
Abstract
Although the majority recovers from the death of a loved one, nearly 5% exhibit persistent symptoms of grief, known as Persistent Complex Bereavement Disorder (PCBD). PCBD has adverse health, social, and psychological consequences. We examined the effectiveness of dialectical behavior therapy (DBT) skills training with a 57-year-old African American woman who met the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria for PCBD and Persistent Depressive Disorder. The client met with a graduate student therapist (i.e., the second author) who applied DBT skills training on an individual basis. By the end of treatment, the participant no longer met the criteria for either of these disorders. Reliable and clinically significant reduction in her grief and depressive symptoms, suicidality, and sleep difficulties were noted from pre- to posttreatment and maintained for 2 months post treatment. Furthermore, she improved her ability to regulate her emotions and cognitions using DBT coping skills and eliminated substance abuse. These results prompt the need for more research to further investigate DBT skills training for PCBD.
1 Theoretical and Research Basis for Treatment
Although the death of a loved one is a common, albeit disruptive, event from which the majority recover, nearly 5% exhibit persistent symptoms of grief for over a year, referred to as Persistent Complex Bereavement Disorder (PCBD), a condition listed for further study in Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013). According to the five criteria (i.e., a through e) of the DSM-5, an individual with PCBD must (a) experience the death of someone whom he or she has had a close relationship, (b) evince one of the following four symptoms (i.e., yearning for the deceased, sorrow, preoccupation with the deceased, and preoccupation with circumstances of the death), (c) experience six of 12 symptoms related to reactive distress and/or social/identity disruption, (d) evidence clinically significant distress or functional impairment, and (e) exhibit distress which is outside of sociocultural norms. In addition, the aforementioned symptoms are present for at least 12 months after the death of a loved one and are not better accounted for by a major depressive disorder, generalized anxiety disorder, or posttraumatic disorder (American Psychiatric Association, 2013). PCBD has been associated with clinically significant health, social, and psychological consequences, including suicidality (Fujisawa et al., 2010; Shear, 2011).
Despite its prevalence and detrimental consequences, treatment for PCBD is in its infancy. Studies investigating the effects of antidepressant medications, such as nortriptyline or bupropion, on individuals with PCBD have shown an inadequate response of PCB symptoms to these medications (Shear et al., 2011). Although emerging evidence supports the efficacy of some PCBD-targeted psychotherapy (Currier, Neimeyer, & Berman, 2008; Fujisawa et al., 2010; Shear et al., 2011; Vergara-Lopez & Roberts, 2015; Wyman-Chick, 2012), more research on treatments that target the specific difficulties and needs experienced by individuals with PCBD is warranted.
Although dialectical behavior therapy (DBT) was originally designed to treat borderline personality disorder (BPD) and has since been applied to other conditions involving pervasive dysregulation of emotions, DBT had not been used to treat PCBD (Chapman, 2006). DBT is grounded in the biosocial theory of Linehan (1993). Per this model, emotional dysregulation is foundational to the problems experienced by individuals with BPD and has its roots in biological and socioenvironmental components. It is posited that these individuals’ emotional response systems are easily triggered because of neurobiological vulnerabilities implicated in eliciting and regulating emotions or because of early social experiences involving an invalidating environment, which may include trauma, which in turn may have adversely impacted neural pathways underlying emotion regulation. Consequently, an ongoing transaction can occur between an individual’s biological vulnerabilities and the environment. The highly sensitive emotion system of individuals with BPD reacts to environmental stimuli faster and with greater intensity compared with other individuals, rendering them vulnerable to dysregulation across five domains: affective (e.g., affective instability), behavioral (e.g., impulsivity), interpersonal (e.g., pattern of unstable and intense relationships), cognitive (e.g., problematic thinking or faulty beliefs and assumptions), and self (e.g., identity disturbance).
Standard DBT addresses these five domains of dysregulation through multiple modes of treatment, including weekly individual therapy, phone coaching as needed, and skills training, which is typically delivered in a group format. Individuals with BPD often have deficits in knowledge or use of skills involving the aforementioned five areas of dysregulation. Thus, the DBT skills training targets these skills deficits by incorporating the following four modules over a 6-month period: (a) core mindfulness skills targeting cognitive and self-dysregulation through training regular practices involving elements of attentional control, (b) emotion regulation skills to address emotional dysregulation, (c) interpersonal effectiveness skills to help individuals learn to be effective in relating to others, and (d) distress tolerance skills targeting behavioral, emotional, and cognitive dysregulation (Linehan, 2014). Moreover, DBT skills training, as a stand-alone treatment, has been effective for treatment-resistant major depressive disorder (Harley, Sprich, Safren, Jacobo, & Fava, 2008). In light of the evidence that DBT skills training has been effectively applied to disorders of emotional dysregulation, DBT may be a promising new treatment for PCBD.
DBT skills training for PCBD is grounded in the biosocial theory of Linehan (1993). Consistent with Linehan’s biosocial model, PCBD is conceptualized as a disorder of emotional dysregulation that emerges from transactions between individuals with predisposing vulnerability and specific environmental influences. The authors propose a sequenced biosocial theory for PCBD as shown in Figure 1. Predisposing vulnerabilities include person factors of the bereaved (e.g., female gender, low perceived social support, and biological susceptibility) and death event factors (e.g., death by suicide and death of an adult child; American Psychiatric Association, 2013; Fujisawa et al., 2010; Shear, 2011; Shear et al., 2011). Researchers have demonstrated evidence of biological differences in emotion regulation that distinguish those with PCBD from those without. For example, when provided reminders of the deceased, those with PCBD, compared with those bereaved without PCBD, evidenced significantly increased activation of the nucleus accumbens, part of the brain’s reward system, which has been associated with more self-reported yearning for the deceased (O’Connor et al., 2008). Moreover, personal vulnerabilities interact with environmental influences over the life span, rendering one more susceptible to PCBD. When individuals with PCBD attempt to discuss their loss with others, they are often met by invalidating environments which ignore or inhibit opportunities to debrief (Maple, Edwards, Plummer, & Minichiello, 2010). In sum, the emotional dysregulation of PCBD arises from predisposing vulnerabilities and death factors transacting over time with an invalidating environment that often denies and rejects the individual’s emotional experience. This transaction ultimately leads to worsening overall dysfunction of the individual with PCBD, which has been described by the criteria in the DSM-5 (American Psychiatric Association, 2013).
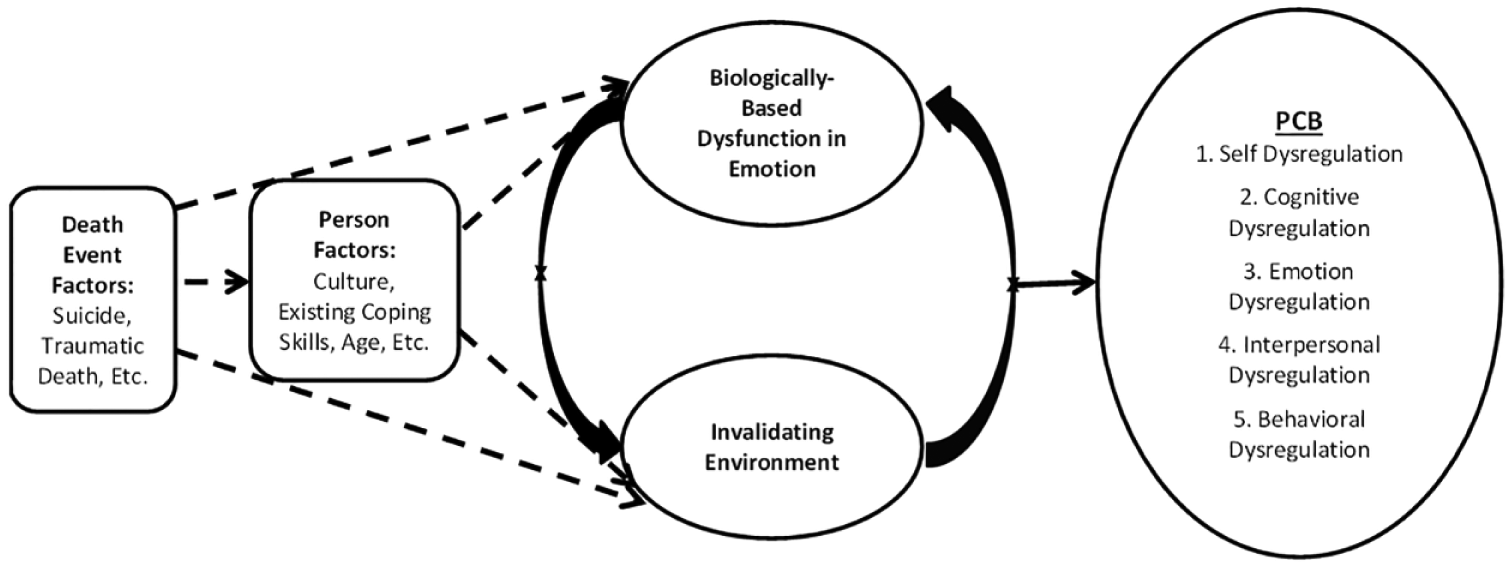
Sequenced biosocial theory of PCB.
DBT skills training is ideally suited to target the following five areas of dysregulation that can be seen in the DSM-5 diagnostic criteria for PCBD: cognitive dysregulation (e.g., preoccupation with the deceased and/or the circumstances of the death), emotional dysregulation (e.g., intense sorrow in response to the death, bitterness or anger related to the loss), interpersonal dysregulation (e.g., difficulty trusting others since the death, feeling alone, or detached from others since the death), behavioral dysregulation (e.g., marked difficulty accepting the death, excessive avoidance of reminders of the loss), and self-dysregulation (e.g., confusion about one’s role in life, maladaptive appraisals about oneself). Specifically, mindfulness skills target the cognitive and self-dysregulation components of PCBD, emotion regulation skills target the affective components, interpersonal effectiveness skills target social functioning, and distress tolerance skills target behavioral components, particularly nonacceptance behaviors. Notably, enhancement of mastery of coping skills has been a predictor of psychological adjustment after bereavement (Onrust, Cuijpers, Smit, & Bohlmeijer, 2007). However, the effectiveness of DBT skills training for PCBD remains to be explored. The present case study investigated the effectiveness of teaching DBT skills to treat PCBD.
2 Case Introduction
“Angela” was a divorced, 57-year-old, African American mother and grandmother, whose only daughter died in her early 20s, more than 5 years prior to this treatment. Her daughter’s death was sudden and unexpected; the cause of death was not known. Since her death, Angela experienced an intense grief reaction on more days than not, including intense yearning for her daughter, rumination about the circumstances of her daughter’s death, and preoccupation with her daughter. She also experienced the following symptoms to a clinically significant degree: difficulty accepting the loss, bitterness related to the loss, difficulty trusting others, meaninglessness of her life without her daughter, self-blame, role confusion, depressed mood, low self-esteem, hopelessness, irritability, frequent crying, and suicidal ideation. During the 5 years since her daughter’s death and prior to DBT skills training, Angela worked with three different therapists. She only attended a few sessions with her first two therapists and terminated because she did not find them to be helpful. She then worked with her third therapist for nearly 3 years and reported that she made “some progress,” but the aforementioned symptoms persisted. At intake, Angela reported that her symptoms were significantly interfering with her ability to function in daily life. She also acknowledged nearly daily use of alcohol and cannabis.
3 Presenting Complaints
Angela was referred for DBT skills training by her individual therapist. She reported that she wanted to improve her coping skills, be less emotionally reactive, improve interpersonal communication (not “hold things in and let them build up”), and reduce angry outbursts at work. She also wanted to reduce depressive symptoms and suicidal ideation. Although Angela did not name goals explicitly linked to the diagnostic criteria for PCBD, she identified that her grief reaction was the underlying cause of all of her other symptoms. She expressed little hope that she could ever “move on” from the loss of her daughter but was hopeful that she could make some improvements on her other “surface problems,” such as conflict at work.
4 History
Angela reported that she had a difficult childhood. She was the middle child in a family of five and the only female. Her parents were both teachers. She reported that her mother was emotionally, verbally, and physically abusive and often made mean comments about Angela’s physical appearance. She was often afraid of her mother and sustained a few significant injuries as a result of the abuse. She described her father as an “emotionally detached whoremonger.” Although her home life was often unpleasant, she indicated that her life outside of home was very happy in childhood. She did well in school and loved being active and playing outdoors. She was outgoing and always had a small circle of close friends. However, she reported that she never really felt like she “fit in.”
Angela earned a bachelor’s degree and at the time of treatment was employed in a full-time salaried position. She had one son in addition to her deceased daughter. She divorced her husband, the father of her children, 10 years prior, after years of marital conflict. They had been married for 18 years. A year prior to the divorce, she began a relationship with a married woman which lasted for nearly a decade. They broke up because Angela wanted greater commitment, but her partner did not. Since the ending of that relationship, she had not dated anyone else. She indicated that she had a strained relationship with her son and reported that he had behavioral problems and had been incarcerated. Prior to her daughter’s death, Angela never participated in therapy, although she did take antidepressants prescribed by her primary care physician for a few months in the immediate aftermath of her divorce.
5 Assessment
Prior to beginning DBT skills training, Angela completed our standard battery of measures for PCBD, including the Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005), the Beck Depression Inventory–II, (BDI-II; Beck, Steer, & Brown, 1996), Brief Grief Questionnaire (BGQ; Shear, Jackson, Essock, Donahue, & Felton, 2006), Suicidal Behaviors Questionnaire (SBQ; Addis & Linehan, 1989), Brief Symptom Inventory (BSI; Derogatis, 1993), DBT-Ways of Coping Checklist (DBT-WCCL; Neacsiu, Rizvi, Vitaliano, Lynch, & Linehan, 2010), Barkley Deficits in Executive Functioning Scale–Short Form (BDEFS-SF; Barkley, 2011a), Barkley Functional Impairment Scale–Long Form (BFIS-LF; Barkley, 2011b), and Pittsburgh Sleep Quality Index (PSQI; Buysse, Reynolds, Monk, Berman, & Kupfer, 1989). Her performance on the MoCA, a brief 30-point screening measure of cognitive functioning, did not indicate cognitive impairment. On the BDI-II, a commonly used 21-item self-report measure designed to quickly assess the presence and severity of symptoms of Major Depressive Disorder, she obtained a score of 25, considered suggestive of a moderate level of depressive symptoms. In addition, she obtained an elevated score of 1.3 on the Global Severity Index of the BSI, a 53-item self-report inventory designed to assess psychological symptoms in nine domains, including somatization, obsessive–compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. She scored a 7 on the BGQ, a five-item self-report measure used to screen for the presence of PCBD on which respondents are asked to rate the extent to which they currently experience different grief symptoms, such as difficulty accepting the death, troubling thoughts related to the death, or feeling distant from others. Scores equal to or above 5 are considered suggestive of PCBD. Angela completed the SBQ, a 34-item self-report inventory designed to assess an individual’s level of suicidality and includes items to measure five suicidal behavior domains (e.g., past suicidal ideation and past suicide threats, as well as the respondent’s estimation of the likelihood of future suicidal ideation, suicide attempts, or death by suicide). For example, in response to the item—“Have you ever told someone that you were going to commit suicide, or that you might do it in the last year,” she endorsed “yes, more than once.” In response to the SBQ item—“Would any of your problems be solved if you committed suicide,” she endorsed “maybe.” She scored an 18 on a 23-item suicidal ideation subscale of the SBQ, raising concerns about suicidality as a score of 0 on this scale would indicate no suicidal ideation. In terms of sleep, on the PSQI, a 19-item self-report questionnaire designed to assess sleep quality and disturbances over a 1-month time interval, she obtained a Global Score of 9; a global score greater than 5 is indicative of poor sleep quality (Buysse et al., 1989).
With regard to DBT constructs in particular, she completed the DBT-WCCL, a 38-item self-report inventory that asks respondents to rate how often they have used various forms of coping strategies over the past month, including both adaptive and dysfunctional strategies. She obtained a score of 2.14 on the Dysfunctional Coping Subscale Mean, which indicates that she used dysfunctional coping skills somewhere between “sometimes used, 2” and “regularly used, 3,” whereas she scored a 1.84 on the DBT Skill Use Mean, which indicates that she used DBT/effective skills somewhere between “rarely used, 1” and “sometimes used, 2.” Her level of daily functioning was assessed by the BFIS-LF, a 15-item, self-report measure designed to assess an individual’s level of impairment in various major life activities, such as managing relationships, work, and money. The threshold for defining whether an individual is impaired in a given area is the rating equivalent to or greater than the 93rd percentile for the normative sample. Although Angela’s mean impairment score, which represents the average impairment scores across all the domains, was 3.5 (i.e., 75th-84th percentile range) and does not meet the aforementioned threshold, this overall score masks her functional impairment in the following domains: work (96th percentile), social interactions with strangers and acquaintances (98th percentile), relationship with friends (98th percentile), and dating relationships (98th percentile). Finally, on a 20-item, self-report inventory (i.e., BDEFS-SF) designed to measure deficits in various domains of adult executive functioning in daily life including self-management to time, self-organization/problem solving, self-restraint, self-motivation, and self-regulation of emotions, Angela’s total Executive Functioning summary score of 57 is equivalent to the 99th percentile, which suggests a deficiency in executive functioning.
6 Case Conceptualization
The characteristics of the death of her daughter, “Carrie,” placed Angela at particular risk for PCBD. Not only did she lose an adult child, but she also was personally involved in the circumstances of her daughter’s death. On the night before her death, Carrie asked Angela to bring her to the local emergency room (ER) because of internal pain. After waiting many hours in the ER waiting room without receiving help, they decided to leave the hospital with the intention of returning the following day. Her daughter died during the night, and thus, Angela has blamed herself for her daughter’s death. At the time of her death, Carrie was Angela’s primary attachment relationship. They were in daily contact and had a close, supportive, and stabilizing relationship. Interaction with her daughter after work and on weekends provided a reliable rhythm to Angela’s life. In addition, serving the role of parent was central to Angela’s core sense of self. Thus, when Angela lost her daughter, she reported experiencing severe cognitive, emotional, and behavioral dysregulation, in addition to profound disruption in her sense of self with regard to her role as a loving mother. She felt confusion about her new role in life, believed that her life was now meaningless, and often considered suicide. She also developed maladaptive appraisals about herself, due to her self-blame for her daughter’s death. She believed that she had failed as a mother and was preoccupied with the circumstances of Carrie’s death, frequently ruminating about how Carrie might still be alive if only Angela had made different choices on the night of her death. She also felt an intense longing for Carrie’s presence, which did not subside with time. She filled her home with pictures of Carrie and thought about her all the time, in an attempt to feel connected to her and to feel some relief from her emotional pain. Perhaps related to her insecure attachment style, she lacked other attachment figures to help fill her daughter’s void. She was divorced and lived alone. Although she also had a son, he lived in another state and they were rarely in contact. She felt close to his children but was only able to visit them a few times per year. In addition, she felt like an “outsider” in her predominantly-Caucasian community, and was reluctant to attempt to make friendships or pursue a romantic relationship. Her intense sorrow persisted for more than 5 years after the death, and she began abusing alcohol and cannabis as an attempt to cope. Thus, Angela’s overall treatment need was help with emotion regulation, which is the primary target of DBT skills training.
7 Course of Treatment and Assessment of Progress
Over 6 months, Angela worked weekly with a graduate student therapist (i.e., second author) and received 26-hr-long sessions of individual DBT skills training covering the four modules of mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness. She was taught a new skill each session and was assigned behavioral practice for homework. Each week, she also received feedback on homework from the previous week.
DBT Skills Training began with the mindfulness module as these skills are considered to be the core set of skills and many of the other skills build upon these skills. The mindfulness skills were taught for the first two sessions and then subsequently taught again for two sessions after each of the other modules were taught. Mindfulness skills emphasize the importance of staying centered in the present moment in a nonjudgmental manner. Clients are first taught how to cultivate a state of mind referred to as “wise mind,” a synthesis of both reason and emotion. Clients learn that when in the state of “wise mind,” they can still experience their emotions without becoming overwhelmed by them or losing control. They are taught several ways to cultivate the state of “wise mind” (e.g., engaging in deep breathing techniques while focusing on the word “wise” on the in-breath and “mind” on the out-breath). Angela effectively used “wise mind” skills at work to curb her angry outbursts; for example, she used the “wise mind” breathing technique whenever a particular coworker with whom she had a history of conflict made insulting comments. This technique helped her to reach a state of calm where she could remember that responding aggressively was inconsistent with her goal of developing a positive impression as a team player and skilled communicator. The next skills covered in this module involve techniques to achieve a “mindful” as opposed to “mindless” state. These skills include observing, describing, and fully participating in life experiences in a particular way: without judgment, attending to one thing at a time, and remembering to act effectively (i.e., focusing on what works rather than on being “right”). For individuals with PCBD, who are often preoccupied with thoughts about the deceased, the circumstances of the death, or negative cognitions about themselves, learning mindfulness skills may increase their ability to shift their attention to the present moment and away from painful rumination. During the second skills training session, the therapist led a mindfulness exercise which involved going on a walk while focusing on the sights and sounds of the environment as well as bodily sensations. Following this session, Angela began to go for mindful walks every evening. By doing so, she reduced and eventually stopped her use of alcohol and cannabis in the evenings. In addition, Angela was profoundly affected by the lesson that thoughts are only thoughts, and do not necessarily represent reality. This idea helped her to more effectively manage maladaptive appraisals about herself, as she recognized that simply because she often had negative thoughts about herself, those thoughts did not indicate that she was hopelessly flawed. Notably, the immediate benefits she observed from using these skills greatly increased her motivation to learn and apply other more difficult skills in the later modules.
Next, the Distress Tolerance module was introduced to Angela with the aim of teaching her how to endure painful, unchangeable situations without resorting to maladaptive responses, such as substance abuse, that might reduce distress in the short term but make problems worse in the long term. The skills described in this module are based upon the premise that experiencing pain in various forms, such as the loss of the loved one, is an inevitable part of the human experience, and thus, skills are needed to manage this pain in effective ways. The module includes both crisis survival strategies and acceptance strategies. The crisis survival strategies include distraction techniques, self-soothing strategies, and improving-the-moment methods, such as engaging in prayer or looking for meaning in a painful situation. These crisis survival strategies may help clients with PCBD to more effectively endure moments of intense, painful yearning for the deceased.
Acceptance strategies teach clients skills to embrace reality just as it is, even if it involves pain. Individuals with PCBD have great difficulty accepting the reality of their loss. This denial of reality manifests itself in many ways, but ultimately hinders the individuals’ ability to move forward after the loss and build a life that is meaningful to them even in the absence of their loved one. Reality acceptance skills address this aspect of PCBD. Although reality acceptance skills are a crucial component of DBT Skills Training for PCBD, they can be very painful skills to learn. Initially, Angela was reluctant to discuss how these skills applied to the loss of her daughter and even asked to end a session early because of the emotional distress brought on by talking about these skills. The therapist was able to motivate her to stay by highlighting how much her efforts toward learning previous skills had helped her. In addition, because Angela had already experienced so much benefit from her work with the therapist, rapport was very strong at this point, and thus, the therapist was able to capitalize on the strength of the therapeutic relationship to convince Angela to try to apply the skills of Radical Acceptance. Radical Acceptance is based on the premise that suffering occurs when an individual refuses to accept pain. Angela practiced completely accepting reality as it is, rather than devoting energy to resist the death of her daughter. Specifically, on Mother’s Day, she radically accepted that she would not see her daughter and decided to plan a trip to see her grandchildren that weekend, rather than ruminating on how she wished that her daughter was still alive. She was very encouraged by how this skill helped her to continue to build a life worth living by engaging in family activities that were important to her, even on Mother’s Day, a day marked by incapacitating sadness in previous years.
Emotion regulation skills were covered next. These skills are designed to help clients like Angela reduce unwanted emotions and increase positive and effective emotions. First, clients are taught how to identify, label, and experience emotions in a nonjudgmental manner. For example, one skill in this module involves visualizing emotions as waves which reach a peak and then subside. Angela used this skill to cope with sadness and anger without resorting to impulsive and harmful actions, such as substance abuse or aggression. By recognizing that the emotion would eventually subside, she was able to refrain from acting on it. She was also taught the skill of Opposite Action, which involves engaging in an activity which is incompatible with the current emotion to change it. For example, when feeling sad and tired one morning, Angela turned on loud, upbeat music and began dancing, which generated happy feelings that lasted for the rest of the morning. Next, clients are taught skills for reducing vulnerability to negative emotional states, such as obtaining adequate sleep, maintaining physical health, and engaging in activities that help clients to feel self-confident and competent. Clients are also encouraged to engage in activities that generate positive emotions. Individuals with PCBD have often withdrawn from many of the activities that brought them joy prior to the death, and these skills help clients to resume engaging in pleasurable and/or meaningful activities. For example, Angela enjoyed exercise, interior decoration, dancing to music, and eating at restaurants and made a plan to engage in these activities on a regular basis to increase positive emotions.
The Interpersonal Effectiveness Skills module was taught last. This module includes strategies for how to make interpersonal requests, say no, and cope with interpersonal conflict. Clients are taught to analyze interpersonal situations to identify goals for interpersonal interactions, such as obtaining objectives, maintaining the relationship, or maintaining self-respect. Those goals are then used as the guide for choosing the appropriate interpersonal skill strategy. Individuals with PCBD often are reluctant to maintain or pursue friendships after the loss and feel detached and distrustful of others. Angela used these skills both at work and in her social life. For example, Angela was able to successfully address a false, negative report made about her made to her boss by a coworker. She successfully used the DEAR MAN technique, an acronym for describing the facts, expressing one’s feelings, asserting one’s needs, and reinforcing desired behavior while remaining mindful, appearing confident, and negotiating as necessary. She used another technique referred to as GIVE to maintain a positive relationship with a friend following an argument. This technique involves gentle responding, showing interest, validating, and using an easy manner.
Results
Angela completed clinical interviews and self-report measures at pretreatment and posttreatment (see Table 1). The Reliable Change Index (Jacobson & Truax, 1991) statistical approach was used to assess whether the changes in scores from pre- to posttreatment were reliable and clinically significant; this approach was applied to all measures where necessary information for the analysis was available in the literature (e.g., mean of the reference population), including the BFIS, BDI-II, BSI, and PSQI. At pretreatment assessment, Angela met DSM-5 criteria for PCBD and Persistent Depressive Disorder. Her BDI-II score indicated a moderate level of depressive severity, and her BGQ score was elevated (i.e., 7). By the end of treatment, Angela no longer met criteria for either PCBD or Persistent Depressive Disorder. Her scores on the BDI-II, BSI, PSQI, and BFIS reliably decreased. Moreover, all of the domains on the BFIS and the BDEFS were well below the clinical threshold suggestive of impairment. In addition, her BGD score decreased from clinically elevated 7 to a score of 2, which was within normal limits.
Changes in Scores on Measures Across Time.
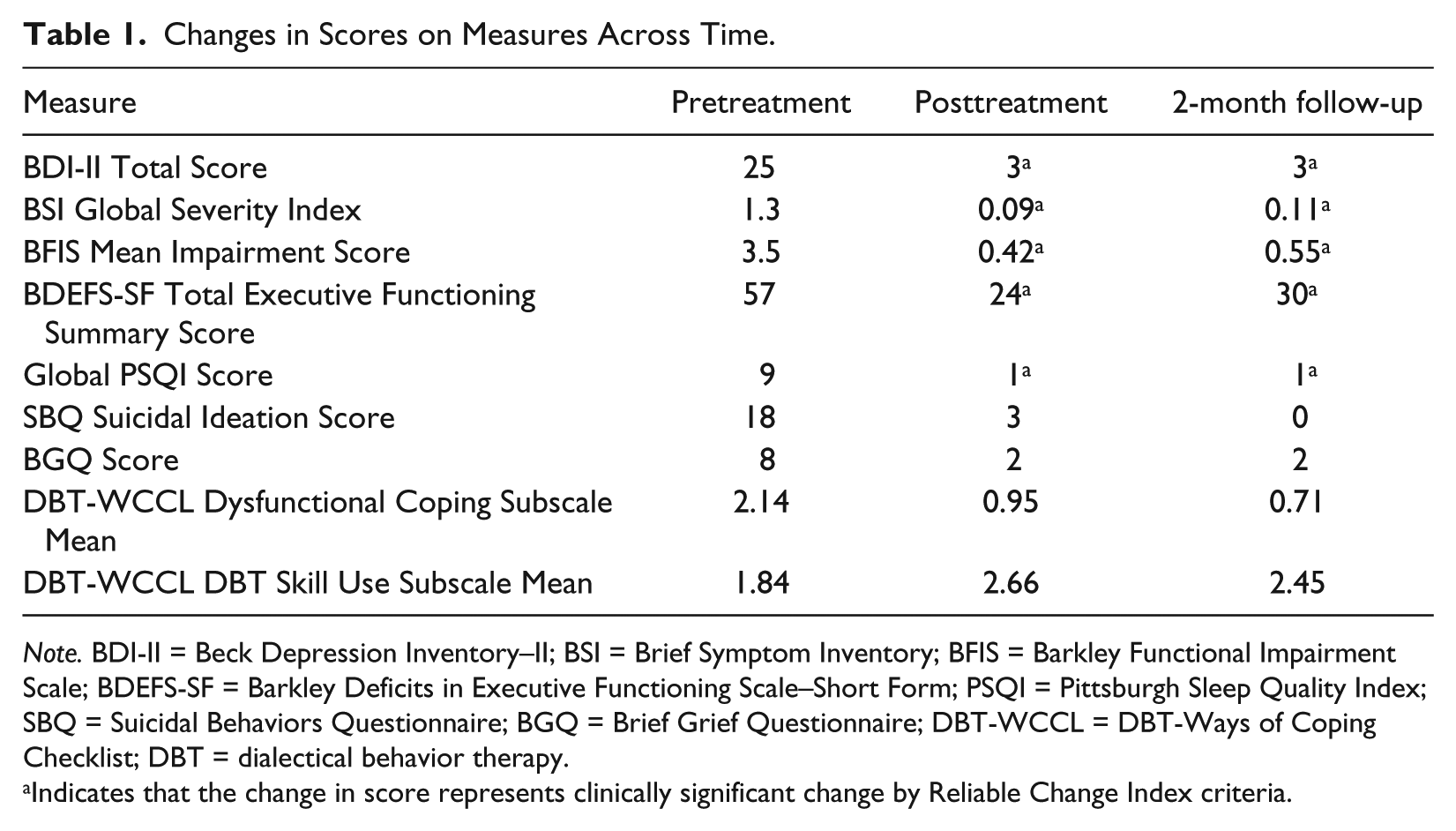
Note. BDI-II = Beck Depression Inventory–II; BSI = Brief Symptom Inventory; BFIS = Barkley Functional Impairment Scale; BDEFS-SF = Barkley Deficits in Executive Functioning Scale–Short Form; PSQI = Pittsburgh Sleep Quality Index; SBQ = Suicidal Behaviors Questionnaire; BGQ = Brief Grief Questionnaire; DBT-WCCL = DBT-Ways of Coping Checklist; DBT = dialectical behavior therapy.
Indicates that the change in score represents clinically significant change by Reliable Change Index criteria.
Scores on a number of measures that the reliable change index could not be calculated also decreased. Her sleep problems score on the PSQI decreased from a global score of 9 to a 1, indicating that at posttreatment and follow-up, she was reporting minimal sleep difficulties. Her suicidal ideation score on the SBQ decreased from 18 at pretreatment to 0 at follow-up, indicating that she was reporting no ideation at the time of follow-up. On the DBT-WCCL, Angela’s score on the Dysfunctional Coping Subscale Mean decreased from 2.14 to 0.71 at follow-up. This indicates that while she was using dysfunctional coping skills somewhere between “sometimes used, 2” and “regularly used, 3” at pretreatment, her use decreased to a range between “never used” and “rarely used.” Her use of DBT skills increased from a mean of 1.84 to 2.66 at posttreatment. Thus, she moved much closer to the maximum score of 3, which indicates that these skills are “regularly used.”
8 Complicating Factors
It is important to note that the client involved in this pilot study did not receive full-scale DBT treatment but only DBT skills training. Full-scale DBT also involves three additional modes of treatment, including individual therapy with a DBT-trained therapist, as-needed telephone coaching, and a therapist consultation team (Linehan, 1993). Although skills training was originally designed to be implemented within the context of full-scale DBT, recent evidence suggests that DBT skills training by itself may be effective as a stand-alone treatment for some individuals (Chapman, 2006).
At the beginning of her DBT skills training, Angela continued to receive individual therapy with the referring therapist in addition to DBT skills training. However, she terminated therapy with the referring therapist after 3 months of skills training. She reported that she terminated individual therapy because she believed that her symptoms were no longer severe enough to warrant participating in both modes of treatment. She did not discuss this with the DBT skills trainer prior to terminating individual therapy but rather reported it after the fact.
9 Access and Barriers to Care
Many with PCBD do not receive adequate treatment ( Shear et al., 2011). One reason for inadequate treatment is that they may have difficulty recognizing it as a problem and underutilize mental health services, which is often the case with older adults (Segal, Qualls, & Smyer, 2011). In addition, those with PCBD are either misunderstood as having a normal grief reaction or are misdiagnosed with depression ( Shear, 2011; Shear et al., 2011). Although symptoms of depression and PCBD overlap, PCBD is distinguishable from depression in terms of risk factors, clinical correlates, and temporal course ( Shear, 2011; Shear, Ghesquiere, & Katzke, 2013).
10 Follow-Up
Follow-up was conducted 2 months post treatment. Angela completed clinical interview and self-report measures at this interval as in the previous time. She maintained the treatment gains at 2 months post treatment, as shown in Table 1. Furthermore, she reported increased DBT skill use in her daily life and decreased use of dysfunctional coping skills.
11 Treatment Implications of the Case
For Angela, it appears that her participation in DBT skills training was associated with a number of positive outcomes related to reductions in the impact of PCBD in her life. The treatment was well-received by Angela. Overall, it appears that the dialectical balance of acceptance-based skills (e.g., mindfulness and distress tolerance) and change-based skills (e.g., emotion regulation and interpersonal effectiveness) was a good match for the problems related to PCBD that Angela was experiencing. There were minimal modifications made to standard DBT skills training. While DBT skills training is often delivered in a group format, individual skills training is an acceptable format (Linehan, 2014). This treatment warrants further exploration for the treatment of individuals with PCBD.
The therapist utilized DBT skills training with Angela due to the manner in which the skills targeted Angela’s problems and the symptoms of PCBD. Angela’s increased utilization of the mindfulness skills allowed her to detach from preoccupations about her daughter and other maladaptive thoughts. As she practiced detachment from these thoughts, they had less impact on her, and as the thoughts had less impact on her, the frequency and intensity of the thoughts decreased. The use of mindfulness skills by individuals with PCBD can help to address their overall cognitive dysregulation. In fact, other preliminary research has supported the effectiveness of mindfulness-based interventions for bereaved individuals (O’Connor, Piet, & Hougaard, 2014; Thieleman, Cacciatore, & Hill, 2014).
Angela also increased her use of distress tolerance skills. She utilized strategies for enduring painful moments in her life through skills like self-soothing. Angela also worked on moving away from strategies such as denial, yearning, and longing and instead practiced completely accepting reality as it is. Individuals with PCBD suffer from significant problematic outcomes due to nonacceptance of reality. Furthermore for Angela, over the course of learning skills, she went from having significant suicidal ideation to none. For example, when asked how likely she is to consider killing herself in her life at pretreatment, Angela responded with a 2 indicating “some chance.” At posttreatment and follow-up, Angela responded to the same question with a 0 indicating “no chance at all.” Also, when asked whether she had a plan for killing herself if she decided to do it, Angela endorsed “yes, a definite plan” at pretreatment and “no” at posttreatment and follow-up. Often, suicide and suicidal rumination can be utilized as a way to avoid and escape from problems. When asked whether any of her problems would be solved if she committed suicide, Angela endorsed “maybe” at pretreatment and “no” at posttreatment. Individuals with PCBD are at significantly increased risk for suicide (Latham & Prigerson, 2004). DBT has consistently been shown to be effective at reducing suicidal behaviors (Lynch, Trost, Salsman, & Linehan, 2007). DBT skills training has promise as an intervention to help those individuals with PCBD who may view their lives as no longer worth living.
Through the use of increased emotion regulation skills, Angela was able to increase practices of emotional acceptance rather than avoidance, changing unhelpful emotional states, and decreasing her vulnerability to emotional dysregulation. Angela avoided her emotions in a variety of ways that had problematic consequences including substance abuse and aggressive actions. Boelen, van den Bout, and van den Hout (2006) found that in a prospective study, emotional avoidance among bereaved individuals was predictive of a variety of problems at later time points including depression and PCBD. Angela’s increased use of emotion regulation skills was correlated with her reductions in depression, symptoms of PCBD, and other symptoms. Thus, emotion regulation skills training among individuals with PCBD shows promise.
Finally, through the use of increased interpersonal effectiveness skills, Angela was able to maintain and improve relationships at work and socially. Among bereaved individuals, social support has been found to be a protective factor against PCBD and depression (Vanderwerker & Prigerson, 2004). For Angela, the improved interpersonal functioning, decreased isolation, and improved connections were cited as helpful to her overall well-being and quality of life. It is possible that the DBT interpersonal effectiveness skills can help individuals with PCBD with problems such as their detachment and difficulties with trusting others. Utilization of interpersonal skills may help individuals with PCBD influence the environment to increase the likelihood of validation rather than invalidation.
12 Recommendations to Clinicians and Students
DBT skills training can be successful with a person with PCBD and significant suicidality when delivered by a graduate student therapist (i.e., second author). The individual DBT skills training sessions were delivered by the graduate student therapist who had gone through in-depth training in DBT. The graduate student therapist trained in DBT for a 1-year period under the guidance of a faculty mentor (i.e., third author) who is a DBT expert. The training included guided reading of the DBT manuals, watching video-recorded DBT sessions, role-play rehearsal, and participation and practice in a full cycle of DBT skills training. It is recommended that individuals, including students, who have been trained in DBT, apply skills training with clients with significant difficulties including PCBD and significant suicidality.
It is also recommended that therapists assess for PCBD carefully and avoid treating it and the associated problems as normal grief. Furthermore, individuals with PCBD may be treated by inadequately informed health providers who see their grief as normal grief ( Shear et al., 2011). There is a paucity of treatments available for individuals with PCBD, and some of the most widely available support-oriented treatments designed for those with normal grief may not be effective for individuals with PCBD (Jordan & Neimeyer, 2003). Therapists may be able to access one of the treatments with preliminary empirical support such as Complicated Grief Treatment developed by K. Shear, Frank, Houck, and Reynolds (2005). Therapists may also consider directly targeting the problems of PCBD by applying DBT skills training. Although more research is needed, DBT skills training shows promise as a potential option for treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.