
Abstract
Smokers suffer from high rates of anxiety disorders, presumably because some individuals with anxiety disorders rely on smoking as a maladaptive attempt to manage anxiety. Cognitive behavioral therapy (CBT) is an efficacious smoking cessation treatment, yet outcomes are worse for patients with elevated anxiety. The integration of CBT for smoking cessation with False Safety Behavior Elimination Therapy (FSET) may be useful with anxious smoking cessation patients, as smoking to manage anxiety and associated negative affect can be targeted as a false safety behavior (i.e., behavior aimed at decreasing anxiety in the short-term but which may maintain or exacerbate it in the long-term). Here, we describe the integrated treatment, Treatment for Anxiety and Smoking Cessation (TASC), and the successful use of it with two smoking cessation patients—one with comorbid generalized anxiety disorder (GAD) and one with clinically elevated social anxiety that did not meet diagnostic threshold for an anxiety disorder. Data support the feasibility of TASC as a viable approach to smoking cessation treatment for patients with comorbid anxiety disorder and with elevated anxiety that does not meet diagnostic threshold. Future controlled trials are now warranted to further evaluate the intervention.
Theoretical and Research Basis for Treatment
Cigarette smoking is the leading cause of death and disability in the United States, contributing to over 480,000 deaths each year (Centers for Disease Control and Prevention, 2018). Although approximately 70% of current adult smokers are motivated to quit (Centers for Disease Control and Prevention, 2017), only 11% to 40% smokers who participate in intensive front-line smoking cessation treatments achieve long-term abstinence (e.g., Cahill, Stevens, Perera, & Lancaster, 2013; Heckman, Egleston, & Hofmann, 2010). The U.S. Department of Health & Human Services’ Clinical Practice Guidelines for Treating Tobacco Dependence identified smokers with comorbid conditions as important targets for treatment intervention (Fiore et al., 2008).
Among the various affect-based psychopathologies, anxiety symptoms and syndromes are particularly important to study because they are highly prevalent in the general population and remarkably comorbid with smoking (e.g., Leventhal & Zvolensky, 2015). To illustrate, nearly one fourth of individuals with nicotine dependence suffer from at least one comorbid anxiety disorder compared with 11% of the general population (Grant, Hasin, Chou, Stinson, & Dawson, 2004). The relation of smoking incidence and maintenance to anxiety disorder generalizes across various clinical conditions, including panic disorder, social anxiety disorder, and generalized anxiety disorder (GAD; Piper, Cook, Schlam, Jorenby, & Baker, 2011). Furthermore, elevated anxiety symptoms and disorder status increases the risk of smoking experimentation (Leventhal, Ray, Rhee, & Unger, 2011), progression to daily smoking (Audrain-McGovern, Rodriguez, Rodgers, & Cuevas, 2011), and development of nicotine dependence (McKenzie, Olsson, Jorm, Romaniuk, & Patton, 2010). Among current smokers, anxiety symptoms and disorders often increase risk of smoking cessation failure (e.g., Piper et al., 2010) and heighten severity of tobacco withdrawal (e.g., Buckner, Langdon, Jeffries, & Zvolensky, 2016). The relation between smoking and anxiety appears to be bidirectional as smoking can increase the severity of anxiety disorders symptoms. For example, daily smoking prospectively increases the risk for developing anxiety symptoms (e.g., Johnson et al., 2000) and can exacerbate the severity of such symptoms (e.g., Zvolensky et al., 2004).
Numerous studies indicate anxiety disorders significantly impair smoking cessation success. For example, Piper and colleagues (2010) examined the relation of psychiatric disorders to tobacco dependence and smoking cessation outcomes among 1,504 people making an aided smoking cessation attempt as part of a clinical trial. Six months after quitting, those with a lifetime history of an anxiety disorder had the lowest abstinence rates. These findings provide evidence that anxiety disorders are important in reducing the odds of successful quitting. Yet, anxiety is frequently not addressed in smoking cessation treatment.
Negative reinforcement models of addiction motivation assert that self-administration of a substance is contingent on the extent to which it serves to terminate or mitigate an aversive event (Baker, Piper, McCarthy, Majeskie, & Fiore, 2004). Given that nicotine can produce acute perceived and objective anxiolytic effects, smokers with anxiety may self-medicate or cope with distress by smoking (Baker et al., 2004). Indeed, smokers who experience greater anxiety and anxiety-related negative affect during a quit attempt may return to smoking, in part, to alleviate increased anxious states. Among the most prominent and clinically significant constructs, accumulating research suggests that false safety behaviors (FSB; behaviors used to attempt to decrease anxiety in the short term but which may maintain or exacerbate anxiety long term) may be especially important to understanding the effects of anxiety on smoking cessation.
FSBs are highly utilized across anxiety conditions because they often temporarily alleviate anxiety (e.g., avoiding a situation that engenders fear; Schmidt, Buckner, Pusser, Woolaway-Bickel, & Preston, 2012). Yet, repeated use of FSBs in the context of false threats can contribute to the maintenance of heightened anxiety symptoms. Notably, FSBs are related to, but distinct from other anxiety-related constructs (e.g., worry; Buckner, Zvolensky, Businelle, & Gallagher, 2017). Consistent with fear-avoidance models of anxiety, FSB has been identified as a risk factor in the progression of anxiety symptoms and disorders. According to emotional processing models of fear (Foa & Kozak, 1986), there are two key elements needed for correction of pathological fear: (a) elicitation of fear and (b) provision of corrective information. FSBs such as avoidance necessarily limit exposure and activation of fear. Thus, the utilization of FSBs in the context of the phobic stimulus can detract from the acquisition of corrective knowledge. The use of FSBs among anxious individuals is related to greater anxiety, poorer performance, less favorable evaluation from others, and diminished treatment effects (Piccirillo, Dryman, & Heimberg, 2016).
False Safety Behavior Elimination Therapy (FSET) focuses on the elimination of FSBs to decrease anxiety and depression and improve quality of life. In a randomized clinical trial (RCT) of FSET, we found that post-treatment outcomes related to anxiety, depression, and clinician-rated severity were superior among FSET patients compared with waitlist controls (Schmidt et al., 2012). Importantly, gains were maintained at 6-month follow-up. FSET involves the identification and elimination of FSBs in anxiety disorders. FSET may be especially useful with patients with elevated anxiety who smoke given that learning that elimination of smoking as a safety behavior will help patients better manage their anxiety can help motivate them to change their smoking, as these patients are often motivated to change their anxiety (which is distressing) but not necessarily to change their smoking.
Several streams of growing empirical evidence suggest FSBs are highly theoretically relevant and clinically significant for better understanding smoking among persons with psychiatric vulnerabilities such as anxiety. Smokers, especially those prone to negative affect, are more apt to expect smoking to alleviate distress (e.g., Garey et al., 2018) and motivated to smoke to mitigate such distress (Bradford, Curtin, & Piper, 2015). Furthermore, such negative reinforcement smoking motives and expectancies have a high degree of clinical utility, being related to smoking initiation (Doran et al., 2013), dependence (Myers, MacPherson, McCarthy, & Brown, 2003), withdrawal (Langdon & Leventhal, 2014), and smoking cessation outcome (e.g., Wetter et al., 1999). Other work suggests coping motives are related to individual differences in affective vulnerabilities that undergird problematic use and impede smoking cessation, including negative affectivity (e.g., Wetter et al., 1994). Second, FSB is related to more severe substance use problems even after controlling for anxiety and substance use frequency (Buckner, Zvolensky, Businelle, et al., 2017), suggesting that those that use substances more frequently may engage in more maladaptive attempts to manage anxiety. Furthermore, FSB was significantly related to anxiety symptom severity and substance use severity, and anxiety symptom severity was indirectly (via FSB frequency) related to substance-related problem severity (Buckner, Zvolensky, Ecker, et al., 2017). The scientific knowledge base suggests that anxious individuals smoke to help manage their anxiety (e.g., Buckner, Farris, Schmidt, & Zvolensky, 2014); in other words, smoking is commonly used as a “FSB” for smokers, especially those with elevated anxiety.
Given that nicotine can produce acute anxiolytic effects, smokers with high anxiety may be more likely to return to smoking following a quit attempt, in part, to alleviate abstinence-induced increases in anxiety (e.g., Ditre, Zale, LaRowe, Kosiba, & De Vita, 2018). Thus, consistent with the fear-avoidance model of anxiety, reducing the reliance on FSB prior to a quit attempt may enable smokers to better manage their anxiety during the quit attempts (e.g., less severe and disabling anxiety, less likelihood of catastrophizing about anxiety, greater self-efficacy for anxiety coping). Consequently, these smokers may be less likely to rely on maladaptive anxiety coping skills (e.g., smoking), and therefore, less likely to return to smoking following a smoking cessation attempt.
Consistent with the notion that smoking cessation treatment that is personalized to the psychological needs of the client is needed (e.g., Banducci, Long, & MacPherson, 2015; Rath, Walitzer, & Deffenbacher, 2016), Treatment for Anxiety and Smoking Cessation (TASC) integrates FSET with CBT for smoking cessation to simultaneously treat smoking and anxiety disorders. TASC integrates CBT techniques designed to help patients quit smoking (e.g., refusal skills, coping with craving) with FSET skills designed to help patients learn to manage their anxiety (e.g., elimination of FSBs). TASC may also increase confidence to change anxiety and quit smoking as patients learn alternative, more adaptive coping skills to help them cope with anxiety and other high-risk smoking situations. TASC was developed after FSET was successfully integrated with CBT for CUD to successfully treat comorbid anxiety and cannabis use disorders (Buckner et al., 2019; Buckner, Ecker, et al., 2016). To illustrate the utility of TASC for smoking cessation patients with a variety of co-occurring anxiety disorders, we first provide an overview of TASC sessions and then present two case examples. Informed written consent was obtained for treatment and research purposes. These cases have been deidentified and some details of the cases have been changed to protect confidentiality.
TASC
TASC consists of eight sessions that integrate FSET for anxiety disorders with CBT for smoking cessation (Table 1). This approach differs from simultaneous treatments in which two evidence-based treatments are used at the same time without efforts to integrate them into a single treatment. Session 1: This session includes integration of the following FSET skills: Emotional processing model of anxiety and how it relates to smoking and Anxiety terminology. Therapists provide psychoeducation about anxiety and the emotional processing model of anxiety that provides the rationale for fading (reducing until eliminated) FSBs. In addition, the following CBT for smoking cessation topics are also covered: Provide reinforcement and support for quitting, Discuss past quit experiences, Set quit date, Initiate self-monitoring, and Relaxation. Session 2: How to identify false safety behaviors, Why eliminate false safety behaviors, and How to eliminate false safety behaviors. Therapists provide psychoeducation on FSBs along with rationale for eliminating them. FSB elimination begins with the identification and assessment of FSBs followed by a “fading” or reduction of these behaviors. From this session on over the course of treatment, a variety of categories of FSBs are reviewed and each week patients are asked to reduce such behaviors until all FSBs have been eliminated. This session also includes the following CBT for smoking cessation topics: Identify high-risk smoking situations, Alcohol and smoking, Abstinence violation effect, and Develop smoking-related coping strategies. Session 3: Substance use (including smoking) as a false safety behavior. Therapists introduce the concept of substance use generally and smoking specifically as FSBs and work with patients to develop a plan to eliminate the smoking as a FSB. Thus, they also incorporated the following CBT for smoking cessation topics: Enlisting social support to prepare to quitting smoking and Smoking self-help materials (Clearing the Air). Session 4: Phobic versus antiphobic attitude and Antiphobic exercises. Therapists provide psychoeducation about the anti-phobic attitude (i.e., facing one’s fears) and instructions for how to engage in antiphobic exercises. Anti-phobic exercises are behaviors that directly oppose the patient’s phobic tendencies (i.e., doing the opposite of what the anxiety response is motivating the person to do). Often, anti-phobic behaviors are fairly challenging for patients. However, these exercises can provide a potent disconfirmation of the false threats that are maintaining the anxiety problem. For example, anti-phobic behaviors for a patient with panic disorder might include going to work wearing a heavy sweater to bring on sensations of sweating and flushing. The goal of such exercises is for patients to learn that they are overestimating the consequences of the feared stimuli. Antiphobic exercises are often novel and challenging ways to gain disconfirming evidence of maladaptive automatic thoughts that maintain pathological anxiety. Each week following Session 4, patients are challenged to engage in relevant antiphobic activities. Given that these exercises could increase urge to smoke to manage elevated anxiety, the session also includes the CBT for smoking cessation topic, Coping with cravings and urges to smoke. Patients are encouraged to Continue fading false safety behaviors while adding antiphobic exercises. Session 5: Fading other types of false safety behaviors. Patients receive psychoeducation of other types of FSBs (e.g., idiosyncratic behaviors, such as wearing a certain outfit for “good luck”). Patients are also encouraged to Continue fading false safety behaviors and engaging in antiphobic exercises. The session also includes the following CBT for smoking cessation topics: Prepare for quitting, Nicotine patch, and Relaxation (review). Session 6: Quit week: Discussion of Quitting Experiences, Develop social support for nonsmoking, Relaxation (review). These CBT for smoking cessation topics are discussed in addition to Continue fading false safety behaviors and engaging in antiphobic exercises. Sessions 7 to 8: These sessions include the following CBT for smoking cessation topics: Provide support, Lifestyle changes, Relaxation (review), and Anticipate high-risk smoking situations along with Continue fading false safety behaviors and engaging in antiphobic exercises and Becoming your own therapist (i.e., relapse prevention).
Describes Skills Discussed Per Treatment Per Session.
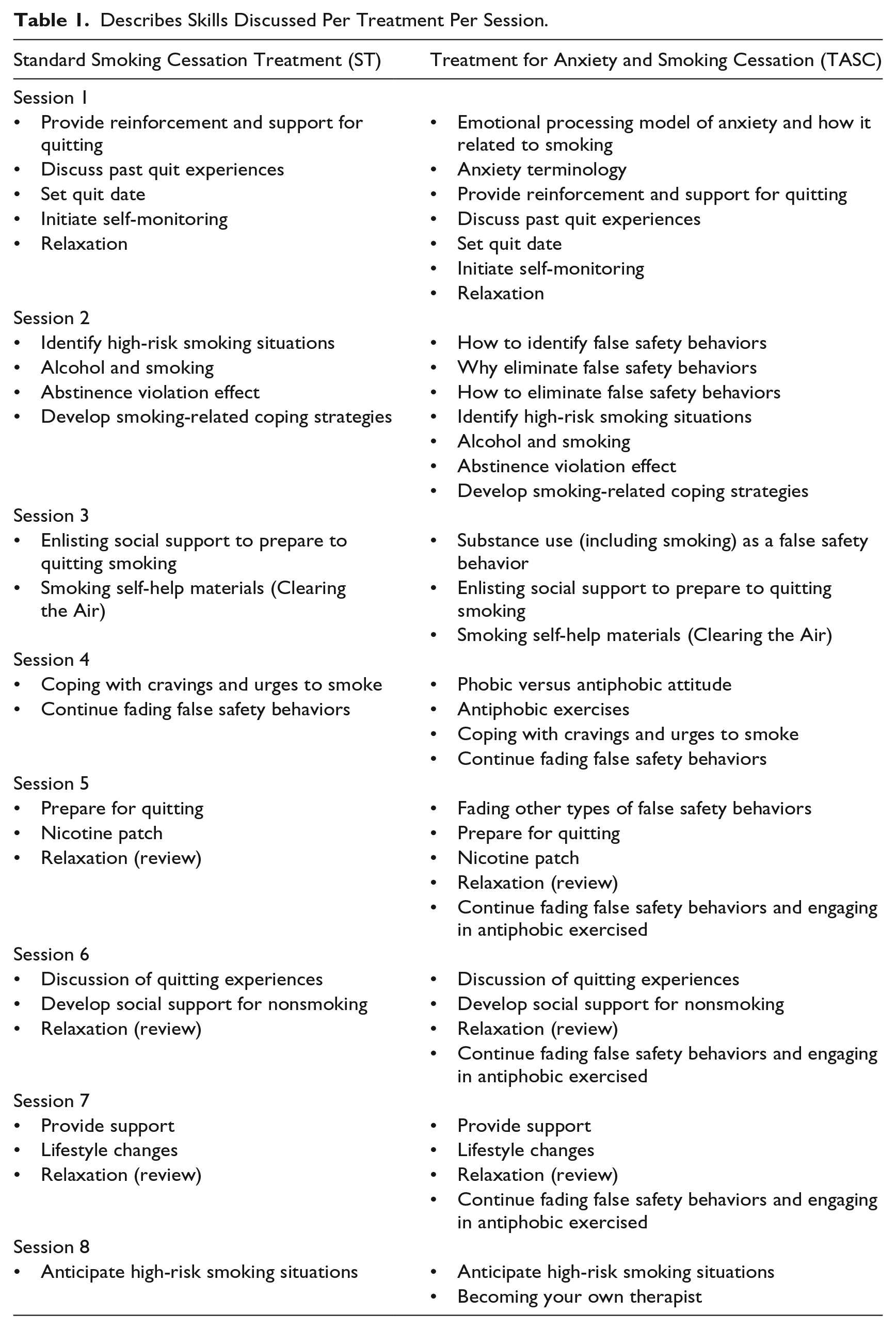
The FSET manual has been modified to best serve the unique needs of smoking cessation patients by (a) psychoeducation about the role of anxiety in maintaining smoking and asking patients to complete weekly self-monitoring forms of smoking as well as anxiety and depression. Patients are asked to indicate whether smoking was related to anxiety or other negative mood states. Collecting this information facilitates a continued focus on the functional relationship between anxiety, negative emotionality, and smoking that is introduced during initial TASC sessions (b) modifying vignettes and sample forms so they are relevant for smoking cessation patients with elevated anxiety. For example, when describing FSBs, vignettes illustrating cases of smoking as a FSB are included; (c) highlighting the importance of abstaining from smoking during FSB fading and antiphobic activities as well as offering specific strategies to do so that are consistent with the CBT approach (e.g., strategies to cope with cravings that may occur in anxiety-provoking situations); (d) pacing of introduction of skills (eliminating FSBs, antiphobic exercise) to prepare patients for quit day; and (e) including material on goal setting and termination that is most relevant to smoking cessation patients with elevated anxiety (e.g., forming new social connections with people who do not smoke).
Case Study 1: Co-occurring Tobacco Use Disorder (TUD) and GAD
1 Case Introduction
Patient A is a White woman originally from Spain in her 20s who presented to our university-affiliated outpatient clinic for the treatment of anxiety and smoking cessation.
2 Presenting Complaints
Patient A reported that she wanted to quit smoking but had difficulty quitting on her own. She made three prior attempts to quit smoking in the past 3 years and each attempt lasted no longer than 5 days. During the clinical interview, she reported that she often smoked to cope with her anxiety. She presented for treatment to learn to manage excessive anxiety and worry because it was interfering with several domains of her life. For example, she often had difficulty completing her schoolwork efficiently due to worry and often spent hours checking and rechecking her work for typos. Her reasons to quit smoking included to develop more adaptive ways to manage her anxiety and to improve her health.
3 History
Patient A reported a history of psychological treatment. From ages 15 to 17, she attended talk therapy weekly with a psychologist to manage symptoms related to her eating disorder (described below in Assessment section). She reported that she did not find that therapy was helpful because she did not feel comfortable disclosing personal information at that time. At the time she sought treatment at our clinic, Patient A attended talk therapy weekly at the on-campus student health center to manage symptoms related to her eating disorder. Patient A reported that she found talk therapy with her current counselor helpful because she was able to discuss her problems without judgment.
Patient A also reported a history of medical problems. Specifically, she was diagnosed with nighttime hypoglycemia a few years ago and took insulin medication nightly to manage her symptoms. She denied any functional interference associated with her hypoglycemia.
4 Assessment
A clinical interview was conducted by a doctoral student in clinical psychology and diagnoses were determined via a group consensus meeting with a licensed clinical psychologist.
The Structured Clinical Interview for DSM-IV Criteria–Patient Version with Psychotic Screen (SCID; First, Spitzer, Gibbon, & Williams, 2007) is a semistructured clinical interview for DSM-IV disorders, including anxiety disorders, mood disorders, substance use disorders, eating disorders, and psychosis. Additional questions were asked when appropriate to assess Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) criteria. Regarding GAD, Patient A reported that she experienced excessive anxiety and worry occurring more days than not since childhood about several events and activities (e.g., school, the well-being of her family, her career, her future). She reported that she had difficulty controlling the worry and that she worried most of the day nearly every day. Patient A also experienced the following symptoms associated with her anxiety and worry on most days: feeling physically restless or keyed up or on edge; difficulty concentrating, difficulty sleeping, and muscle tension. She reported that her anxiety interfered with her life in several significant ways (e.g., missed class several times due to worry, frequent back pain due to muscle tension). Patient A met DSM-5 criteria for GAD.
At intake, Patient A reported that for the past 3 years, she smoked 15 or more hand-rolled cigarettes per day. She typically smoked more cigarettes than she planned to and reported three unsuccessful quit attempts in the past few years. She reported that as a result of her smoking, she experienced a recurrent cough and decreased stamina, but that she continued to smoke despite the effects. She endorsed tolerance, strong cravings, and withdrawal (i.e., increased appetite, anxiety, headaches, irritability). Patient A met DSM-5 criteria for TUD, moderate.
Patient A also endorsed history of major depressive episodes. Her most recent major depressive episode last for 3 months and ended approximately 2 months before she presented for intake. At intake, she continued to experience some depressive symptoms (e.g., depressed mood, loss or interest or pleasure in activities, insomnia), but denied that these symptoms occurred more days than not. She experienced symptoms of a depressive episode at age 18, but was unable to provide further specific details about the length of the episode or symptoms she experienced. Patient A met DSM-5 criteria for major depressive disorder, recurrent episode, in partial remission.
Patient A also endorsed a history of recurrent episodes of binge eating during which she would eat an amount of food that was larger than most people would eat in a similar period of time under similar circumstances (e.g., a half a loaf of bread, half a box of cereal in one sitting) as well as a lack of control over eating during these episodes. From ages 15 to 17, she binged almost daily and engaged in recurrent inappropriate compensatory behaviors (i.e., excessive exercise, taking laxatives). From ages 17 to 24, she binged and/or engaged in inappropriate compensatory behaviors less than once per week. At intake, she reported a 1-month period in the past year during which she binged and excessively exercised 3 to 5 times per week. She denied binging or engaging in inappropriate compensatory behaviors in the month prior to intake. Patient A met DSM-5 criteria for bulimia nervosa, in partial remission.
The Hamilton Anxiety (HAM-A; Hamilton, 1959) and Depression (HAM-D; Hamilton, 1960) scales are widely used structured clinical interviews of anxiety and depression. At intake, Patient A scored a 22 on the HAM-A, indicating moderate to severe levels of anxiety (Hamilton, 1959) and a 17 on the HAM-D, indicating mild to moderate levels of depression (Hamilton, 1960).
The Overall Anxiety/Depression Severity and Impairment Scales (ODSIS; Bentley, Gallagher, Carl, & Barlow, 2014; OASIS; Norman, Hami Cissell, Means-Christensen, & Stein, 2006) are brief, five-item self-report measures of anxiety/depression symptoms and related impairment. Both the OASIS and ODSIS have demonstrated validity, diagnostic specificity, and sensitivity to change after treatment. At intake, Patient A scored a 11 on the OASIS, indicating clinically elevated anxiety (Norman et al., 2006), and a 12 on the ODSIS, indicating clinically elevated depression (Bentley et al., 2014).
5 Case Conceptualization
TASC was recommended to treat Patient A’s GAD and to help her quit smoking. By the patient’s report, she often smoked to manage her anxiety.
6 Course of Treatment and Assessment of Progress
Patient A quit smoking and experienced clinically significant reductions in anxiety during TASC. The first two sessions were comprised mainly of diagnostic feedback and treatment rationale, motivational interviewing (MI; Miller & Rollnick, 2013) focused on smoking-related behavior, and psychoeducation about anxiety. MI consisted primarily of presenting the patient with personalized feedback related to her smoking and exploring and resolving ambivalence regarding quitting smoking. Psychoeducation primarily consisted of information on anxiety and fear structures. In Session 3, Patient A identified FSBs in which she engaged in, including re-checking already-completed tasks, checking texts and emails repeatedly before sending them, avoiding being late, and smoking cigarettes. The therapist explained how engaging in such FSBs maintain anxiety disorders, and that by gradually decreasing their use, Patient A will begin to change the associations between feared stimuli and the anxiety response. Patient A began to fade these FSBs for homework and fading FSBs was assigned for homework for all following sessions. She also identified alternative coping strategies she could use instead of smoking, including exercise and using distracting activities (e.g., drink a glass of water). Session 4 integrated functional analysis of smoking with discussions of smoking as a FSB, facilitating Patient A’s understanding of her particular smoking patterns (both coping and noncoping motivated use) as well as positive/negative consequences of smoking. In Session 5, Patient A’s smoking had reduced from 15 or more cigarettes daily to 10 to 15 cigarettes daily (Figure 1). Patient A discussed how understanding her smoking patterns helped her reduce the number of cigarettes smoked per day. To illustrate, she noted that she often smoked when she studied outside. She chose to study indoors and noticed a reduction in smoking. Also in Session 5, antiphobic exercises were introduced, and the patient gave several examples of antiphobic exercises she could conduct (e.g., raising her hand and saying something incorrect in class, sending an email with a typo). To help Patient A prepare for quit day (Session 6), the therapist discussed benefits of nicotine replacement therapy (NRT), encouraged Patient A to purchase nicotine patches, and reviewed proper application of the patch. Other quit strategies were reviewed, such as identifying maladaptive automatic thoughts related to smoking.
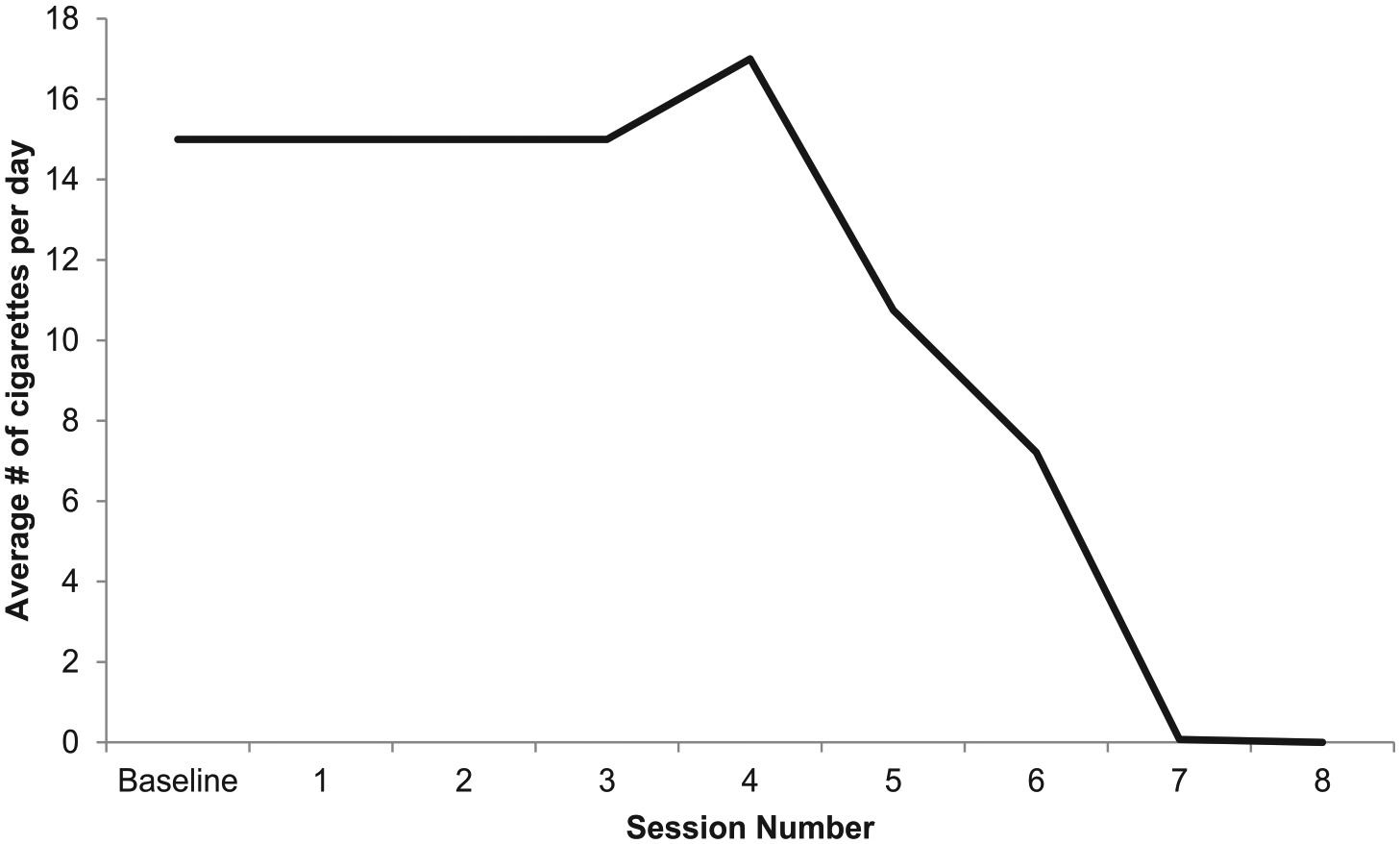
Average number of cigarettes smoked per day in past week for Patient A.
In Session 6 (Quit Day), Patient A reduced her smoking to three cigarettes per day. She purchased nicotine patches and used her first one earlier that day. She reported that her craving and withdrawal symptoms (i.e., irritability, difficulty concentrating) were intense and difficult to manage. She reported that she found distraction techniques (e.g., chewing gum) helped her avoid smoking. She also reported that she tried to spend more time with nonsmokers and told her friends who smoke that she is quitting. Patient A reported some hesitation about quitting and time was spent in session on identifying and challenging maladaptive thoughts related to quitting. Patient A reported experiencing several benefits of fading and antiphobic exercises after completing these exercises for homework for several weeks, including discovering that situations she would normally avoid (e.g., being late to class, speaking up in class) were not nearly as threatening as she originally believed they were and completing tasks on her to-do list rather than procrastinating due to worry (e.g., turning in homework assignments, applying to jobs). She also reported feeling frustrated that she had spent so much time in the past worrying about these different situations when they were “no big deal.” Exposure to anxiety-provoking stimuli via fading FSBs assisted the patient to engage in self-facilitated cognitive restructuring and motivated her to continue to engage in fading FSBs and antiphobic exercises to reduce her anxiety. Relaxation strategies were also discussed (i.e., urge surfing, diaphragmatic breathing).
In Session 7, Patient A reported smoking 1 cigarette in 2 weeks and noted that the NRT helped her manage her withdrawal symptoms. She noted that she smoked in a high-risk situation (e.g., drinking alcohol). Patient A reported using relaxation techniques to manage her anxiety and continued benefits from fading FSBs. Positive changes due to quitting (e.g., improved breathing during exercise), barriers to quitting (e.g., being at bars around others who smoke), and the importance of making lifestyle changes to reduce the impact of high-risk situations (e.g., avoiding situations she used to smoke in) were discussed.
In Session 8, Patient A denied smoking any cigarettes since Session 7. Patient A identified possible high-risk situations (e.g., school-related stress) and alternative ways to cope (e.g., take a walk, call a friend). She expressed pride in eliminating her FSBs and in quitting smoking. She reported that using self-talk was helpful for avoiding smoking. To illustrate, when she experienced cravings she would tell herself, “I’ve worked so hard to this point—I don’t want to waste my time and willpower.” She also reported decreased avoidance (e.g., paying bills, going to eat with friends) and increased self-efficacy to manage anxiety.
7 Complicating Factors
Patient A canceled and rescheduled three sessions due to illness, injury, or running late. Patient A also continued to attend regular concurrent treatment at the Student Health Center for her eating disorder during TASC. Some of her eating disorder symptoms were also related to her smoking. To illustrate, Patient A reported that a perceived benefit of smoking was appetite suppression and she initially expressed worry about gaining weight if she quit smoking. To address these concerns, therapist presented psychoeducation on weight gain following a quit attempt, and Patient A reported that she believed that even if she gained some weight if she quit smoking, quitting smoking would be the healthiest option for her overall. She endorsed minor weight gain after quitting, but reported that she was not overly concerned about the weight gain. Furthermore, she was able to generalize her skills to her eating disorder symptoms and eliminated FSBs related to her fear of weight gain. To illustrate, she identified that she used FSBs (i.e., wearing the same clothes to every appointment, not eating or drinking anything prior to appointment) to manage anxiety prior to weighing herself during her weekly nutritionist appointment; she then eliminated these FSBs in the context of TASC.
8 Access and Barriers to Care
Patient A endured an ankle injury during treatment which was related to a brief increase in depressive symptoms that lasted a few days and self-reported difficulties with completing assigned homework. However, this did not seem to interfere significantly with progress as the patient still completed assignments and attended sessions.
9 Follow-Up
During the course of treatment, Patient A made marked improvements concerning her anxiety, depression, and smoking. Regarding her anxiety, her OASIS score decreased from the clinical range at intake (11) to below the clinical cut score (Norman et al., 2006) at termination (6) and her HAM-A score decreased from the moderate to severe range at intake (22) to the mild range (5) at termination (Hamilton, 1959). She reported experiencing excessive and difficult-to-control worry and anxiety only 1 to 2 days per week in the past month at termination compared with daily excessive worry at intake. During the 24 days preceding termination, Patient A smoked one cigarette (12 days prior to her final session), representing a significant reduction from 15 or more cigarettes per day at intake (Figure 1). Furthermore, she reported experiencing only two TUD symptoms (craving and withdrawal symptoms) in the past month at termination. In fact, Patient A no longer met DSM-5 criteria for GAD. She continued to meet DSM-5 criteria for TUD, as she had experienced withdrawal and craving in the past month at termination. Her depression also decreased as evidenced by a decrease on the ODSIS from clinical range at intake (12) to below clinic cut score (Bentley et al., 2014) at termination (7). Furthermore, scores on the HAM-D decreased from the moderate to severe range at intake (17) to the mild range (6) at termination (Hamilton, 1960).
Consistent with prior case studies (Stewart et al., 2016), treatment outcomes were assessed using three indicators of individual-level change: the Reliable Change Index (RCI; Evans, Margison, & Barkham, 1998); clinically significant change cutoff scores, a more exacting index of change compared with the RCI (Evans et al., 1998); and reliable changes defined as being equal to or exceeding a decrease of 50% in a given behavior (e.g., Stewart et al., 2016). To calculate RCI, the SD and r were drawn from the literature because these data are based on two patients, which is consistent with prior small sample size studies (e.g., Stewart et al., 2016). Patient A’s scores on the ODSIS were deemed reliably improved based on the RCI. Next, clinically significant change scores identify scores within the healthy population range. Based on this criterion, Patient A’s scores on the HAM-A, HAM-D, and OASIS were deemed clinically significant. Last, for single-item measures where reliability cannot be calculated, reliable change can be identified as those equal to or above a 50% decrease in a given behavior (i.e., number of cigarettes). Patient A evidenced reliable change in the average number of cigarettes per day, given her 100% decrease. Overall, Patient A displayed significant improvements from pre-to post-treatment on all anxiety, depression, and smoking outcome measures.
Theoretical and Research Basis for Treatment
The utility of TASC for smoking cessation with a patient with clinically elevated social anxiety that did not meet DSM-5 threshold for an anxiety disorder is illustrated here.
Case Study 2: Smoking Cessation With Patient With Elevated Social Anxiety
1 Case Introduction
Patient B was a White woman in her 30s who presented to our hospital-affiliated outpatient clinic with a strong desire to manage her anxiety and quit smoking.
2 Presenting Complaints
Patient B reported clinically elevated anxiety in social situations and difficulty controlling her worries. The patient expressed a desire to manage her anxiety so that she could feel better throughout the day and stop relying on cigarettes to relax. She also reported that she was avoiding telling her husband that she had not quit smoking (despite telling him that she quit a year ago), and that she did not want to continue being dishonest with him.
3 History
Patient B endorsed a history of anxiety and distress related to social anxiety and worry that was difficult to control. She reported a history of avoiding social situations that increased her anxiety and related distress in social anxiety provoking settings. Patient B reported that she had not sought psychotherapy for anxiety or smoking in the past. Regarding medical history, she reported that she experiences upper back/neck tension due to anxiety, and she reported smoking to manage the anxiety-related tension.
4 Assessment
As with Patient A, the SCID (First et al., 2007) was used to assess DSM-5 criteria Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013). Patient B reported that she experienced excessive fear and anxiety in several situations (e.g., trying to make new friends). She reported that she experienced anxiety nearly every time she experienced the above situations and that she believed the fear was excessive. She reported experiencing this anxiety for as long as she could remember. She also reported anticipatory anxiety prior to engaging in these situations. Patient B often avoided some of these situations (e.g., avoided telling her husband about her cigarette use). Despite this avoidance, Patient B denied experiencing clinically significant levels of distress or impairment due to her anxiety, and thus did not meet DSM-5 criteria for social anxiety disorder.
Patient B met DSM-5 criteria for TUD, moderate. She stated that for the past 10 years, she smoked up to 28 cigarettes per day. She reported that she often smoked more than she was planning to, and often smoked cigarettes rather than engaging in other planned activities (e.g., preferring to smoke instead of spending time with her husband and children). She endorsed tolerance, strong urges to use, and withdrawal symptoms (e.g., increased anxiety) when she used tobacco less often.
Because this patient was treated by a different clinician, different measures were used by the clinician to monitor treatment progress. The State-Trait Anxiety Inventory (STAI; Spielberger et al., 1983). The STAI is a 40-item measure used to identify clinically elevated levels of state anxiety and trait anxiety levels. This measure has shown good to excellent internal consistency. Patient also reported clinically elevated scores on the STAI at intake (STAI-S: 56, T: 62). Patient B completed the STAI at the beginning of treatment and at termination and completed a self-monitoring assessment of her cigarette use weekly during treatment.
5 Case Conceptualization
TASC was recommended to treat Patient B’s clinically elevated anxiety and TUD. During the clinical interview, Patient B reported that she smoked to cope with negative emotional states, including anxiety and boredom. She also reported smoking to relax and to be social with friends. She also reported smoking prior to and during social encounters to cope with anxiety-related cognitions (e.g., fear of negative evaluation, worrying about completing daily tasks).
6 Course of Treatment and Assessment of Progress
The skills presented in each of the nine sessions were presented in the same order as for Patient A. The first two sessions focused on psychoeducation, during which Patient B also reported many reasons to quit smoking, including to be more present with her family, to expand her social life to people who do not smoke, and to reduce her anxiety. By Session 2, Patient B was able to identify other FSBs that she used to cope with anxiety (e.g., avoiding confrontation). Also in Session 2, the patient was asked to discuss new coping strategies as alternatives to smoking as a safety behavior. She readily identified actions and lifestyle changes that would be more adaptive, such as staying more active and using Wellbutrin to help manage tobacco cravings (which she started taking the same day as Session 2). Although use of an NRT during treatment was recommended, Patient B reported that she did not want to use an NRT to manage cravings, as she wanted to use Wellbutrin during treatment to reduce cravings. She stated that she was excited to use these alternative coping strategies.
In Session 3, additional FSBs were identified. Patient B stated that she smoked to cope with anxiety, avoided situations such as new social situations when she was unable to smoke, engaged in reassurance seeking at work, and checked her belongings ritualistically (e.g., phone). She also identified alternative coping strategies to smoking, including reminding herself of the positive and negative consequences of use, distraction, using positive self-talk, and daily goal setting and creating a reward schedule when goals are met. By Session 7, the patient demonstrated successfully fading all FSBs (e.g., going to work and not smoking before, during, or immediately after work).
During Session 5, antiphobic exercises were added as a weekly homework assignment. The patient understood the purpose of the exercises; however, she was hesitant to engage in these exercises due to her extreme fear of facing her fears. The therapist worked with the patient to develop antiphobic exercises in which she was willing to engage. The patient feared being negatively evaluated for her work and she was initially unwilling to present a project (either at work or personal life) that could evoke negative evaluation (e.g., present a project for the neighborhood program that has a small mistake). Thus, she initially made very small changes to her projects (e.g., writing letters on a sign messier on purpose). When the patient made gains in fading avoidance, asserting her right to quit smoking with friends, and completing antiphobic exercises, she reported feeling very proud of herself, and she was excited to share her successes during treatment sessions. For the remaining sessions (Sessions 5-10), fading safety behaviors and completing antiphobic exercises were discussed.
Following Session 5, Patient B reported that she was happy with her overall progress, although she felt somewhat guilty about her continued smoking. She reported that the intention of her continued use was not to manage anxiety, but because “it was a habit” rather than to decrease anxiety or cope with stress. She stated that she had smoked with friends when it was offered to her because she found it to be enjoyable; however, she stated that she was still motivated to quit smoking, and an additional therapy goal was set for Patient B to tell her current friend group that she was no longer smoking. She stated that daily goal setting with the reward schedule and reminding herself of the positive and negative consequences of smoking were the most effective strategies to cope with cravings and deal with high-risk situations.
The final session consisted of relapse prevention. High-risk situations were identified and discussed as opportunities to become her own therapist, implement problem-solving techniques, and cope with high-risk situations related to anxiety/boredom and smoking. Patient B reported feeling more confident to deal with fading FSBs and problem solving during high-risk smoking situations.
During the course of treatment, Patient B made marked improvements concerning her anxiety and smoking. Regarding her anxiety, her STAI score decreased from the clinical range at intake (State: 56, Trait: 62) to below the clinical cut score at termination (State: 36, Trait: 34). Furthermore, from Session 8 until 1 month post-termination, she reported continued abstinence from smoking and no additional problems related to smoking.
7 Complicating Factors
Patient B’s treatment was complicated by a few factors. For example, during Session 5, Patient B reported decreased smoking; however, an initial increase in other safety behaviors was noted as smoking decreased (e.g., phone checking, perfectionistic behaviors). The therapist assessed the increase in other safety behaviors during weekly monitoring forms and brought this increase in safety behaviors to the patient’s attention. The patient acknowledged that she was engaging in behaviors geared toward avoidance of her anxiety and reported that she did not want to introduce new safety behaviors. She reduced these behaviors by identifying them as FSBs and incorporating them into her self-monitoring homework to fade and eventually eliminate these behaviors. Furthermore, Patient B reported that she preferred to continue to use Wellbutrin to help manage her cravings, despite continued cravings on Wellbutrin, and refused to use NRT as recommended during treatment.
8 Access and Barriers to Care
There were no significant barriers to treatment for Patient B. Factors that could become barriers to care (e.g., taking time off work for treatment and avoiding talking with boss about taking this time) were addressed early in treatment and did not present as a significant barrier to treatment.
9 Follow-Up
Throughout treatment, smoking reduced considerably (Figure 2), with triggers including availability of cigarettes, friends smoking in front of her, stress, and other high-risk situations (e.g., being in the car alone, being at a coffee shop). Notably, she smoked several cigarettes per occasion on the majority of times she used at intake. Frequency of smoking decreased from daily at intake to no smoking from Session 8 to termination (Session 10). At termination, she denied past-month problems related to her tobacco use and her STAI score was below the clinical cut score at termination (State: 36, Trait: 34). During a 1-month posttreatment follow-up phone call, Patient B reported that she remained abstinent from cigarette use and given her treatment gains, the patient was considered in remission for TUD. Using indicators of individual-level change, Patient B demonstrated significant improvements from pre- to post-treatment on all anxiety and smoking outcome measures. Patient B’s scores on the STAI-S and STAI-T were clinically significant based on the clinical cutoff score criteria, the more stringent index of change. Patient B also evidenced reliable change given her 100% decrease in the greatest number of cigarettes per day exceeding the cutoff of at least a 50% decrease in a given behavior criterion.
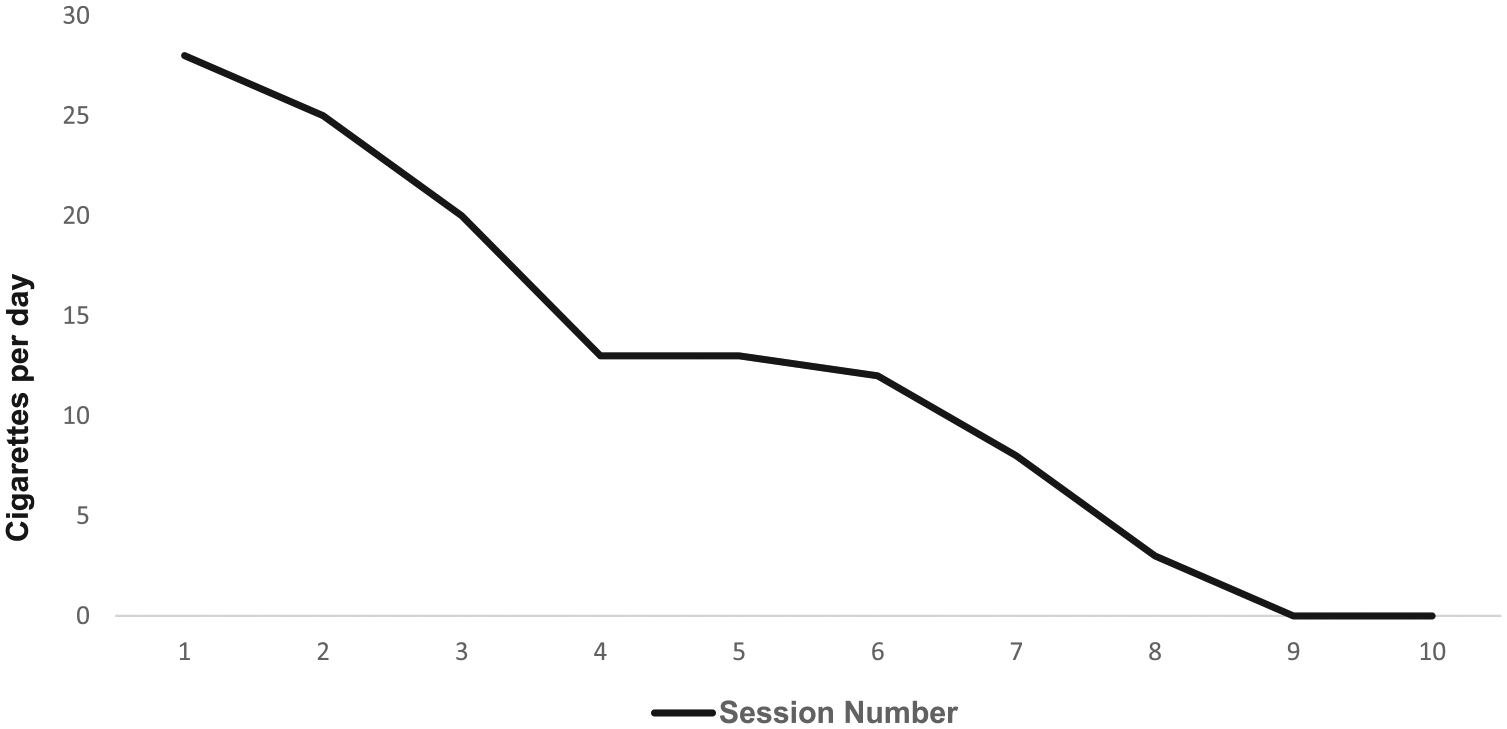
Number of cigarettes used on greatest smoking day in past week per daily self-monitoring homework for Patient B.
Treatment Implications of the Cases
Although preliminary, these case reports point to the potential utility of TASC, an integrated psychosocial treatment that integrates FSET for anxiety disorders (Schmidt et al., 2012) with CBT for smoking cessation patients with clinically elevated anxiety. In the context of TASC, these two patients quit smoking and decreased their anxiety. Importantly, these patients quit smoking despite smoking daily at intake. Also, Patient A experienced remission of her anxiety disorder, despite not responding to previous psychosocial treatment and Patient B quit smoking despite not responding to pharmacological treatment for smoking cessation. Furthermore, our data suggest that patients who received TASC may experience decreased depressive symptoms. Importantly, Patient A met her treatment goals despite comorbid psychopathology and Patient B met hers despite her refusal to use NRT to help her manage her cravings while simultaneously confronting anxiety-provoking situations. These data are therefore very promising, especially when considering data suggesting that co-occurring anxiety results in poorer smoking cessation outcomes (e.g., Hall et al., 1994).
Providing patients with skills to manage their smoking cravings and high-risk smoking situations while simultaneously teaching them skills to manage their anxiety is a unique strategy of this treatment and it shows great promise. The manual was developed such that techniques from FSET (Schmidt et al., 2012) could work in concert with those from CBT for smoking cessation to increase motivation to quit smoking while also targeting the patient’s clinically elevated anxiety. The clinical improvement shown by the two patients in our case studies suggest that TASC may be a promising treatment for patients seeking smoking cessation treatment who are also interested in learning to better manage their anxiety symptoms. Future work would benefit from randomized controlled trials to test efficacy, retention, and long-term effects of TASC on smoking, anxiety, and associated negative emotional symptoms (e.g., depression). Future work is also necessary to test whether TASC can be used to increase motivation to quit among smokers with elevated anxiety who are not motivated to quit smoking.
It is also notable that FSET skills have been integrated into MI-based CBT for cannabis use disorder (Steinberg et al., 2005) to treat co-occurring CUD and anxiety disorders (Buckner, Zvolensky, et al., 2014). That integrated treatment resulted in decreases in anxiety and cannabis use in case studies (Buckner, Ecker, et al., 2016) and a pilot RCT (Buckner et al., 2019). When considered in light of the current data, it appears that FSET is a transdiagnostic anxiety treatment that can be readily integrated into extant CBT manuals for substance use disorders to simultaneously treat substance use and anxiety disorders.
Recommendations to Clinicians and Students
Per the TASC protocol, initial session began with psychoeducation about the nature of anxiety as well as the relationship between each patient’s type of anxiety (e.g., social anxiety, generalized anxiety, panic) and smoking. It is also important to note in the initial sessions that not all smoking will be for anxiety management. As evidenced in the case of Patient B, some smoking will be for other reasons (e.g., to be social with friends). Thus, it is important to teach patients not only skills to manage their anxiety without smoking but also ways to manage cravings that occur in other, non-anxiety-related, high-risk smoking situations.
It is noteworthy that TASC resulted in decreases in anxiety and smoking in eight to 10 sessions, despite most anxiety treatment protocols recommending at least 10 sessions of treatment to address pathological anxiety (e.g., Zinbarg, Craske, & Barlow, 2006). Although 10 sessions is longer than typical smoking cessation protocols, the additional session are necessary to incorporate anxiety management techniques into CBT for smoking cessation and is consistent with the notion that comorbidity can result in a longer course of treatment. This longer treatment “dose” resulted in abstinence from smoking for both patients despite daily smoking and meeting DSM-5 criteria for TUD with moderate severity at intake.
In sum, although RCTs are warranted to test the efficacy of TASC for anxiety and smoking cessation, data from these initial case studies are promising. The excellent response demonstrated by these patients suggests that integrating FSET with CBT for smoking cessation may be useful in helping anxious patients achieve abstinence from smoking while simultaneously learning to manage their chronically elevated anxiety. Given that nearly one fourth of individuals with TUD suffer from at least one comorbid anxiety disorder (Grant et al., 2004) combined with data that these patients have more severe pathology and poorer outcomes (e.g., Hall et al., 1994), treatments aimed at decreasing co-occurring negative affect and associated functional impairment while achieving abstinence from smoking has the potential to benefit a great many patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.