
Abstract
We report the case of a woman who had intellectual disability, made frequent bathroom requests, and spent excessive time in the bathroom at a day-habilitation center. Functional behavioral assessment suggested that frequency and duration of bathroom requests were escape-motivated. Intervention was directed at reducing the reinforcing effects of visiting the bathroom through (a) activity scheduling, (b) cuing the woman to exit the bathroom according to a fixed time limit, and (c) gradually reducing the time limit to an acceptable duration. Compared with a baseline phase, intervention was associated with decreased bathroom requests and duration of bathroom visits that were maintained at 2-month follow-up. We discuss clinical implications of these findings and recommendations to practitioners.
Keywords
1 Theoretical and Research Basis for Treatment
Some individuals who have intellectual disability (ID) exhibit challenging behaviors that are negatively reinforced by escape from particular interactions and environmental conditions (Beavers, Iwata, & Lerman, 2013; Miltenberger, 2006). For example, aggression, self-injury, property destruction, and related problems have been shown to be maintained by escape from task demands, transition requests, medical procedures, and setting locations (Luiselli, 2008). Conducting preintervention functional behavioral assessment (FBA) is necessary to identify the antecedent and consequence conditions that consistently precede and follow challenging behaviors (Reed & Azulay, 2011). Indirect methods of FBA rely on rating scales and questionnaires (Durand & Crimmins, 1988; Paclawskyj, Matson, Rush, Smalls, & Vollmer, 2000), while descriptive methods of FBA entail direct observation coding and conditional probability analyses (Bijou, Peterson, & Ault, 1968; Martens, DiGennaro, Reed, Szczech, & Rosenthal, 2008). Research shows that intervention plans derived from FBA are more likely to be effective than procedures that are arbitrarily selected without regard to behavior function (Call, Scheithauer, & Mevers, 2017).
Changing antecedent variables that reliably provoke or set the occasion for escape-motivated challenging behaviors is an effective intervention methodology, notably (a) reducing task difficulty (Dunlap, Foster-Johnson, Clarke, Kern, & Childs, 1995), (b) fading instructions (Zarcone et al., 1993), (c) shaping approach responses (Kozlowski, Mahan, & Matson, 2010; Schmidt, Luiselli, Rue, & Whalley, 2013), (d) allowing choice-making (Cannella, Reilly, & Lancioni, 2005), (e) scheduling noncontingent escape (Kodak, Miltenberger, & Romaniuk, 2003; Moore, Robinson, Coleman, Cihak, & Park, 2016; Vollmer, Marcus, & Ringdahl, 1995), and (f) teaching an individual to appropriately request escape through functional communication training (FCT; Carr & Durand, 1985). From the perspective of consequence control, the basis of intervention is applying escape extinction (Lerman & Iwata, 1996) that prevents access to preferred sources of reinforcement such as attention, objects, and activities.
Many times, intervention plans for escape-motivated challenging behaviors combine several procedures. In illustration, Butler and Luiselli (2007) treated a 13-year-old girl who had autism and exhibited escape-motivated aggression, self-injury, and tantrums during instructional sessions at school. One intervention procedure scheduled a brief break from sessions starting at a fixed time of 20 s and gradually increased this duration. A second procedure, instructional fading, slowing increased the number of task requests presented to the girl across consecutive sessions. This multi-procedure intervention plan eliminated the challenging behaviors, the fixed-time break from sessions was advanced to a 5-min duration, and the girl responded successfully to task requests approximately every 20 s.
The present case study describes intervention with a woman who had ID and high-frequency requests that led to prolonged durations in the bathroom. Pre-intervention assessment determined that bathroom requests and time in the bathroom were escape-motivated, leading to an intervention plan intended to reduce the reinforcing effects of bathroom visits. The study illustrates the contribution of FBA to case formulation and the design of multi-procedure treatment of escape-motivated challenging behaviors. To our knowledge, this is the first reported case in which seeking the bathroom was the escape-motivated behavior requiring treatment.
2 Case Introduction
Mandy (a fictitious name) was a 22-year-old female who had been diagnosed with autism, severe ID, and impulse control disorder. She communicated primarily through gestures, pointing to pictures, an assistive device, and sometimes verbal approximation of single words. Mandy was able to make requests, respond to simple instructions, and complete self-care and daily living routines with adult support. At the time of the study she lived in a community-based group home and attended a day-habilitation center for adults with similar developmental disabilities. Mandy had a lengthy history of challenging behaviors, including self-injury, aggression, and noncompliance, which were treated with variable success through applied behavior analysis (ABA) intervention and psychotropic medications.
3 Presenting Complaints
Mandy made frequent requests to use the bathroom when attending her day-habilitation center from approximately 9:00am to 3:00pm on weekdays. Upon entering a single-person bathroom, she would occasionally use the facilities appropriately but also remain in the bathroom without purposeful activity, often vocalizing loudly, becoming agitated, and engaging in masturbation. Attempts by care-providers to interrupt these behaviors or assist Mandy to exit the bathroom were usually associated with further disruption and aggression. On some days, she was spending more than 2 hours cumulatively in the bathroom, an excessive amount of time that seriously compromised her participation in training activities and socialization opportunities at the center.
4 History
Mandy had received special education services from an early age within public and private school programs. Before entering the location of the current study, she was a student at a residential school for children and youth who had developmental disabilities. As noted previously, she required support to treat and manage challenging behaviors that were disruptive, self-harming, and dangerous to care-providers. The problem of high-frequency and long-duration bathroom visits was also a clinical priority at previous educational settings.
Medical and nursing evaluations had ruled out physical causes that might have accounted for her seeking and remaining in the bathroom so frequently and for such long periods of time, respectively. Specifically, she had never been diagnosed as having enuresis or encopresis, problems with bladder or bowel control, or related elimination disorder (Lytle, Ruedrich, Kaelber, & Mikkelsen, 2016).
The case study was initiated approximately two months after Mandy entered the day-habilitation center based on historical review and observations conducted by the supervising psychologist (first author) and center director (second author). Upon meeting with care-providers at the center, it was determined that Mandy would benefit from formal assessment and intervention directed at her frequent bathroom requests and prolonged bathroom visits. The supervising psychologist, center director, and care-providers formed a treatment team that was responsible for designing, implementing, and evaluating the study.
5 Assessment
Care-providers at the day-habilitation center were assigned to supervise and interact with Mandy individually during all of her daily scheduled activities. These care-providers were responsible for recording two dependent measures within all phases of the study. Frequency of bathroom requests was defined as Mandy asking to use the bathroom through a verbal or nonverbal communication response. The care-providers recorded her bathroom requests on a form that was located on a clipboard they carried with them throughout the day. The second dependent measure, duration of bathroom visits, was defined as the cumulative amount of time Mandy spent in the bathroom per request. Using the same form, care-providers recorded the time to the nearest minute that Mandy entered and exited the bathroom. The second author trained the care-providers to conduct frequency and duration recording several days before initiating formal baseline assessment.
6 Case Conceptualization
We conducted FBA preceding intervention to identify antecedent and consequence conditions that were associated with bathroom requests and visits. The FBA included (a) direct observation of Mandy at the day-habilitation center, (b) review of baseline data, and (c) care-provider interviews according to the semistructured format contained in the Functional Analysis Interview (FAI; O’Neill, Horner, Albin, Sprague, Storey, & Newton, 1997).
The results of FBA suggested that Mandy frequently requested the bathroom when she was interacting with care-providers during “demand” activities such as completing prevocational tasks, participating in domestic routines, making transitions, and working with unfamiliar materials. She initiated bathroom requests less frequently when engaged with more preferred activities, for example, eating snacks and lunch, listening to music, and watching videos. Concerning the duration of time Mandy spent in the bathroom, FBA suggested that her disruptive behavior was maintained by care-providers not interacting with her and possibly, automatic (sensory) reinforcement that was contacted by masturbating.
Our case conceptualization was that bathroom requests and long-duration bathroom visits were escape motivated and negatively reinforced by termination of nonpreferred activities and interactions. Mandy clearly requested the bathroom within these conditions compared to less demanding and more preferred activities. Upon entering the bathroom, she could continue to avoid activities and interactions by remaining there for extended periods of time. Occasions of masturbation in the bathroom further reinforced escape by gaining access to pleasurable stimulation.
The focus of function-based intervention was to implement antecedent and consequence procedures that have been used effectively for treating escape-motivated challenging behaviors (Luiselli, 2008; Miltenberger, 2006). From an antecedent perspective, the procedures were eliminating a daily setting event that was associated with high-frequency bathroom requests, and cuing Mandy to exit the bathroom according to a gradually decreasing time limit. The cuing procedure was also considered a consequence method of response interruption and redirection (RIRD; Martinez & Betz, 2013). The intervention objective of this multi-procedural plan was to reduce escape motivation by attenuating the reinforcing effects of extended bathroom visits.
7 Course of Treatment and Assessment of Progress
Several procedures were applied identically within all phases of an A-B-C single-case design (Kazdin, 2011). First, care-providers always acknowledged Mandy when she requested the bathroom. To ensure privacy, Mandy remained in the bathroom by herself, with a supervising care-provider standing outside the bathroom door. Third, care-providers implemented a behavior support plan (BSP) with Mandy that instructed them in how to present task materials to her, deliver positive reinforcement (praise, approval), withdraw attention contingent on noncompliance, and physically intervene as a consequence for aggression and self-injury. Note that the BSP was not directed at the problem of bathroom requests and visits, which were targeted in a separate intervention plan, described below.
There were no changes in implementation of the BSP throughout the study. That is, care-providers consistently delivered praise to Mandy when she complied with instruction, allowed her contingent access to preferred activities, and maintained individual (1:1) supervision throughout the day.
Baseline
After acknowledging her bathroom request, the supervising care-provider “shadowed” Mandy as she walked to and entered the bathroom. There was no further interaction between Mandy and the care-provider until she independently exited the bathroom, at which time the care-provider delivered praise (e.g., “Very good, thank you.”) and directed her to return to ongoing activities. Other than the previously described assessment procedures, the conditions during baseline had been in effect preceding the study.
Activity Scheduling
Baseline data revealed that Mandy often resisted activities, demonstrated increased agitation, and requested bathroom visits persistently during mid-day activities at the day-habilitation center. We reasoned that substituting alternative activities might interrupt this pattern and reduce Mandy’s motivation to seek the bathroom. The activity schedule manipulation consisted of care-providers taking Mandy and several of her peers on a recreational van ride though neighboring communities from approximately 1:00 p.m. to 1:45 p.m. each day. This free-time activity was simply integrated within Mandy’s daily schedule and with baseline procedures still in effect. Going on a van ride had been previously identified as a pleasurable activity for Mandy.
Cuing and Demand-Fading
Identical to baseline and activity scheduling phases, care-providers continued to acknowledge every bathroom request by Mandy and took her on the mid-day van ride. The following multi-procedure intervention plan was added:
Bathroom visits were restricted to a fixed time limit starting at 7 min. This initial duration was calculated based on approximately 60% of the average duration recorded in the baseline phase.
The fixed bathroom time limit in effect was indicated on the daily recording form. Whenever Mandy entered the bathroom following a request, the supervising care-provider set an interval timer to this duration.
If Mandy exited the bathroom independently before the interval timer sounded, the supervising care-provider delivered praise and directed her to return to ongoing activities.
When the interval timer sounded, signaling that Mandy had not exited the bathroom independently, the supervising care-provider informed her, “It is time to leave the bathroom now.” If Mandy did not exit the bathroom when cued, the supervising care-provider withdrew attention, reset the interval timer to the specified duration, and repeated procedures until Mandy either exited the bathroom when cued again or independently between timed-cues. Upon exiting the bathroom, the care-provider delivered praise and directed Mandy to return to ongoing activities.
We progressively reduced the initial 7-min bathroom duration by 1-min segments to a terminal criterion of 3 min. These reductions were made every 3 to 4 weeks in an effort to expedite duration-fading.
Figure 1 presents the average duration of daily bathroom visits each week. During the baseline phase, bathroom visits averaged 11.4 min. With activity scheduling, Mandy spent less time in the bathroom, averaging 8.7 min per visit. The effect of cuing and demand-fading was a variable but gradual decrease in average duration, starting with the 7-min bathroom time limit and ending with the 3-min bathroom time limit. During the final 2 weeks of cuing and duration-fading, the average duration of bathroom visits had decreased to 3.7 min.
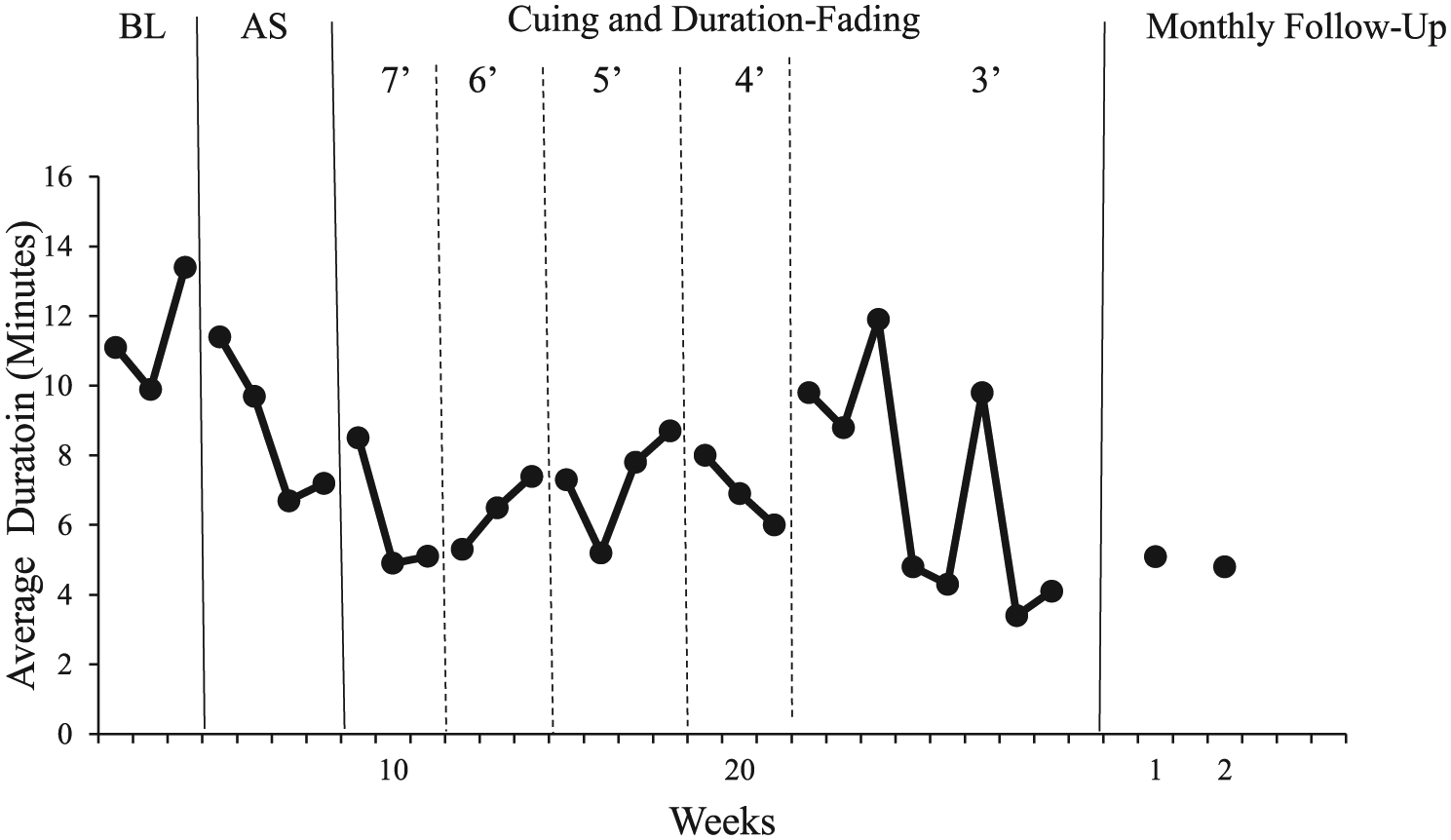
Average duration of daily bathroom visits.
Figure 2 presents the average frequency of daily bathroom requests each week. Mandy averaged 5.6 bathroom requests per day in the baseline phase, followed by 4.9 bathroom requests per day during the activity scheduling phase. Average frequency of bathroom requests increased during the initial 6 weeks of cuing and duration-fading but then decreased steadily in the remaining weeks, falling to 3.2 per day in the final 2 weeks of intervention.
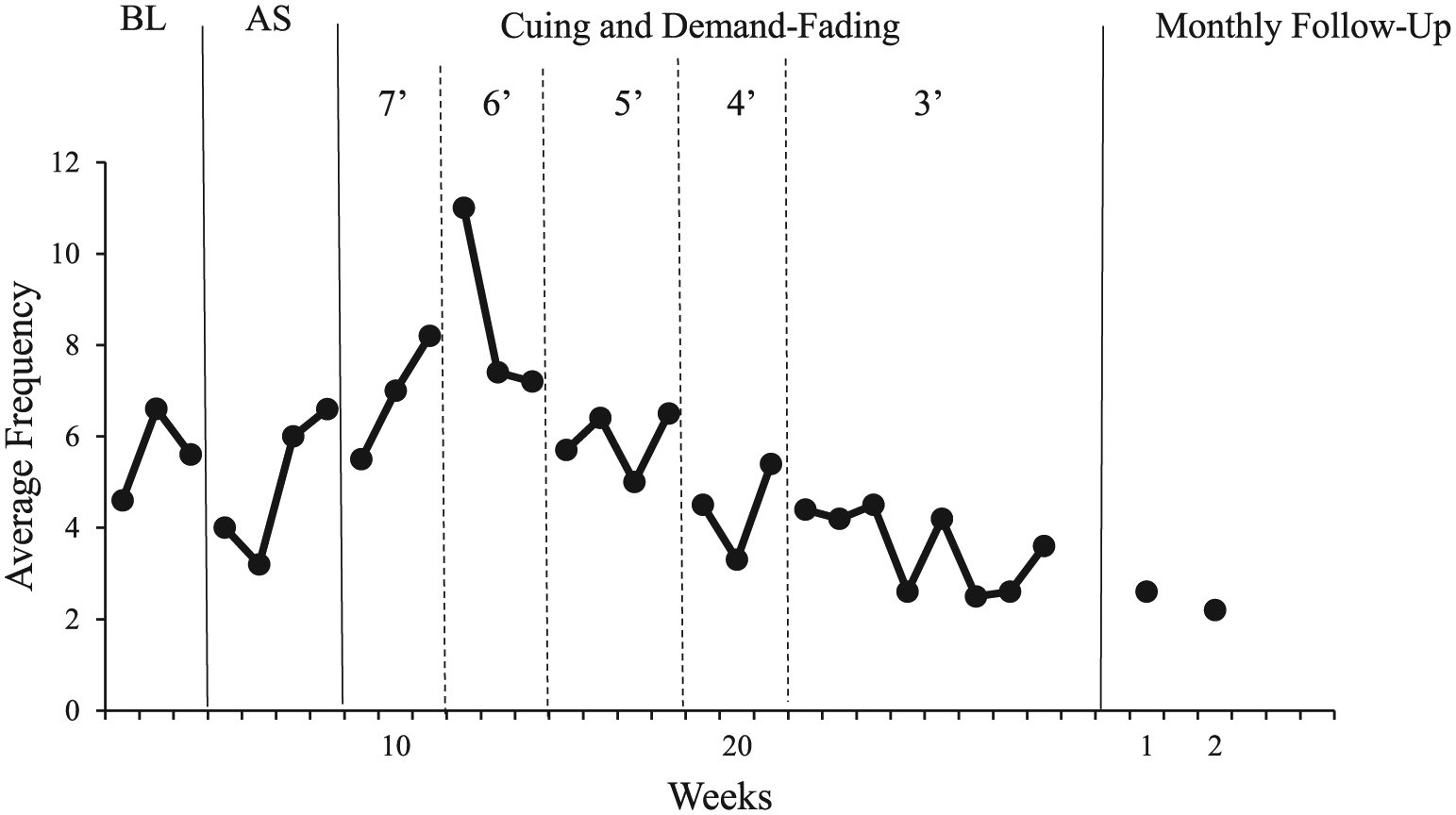
Average frequency of daily bathroom requests.
Routine observations at the day-habilitation center and reports by care-providers confirmed that Mandy exhibited fewer challenging behaviors over successive weeks of the study For example, although it was not uncommon for her to behave disruptively in the bathroom during baseline, she did so much less frequently throughout intervention. Furthermore, her compliance with instructions to exit the bathroom when cued also improved considerably during the study.
8 Complicating Factors
The primary complicating factor in developing intervention with Mandy was avoiding procedures that might provoke serious challenging behaviors. In addition, we could not consider a plan that denied her requests to access to the bathroom. Intervention through activity scheduling, cuing, and duration-fading appeared to reasonably address these factors, Mandy responded favorably, and she did not demonstrate unanticipated problems.
9 Access and Barriers to Care
The day-habilitation center Mandy attended was a publically funded program that fully supported all aspects of service delivery. She was transported to and from the center each day, her attendance was exemplary, and there were no barriers to care.
10 Follow-Up
Following intervention, care-providers continued to implement activity scheduling, cuing, and duration-fading (3-min bathroom time limit) with Mandy at the day-habilitation center. Figure 1 shows that Mandy averaged 2.6 and 2.2 bathroom requests per day at 1- and 2-month follow-up assessments, respectively. The average duration per bathroom visit was 5.1 min at 1-month follow-up assessment and 4.8 min at 2-month follow-up assessment. These data reflect good maintenance of intervention effects from average baseline levels of 5.6 bathroom requests each day and 11.4 min per bathroom request.
11 Treatment Implications of the Case
In the present case, high-frequency and prolonged-duration bathroom visits were assessed as escape-motivated. The intervention plan (a) altered one of the conditions associated with bathroom requesting (activity scheduling), (b) time-limited bathroom visits (cuing), and (c) slowly decreased bathroom time limits to an acceptable level (duration-fading). These procedures were informed by preintervention FBA and were also selected because they were relatively easy for care-providers to implement at the day-habilitation center. Of course, as a multi-procedure intervention plan, the study cannot confirm whether one or a combination of the procedures were responsible for outcome.
Similarly, the source of control exerted by the intervention procedures is unclear relative to the treatment objective of decreasing and ultimately eliminating the reinforcing effects of bathroom visits. Through activity scheduling Mandy had less exposure to conditions that appeared to provoke escape by requesting the bathroom. Cuing was intended to limit her time in the bathroom without causing agitation—the approach in this regard was allowing Mandy to “choose” when to exit the bathroom after being instructed. Finally, duration-fading further reduced time in the bathroom, gradually, and consistent with choice-making. The bathroom duration changes achieved by the end of the study and at follow-up suggest that intervention was effective but these results should be interpreted cautiously given threats to internal validity inherent with a single-case sequential design (Barlow, Nock, & Hersen, 2009). That is, other factors not controlled in the study (e.g., social reinforcement from care-providers, in-bathroom masturbation) may have influenced Mandy’s response to intervention.
The impact of intervention on the reinforcing effects of bathroom visits is further suggested by the daily frequency of requests. Recall that the emphasis of intervention was to reduce duration of bathroom visits and as described, Mandy’s requests to access the bathroom were never restricted during the study. However after increasing for several weeks following the baseline phase, bathroom requests dropped substantively as intervention progressed, stabilizing at an average frequency of 2-3 requests per day. Possibly, this outcome may have occurred because over the course of the study Mandy was less motivated to escape activities and interactions by requesting the bathroom.
Notably, there was a variable trend for both bathroom duration and requests within and between intervention phases. Following baseline, the average duration per bathroom visit decreased when activity scheduling was implemented and remained relatively stable during the initial four phases of cuing and duration-fading. Average duration increased in the first 3 weeks at the 3-min bathroom limit but then decreased, with further variability, until reaching a sustained lower duration. It is not clear what factors may have been responsible for the variability demonstrated within the 3-min duration phase, perhaps Mandy’s reaction to the most stringent limit on bathroom time that had been imposed and/or a longer period for her to adjust. As for the average frequency of bathroom requests, there was a 2-week decrease following the baseline phase, then increased requesting for 6 weeks, followed by a steady and less variable reduction through follow-up. In summary, these variable response trends must be acknowledged, notwithstanding the positive results that were ultimately achieved with a long-standing, interfering, and socially stigmatizing challenging behavior.
12 Recommendations to Clinicians and Students
While focusing on the functional influences controlling escape-motivated challenging behaviors of persons with ID, clinicians and students should consider other characteristics of the presenting problem. For example, in this case, requesting and spending time in the bathroom had several concerns beyond the goal of behavior reduction. First, because Mandy was able to use the bathroom appropriately, her requests could not be denied. Second, her privacy in the bathroom was respected by unobtrusive monitoring outside the door. Finally, and to reiterate prior description, the cuing procedure was applied strategically to decrease time in the bathroom while allowing Mandy to exit when she was ready. Thus, in addition to function, the topography and associated features of challenging behaviors should inform intervention formulation.
The duration-fading component of intervention was consistent with a transfer of stimulus control methodology (Touchette & Howard, 1984). Some practitioners may choose to only initiate duration changes when a person consistently meets an imposed criterion and with little variability. In our case, we continued to drop the time limit of bathroom visits when the duration data suggested that Mandy was responding successfully, albeit not precisely aligned with the selected time limit. The already noted increase in average bathroom duration when we initiated the 3-min time limit could have been addressed by reinstating the preceding time limit, establishing control at that level, and advancing once again to the more stringent criterion. We recommend that clinicians and students consider the exigencies of slower-paced fading protocols versus more accelerated but less precise sequences that may hasten desired intervention effects.
An additional recommendation is that following initial training, care-providers should be closely supervised to ensure that they implement intervention accurately. In this study, the director of the day-habilitation center routinely observed care-providers conducting intervention with Mandy and provided performance feedback to them. The center director also reviewed intervention progress with the clinician who was responsible for planning and evaluating the study. We suggest that this degree of oversight is essential when intervening with persons who have ID and complex challenging behaviors, training care-providers in natural service settings, selecting function-based procedures, and supporting intervention integrity (DiGennaro Reed, Hirst, & Howard, 2013; Luiselli, 2015a, 2015b; Parsons, Rollyson, & Reid, 2012).
Footnotes
Acknowledgements
We thank the care-providers who implemented assessment and intervention procedures during the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.