substance dependence. Although Amelia reported experiencing two panic attacks over her lifetime, she did not have a persistent fear of another attack. Amelia further reported periods of binge eating without inappropriate compensatory behaviors during adolescence. She experienced two major depressive episodes between the ages of 16 and 18. Although her BDI-II score was elevated, she did not endorse persistently depressed mood or anhedonia. It is likely that her Generalized Anxiety Disorder (GAD) symptoms accounted for her elevated score. Specifically, Amelia endorsed decreased sleep, decreased appetite, difficulty concentrating, guilt, and self-criticalness on the BDI-II, which are likely due to her GAD and/or repeated unsuccessful attempts to quit smoking syntehtic marijuana. Amelia indicated a variety of psychosomatic symptoms (e.g., stomach pains, feeling hot, feeling shaky) in addition to cognitive symptoms of anxiety (e.g., excessive worrying about her job, money, health, weight, parents, and her friends and a perpetual state of feeling nervous and scared).
Amelia reported using several substances throughout her life including regular use of marijuana (synthetic and non-synthetic), alcohol, tobacco, Lysergic acid diethylamide (LSD), and mushrooms in addition to experimental use of Xanax, crank, opium, Codeine, cocaine, and ecstasy. Amelia began using marijuana and alcohol at age 12. She used both intermittently until age 16 when she began smoking every day. At age 17, she stopped all substance use for 6 months. Between the ages of 17 and 18, she consumed alcohol occasionally and began smoking tobacco; she resumed experimental use of other substances at age 18. Amelia also reported that between the ages of 20 and 23, she pledged a sorority and believed that she abused alcohol (e.g., consumed 15-20 standard drinks 2 to 3 times a week, often resulting in blackouts, getting sick, etc.). Amelia began using synthetic marijuana at age 25 to avoid detection while in the military.
Amelia reported that she made several attempts to cut down her use of synthetic marijuana, but typically relapsed after 2 to 3 days of abstaining. She indicated that she experienced difficulty concentrating and sleeping, and fatigue, headaches, and irritability while attempting to abstain.
6 Case Conceptualization
Amelia met the criteria for Generalized Anxiety Disorder, as evidenced by her frequent, global worry and excessive rumination, trouble controlling her worry, sleep difficulties, concentration difficulties, irritability, and psychosomatic symptoms.
Amelia met DSM-IV criteria for Cannabis Dependence. Amelia was assessed 7 months prior to the release of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5, APA, 2013), but it is noteworthy that she would have met the criteria for Substance Use Disorder per the revised criteria. She was smoking up to four dozen times per day and suffering major consequences associated with finance, her education, and personal relationships. She indicated experiencing tolerance, withdrawal symptoms, and multiple unsuccessful attempts to moderate her use. Amelia reported using Spice/K2 to avoid experiencing emotions and anxiety and to help her sleep.
Amelia has experienced several events in her lifetime that are somewhat atypical for children and adolescents. Rather than appropriate coping mechanisms and skills being modeled by her parents or other family members, the common method used to cope was using substances (from alcohol, to marijuana, to cocaine). Amelia began using substances to cope with depression, anxiety, and other significant emotional distress beginning at age 12. The behavior was reinforced over time because in Amelia’s words, she was able to “escape and chill without having to deal directly with my [her] feelings.”
Amelia first aimed to moderate her marijuana use but after unsuccessful attempts, she changed her goal to abstinence from marijuana early in treatment. At the time of assessment, her alcohol use was infrequent; thus, changing her alcohol use was not a stated goal at the time of assessment. However, as her marijuana use decreased, an increase in risky alcohol consumption was observed and Amelia set a goal of moderating her alcohol use. Years of empirical research suggest that controlled drinking is an appropriate goal for many individuals with problematic alcohol use (Saladin & Ana, 2004).
Given Amelia’s course, history, and symptoms, the first step was to engage her in Motivational Interviewing (MI), a style of therapy where the goal is to guide the client and strengthen motivation for change (Miller, 1983). Then, an adapted form of Dialectical Behavior Therapy (DBT) was used to help Amelia cope with and regulate her emotions in a healthy way, thereby reducing her urges to use. Finally, Relapse Prevention (RP; Marlatt & Gordon, 1985) was used concurrently to maintain treatment gains.
When examining the behavioral chain of substance use for Amelia, it became apparent that her underlying anxiety was exacerbated by underdeveloped distress tolerance, coping, and interpersonal skills. An anxiety-provoking event often directly preceded Amelia’s urges (and actual) use. Thus, we hypothesized that if we could intervene before the urge occurred by teaching her how to cope with her anxiety in a healthy way (and avoid unnecessary interpersonally caused distress), her urges would occur less frequently and thus the substance-use-specific interventions would be more likely to be effective. In addition, when Amelia presented for treatment, she was very unhappy with the current state of her life and current relationships. One of DBT’s main goals is to empower and assist the client to create a life worth living. For these reasons, DBT was added to standard evidence-based substance use treatment of MI and RP.
Although not traditionally used together, MI and DBT have a great deal of overlap to the extent that Marsha Linehan and William Miller (the creators of DBT and MI, respectively) have acknowledged their similarities (Osborn, 2011).
MI/Motivational Enhancement Therapy (MET)
The positive reinforcing properties of substances are often so strong that they outweigh punishment or negative consequences. MET is a therapy that is designed to join the therapist and the patient, while the therapist aims to move the patient through stages of change. The Transtheoretical Model (TTM) proposes a five-stage sequential model of behavior change (Prochaska & DiClemente, 1983). The stages include Precontemplation, Contemplation, Preparation, Action, and Maintenance.
MI and MET are often used interchangeably; however, MET is a time-limited protocol, while MI is a broad framework and style of therapy that can be used in a more general sense throughout therapy services. Hallmarks of both include joining with the client, rolling with resistance, supporting self-efficacy, and developing discrepancy. Both services begin with identifying the person’s current stage of change with the goal of using the abovementioned strategies to motivate them along the stages. MI has been demonstrated to be effective for a variety of problems from substance use to diet and exercise. Multiple studies have demonstrated significant effects with marijuana abuse/dependence (Babor, 2004; Stephens, Roffman, & Curtin, 2000), poly-substance use (Miller, Yahne, & Tonigan, 2003), and a meta-analysis conducted in 2003 showed a combined effect d = 0.56 (95% confidence interval [CI] = [0.31, 0.82]) for drug addiction and d = 0.53 (95% CI = [0.20, 0.86]) for blood alcohol content (Burke, Arkowitz, & Menchola, 2003).
RP
RP (Marlatt & Gordon, 1985) is a cognitive-behavioral intervention which uses functional analysis to identify the behavior chain of substance use. Together, the therapist and client analyze and identify the antecedents and consequences of substance use and then develop alternative skills to reduce the risk of future use. Triggers, thoughts, feelings, use patterns, and consequences of use (positive and negative) are all considered. After successful analysis, the therapist and client work as a team to develop strategies for altering thoughts, feelings, and behaviors to help manage situations in which one’s commitment to their goals may be threatened. As with MET/MI, the therapist–patient relationship is as important to the therapy process as the interventions themselves.
DBT
DBT (Linehan, 1987) has a considerable amount of empirical support (Linehan et al., 2006). DBT is unique in that it focuses on the intersection of biological and environmental causes. Linehan posits that emotional dysregulation observed in many people results from emotional vulnerability combined with a deficit in skills necessary to regulate emotions in a healthy way. DBT focuses on balance between the rational and the emotional as well as between acceptance of situations and change. Skills training occurs in four areas: mindfulness, distress tolerance, interpersonal effectiveness, and emotion regulation. The goal is for the patient to be aware of emotionally driven behavior and use their new skills to regulate and manage said behavior. Traditionally, DBT skills training is implemented in a group format in addition to individual therapy sessions and phone coaching. In the present case, a group setting was not feasible. As such, all components outlined in the manual were adapted for one-on-one delivery.
7 Course of Treatment and Assessment of Progress
For clarity, treatment has been divided into three components: (a) Psychoeducation and Coping Skills (e.g., Progressive Muscle Relaxation [PMR], Sleep Hygiene), (b) MI/RP, and (c) DBT. A clinical psychology doctoral student delivered twenty-seven 120-min treatment sessions over the course of 9 months.
Continuing Assessment Procedures
Amelia was given a BDI-II and BAI on a monthly basis. Substance use was tracked on a weekly basis. Several variables were calculated from weekly data, including number of smoking days per week, number of smoking episodes per week (i.e., total number of bowls of marijuana smoked), peak number of smoking episodes per day, number of standard drinks, number of drinking days, typical estimated blood alcohol content, and peak estimated blood alcohol content.
Phase 1: PMR, Sleep Hygiene (Sessions 1-3)
Amelia reported that a large reason she smoked was to help her sleep at night; thus, PMR training was administered. Amelia participated in PMR (see Ferguson & Sgambati, 2009 for protocol) during the sessions and was provided with constructive feedback. She was directed to practice at least once a day. Amelia was also given information about establishing good sleep hygiene.
Phase 2: MI and RP (Sessions 3-7)
Substance use logs were reviewed and discussed. MI strategies such as developing discrepancy and eliciting change talk were used to increase motivation for change. Client discussed antecedents and consequences of use, with special attention given to risky situations (i.e., a Blood Alcohol Content (BAC) greater than 0.08 or behavior inconsistent with client’s goals). A RP plan was developed for the upcoming week and strategizing and planning for upcoming special occasions occurred.
Strategies for coping with family-related stressors, environmental stressors, and boredom were discussed. Amelia’s thoughts and feelings regarding sobriety were explored. Values clarification also took place during this phase. Amelia reported that the most important things in life to her were being an English teacher, being creative, being a “good” family member, and exploring other cultures.
Amelia also admitted to experiencing suicidal ideation recently. She adamantly reported that she did not have a plan or intent, but that she was experiencing a great deal of stress related to final examinations, abstaining from substance use, and familial and marital conflicts and wondered what it would be like to “just not wake up.” Strategies for managing stress were elicited from Amelia. Specific activities named included cross-stitching, reading, exercising, eating healthfully, and talking with someone when she felt overwhelmed.
Consistent with her personal goals, Amelia did not purchase marijuana, transport it, purchase paraphernalia, or use more than she intended. At this time, it became clear that although Amelia was reducing her marijuana use, her alcohol use gradually increased. Amelia was asked to begin tracking her alcohol use on a daily basis as well. Specific goals related to alcohol management were also addressed (e.g., staying below a 0.06 BAC). Amelia was given a personalized BAC estimation card with instruction on the proper use. Amelia practiced identifying combinations of numbers of drinks over varying time periods that yielded a BAC of 0.06 or below.
Amelia reported a lapse after seeking medical treatment for stomach pain. She reported taking double the dosage of prescribed narcotic pain relievers per 6 hr and splitting a bottle of wine with her husband while consuming the pills. Amelia was provided education on the dangers of mixing opiates and alcohol, and she agreed that she would not use them together again. Amelia expressed feeling shame and embarrassment related to her lapse, which was processed. That is, the lapse was analyzed by having Amelia identify and respond to environmental and emotional characteristics of the given situation that were potentially associated with her lapse. Backward examination also occurred, which involved examining lifestyle factors that increase her exposure to this and other high-risk situations. Finally, strategies to target weaknesses were discussed and planned for to reduce future risk (see Larimer, Palmer, & Marlatt, 1999).
Amelia visited family in Alabama over Winter Break. Because many family members misuse substances, planning for family situations that may serve as triggers occurred. Amelia also briefly discussed that she and her husband were considering a divorce at this time. Although she previously reported that she felt supported and unconditionally loved, she said that she was unhappy with the way her husband treated her (e.g., calling her names, not prioritizing their relationship, engaging in explosive arguments, etc.). Subequent to the holiday break, she reported that after her husband refused to participate in couple’s counseling or other methods to improve their relationship, she decided to proceed with a divorce. Planning for her conversation with her husband and troubleshooting possible outcomes were discussed.
General Outline for Phase 3
Each session followed an abbreviated version of the session format outlined in Phase 2. The session then shifted to DBT. Skills homework was reviewed and discussed. Troubleshooting and planning for the following week took place. Finally, new DBT material was introduced and homework was assigned. DBT material followed the sequence and schedule suggested by the manual. Each sub-phase covered all module material presented in the manual.
It is noteworthy that no specific controlled drinking intervention was used in its entirety because much of the information and exercises overlap with RP and/or MI. Instead, interventions were loosely based on portions of “Responsible Drinking: A Moderation Management Approach for Problem Drinkers” by Rotgers, Kern, and Hoelzel (2002).
Phase 3.1: DBT (Mindfulness), MI/RP as needed (Sessions 8-13)
Specific strategies discussed included spacing drinks, alternating with a non-alcoholic beverage, counting number of drinks, setting a limit on the number of drinks, and deciding on a designated driver before beginning. Amelia’s conflicting reports (e.g., saying she does not want to smoke marijuana any more but reporting smoking approximately three occasions per week on her tracking sheet) were processed and explored.
Amelia acknowledged what she considers a “slip” (i.e., “snowballing” from occasional use to all day, every day for 3 days). Amelia exhibited a good degree of insight, in that she concluded that she is simply unable to moderate her use in accordance with her personal goals. Amelia revised her goal to abstinences from all forms of marijuana.
An introduction to DBT Core Mindfulness skills including rationale and basic introduction to the concept was administered. Amelia reported success with most aspects of mindfulness with the exception of continuing to struggle with not judging many of her thoughts. An exercise of simply mentally sorting thoughts into labeled “bins” (e.g., “thoughts about myself,” “emotions,” “thoughts about others”) was introduced to reduce the urge to pass judgment.
Amelia reported an improvement in her attendance of classes and completion of homework and studying.
Phase 3.2: DBT (Interpersonal Effectiveness), MI/RP as needed (Sessions 14-18)
Amelia began tracking substance use on her phone during this phase. She reported that she liked the method and that she found it less aversive and reported a higher confidence in her ability to comply with tracking.
Amelia lapsed twice during this phase, purchasing her own marijuana and smoking for 4 consecutive days on one occasion and for 2 consecutive days the following week. The majority of the proceeding sessions were spent engaging in a cost-benefit analysis regarding her continued marijuana use. After affirming that her goal was abstinence, discussion of more serious boundary setting, asking for help and support in her relationships, and eliminating or changing other relationships occurred.
A goal was set for a small, 1-week abstinence period to re-build Amelia’s sense of self-efficacy with regard to abstinence. Amelia was ultimately successful in achieving this goal and she began setting successively longer periods to abstain. Amelia reported feeling very strong and accomplished following this exercise, noting that she had not craved marijuana as she had previously.
Core Mindfulness skills were reviewed and bolstered briefly before Interpersonal Effectiveness (IPE) skills were administered. Amelia was introduced to the concept of IPE skills and the three type of effectiveness: getting what she needs, maintaining her self-respect, and maintaining the relationship. We discussed her experience with maintaining the three goals within her interactions and also discussed that depending on the interaction, different goals may be prioritized. Amelia identified that feeling stressed or sleepy made her more likely to be less effective. Amelia discussed cheerleading statements which she found helpful (i.e., “It is okay to ask for help; it does not mean I am weak.”). Determining the appropriate intensity of saying no and/or making requests was also discussed. Amelia reported that she had practiced a great deal, while communicating with her estranged husband about breaking their apartment lease. More skillful responses were elicited and reinforced when relevant. Amelia committed to behavioral rehearsal of at least one new skill per day. Coordinating homework worksheets were given each week.
Amelia engaged in increased self-care. A goal was set for spending 30 min each day to do something she enjoyed (e.g., reading, writing, running). She met that goal and reported a tremendous decrease in stress, despite the approach of final exams and her pending move.
Phase 3.3: DBT (Emotion Regulation), MI/RP as needed (Sessions 19-23)
Amelia abstained from smoking marijuana successfully for much of this phase. She gradually reduced her drinking from five to seven occasions per week to two to three occasions per week. She reported that she was trying to not use alcohol as a coping tactic and rather only in social situations. On one occasion, she reported that she made the “conscious decision to cope poorly” before beginning to drink and consumed alcohol to an estimated BAC of 0.18. Although this BAC is associated with high risk, this represented a shift because in the past, Amelia did not recognize she was coping with emotions poorly until several days after the event. She also arranged to have a designated driver and chose to drink when she did not have to work the following day, so she assessed the situation as “being more responsible.”
Amelia initially did not engage in self-care as planned. She moved out of the apartment she shared with her estranged husband and was experiencing feelings of failure and grief. She was also asked to detail emotionally charged experiences when filing a claim for Veteran Affairs benefits. She reported dealing with the related emotions for the first time as she typically used substances to cope and “stuff them down.” A goal was set to return to her previous successful pattern of self-care. Despite the fact that she had not been coping well, she did not use marijuana except for two occasions during this phase of treatment. After the first 2 weeks of this module, Amelia returned to engaging in self-care and reported an overall sense of well-being and satisfaction.
Emotion Regulation was administered and time was spent discussing the purpose of emotions, the difference between primary and secondary emotions, the difference between emotional reactions to the environment and the self, challenging myths about emotions, increasing positive emotions, letting go of emotional suffering, and acting oppositely.
Phase 3.4: DBT (Distress Tolerance), MI/RP as Needed (Sessions 24-27)
Throughout the course of this module (five sessions) Amelia smoked marijuana on two occasions. Although she was upset that she violated her goal of abstaining, she was pleased that she took only one hit and did not use again, despite being offered. She drank alcohol an average of 2.5 times per week, which was within her moderation goal (2 to 3 times per week). Although she drank to intoxication on several occasions, her peak BAC for the module was 0.15 and her mean BAC was at or below 0.08 every other week. She also reported diminished cravings and urges.
Amelia ended a 3-month dating relationship immediately before the third session of this module. She realized that despite him verbalizing that he wanted to support her, he acted in direct opposition to his promises. A plan for structuring her increased free time in a positive manner with focus on achieving her goals was made.
Following a brief orientation to the Distress Tolerance module, the final phase of DBT, brief planning for treatment termination was discussed. The four main categories of Distress Tolerance were discussed: Distraction, Self-Soothing, Improving the Moment, and Evaluating Pros and Cons. Radical Acceptance and the difference between Willingness and Willfulness were also discussed.
Amelia reported that she continued engaging in self-care activities and maintained her sense of successful emotional regulation and overall well-being.
Treatment was terminated at this time for two reasons: First, Amelia achieved her goals of abstaining from marijuana use and moderating her alcohol use. She was also comfortable with her decreased levels of anxiety and satisfied with other important factors in her life such as enrollment in graduate school and adopting appropriate self-care activities. She also reported confidence in her ability to maintain these skills and was comfortable with the idea of returning to treatment in the event of any changes. Second, Amelia completely worked through the DBT manual and reported confidence in her ability to continue to implement her skills.
8 Complicating Factors
Little is known about synthetic marijuana from empirical research. Although a summary of the extant literature was provided earlier in the present article, a complete understanding of effects and possible side effects of synthetic substances has yet to be elucidated. Poison control center data, crisis intake facilities, and hospitals have provided what experience they have had with persons under the influence of synthetic marijuana, but there is still much to be learned. However, because the formulation and effects of the drug are so similar to marijuana, the assumption that abuse of the synthetic version be treated similarly to non-synthetic marijuana is the best guideline we have.
Amelia also had a combination of Cluster B traits. Although she did not meet the criteria for Borderline Personality Disorder, she endorsed engaging in “black and white thinking,” engaging in impulsive behavior, and being emotionally labile particularly in the context of romantic relationships. These traits were directly contributing to her substance use and thus were addressed with DBT.
At the time of treatment, Amelia was in a dysfunctional marriage. Frequent screaming matches, verbal abuse and belittling, and inter-familial difficulties occurred on a near daily basis. Amelia’s tumultuous environment made it difficult for her to begin her recovery in a supportive setting and served as additional stressors for Amelia to manage. Also of significance, Amelia reported suspecting that her husband “had a problem” with alcohol. She indicated that her husband would become angry with her for using synthetic marijuana but encouraged their mutual overuse of alcohol, further complicating treatment efforts.
Finally, compliance with tracking sheets can be difficult to ensure. After Amelia did not bring her tracking sheet to the session for several weeks, together the clinician and client strategized to track her substance use electronically. Amelia set up a form on her phone via a file hosting service that offers cloud storage and file synchronization across several devices. A password-protected spreadsheet was created by the client and hosted in the cloud, so that it was accessible on both her smartphone and laptop. She updated her use data on a daily basis. The clinician could view the updates in real time. Row numbers 1-7 corresponded with Sunday-Saturday. In the cell next to the row number, she entered a code that indicated the time she began drinking, maintained a running tally of drinks consumed or marijuana smoked, and the time she finished. Amelia used an “X” to indicate alcoholic beverages and an “O” to indicate smoking marijuana (e.g., “7XXXXXX12” in row 2 indicated that she recorded for Monday, began at 7:00, and consumed six standard drinks until 12:00). Amelia designed this method based on what made sense for her and to maximize privacy. If anyone were to circumvent double password protection (i.e., the application password and document password) and access the file, they would have no way of identifying what the characters meant. Amelia reported less aversion to tracking her use as well as increased personal benefit (because she was updating daily and often in real time, allowing her to monitor herself, rather than filling it out post hoc).
After observed success of tracking in the cloud, Amelia also sought out a smartphone application called “DBT.” The app provides a space for the client to log emotions experienced and skills used on a daily basis. The app also features a “coaching” section where all acronyms and skills are stored and explained should the client forget what to do in a particularly emotional exchange or when practicing a newly learned skill. The app also has an option to automatically e-mail encrypted diary cards to the therapist. Amelia very much enjoyed the app, which costs US$7.00. She reported that the reference/coaching sections were helpful during weekly practice and that she liked the ease of simply checking off skills used and emotions experienced rather than keeping up with a paper-and-pencil alternative.
9 Access and Barriers to Care
Amelia was treated at a reduced-cost student training clinic. As such, there were no managed care considerations. The cost of services was modest as cost at the clinic is calculated on a sliding scale basis (i.e., US$5 per session for Amelia). Also of relevance to the absence of managed care, Amelia was able to continue with services for as long as necessary.
While access to modern technologies such as a smartphone benefitted Amelia (by using an application for DBT diary cards and tracking her substance use on a shared document), both DBT and substance monitoring cards have been effective with paper-and-pencil methods for decades.
10 Follow-Up
One month after treatment termination, Amelia reported that she continued to maintain abstinence from all types of marijuana. She also reported that she consumed alcohol on less than six occasions during the past month, did not drink to intoxication, and used learned strategies to reduce the risk. Amelia also reported that she was admitted to graduate school and was busily planning for the new school year.
Although Amelia did not present to the clinic for a formal follow-up session at 5 months post-treatment termination due to relocation for graduate school, she contacted the clinician to inform her that she still had not consumed marijuana, was rarely drinking alcohol (weekly or less), quit smoking cigarettes, and was not experiencing any impairment or difficulty related to depression or anxiety symptoms.
11 Treatment Implications of the Case
The present report details the successful treatment of substance use dependence using a unique approach that united MI/RP and DBT. This is a unique case, in that the extant literature does not contain empirical studies that treat a substance use disorder with DBT in an individual who does not also have Borderline Personality Disorder. However, controlled trials have supported the efficacy of DBT adapted for substance use disorders (Dimeff & Linehan, 2008).
Amelia’s BDI-II and BAI scores (Figure 1) decreased from 29 and 28, respectively (falling within the severe range), to 1 and 3 (minimal range). Her first 2 weeks of substance use monitoring revealed 133 and 57 instances of synthetic marijuana use per week with her daily peak usage in the 20 to 30 range. Amelia used marijuana on three occasions in the last 12 weeks of treatment. Although Amelia has demonstrated very large reductions in marijuana use, she continues to make progress in the moderation of her alcohol use. Figure 2 displays Amelia’s synthetic marijuana use change over time. It is noteworthy that for the first 14 weeks of treatment (and prior to presenting for treatment), Amelia used synthetic marijuana exclusively. After this period of time, she used primarily non-synthetic marijuana as a shift in peer group after separating from her husband resulted in marijuana present at social functions. Amelia also preferred to purchase marijuana because she could not charge it to her credit cards as she did while purchasing synthetic marijuana (which resulted in significant delinquent debt). Amelia met her goal of not drinking on more than three occasions per week for the last 5 weeks of treatment. In addition, her mean BAC was at or below 0.08 for 7 of the last 8 weeks of treatment. Her CUDIT score prior to treatment was 25, which decreased to 9. The score is still partially inflated by earning 4 points for making an attempt to quit within the last 6 months.
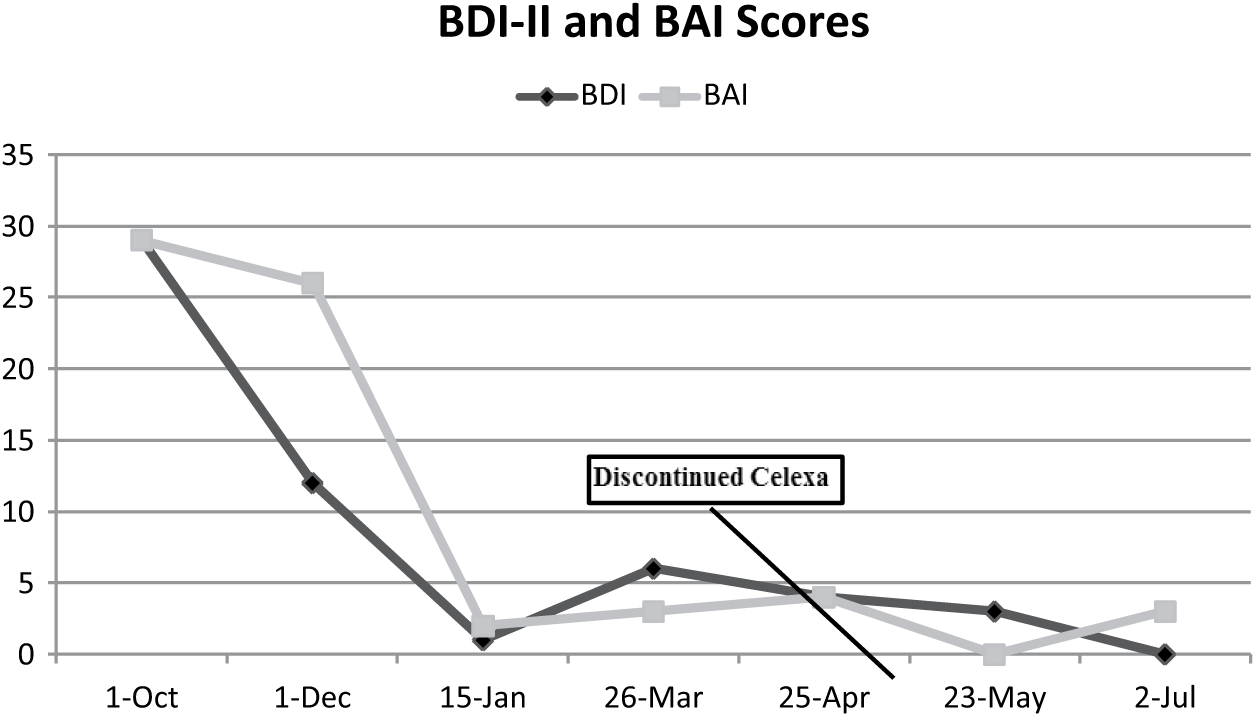
BDI-II and BAI scores by month.
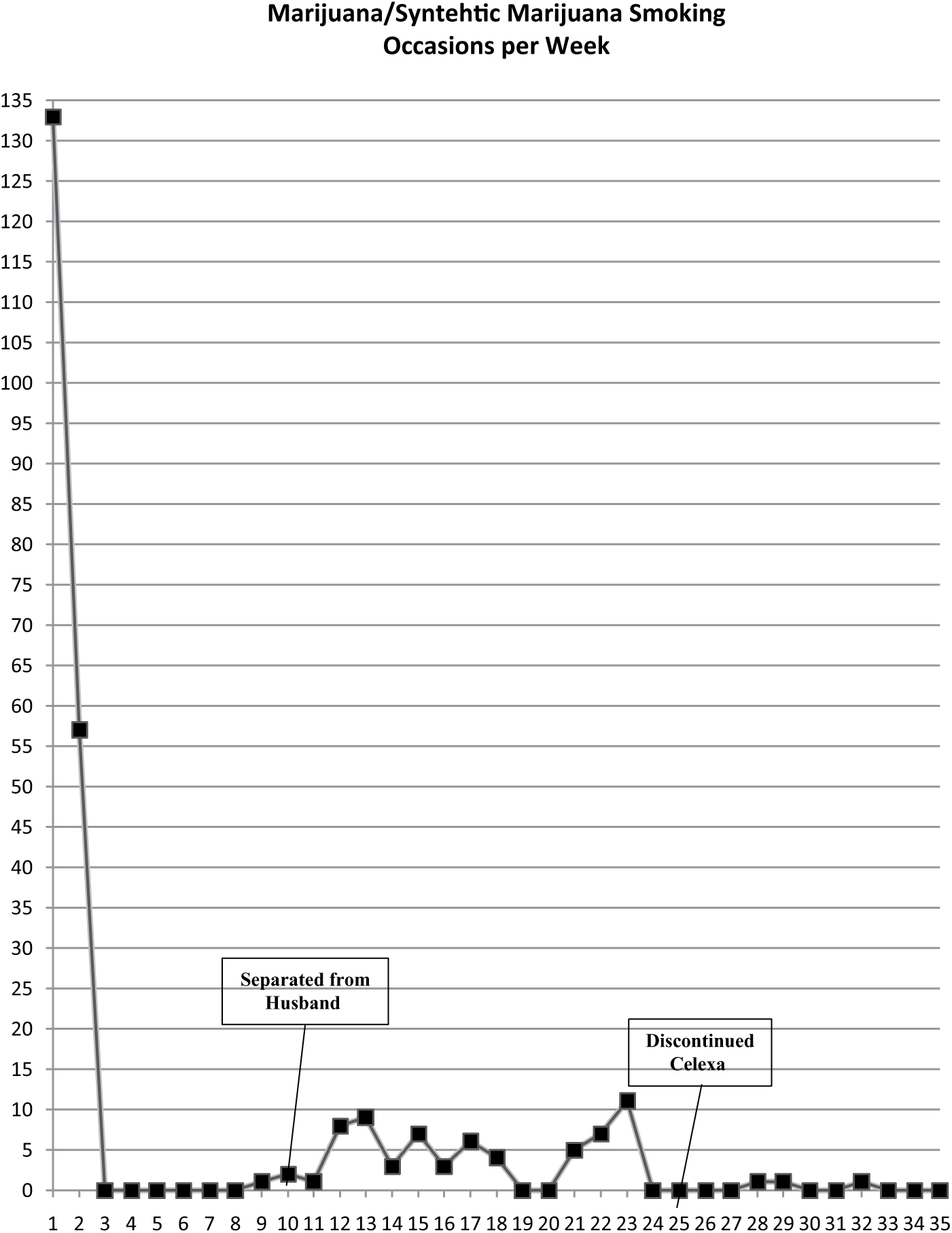
Instances of smoking marijuana/synthetic marijuana per week in treatment.
When Amelia began treatment, she was experiencing marital difficulties with her husband, occupational impairment (suspended for a week due to calling out to cope with the after-effects of staying awake to smoke all night), educational impairment (failing three of her four classes), and physical and cognitive health issues (e.g., coughing up black phlegm; feeling “winded” easily; suffering from frequent upper respiratory infections; difficulties with memory, attention, and sleep). Amelia has since filed for separation from her husband, did not call out of work to recover from after-effects of substance use, and earned a 3.0 GPA for the most recent academic semester. She passed the exam to earn a temporary teaching certificate and is currently attending a graduate program that will earn her a full certificate. She reported an overall improved physical health, most notably the absence of discharge when she coughs and self-reported improved memory, attention, and sleep. Amelia is also no longer taking psychoactive medications, as she discontinued use of Celexa during Week 25 of treatment.
Although this report demonstrated an individual who was successful in reducing substance use and improving several areas of her life, it is not without limitations. First, Amelia is exceptionally intelligent and insightful. As the daughter of a yoga teacher, she was aware of, and knew how to engage in, mindfulness and meditation prior to the onset of treatment. Therefore, Amelia may have taken to DBT easier than the average adult.
Second, this protocol was administered in a training clinic. Amelia was able to participate in services on a sliding scale fee, which relieved some potential barriers to treatment. In addition, because Amelia was a student, she often traveled out of town during semester breaks. Although full sessions were not held, coaching and check-ins were conducted via telephone. Finally, although geographic restriction prevented a formal extended follow-up period, Amelia reported continued success at 5 months post-treatment; a lack of formal follow-up data may be viewed as a limitation.
This case also has implications for incorporating modern technology into therapeutic interventions. Amelia began tracking her substance use electronically (predominantly via smartphone) about halfway through treatment and her compliance improved greatly. Amelia also reported that using the DBT smartphone application empowered her and motivated her to keep practicing and set goals to challenge herself beyond the therapy room. Clinicians should work with their clients to explore their comfort using technology such as smartphone apps to better track progress and improve treatment generalizability and outcomes.
12 Recommendations to Clinicians and Students
When assessing someone who presents with a substance use disorder, it is absolutely imperative to conduct a functional analysis of the substance use behavior. In the present case, it informed treatment in that it became apparent to both the client and the clinician that the client was using substances to cope with strong emotions. Upon further exploration, the client indicated that she did not know how to cope with emotions in a healthy way. DBT was a natural fit for the client because it taught her how to regulate emotions, while also teaching her to communicate and behave in interpersonally appropriate ways all while being mindful and non-judgmental of herself and her thoughts. Eventually the skills she learned replaced her substance abuse.
Relatedly, when treating someone for substance use, it is important to regularly monitor and assess for “substance substitution.” In this case, it became evident that as Amelia decreased her synthetic marijuana use, her alcohol use increased. Clinicians and students should be diligent about this potential problem and intervene when necessary.
Lapse and relapse are very common among marijuana-dependent patients. Marijuana lapse and relapse (4 or more days of use per week) rates are estimated at approximately 60% to 70% in those who achieved a minimum period of 2 weeks abstinence (Moore & Budney, 2003). Thus, consistent with frameworks of MI and RP, clinicians should be careful to monitor for lapses/relapses yet remain without judgment. Planning focused on preventing lapses from progressing to relapses should occur.
Finally, leveraging technology to improve treatment outcomes is a burgeoning area of study in the field. Clinicians and students should carefully evaluate the potential role of technology in treatment and carefully consider relevant ethical and confidentiality issues. When used appropriately, technology can increase compliance, self-efficacy, and “buy-in” to homework tasks. Be willing to try new modalities of record and discuss what works for the client in the context of technology that they have available to them.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.