
Abstract
Sleep medication is the most common treatment for insomnia in older adults. However, prolonged use of hypnotics has several negative side-effects and can lead to a pattern of tolerance and dependence. Recent research has found promising results for interventions that included both supervised gradual medication withdrawal and cognitive behavior therapy (CBT) for the treatment of hypnotic-dependent insomnia. Furthermore, there is increasing evidence that incorporating mindfulness meditation can result in a more potent CBT intervention for insomnia. In this article, the authors describe and discuss the effects of a broadly focused intervention for treating hypnotic-dependent insomnia in an older adult. The treatment simultaneously targets insomnia symptoms, comorbid symptoms such as pain, dependency issues, and the discontinuation of hypnotic medication.
Keywords
1 Theoretical and Research Basis for Treatment
Insomnia or subjective complaints of poor sleep accompanied by impairment of daytime functioning are common among older adults aged 60 to 65 years and above (Morin et al., 2004). It has been estimated that between 25% and 50% of the elderly population report sleep problems (Benca, Ancoli-Israel, & Moldofsky, 2004). Insomnia has been found to predict depression in older people, and it can affect daily functioning and quality of life (Avidan, 2003; Cole & Dendukuri, 2003; Ohayon, 2002). Many of the chronic diseases that older persons suffer from often cause pain and have a negative effect on sleep (Garcia, 2008; Waters, Woodward, & Keefe, 2005). Thus, sleep problems, pain, and depressive symptoms appear to mutually exacerbate one another (Benca et al., 2004). Moreover, older adults have a high rate of hypnotic drug use compared with younger adults (Morin et al., 2004). Continuous use of sleep medication has a number of negative side-effects that are particularly harmful in older adults and that can lead to a pattern of tolerance and dependency (Gould, Coulson, Patel, Highton-Williamson, & Howard, 2014). Common side-effects include an increased risk of falls, injuries, and traffic accidents, as well as cognitive impairment and altered sleep physiology (Gould et al., 2014; Morin et al., 2004). Insomnia and continuous use of sedative hypnotic drugs can thus lead to significant individual suffering and economic costs due to increased utilization of health care services (Dalrymple, Fiorentino, Politi, & Posner, 2010; Morin et al., 2004).
Several studies have documented that older adults with insomnia benefit from interventions based on cognitive behavior therapy (CBT; Irwin, Cole, & Nicassio, 2006; Montgomery & Dennis, 2003; Sivertsen et al., 2006). There is also increasing evidence that older adults with long-term use of hypnotics and benzodiazepines for the treatment of sleep problems benefit from interventions that include both supervised drug withdrawal and psychotherapy (Lichstein, 2006; Morin et al., 2004). It is underlined that a medication tapering regimen based on gradual reduction, combined with CBT specifically targeting insomnia symptoms is essential in the initial discontinuation phase to reduce withdrawal symptoms (Morin et al., 2004). CBT for insomnia (CBT-I) consists of various behavioral components such as sleep restriction, stimulus control, and relaxation training, as well as cognitive components such as sleep education and cognitive restructuring (Morin et al., 2004). In a recent meta-analysis, Gould and co-workers suggest that the key mechanism of change might be to target underlying pathology, such as insomnia, rather than dependency and withdrawal issues (Gould et al., 2014).
Combining mindfulness meditation with CBT to improve sleep has also shown promising results in both younger and older adults (Ong, Shapiro, & Manber, 2008). In a treatment-development study, Ong and co-workers found that a combination of mindfulness meditation and CBT-I was associated with reduction in both sleep and sleep-related arousal (Ong et al., 2008). A challenge is how to combine two seemingly opposed therapy goals, that is, symptom reduction versus the development of a more flexible behavior repertoire (Lau & McMain, 2005). However, it has been argued that incorporating mindfulness meditation could result in a more potent CBT intervention for insomnia by targeting both arousal and nocturnal wakefulness (Ong et al., 2008). Arousal has been identified as a contributory factor in the development and maintenance of insomnia (Ong et al., 2008; Ong, Ulmer, & Manber, 2012). It has been hypothesized that insomniacs are not necessarily sleep deprived but rather that they are hyperaroused and therefore unable to fall asleep (Bonnet & Arand, 1998; Stepanski, Zorick, & Roehrs, 1988). Mindfulness meditation targets the process of letting go and the willingness to let thoughts, experiences, and sensations be as they are in the present moment, whether pleasant or unpleasant, and neither change them nor act on them (Baer & Krietemeyer, 2006). Mindfulness and acceptance-based interventions for insomnia thereby help the person concerned to increase his or her awareness of the mental and physical states that arise when experiencing insomnia symptoms and to respond to these symptoms in more adaptive ways (Ong et al., 2012). Furthermore, an increasing number of studies have documented that mindfulness interventions are effective in treating addictive behavior and substance use and misuse, as well as chronic pain conditions (Chiesa & Serreti, 2014; Veehof, Oskam, Schreus, & Bohlmeijer, 2011).
Against this background, the purpose of the current case study is to describe and show the feasibility of a broadly focused intervention targeting both the medication dependence as well as the underlying symptomatology of insomnia, pain, and worrying in an older adult. To our knowledge, this is the first study that combines mindfulness meditation with CBT and gradual supervised medication taper for hypnotic-dependent insomnia. Strength of the study is the supplement of motivational interviewing (MI; Rollnick, Miller, & Butler, 2008) in the initial phase of the treatment. In a recent article by Kyle and co-workers, MI has been recommended as a supplementary component in CBT for insomnia (Kyle, Crawford, & Espie, 2013).
2 Case Introduction
“Hanna” was a 63-year-old married woman who was referred to an outpatient clinic at a specialist drug-treatment service unit for treatment of her prolonged use of prescribed sedative hypnotic medication. Hanna was working part-time (3 days a week) as an accountant in a company selling kitchen decor. She liked her work very much, and despite her sleep problems, she had seldom been absent from work apart from during the past year, when she had been absent for shorter periods of sick leave.
Hanna and her husband had one child, a son. Hanna also had a daughter from a former marriage and two grandchildren. Hanna described her relationship with her husband and children as good.
3 Presenting Complaints
When Hanna presented for treatment, she stated that she needed help with two issues: reducing and stopping her hypnotic drug use and improving her sleep. At the same time, she admitted that she felt ambivalent about discontinuing the medication. After all, she had found that the medication had helped her to sleep. Hanna had started taking sleep medication on a regular basis 20 years previously, when her mother died of cancer after being ill for several years. Hanna had been the main caregiver during her mother’s terminal illness, and she developed sleeping problems. She had tried to discontinue her medication on several occasions, but she had relapsed each time after a relatively short period. Five years back, Hanna had been referred to some kind of behavioral treatment consisting of sleep education and a sleep restriction regimen. She had failed to follow the regimen and dropped out of treatment after a short time. Hanna’s sleep complaints consisted of problems initiating sleep the night before a work day, as well as frequent awakenings during the night despite taking hypnotic medication. She occasionally experienced poor daytime functioning. She had no specific system with regard to bedtime hours, but she usually went to bed before midnight if she was going to work the next day. On weekends, she spent longer time in bed hoping to regain the sleep she had lost during the week. Her average use of sleep medication was 12.5 mg Zopiclone 5 nights a week. She tried not to take medication on Fridays and Saturdays, only when she felt she needed to. In the evening, she drank coffee and smoked two cigarettes, a habit she had developed when caring for her mother. She was not aware that both caffeine and nicotine are stimulants that make it difficult to induce sleep. She took her medication approximately 15 min before going to bed. Hanna reported that, on average, it took 45 min to fall asleep. She reported tension and symptoms of unrest at bedtime most evenings, leading to more tension and fear of not falling asleep. Hanna had recently developed osteoarthritis of the knees, and she described a constant background pain that often intensified during the evening. The pain reinforced her tension at bedtime as well as her worries about not falling asleep. She used no prescription medication for her pain. Some nights when her knee was particularly painful, she lay awake for more than an hour despite her use of hypnotics. She occasionally took more medication than prescribed by her general practitioner (GP). She usually woke up 2 or 3 times a night, each awakening lasting for at least half an hour. Hanna usually drank a glass of milk or ate a piece of bread on the first awakening, hoping this would make her fall asleep again. On an average night, she thought she got a total of 5.5 to 6 hr of sleep. She usually woke up in the morning feeling drowsy and unrestored.
4 History
Hanna had been the youngest of three children in her family. Her two older brothers were 7 and 11 years her senior. They had both left home when Hanna was 12. Hanna recalled that, during her childhood, her mother suffered from insomnia, and that she started to use sleep medication on a regular basis when Hanna was in her early teens. Hanna related this to her father’s alcohol abuse. He was an excessive drinker for a period of 10 years. He eventually underwent a rehabilitation program and was abstinent until he died when Hanna was 25 years old. Hanna remembered that her mother occasionally offered her sleeping medication when Hanna had difficulty sleeping during her father’s drinking periods. It was not until her mother’s illness, however, that Hanna herself developed insomnia and became dependent on sleep medication. This period of her life was stressful, caring both for her young children and her seriously ill mother.
5 Assessment
Before starting treatment, Hanna had to report the exact daily doses of the hypnotic drug, and this was checked with the information from her GP. Hanna then underwent an assessment, including a self-report scale that measures insomnia, an anxiety and depression screen, an instrument assessing pain, and an instrument assessing the ability to be mindful in daily life. She was assessed using the same instruments on completing treatment, and after 6 months. In addition, a medication taper schedule was set up to monitor her gradual discontinuation of the hypnotic medication, and she had to report the status weekly. At the end of treatment, she filled in a questionnaire assessing her impression of global change. The instruments are described as follows.
Sleep Complaints
The Bergen Insomnia Scale (Pallesen et al., 2008) is a self-administered scale designed to measure insomnia. It contains six items. The first three items ask about sleep onset, maintenance, and early morning wakening. Items 4 to 6 refer to not feeling adequately rested, experiencing daytime impairment, and being dissatisfied with current sleep. Each item is rated on an 8-point scale, ranging from 0 to 7 days per week. The scores for each item are added together to produce a total composite score ranging from 0 to 42. The Bergen Insomnia Scale has been found to have good psychometric properties (Pallesen et al., 2008).
Symptoms of Anxiety and Depression
The Hospital Anxiety and Depression Scale (HAD; Zigmond & Snaith, 1983) is a self-report measure with 14 items, of which 7 measure non-vegetative symptoms of anxiety and 7 non-vegetative symptoms of depression. Each item is scored on a 4-point scale (0-3); a high score indicates more severe problems. The scale has good psychometric properties (Bjelland, Dahl, Haug, & Neckelmann, 2002).
Pain Experience
Pain intensity was measured using the Visual Analogue scale (VAS) and the present pain intensity (PPI) measure in the Short-Form McGill Pain Questionnaire (SF-MPQ; Melzack, 1987). PPI consists of verbal descriptors that yield an overall intensity score on a vertical 6-point scale ranging from no pain (0) to unbearable pain (5). VAS assesses pain intensity on a 10 cm horizontal VAS ranging from no pain (left) to worst possible pain (right).
PPI and VAS have demonstrated acceptable psychometric properties and feasibility in older adults (Herr, 2005).
Mindfulness
The Five Factor Mindfulness Questionnaire (FFMQ; Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006) is a self-report instrument measuring a general tendency to be mindful in everyday life. It consists of five facets or subscales containing a total of 39 items describing the ability to respond mindfully: (a) be aware of inner experiences as well as one’s surroundings (observe), (b) put inner experiences into words (describe), (c) act with full awareness and presence rather than in a distracted manner (act aware), (d) refrain from judging one’s experiences and instead relate to it with a stance of acceptance (non-judge), and (e) not react excessively to inner experience (non-react). Each item is scored on a 5-point Likert-type scale from “never or very rarely true” to “always or almost always true.” The FFMQ has been found to have acceptable psychometric properties for use in Norway (Dundas, Vøllestad, Binder, & Sivertsen, 2013).
Medication Tapering Schedule/Plan
An individualized step-by-step written plan (see Figure 2) describing the baseline intake of medication (frequency and quantity) and the systematic and gradual withdrawal and discontinuation of the medication during the course of treatment (Morin et al., 2004).
Patient Global Impression of Change
Patient global impression of change (PGIC; Farrar, Young, LaMoreaux, Werth, & Poole, 2001) is a 7-point ordinal scale used as a rough measure of clinically important change after treatment. A score of 4 means no change in the condition, while scores <4 indicate an improvement: 1 = very much improved, 2 = much improved, 3 = minimally improved, and >4 a worsening: 5 = minimally worse, 6 = much worse, 7 = very much worse, as judged by the patient.
6 Case Conceptualization
It became clear that Hanna’s problems were complex and that different factors such as insomnia symptoms, pain, and worrying, together with inappropriate sleep habits and use of hypnotics, had led her into a vicious cycle that maintained her problems. Comorbidity and multiple symptoms are not uncommon in older adults, and standard CBT conceptualization is often inadequate as a description of the complexity of age-specific issues (Laidlaw, Thompson, & Gallagher-Thompson, 2004). Laidlaw and co-workers have developed a comprehensive conceptualization framework of CBT with older adults (Laidlaw et al., 2004). In this framework, age-related issues such as physical health and intergenerational linkages are incorporated. To fully understand Hanna’s situation and the development of her symptoms, the therapist set up a conceptual framework (see Figure 1) based on Laidlaw and co-workers’ model (2004). Hanna’s story of coping with sleep-related stress by prolonged use of sleep medication had reinforced her psychological dependence on hypnotics. Hanna realized that she had somehow inherited her mother’s sleeping problems as well as her inappropriate use of sleep medication. Her knee pain that interfered with sleep reinforced her worries about not getting enough sleep. This negative reinforcement paradigm discouraged her and she felt inadequate and worried that her increased age and long-lasting problems would make her insomnia and hypnotic dependence difficult to treat.
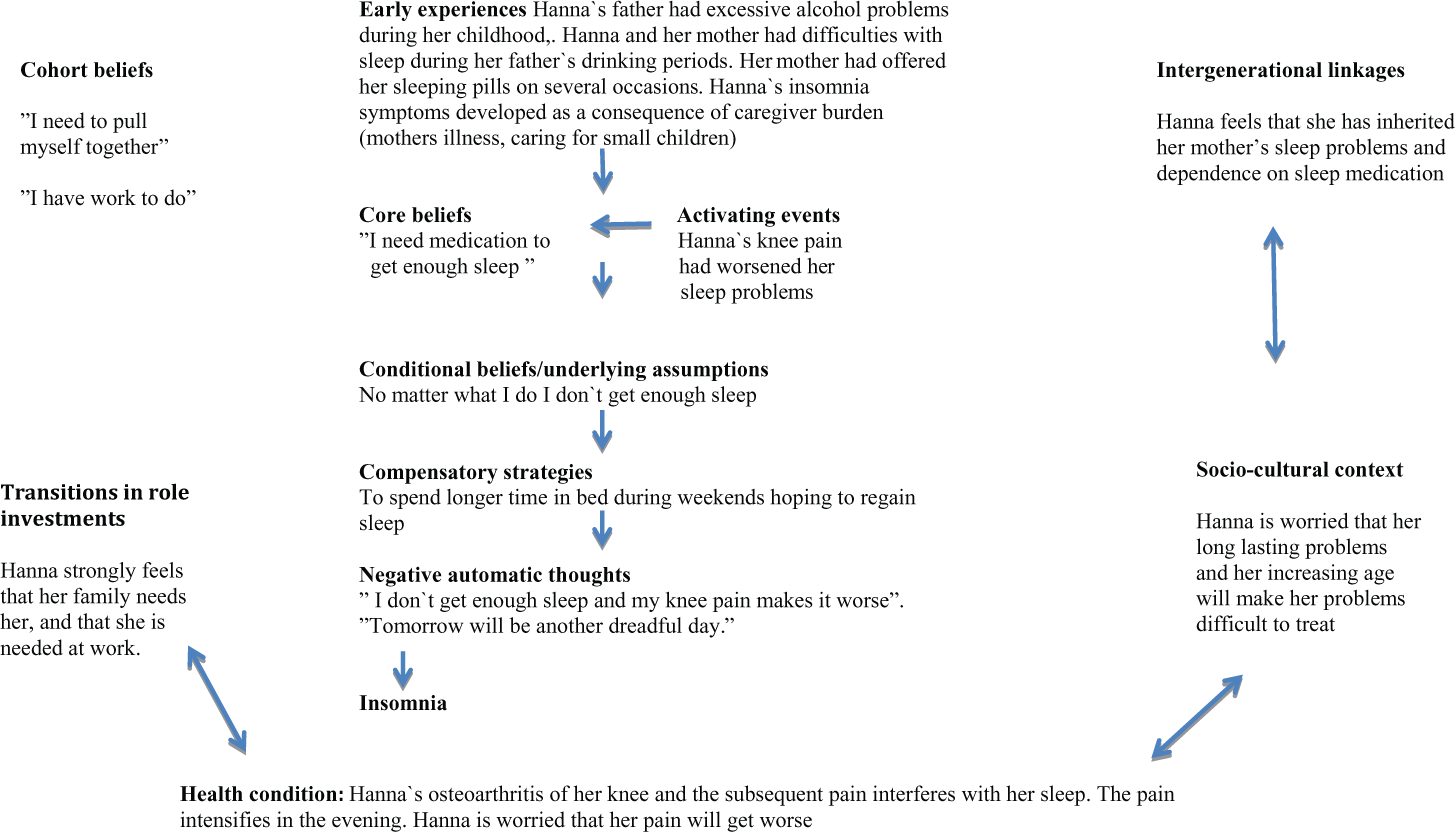
Conceptual framework.
7 Course of Treatment and Assessment of Progress
Course of Treatment
Hanna was offered a brief 10-session therapy, combining components from CBT-I (Morin, Bastien, & Savard, 2003) with mindfulness meditation and a systematic medication taper regimen. The cognitive behavioral components consisted of stimulus control instructions, sleep education, and cognitive restructuring (Lichstein et al., 2013). Ong and co-workers included sleep restriction, stimulus control, sleep education, and mindfulness meditation in their treatment-development study (Ong et al., 2008). In the present study, sleep restriction was omitted due to Hanna’s earlier negative experiences with this regimen. It has been pinpointed that implementation of sleep restriction should be flexible and adjusted to the patients’ acceptance and willingness to adhere to the regimen (Kyle et al., 2013; Morin et al., 2004). The treatment was conducted by an experienced clinical psychologist (the first author) at a specialist drug treatment outpatient clinic. In the initial phase, the therapist utilized principles from motivational interviewing (Rollnick et al., 2008) to address Hanna’s ambivalence to discontinuing her sleep medication. She was given psychoeducation about the process of change and the different stages that the patient goes through to become ready to change habits and behavior (Prochaska & DiClemente, 1984). It became clear that Hanna had already been through some of the stages prior to the start of treatment, and that she felt less ambivalent and was fairly motivated to start changing her behavior when treatment started.
After completing the baseline assessment, a psychiatrist at the clinic (the second author) provided consultation on the medication taper schedule and pharmacological psychoeducation on the effects and side-effects of Zopiclone. In cooperation with Hanna and the psychologist, he drew up a step-by-step withdrawal schedule, which Hanna was committed to following during the treatment period of 10 weeks (see Figure 2). The goal was to eliminate Zopiclone use by the 10th week of treatment. To stabilize her medication use, Hanna was encouraged to take Zopiclone at a fixed time, rather than on an as-needed basis, which meant that she had to take medication on Fridays through Sundays as well as on weekdays. First and foremost, the medication tapering schedule foresees that the intake of the medication will be restricted to specific hours and not be taken as needed. The rationale for stabilization has to be understood by the patient. Hanna was told that stabilization and gradual withdrawal of the hypnotic medication would minimize the negative withdrawal effects as well as breaking the habit of taking medication to alleviate unpleasant symptoms. According to Lichstein and co-workers (2013), research has not determined the characteristics of the optimal drug withdrawal schedule. In general, the specific dose reduction varies as a function of the patients’ motivation and readiness to discontinue the medication. Some researchers recommend reducing the dosage by approximately 25% per week (Morin et al., 2004).
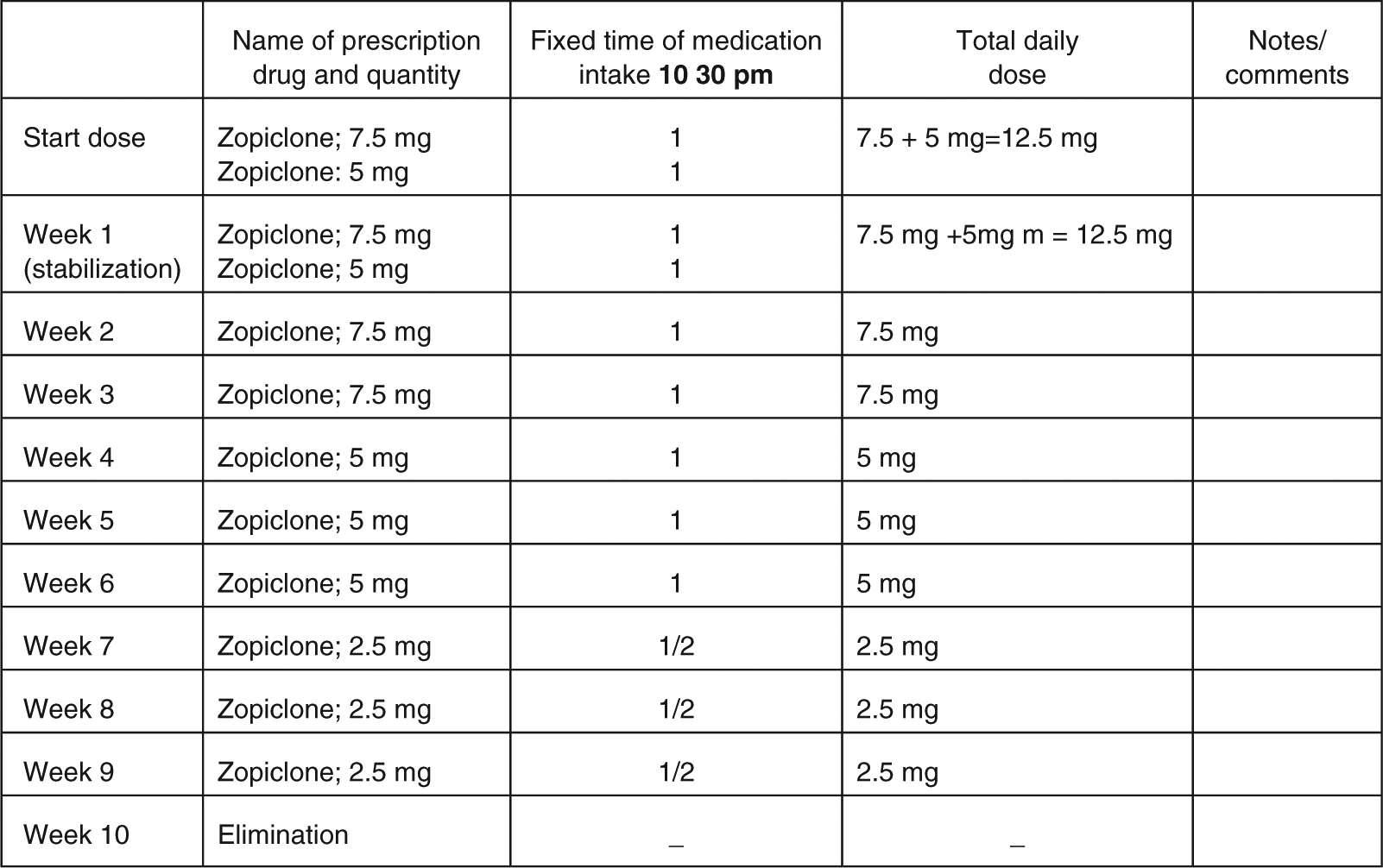
Step-by-step medication taper schedule.
When total cessation of the medication approaches, many patients will need to slow down the medication tapering. As a rule, the patient should seek to avoid a re-escalation, and extend the intervals instead. Hanna’s GP received a copy of the plan and was responsible for prescribing the drugs during the treatment period. At each session, Hanna had to bring along her copy of the plan and the status was recorded by the therapist. Adjustments and amendments of the plan were made in cooperation with the psychiatrist at the outpatient clinic. Weekly status reports concerning the withdrawal schedule, as well as regular encouragement, firm support, and repetition from the therapist, are essential parts of the treatment.
Therapy was given weekly, lasting 60 min per session. Each session was structured in four sections: (a) mindfulness exercise; (b) status report/review of medication taper and withdrawal symptoms, and review of homework from last session; (c) psychoeducation about sleep and how sleep problems, pain, and depressive symptoms exacerbate one another, the importance of breaking vicious cycles, and introduction and discussion of cognitive restructuring strategies and skills; and (d) homework assignment for the upcoming week. Hanna was given a notebook and a folder in which to keep the medication withdrawal plan, home practice, and in-session material. During the sessions, the therapist used a whiteboard to illustrate important points.
Hanna was introduced to mindfulness at the first treatment session. The mindfulness exercises are meant to help the patient break away from habitual reactions to the craving for drugs once the withdrawal schedule starts as well as targeting sleep-related stress and arousal and pain experience (Ong et al., 2012; Veehof et al., 2011). The exercises help the patient to expose himself or herself to different symptoms rather than avoid discomfort. At the same time, they are also intended to enable the patient to experience how systematic training in mindfulness can enhance awareness of momentary personal choices and actions (Lau & McMain, 2005). The guided mindfulness exercises consisted of two of the exercises used in Mindfulness Based Stress Reduction (MBSR; Kabat-Zinn, Lipworth, & Burney, 1985): sitting meditation and body scan. The exercises were shortened and lasted for about 15 to 20 min. The therapist guided Hanna through one of the exercises each therapy session, and Hanna was encouraged to practice on a daily basis between sessions, at least for 15 min. In addition, Hanna was introduced to different mindfulness exercises taken from Acceptance and Commitment Therapy (ACT; Hayes, Strosahl, & Wilson, 1999). One of these exercises focused on breathing, and Hanna was taught to practice the exercise at bedtime to reduce sleep-related stress and arousal. She was instructed to observe and notice her breathing in a non-judgmental way, without trying to change it (Dahl, Wilson, Luciano, & Hayes, 2005). Hanna reported that, at bedtime, the exercise helped her shift her attention away from thoughts about not going to sleep and worries about the next day. This exercise was supplemented by another exercise in which Hanna was taught to envisage thoughts as leaves floating in a stream (Hayes et al., 1999). These exercises became particularly important to her as cessation of the medication approached during the middle to final phase of the treatment (Sessions 6-10).
After a week of stabilization of the medication at a fixed time, 10:30 p.m., Hanna was ready to reduce Zopiclone from a dose of 12.5 mg per night to 7.5 mg per night during the next 2 weeks. She was given information about common withdrawal symptoms and told to monitor them on a regular basis by writing in her notebook. She was given psychoeducation about normal sleep and aging, and was introduced to sleep hygiene principles concerning the effects of caffeine, alcohol, and exercise on sleep. Stimulus control consisted of the following instructions: (a) Go to bed and get up at the same time every night and morning. (b) Do not stay in bed if awake for more than 15 min. (c) Return to bed only when feeling sleepy again. (d) Avoid canceling activities and appointments the day after a sleepless night. The rationale for establishing new sleep habits was underlined. Hanna was made aware that compensating strategies such as spending more time in bed during weekends to regain sleep contributes to maintaining insomnia symptoms. In the first homework assignment, Hanna was asked to set herself goals for what she wanted to achieve during the treatment and to make the goals as concrete and attainable as possible.
At the second session, Hanna reported that she was following the medication withdrawal plan, and that she had no withdrawal symptoms so far. When reviewing the homework assignment, she announced that her main goals, besides discontinuation of hypnotic medication, were to establish new sleep habits and to change her mental attitude to sleep. She acknowledged that her prolonged use of sleep medication had led her into a vicious cycle and that her dependence on hypnotic medication contributed to reinforcing her insomnia. The therapist illustrated this by drawing Hanna’s vicious cycle on the whiteboard (see Fig 3).
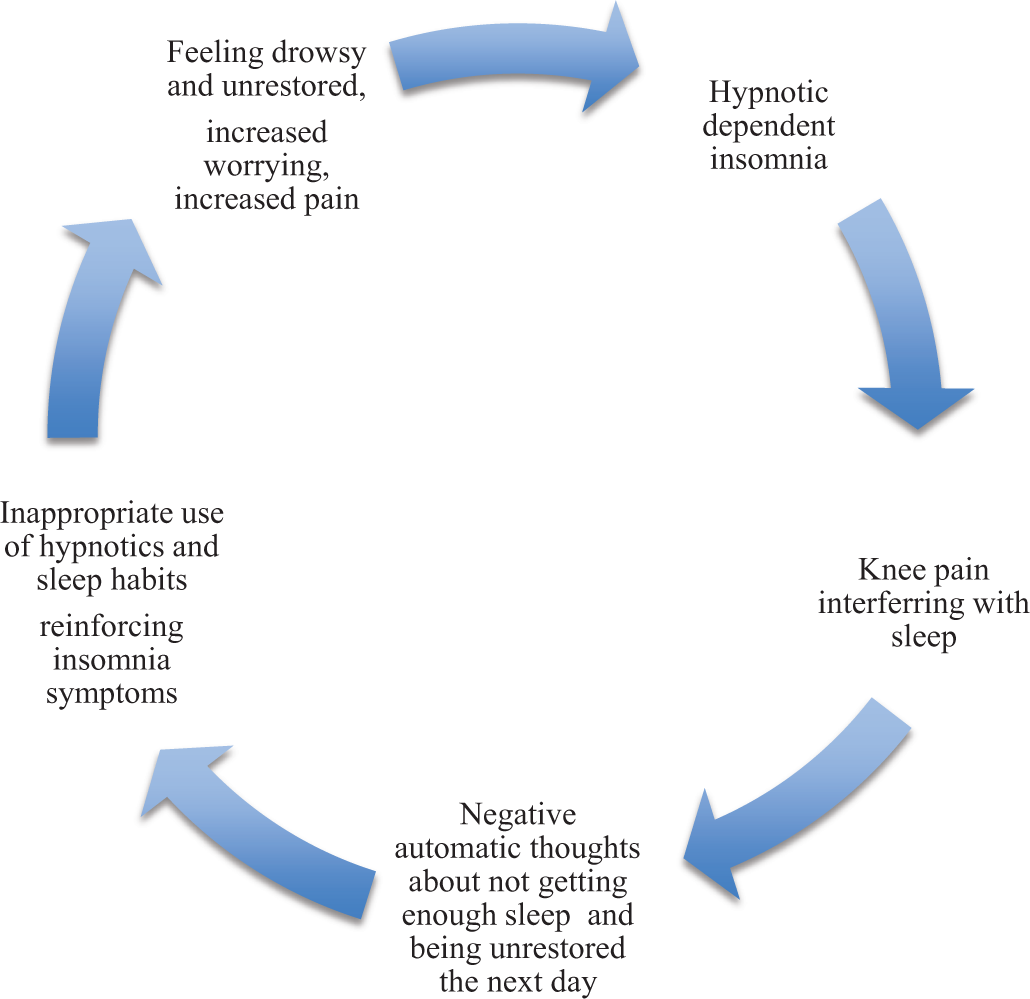
Hanna’s vicious cycle.
In the homework assignment for the third session, Hanna was asked to reflect on her struggle with sleep and her efforts to solve her sleep problems, and to suggest ways of establishing better sleep habits based on general sleep hygiene principles.
At the third session, Hanna reported worse sleep, taking a longer time to initiate sleep most evenings, and more frequent awakenings. She also admitted that she had exceeded the recommended dose of medication on two occasions in the preceding week due to increased knee pains. She had been overwhelmed by thoughts about not getting enough sleep and had worried about the next day. She felt ashamed and disappointed in herself. Hanna’s experiences gave the therapist an opportunity to remind her about common withdrawal symptoms and to introduce relapse prevention and procedures to facilitate discontinuation of the medication. Hanna’s beliefs and negative thoughts about not getting enough sleep and the consequences for her daily functioning were challenged by the therapist, and in the session, she was asked to reflect on the validity of her thoughts and assumptions. She was given psychoeducation about common negative beliefs and misperceptions about sleep, and, as homework assignment the upcoming week, she was to identify negative thoughts about not falling asleep and the consequences of a sleepless night. To reduce worrying at bedtime, Hanna was encouraged to write down her worries in the notebook earlier in the evening or afternoon, as well as to systematically practice the mindfulness exercises at bedtime. Hanna had made several changes to her evening and bedtime routines and rituals to attain the goals set in the first homework assignment. She had stopped drinking coffee and smoking cigarettes after 5 p.m. as well as drinking and eating when she woke up during the night. Instead, she had a light meal in the evening. She had also increased her activity level and had started to go for walks in the afternoon.
In the fourth session, Hanna was “back on track” and proclaimed that she was ready to reduce the Zopiclone dose to 5 mg per night. She had fewer withdrawal symptoms. She reported less tension at bedtime, and better sleep. She experienced fewer awakenings during the night, and each awakening lasted for a shorter time. An Ibuprofen gel that she smeared on her knee at bedtime alleviated her knee pain. She found that writing down her worries in the afternoon gave her a kind of distance to these thoughts. Hanna’s negative thoughts dwelled on not getting enough sleep to function well during the day, and she felt that she tried to force herself to sleep some evenings. She realized that struggling with sleep and trying to control her sleep were hopeless endeavors. In the session, she was taught how to view her negative thoughts about sleep in a different way by letting them come and go like leaves in a stream. In Sessions 5 and 6, Hanna reported another relapse, taking 7.5 mg Zopiclone on two occasions during a 2-week period due to knee pains and worries about the next day. For her homework assignment, the therapist recommended that she formulate positive self-instructions for use on critical occasions. One such self-instruction was as follows: “I’ll manage. Changing sleep habits and finding new ways to get to sleep takes time, I have to be patient.”
At the end of the treatment, Sessions 7 to 10, the focus was on cessation of Zopiclone and relapse prevention, and on how to continue to use the techniques and skills acquired during the treatment. In Session 9, Hanna proudly announced that she had eliminated Zopiclone. She reported that she still had problems initiating sleep, but that her mental attitude toward sleep had changed. She practiced mindfulness every evening and felt that the exercises calmed her down and made her more relaxed when lying in bed. She also experienced that the mindfulness exercises helped her to cope better with the pain. Hanna emphasized that the new way of relating to her thoughts, by observing them and letting them pass without acting on them, was the most important lesson she had learned. She estimated her average amount of sleep to be 6 hr, 5 to 7 hr on most weekdays, and she usually fell asleep within 30 min. She realized that changing sleep and sleep habits takes some time and that sleeping through the night without awakenings was unrealistic. She felt she could function well during the daytime despite having an occasional sleepless night.
Assessment of Progress
Hanna’s scores for the self-report measures at the start of treatment, at the end of treatment, and at 6-month follow-up are presented in Table 1.
Scores on Self-Report Measures at Pretreatment, Posttreatment, and Follow-Up.
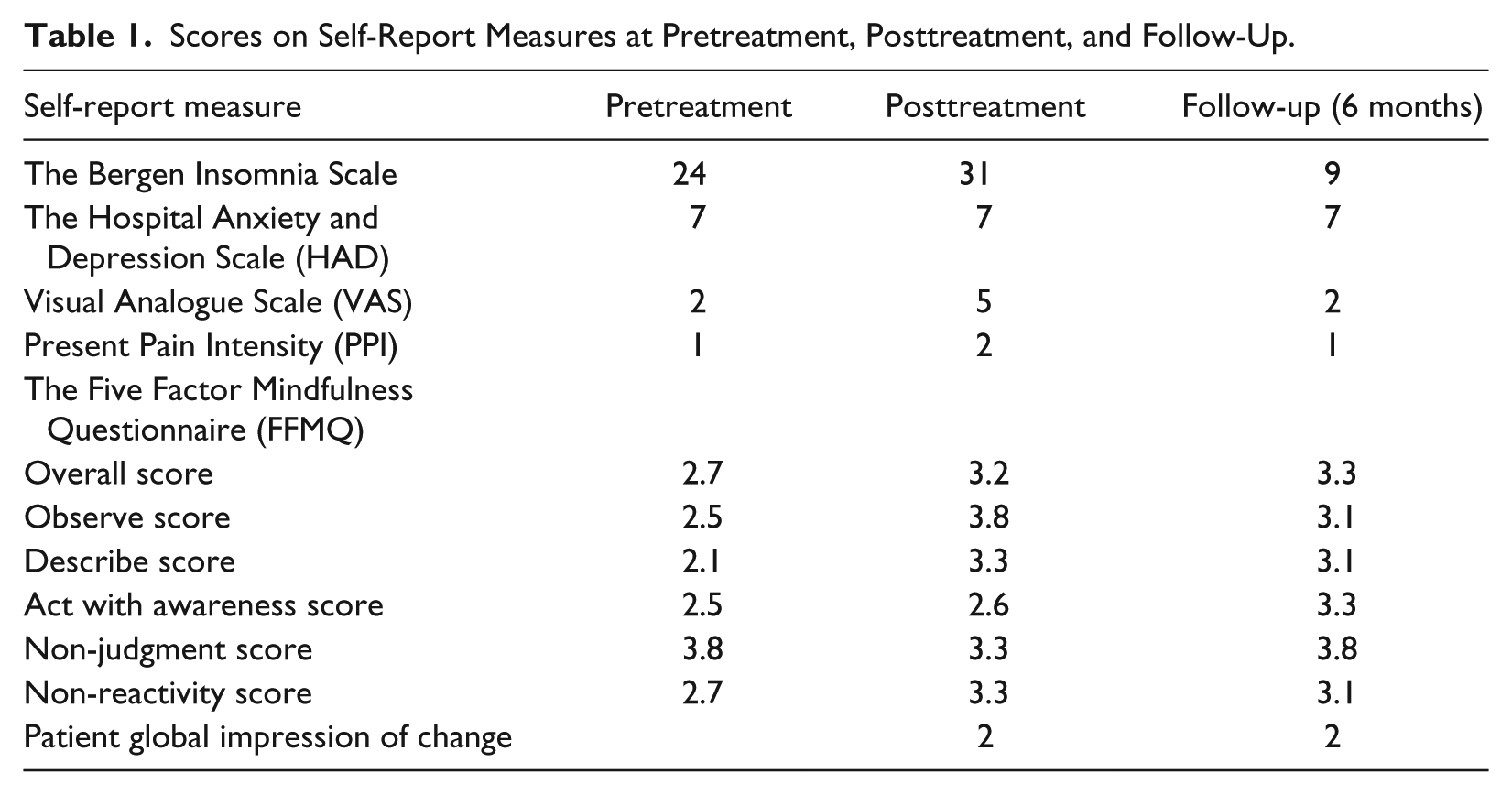
At intake assessment, the scores on the Bergen Insomnia Scale confirmed that Hanna had symptoms of insomnia. Most pronounced were problems initiating sleep despite her use of hypnotics, and frequent awakenings during the night. She also had a relatively high score for feeling unrestored during the day. At the end of treatment, the total score had increased, indicating even more severe insomnia compared with treatment start. One important explanation was the discontinuation of medication, which caused withdrawal symptoms such as rebound insomnia, a common phenomenon when eliminating hypnotics (Morin et al., 2004). Furthermore, her knee pain had worsened during the course of treatment and this had a negative impact on sleep as well. However, at follow-up, her total score had dropped below the pretreatment score, and Hanna reported that she felt refreshed and satisfied with her sleep. She still had problems initiating sleep some nights, but she coped better with the symptoms. First and foremost, she was still abstinent and had not relapsed into taking hypnotics, and she reported better short-term memory and better balance.
Hanna’s scores on HAD, both initially and after treatment, indicated only minimal symptoms of anxiety and depression. During the course of treatment, she reported tensions and anxiety-like symptoms at bedtime, but regularly practicing the mindfulness exercises helped her regain calm. Her scores for the pain self-report measures (VAS and PPI) increased at the end of treatment due to a worsening of her knee pain. At follow-up, however, the scores were in the low range, indicating minimal pain.
Results on the mindfulness measure showed that Hanna’s ability to stay present with perceptions, sensations, thoughts, and feelings, even when they are unpleasant, had increased during treatment. At follow-up, her overall FFMQ score indicated a persisting change in her ability for being mindful.
By and large, Hanna managed to follow the gradual medication withdrawal schedule despite the minor relapses described above, and she reached the goal of elimination within the course of treatment of 10 weeks. She reported few long-lasting withdrawal symptoms, most of the symptoms being transient.
At the end of treatment and at follow-up, Hanna filled in the Patient Global Impression of Change questionnaire, reporting that her condition was much better compared with treatment start. This indicates an important clinical significant change.
8 Complicating Factors
Older adults have an increased susceptibility to comorbid somatic and psychiatric disorders that may have an effect on the course of treatment (Waters et al., 2005). Chronic pain conditions influence sleep and can complicate treatment progress. In this particular case, the patient’s osteoarthritis and resultant pain interfered with the medication withdrawal schedule. Prior to treatment, Hanna’s insomnia symptoms had worsened as a consequence of her pain situation. During the course of treatment and withdrawal schedule, she experienced two relapses in which she exceeded the recommended dose of medication. Hanna primarily related these relapses to her knee pain. Minor relapses are not uncommon during a step-by-step medication withdrawal regimen, and should be expected in most cases. However, it is important that the patient learns to identify situations and symptoms that increase the craving for medication to prevent major relapses.
9 Access and Barriers to Care
There were no access barriers in this particular case.
10 Follow-Up
At 6-month follow-up, Hanna was still abstinent and reported no drug relapse. By and large, she slept well and felt more restored during daytime. She had not been absent from work. She had problems initiating sleep some nights, and she still woke up once or twice most nights. The awakenings were shorter than before, however. Overall, Hanna experienced better coping and she systematically practiced mindfulness exercises and positive self-instruction at bedtime. Furthermore, she described increased awareness of the present moment in several everyday situations. She believed that changing her mental attitude toward sleep and using the tools she had acquired in therapy had a positive side-effect on her pain, as well as on other areas of her life.
11 Treatment Implications of the Case
This case indicates that hypnotic-dependent insomnia can be treated with a step-by-step medication taper, at the same time as the underlying sleep problems are addressed through a combined intervention of mindfulness meditation and elements from CBT for insomnia. Although hypnotics were eliminated within 10 weeks, treatment did not have the intended effect on insomnia symptoms, at least on a short-term basis. This calls for caution when interpreting the findings. However, at the end of treatment, Hanna reported better overall functioning compared with treatment start, and at follow-up, her insomnia symptoms had improved. Behavioral corrections of poor sleep habits may be useful in minimizing sleep difficulties (Morin et al., 2004). Cognitive techniques are effective in reducing misperceptions about sleep and can lead to adaptive changes in thought patterns (Morin et al., 2004). Mindfulness meditation fosters the development of a non-judgmental attitude toward unpleasant experiences, which, in turn, may reduce sleep-related arousal, as well as pain and substance misuse (Chiesa & Serreti, 2014; Ong et al., 2008; Veehof et al., 2011). Hanna is in many ways representative of older patients typically seen in clinical practice, often presenting with complex symptoms and complaints such as insomnia, pain, and drug dependence. Given the increased susceptibility of older adults to comorbid symptoms and distressing phenomena, a broadly focused intervention simultaneously targeting the multiple problems could result in more helpful and cost-effective treatment.
A major limitation of this study was the lack of specific sleep parameters such as sleep diary. A sleep diary is recommended as a reliable self-report measure of sleep and yields more specific daily estimates on several sleep and daytime variables such as sleep onset latency, number of awakenings during the night, wake time after sleep onset, total sleep time, and sleep efficiency, as well as overall functioning during daytime (Buysse, Ancoli-Israel, Edinger, Lichtstein, & Morin, 2006).
12 Recommendations to Clinicians and Students
We believe that it is essential to devote more attention to stabilization of the intake of medication prior to the start of treatment to prevent and minimize relapses during the course of treatment. In our experience, the rationale for stabilization of the medication intake should be explained as concretely as possible, underlining both the psychological aspect of breaking the habit of taking medication on an as-needed basis to avoid unpleasant experiences and the aim of reducing withdrawal symptoms. Furthermore, incorporating principles from motivational interviewing in the initial treatment phase could enhance motivation and reduce resistance to change behavior and habits (Rollnick et al., 2008). As in the present case, major improvement in sleep may only be noticeable after several months of abstinence. It is therefore important to inform the patient about this potential delay at the start of treatment (Morin et al., 2004). The use of mindfulness exercises is intended to help the patient break away from habitual reactions to the craving for drugs once gradual medication withdrawal starts. The aim is also to enable the patient to experience how systematic training in mindfulness can enhance awareness of momentary personal choices and actions related to unpleasant and distressing phenomena, as well as to pleasant experiences. The rationale for combining two seemingly different therapy goals, that is, symptom reduction versus a more flexible behavior repertoire, should be thoroughly explained to the patient. First and foremost, cognitive behavioral tools and techniques combined with mindfulness exercises may bolster confidence and competence in internal methods of initiating and maintaining sleep without the use of medication.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.