
Abstract
Social Anxiety Disorder (SAD) is a condition defined by an excessive and persistent fear of negative evaluation in social or performance situations. Whilst Cognitive Behaviour Therapy (CBT) is the gold standard treatment, not all individuals with SAD respond to CBT. The Schema Therapy Mode Model is frequently applied to chronic and hard-to-treat conditions and therefore may be applicable for SAD individuals who are non-responders to CBT. This case study describes how the Mode Model was successfully used to treat a woman in her 20s who presented with excessive fears of negative evaluation and pervasive social avoidance. Experiential techniques, such as chair dialogues and imagery rescripting, resulted in cognitive modification of negative core beliefs, reduced experiential discomfort and increased engagement in social and relational activities. This case offers a preliminary indication that the Schema Therapy Mode Model may be an effective treatment for socially anxious individuals and that further theoretical and empirical study in this area is warranted.
1 Theoretical and Research Basis for Treatment
Social Anxiety Disorder (SAD) is defined by an excessive and persistent fear of negative evaluation in social or performance situations (Diagnostic and Statistical Manual 5th Edition (DSM-5); American Psychiatric Association (APA, 2013)). The psychological, economic and community impact of SAD is significant given it is the fourth most common psychiatric disorder (Australian Bureau of Statistics, 2007), has an earlier onset than other anxiety disorders, takes a chronic course and has a low incidence of spontaneous remission (Beesdo-Baum et al., 2012; Bruce et al., 2005).
Cognitive Behaviour Therapy (CBT) is considered the gold standard treatment for SAD (Mayo-Wilson et al., 2014); however, there are a proportion of SAD patients who do not improve with CBT or maintain gains, with most continuing to experience residual symptoms post-treatment (Heimberg, 2002; Mörtberg et al., 2011; Rodebaugh et al., 2004). Factors predictive of poor CBT prognosis include the significant comorbidity associated with SAD including depressive disorders, other anxiety disorders, substance use disorders and personality disorders (Crome et al., 2010; Heimberg, 2002; Rodebaugh et al., 2004).
Recent empirical focus on aetiological factors in SAD, for example, peer social traumas, critical or over-controlling parenting styles, insecure attachment and childhood emotional maltreatment (Norton & Abbott, 2017; Spence & Rapee, 2016), is likely to improve SAD treatment specificity and prognosis. Schema Therapy (ST; Young, 1999; Young et al., 2003) may provide a helpful framework for extending the clinical understanding and treatment of SAD because of its emphasis on the aetiology of symptoms and defence mechanisms. Whilst ST has traditionally been applied to personality disorders (Bamelis et al., 2011), there is emerging research that it may be helpful for other clinical conditions, such as depression (Renner et al., 2013), eating disorders (Simpson et al., 2010) and post-traumatic stress disorder (Grunert et al., 2007). Schema Therapy’s integration of aetiological factors and its implementation of cognitive, behavioural and experiential techniques may provide an efficacious alternative for individuals who do not make or maintain gains with CBT (Arntz & Jacob, 2013).
Originally, ST focussed on early maladaptive schemas (EMSs), which have been described in the literature as pervasive life patterns that develop in response to unmet childhood needs (Arntz & Jacob, 2013; Young, 1999). Eighteen recognized EMSs are theorized to develop within five domains of childhood experiences: Disconnection and rejection, impaired autonomy and performance, impaired limits, other-directedness and over-vigilance and inhibition. Early ST treatments focussed on reducing core EMSs that underlie pervasive symptoms and maladaptive life patterns (Arntz & Jacob, 2013; Young, 1999).
Empirical evidence supports a strong association between SAD and the EMSs within the disconnection and rejection domain, particularly defectiveness/shame and social isolation EMSs (Calvete, 2014; Calvete et al., 2018, 2013; Mairet et al., 2014; Pinto-Gouveia et al., 2006), which stem from childhood unmet needs when faced with humiliation, defectiveness and a lack of belonging.
The Mode Model is an updated iteration of ST, which emphasizes the conceptualization of state-based modes rather than trait-based EMSs, which may be more easily identified and addressed compared to EMSs (Arntz & Jacob, 2013). There are four recognized categories of schema modes: (1) Dysfunctional Child Modes (categorized by the experience of intense negative emotions in response to the perception of unmet needs); (2) Dysfunctional Critic Modes (internalized demanding or punitive criticism); (3) Dysfunctional Coping Modes (attempts to avoid, surrender to or overcompensate for the negativity of the Critic Modes or distress of the Child Modes) and (4) Healthy Modes (including an adaptive Healthy Adult Mode and a joyful Happy Child Mode; Arntz & Jacob, 2013; Farrell & Shaw, 2018; Young et al., 2003).
Cognitive (i.e. restructuring), behavioural (i.e. pattern breaking), relational (i.e. limited re-parenting) and experiential (i.e. chair dialogue and imagery rescripting) techniques are used in ST to set limits to critic modes, meet the needs of child modes, replace maladaptive coping modes and enhance the resources of healthy modes (Arntz & Jacob, 2013). Empirical research to date has focussed on ST’s application to personality disorders (e.g. Arntz et al., 2005; Bamelis et al., 2011; Lobbestael et al., 2008). However, the efficacy of ST for complex, comorbid and trauma-based disorders is indicative of its possible efficacy for chronic or comorbid SAD, particularly where an aetiological relational trauma is present, and may provide a novel treatment avenue for CBT non-responders.
Whilst there is emerging research on EMSs associated with SAD, the authors are aware of only one study that has explored schema modes associated with SAD (Norton et al., 2021, under review). Individuals with SAD were more likely to endorse Punitive Critic, Compliant Surrender, Detached Self-Soother and Vulnerable Child modes (Norton et al., 2021; under review). The authors hypothesized that parental over-control may cultivate an early shaming Punitive Critic, which along with experiences of social and relational trauma contributes to the development of an anxious Vulnerable Child. It is theorized that avoidance and compliance-based coping modes help individuals to avoid, distract or resign to anxiety and protect against the intense emotional distress of the child mode. Due to the dominance of these dysfunctional modes, individuals with SAD may have less capacity for the joy associated with Happy Child and resourcefulness associated with Healthy Adult (Norton et al., 2021; under review).
Given this exploratory evidence for a coherent ST mode conceptualization, there is reason to believe that ST may be a useful alternative treatment for SAD warranting further theoretical and empirical investigation. Of particular relevance is the link between aetiological factors, such as social trauma, and the later development of SAD, which is not directly targeted in CBT (Norton & Abbott, 2016a, 2016b). Moreover, there is evidence that imagery rescripting (a component of ST) is efficacious in reducing SAD symptoms and comorbid low mood (Norton & Abbott, 2016b), providing further support for exploratory investigations of ST for social anxiety. Imagery rescripting aims to restructure maladaptive interpretations developed from early negative interpersonal experiences and thereby reduce subsequent SAD symptoms (e.g. Knutsson et al., 2020; Lee & Kwon, 2013; Norton & Abbott, 2016b; Wild et al., 2008).
The clinical goals of ST for SAD are to help the patient defuse from the self-criticism of Punitive Critic, reduce the reliance on maladaptive coping modes for anxiety management, meet the previously unmet needs of Vulnerable Child and increase the adaptive problem-solving and emotion regulation abilities of the Healthy Adult. The purpose of the present article is to illustrate this novel treatment approach via a clinical case study.
2 Case Introduction
The patient’s personal characteristics have been omitted or altered to protect patient confidentiality in line with APA ethical guidelines; however, clinical symptoms and information relevant to the clinical aspects of assessment, treatment and outcomes remain intact. Jill (pseudonym) was a Caucasian woman in her early 20s. Jill was a full-time university undergraduate student majoring in arts and humanities subjects. Her partner had recently ended a 12-month romantic relationship with her.
The treating clinician (and first author) was a female clinical psychologist with a doctoral degree in clinical psychology and formal training in ST.
3 Presenting Complaints
Jill described difficulties with anxiety in social and novel situations. She described anxiety when meeting new people, going on dates, asking questions in class and giving presentations. She reported fears of negative evaluation in these situations, particularly that others would find her ‘unlikable’ and ‘boring’. She described how she would manage these fears with situational avoidance (e.g. not speaking in class or cancelling social plans) or with distraction and self-soothing (e.g. pretending to use her phone or consuming alcohol to reduce the experience of anxiety). She reported, however, that she had a close group of friends with whom she did not feel anxious and could speak freely about her difficulties with them.
Whilst she described episodes since adolescence where she had experienced periods of increased social anxiety, the current episode had begun 5 months ago, after her partner of 12 months had ended the relationship. She had interpreted this ending as being the result of being an ‘unlovable’ and ‘unlikable’ person.
More recently, Jill described that over the last month, she had started to feel depressed for most of the day. She described believing that she was ‘hopeless’, which combined with the low mood, caused the beginning of a lethargy cycle. Whilst she was still managing to complete necessary university and essential tasks, she had been finding it harder to complete enjoyable tasks or see her close friends. She reported that this had prompted her to seek therapy.
Jill reported a strong sense of cognitive–affective dissonance, where she reported that a part of her knew that she was liked and accepted by her close friends, and yet she still felt as if she were an inherently unlikable person. Given this, along with her comorbid depression, and history of reoccurring episodes of social anxiety, the rationale for ST was presented to Jill. It was explained that many of the components of CBT (the current accepted gold standard for SAD) would still be utilized but that ST would provide an opportunity for more experiential re-learning that may help to close the gap of what she knew versus felt to be true. Jill identified strongly with the idea that she had experienced long-standing difficulties and reported motivation to engage in a more experiential treatment approach.
4 History
Jill had reportedly experienced social anxiety and low mood symptoms since early adolescence. She described a father prone to self-criticism and a mother who valued control and certainty. She reported her mother’s parenting style was overly protective and she was often encouraged to stay home rather than face anxiety-provoking situations. She reported a family history of anxiety and mood disorders and described early interpersonal traumas of social exclusion, rejection and isolation from peers at school. Of note was an experience in early adolescence when she felt ostracized from a previously close friend and reportedly believed this had occurred because she ‘did not belong’, was ‘unlikable’ and ‘less interesting’ than the new friends this person had made. She described this as the onset of socially anxious fears.
5 Assessment
Jill’s presenting complaints and psychosocial history were assessed through a semi-structured interview. The clinical interview process determined that Jill met criteria for SAD and major depressive disorder (MDD) as per DSM-5 criteria (APA, 2013). The Depression Anxiety Stress Scales–short form (DASS-21; Henry & Crawford, 2005; Lovibond & Lovibond, 1995) were administered pre- and post-treatment. This is a 21-item self-report measure of progress commonly used in clinical practice assessing depression, anxiety and stress symptoms on a Likert scale from 0 (did not apply to me at all) to 4 (applied to me very much, or most of the time). The DASS-21 has been shown to possess adequate construct validity, as well as adequate to high reliability in a large-scale psychometric study (Cronbach’s alpha was .88 for depression, .82 for anxiety, .90 for stress and .93 for the combined scales; Henry & Crawford, 2005).
Jill described symptoms consistent with a primary diagnosis of SAD as per DSM-5 criteria (APA, 2013). She described a marked anxiety in all social interactions with non-close friends, and generally avoided anxiety-provoking situations, as she anticipated embarrassing herself in front of others or being negatively evaluated as ‘boring’. The fears were above and beyond those expected for normative daily social interactions, caused significant distress and interfered with attending university, occupational and social events. Jill reported that if she did not avoid social interactions, then she would engage in safety behaviours (e.g. pretending to be talking on the phone) or would consume four to five alcoholic drinks to reduce anxiety.
Jill also described a secondary depressive response that was triggered during periods of sustained social avoidance. She described symptoms of MDD as per DSM-5 criteria (APA, 2013). These included symptoms of low mood most of the day and nearly every day, difficulties getting to sleep and staying asleep, fatigue and low energy, feelings of worthlessness and frequent passive suicidal thoughts about death.
Differential diagnoses were considered. Jill did not appear to meet criteria for avoidant personality disorder (AvPD), which can also be characterized by marked anxiety and avoidance in social situations. Jill did not describe globalized patterns of interpersonal fear, distress and psychosocial problems typically present in individuals with AvPD (APA, 2013; Hummelen et al., 2007). Similarly, Jill did not meet criteria for other common anxiety disorders, such as generalized anxiety disorder (GAD). Jill described anxiety focussed in social situations and did not appear to have non-normative fears in other domains (e.g. occupational, educational or global matters) typical in GAD (APA, 2013).
Jill’s general practitioner reported that she had been prescribed a serotonin–norepinephrine reuptake inhibitor (SNRI), venlafaxine, for 2 years prior to psychological treatment as it has been found to have some efficacy with SAD and low mood (Stein et al., 2005). However, Jill did not report significant improvements from this medication. Given the lack of improvement from medication, the early onset, pervasive episodic symptoms, MDD comorbidity and her history of peer social traumas, a ST approach was adopted to specifically target the hypothesized causal social traumas, reduce reliance on avoidant coping modes, defuse from internalized self-criticism and build a Healthy Adult sense of self.
6 Case Conceptualization
From a schema mode perspective, it was theorized that early experiences of parental over-control and over-protectiveness led Jill to feel she was less able and competent than others, resulting in pervasive shyness and a pattern of interpersonal withdrawal. Her father’s self-criticism had also modelled beliefs around self-defectiveness (i.e. ‘not good enough’, ‘unlikable’ and ‘worthless’). Jill experienced social rejection from previously close friends when starting a new school as a young adolescent, and she reported feeling ‘different’ and that she did not ‘fit in’. Jill’s negative core beliefs and subsequent emotional and behavioural patterns appeared consistent with defectiveness, incompetence and social isolation EMSs.
These early experiences resulted in a number of childhood unmet needs, such as unconditional acceptance, encouragement of autonomy and imperfection and a sense of interpersonal belonging. These unmet needs contributed to the development of a Vulnerable Child defined by a fear of negative evaluation and low self-esteem, as well as a shame-inducing Punitive Critic who frequently reinforced negative self-beliefs, such as ‘you’re defective’ and ‘unlikable’. These modes were likely strengthened and reinforced in early adolescence after Jill’s experience with peer rejection and social isolation.
In an attempt to cope with the intense distress of these modes, Jill developed an Avoidant Protector, which enabled her to reduce interpersonal anxiety by avoiding social situations, and a Detached Self-Soother, which enabled her to reduce anxiety through the consumption of alcohol or passive escape fantasies about death. Whilst the short-term consequences of these coping modes were reinforcing and anxiety relieving, in the long-term they increased social isolation and reinforced Jill’s belief that she was not ‘good enough’ and ‘couldn’t cope’. As her social isolation increased, the patient then utilized a Compliant Surrender coping style whereby she would resign herself to the perceived ‘truth’ of the Punitive Critic, which precipitated and perpetuated a secondary depressive cycle (see Figure 1 for diagrammatic schema conceptualization summary). Schema mode case conceptualization for Jill.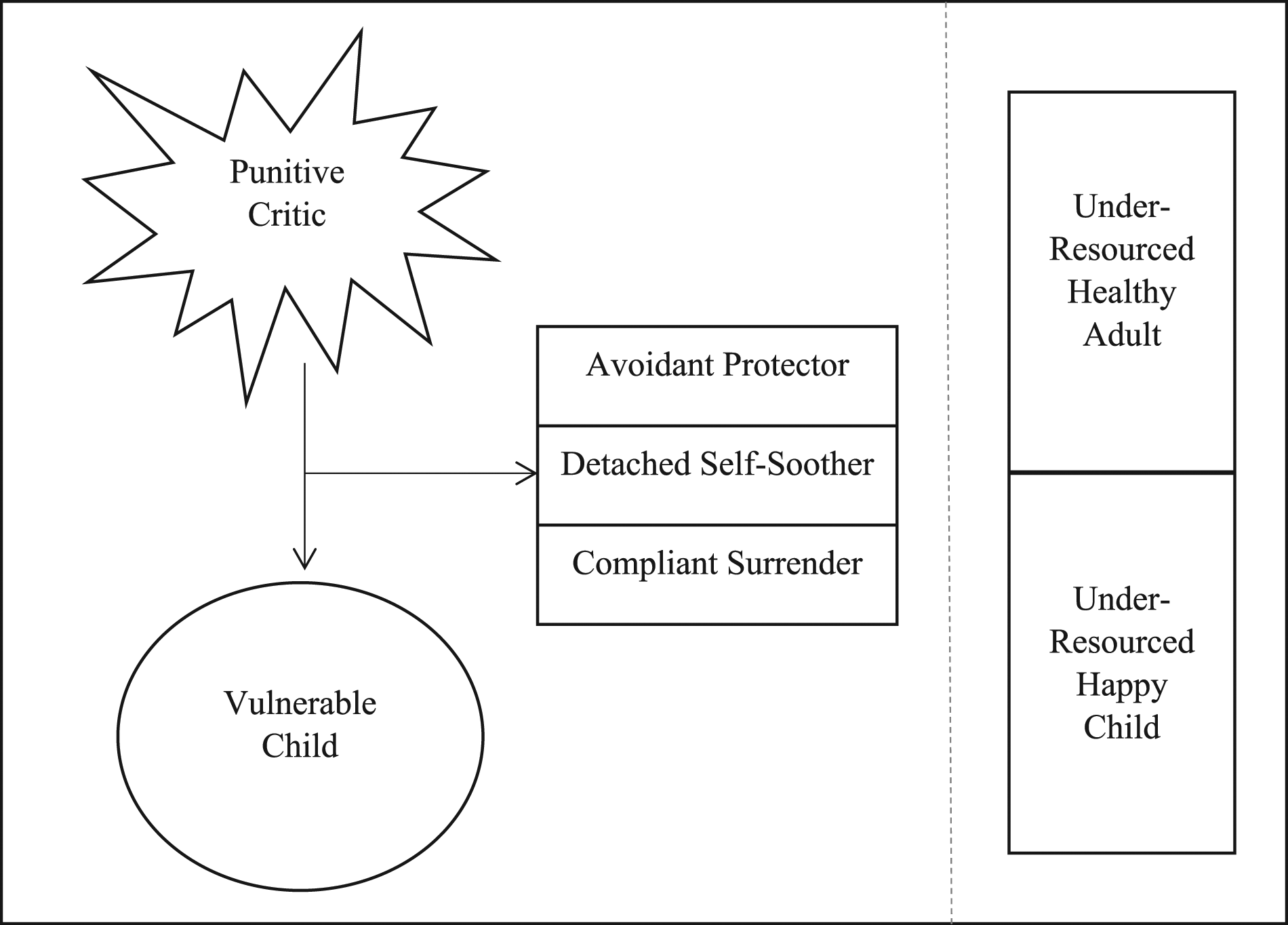
Due to these pervasive and recurrent cycles, Jill had an under-resourced Healthy Adult and Happy Child; however, she was able to psychologically access these modes while with close friends. The collaborative goals of ST in this case were to resource the Healthy Adult Mode to defuse from the Punitive Critic, replace the maladaptive coping modes and meet the needs of Vulnerable Child. The patient’s self-identified goals were to (1) reduce anxiety and increase social engagement and (2) improve mood and positive self-belief. Given the formulation of depression as a consequence of the avoidant SAD symptoms, a clinical decision was made to focus on the maintaining factors of SAD hypothesizing that both disorders would remit if the primary condition was adequately treated.
7 Course of Treatment and Assessment of Progress
Jill attended 10 weekly sessions of ST with the first author. In terms of treatment fidelity, the treating clinician had undertaken formal training in ST and engaged in regular schema-focussed supervision throughout this treatment with an accredited advanced level schema supervisor who had fulfilled the accreditation requirements of the International Society of Schema Therapy.
Overview of Treatment
Brief Overview of Assessment and Treatment Sessions.
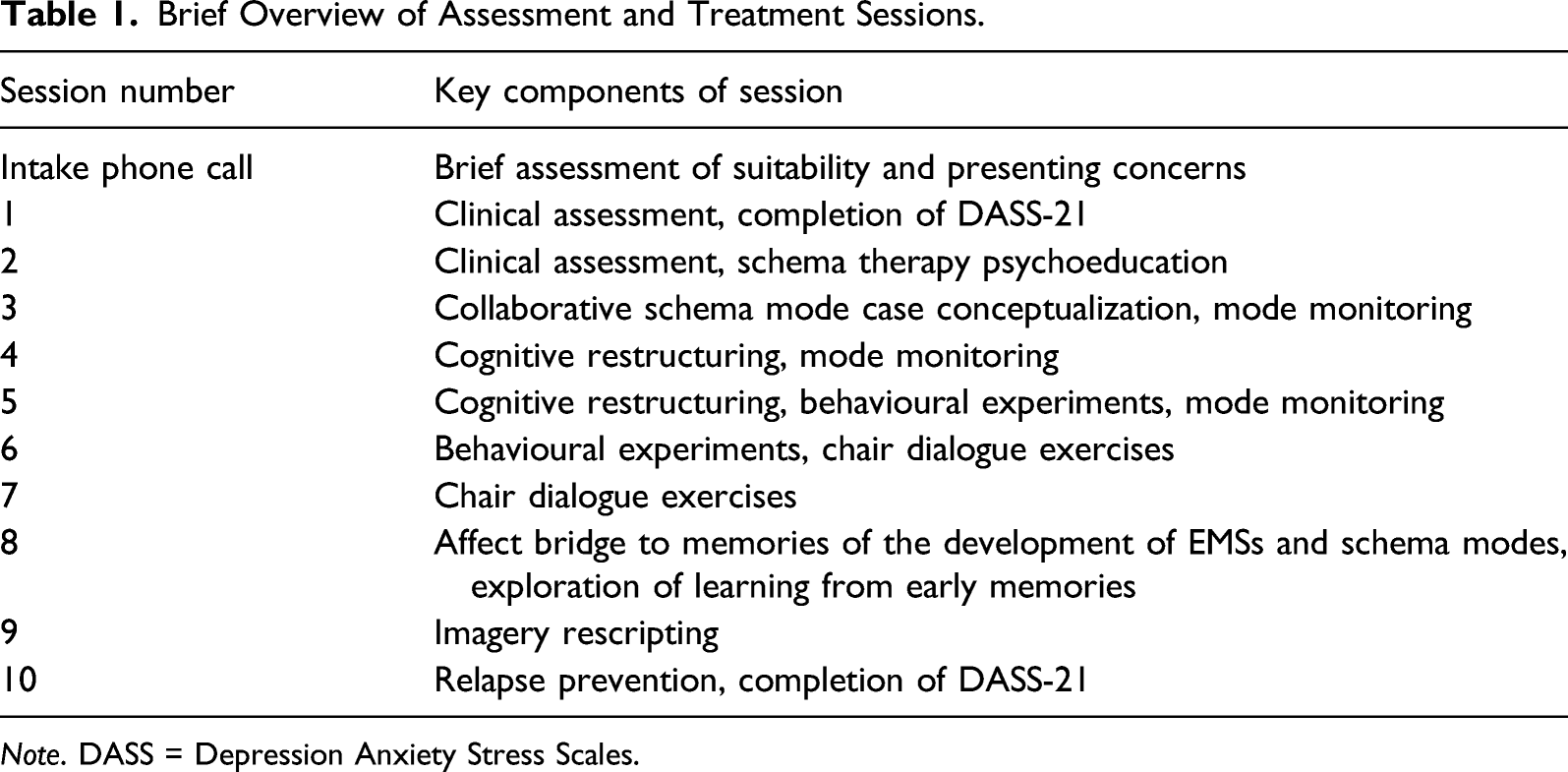
Note. DASS = Depression Anxiety Stress Scales.
Cognitive and Behavioural Interventions
The aim of the cognitive and behavioural intervention components of ST was to increase cognitive insight, decrease maladaptive responses and increase adaptive responses to unmet needs. The patient demonstrated a rapid increase in insight about her previously unmet needs through the mode conceptualization process. She completed mode monitoring between sessions and gained skills to self-identify when each mode had become activated, which appeared to somewhat lessen the amount of fusion she had with these modes. Jill was able to complete a cognitive pros (i.e. ‘I feel less anxious’) and cons (e.g. ‘I stay isolated’) exercise on the utility of relying on her Avoidant Protector and Detached Self-Soother to reduce anxiety. As a result of this and similar cognitive exercises, she engaged in two behavioural experiments (i.e. responding to a message from an acquaintance and going on a date without drinking alcohol) to test her negative anticipatory predictions (e.g. ‘I’ll be rejected’ and ‘I’ll make a fool of myself’). Jill was then able to use the evidence from the behavioural experiments to further challenge both the likelihood and cost of her fears of negative evaluation and identified alternative beliefs (e.g. ‘I am interesting because I’m different’ and ‘I can cope if I’m not universally liked’). Despite these important symptom decreases in behavioural avoidance and improvements in the cognitive re-appraisal process, Jill continued to report a cognitive–affective disconnect where she stated she now ‘knows’ she is not unlikable, but often continued to ‘feel’ unlikable.
Experiential Interventions
The aim of ST experiential intervention components was to establish new emotional and affective learning that would heal the Vulnerable Child, increase self-compassion and increase the ability for Healthy Adult to meet the needs of Vulnerable Child. Chair dialogue techniques aim to create a productive dialogue between different modes by having different chairs represent different modes (Arntz & Jacob, 2013).
Two-chair dialogue techniques were initially utilized with Jill to externalize Punitive Critic and then meet the needs of the Child. Jill identified messages from the Critic (e.g. ‘You’re boring and worthless’), and the therapist modelled Healthy Adult limit setting to the empty chair representative of the Critic (e.g. ‘You cannot speak to Jill like that’). Given the patient’s hypothesized defectiveness, incompetence and social isolation EMSs, limited re-parenting messages were provided in line with Jill’s previously unmet needs (e.g. ‘You are interesting, capable and worthy of belonging’).
The therapist was able to then coach Jill’s own Healthy Adult across subsequent sessions to appropriately defuse the Critic and ‘re-parent’ her Vulnerable Child. In one session, Jill reported significant anxiety about meeting someone new on a date. Jill’s Healthy Adult Mode was coached to set limits on the Critic’s messages (e.g. ‘Your date will find you unlikable and unattractive’) by firmly telling the Critic, represented by an empty chair, to stop and later removing the mode/chair from the room. Her Healthy Adult was able to validate the good intentions of her Avoidant Protector messages (i.e. ‘Avoid all romantic relationships to safeguard against further rejection’) and her Detached Self-Soother messages (i.e. ‘You will cope better if you have a few drinks beforehand’), whilst also weighing the advantages and disadvantages of continuing to cope through these forms of avoidance.
In order to encourage her Healthy Adult to comfort her Vulnerable Child, Jill was prompted with questions, such as ‘How does the Vulnerable Child feel? What does she need to hear from you?’. Jill was able to provide messages of acceptance, love and belonging to her Child mode, as well as remind her of the positive social relationships she has. Jill was then encouraged to sit in the chair of the Child and replay the messages her Healthy Adult had just offered to increase the experiential re-learning. She reported feeling emotional, comforted and connected for the first time. At the end of the exercise, Jill reported that this was a ‘new experience’ and that she was ‘proud of herself’. She reported that she would attend the date and that she believed she had worthwhile contributions to make to the conversation. She acknowledged that attending would still be anxiety provoking for her Vulnerable Child but that her Healthy Adult could normalize being nervous and remind the Child that she was loved and accepted by her close friends. This shift towards self-compassion appeared to be a turning point in her treatment, and she started to report that at times, she could both know and feel that she was a likable and worthwhile person.
Throughout therapy, it became clear that there had been a series of key social traumas that had been seminal in strengthening Jill’s beliefs that she was ‘unlikable’ ‘defective’ and ‘not as competent as others’. She described three key memories from early adolescence involving a romantic rejection, minimization of mental health by a family member and peer rejection. She reported that the experience of peer rejection had been the most impactful for her, and therefore, imagery rescripting focussed on this memory.
The imagery exercise began by exploring the childhood situation, and Jill was able to recall arriving at a new school with positive anticipation to see her close friend; however, as she approached her, she was ignored and dismissed. The image was paused prior to Jill’s experience of explicit rejection from her friend, and Jill was able to imagine her Healthy Adult stepping in to the image to express to the friend that her actions were hurtful before guiding her Vulnerable Child to find a sense of belonging with the peers who later became her close friends. In the post-rescripting debrief, Jill demonstrated a re-appraisal of the original social learning and hypothesized that the previously close friend had likely acted in response to her own anxieties about ‘fitting in’ and identified that she had later made new friends because she was ‘friendly, loyal and interesting’.
After the chair dialogue and imagery rescripting sessions, the patient reported a marked increase in Healthy Adult self-compassion and decrease in Punitive Critic and maladaptive coping modes. Jill demonstrated a new Healthy Adult perspective that generalized to other relational traumas, both from early childhood and her recent relationship breakdown, and therefore, imagery rescripting of additional memories was not deemed necessary.
Relapse Prevention
The final session involved a relapse prevention plan where Jill self-identified SAD and MDD warning signs and how Healthy Adult could prevent and intervene to maintain gains. Healthy Adult was encouraged to utilize cognitive skills (e.g. ask, ‘What would Healthy Adult do?’ or ‘What other perspectives can Healthy Adult take?’), behavioural skills (e.g. taking graded concrete steps towards her goals) and emotion-focussed skills (e.g. dialogue with the modes) to maintain gains and prevent relapse.
Treatment Outcomes
DSM-5 Symptoms of SAD and MDD Pre- and Post-Treatment.
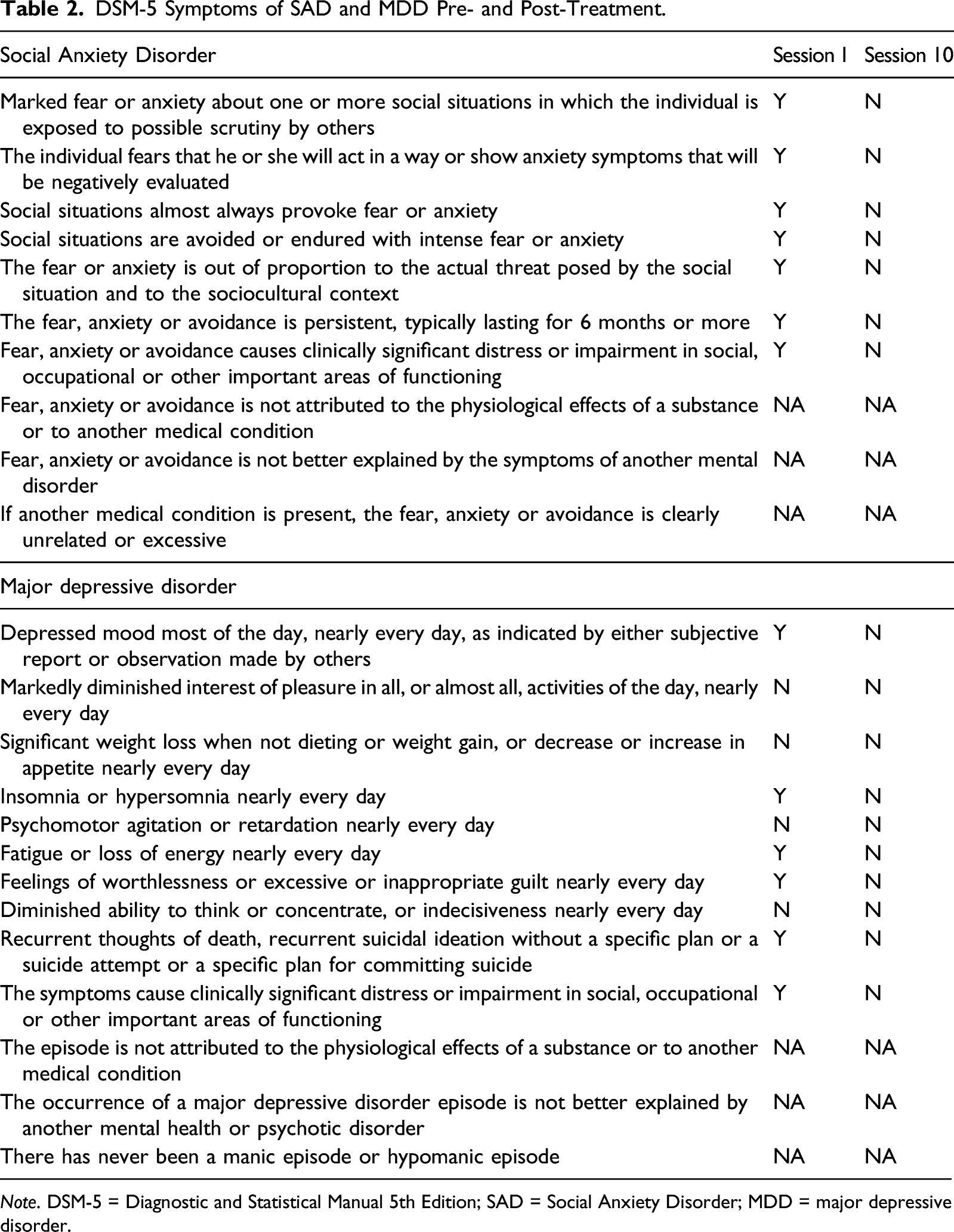
Note. DSM-5 = Diagnostic and Statistical Manual 5th Edition; SAD = Social Anxiety Disorder; MDD = major depressive disorder.
DASS-21 Responses Pre- and Post-Treatment.
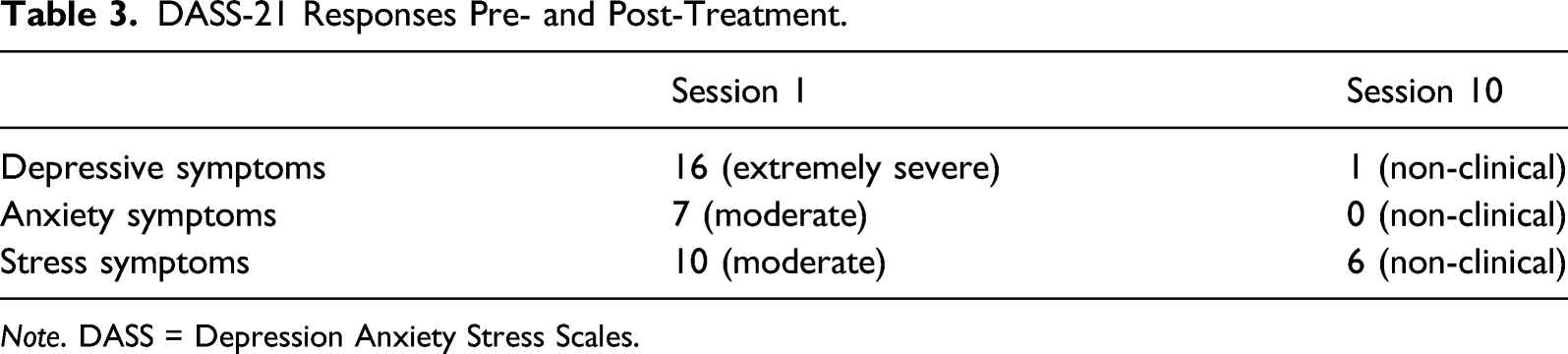
Note. DASS = Depression Anxiety Stress Scales.
8 Complicating Factors
The main challenges to treatment were financial barriers and the limitations of a naturalistic setting as described in detail below.
9 Access and Barriers to Care
The healthcare system in Australia during this time-period meant that only 10 sessions in any given year were eligible for financial rebates from public health care. Jill reported that due to her status as a full-time student with a low income, there would be financial barriers to her completing any further treatment after those 10 rebate-able sessions. This meant that extended experiential work and repetition of helpful exercises (as is common in ST) was not possible. Ethical consideration was given to potential needs for future support. Jill was reminded that she could access free support from her university counselling service, that she could re-engage with our clinic at the lowest allowable rate or that she could return in the new year when she would be eligible for another 10 rebate-able sessions.
10 Follow-Up
Treatment progress was assessed pre- and post-treatment. This treatment occurred in a naturalistic clinic setting, which did not include a follow-up process for patients unless they re-presented to the clinic for further treatment at a later date. Further comment on this is made below.
11 Treatment Implications of the Case
This case study provides preliminary support for the ST Mode Model as an intervention for individuals with SAD. Given the prevalence and chronic course of SAD, it is important to identify effective treatments for the subgroup of SAD individuals who do not respond sufficiently to CBT. Jill no longer met DSM-5 criteria for SAD and comorbid MDD by the end of the treatment. She reported and demonstrated diminished anxiety, improved mood, increased self-compassion and increased skills for adaptive coping by the final session.
Whilst the cognitive and behavioural interventions, similar to those used in traditional CBT, were effective in shifting unhelpful core beliefs and behavioural patterns, they left her with residual anxiety symptoms and a dissociation between knowing she is a worthwhile and likable person and yet still feeling worthless and unlikable. This is consistent with clinical anecdotal evidence, as well as empirical findings that many individuals with SAD continue to experience residual symptoms after CBT (Heimberg, 2002; Mörtberg et al., 2011; Rodebaugh et al., 2004). The ST-specific treatment components (i.e. experiential chair dialogues and imagery rescripting) appeared to have bridged the disconnect between cognitive and affective learning and helped her to meaningfully ‘unlearn’ negative messages from her early development. The patient reported the imagery exercise as one of the most helpful activities of therapy, consistent with findings that even a single session of imagery rescripting of a social trauma for an individual with SAD can reduce the severity of symptoms (Norton & Abbott, 2016b).
When ST and imagery rescripting are utilized with personality disorders, patients often need extensive modelling of a Healthy Adult response before their own Healthy Adult can step into the image (Arntz & Jacob, 2013). However, in this case, Jill was able to step into the role from the beginning after the Adult had been previously strengthened utilizing cognitive, behavioural and chair dialogue techniques. This is consistent with previous findings where most SAD participants were able to step into the Healthy Adult role without previous modelling (Norton & Abbott, 2016b).
This highlights an important ongoing empirical question, where further research is needed to determine which ST components, and in what dosage, are necessary to see sustained progress for SAD. If the effectiveness of ST were found to be generalizable to the broader SAD population, it may be a cost-effective and efficacious treatment choice, especially for those who do not respond to CBT alone. If the current 10-session treatment is generalizable to broader SAD cases, this may be meaningfully shorter than the approximately 50 ST sessions required for personality disorders (Bamelis et al., 2011) or the 16 sessions described for SAD in some CBT protocols (see: Clark et al., 2003).
This case study provides an important example of the use of ST to treat SAD and comorbid MDD in a young adult. Nonetheless, the case study is not without its limitations. It is difficult to identify underlying mechanisms of change or the most efficacious components to the treatment with a sample size of one. However, based on the self-report of the patient and the ST Mode Model theory (Arntz & Jacob, 2013), it is the authors’ impression that it was the experiential techniques (i.e. chair-work and imagery rescripting) that provided the most corrective emotional experience and allowed for meaningful re-appraisal of long-held negative core beliefs.
An additional limitation is that because this case was treated in a naturalistic and non-research setting, more formal measures for EMSs (i.e. Young Schema Questionnaire; Young, 2005), Schema Modes (i.e. Schema Mode Inventory; Lobbestael et al., 2008; Young et al., 2003) and Social Anxiety symptoms (i.e. Social Interaction Anxiety Scale; Mattick & Clarke, 1998) were not administered. The authors believe that the results of these measures may have provided further support for the patient’s recovery from SAD through the resolution of underlying EMSs and dysfunctional modes.
Finally, the case study was limited as there was no opportunity for a follow-up session, and therefore, it is difficult to say with certainty if the therapeutic gains were maintained post-treatment. However, given the experiential re-learning and shifts in underlying core beliefs about the self, the authors hypothesize that ST is likely to produce long-term characterological shift, consistent with findings of its use for other disorders (e.g. Bamelis et al., 2011); however, further replication and empirical study is warranted.
12 Recommendations to Clinicians and Students
Clinicians and training clinicians are encouraged to consider the evidence base and clinical applicability of ST for SAD, particularly when working with patients with a cognitive–affective dissonance (i.e. to know a belief to be false, but to continue to feel it is true). It may be that patients who do not respond to the cognitive and behaviourally focussed components of CBT alone may benefit from increased experiential learning from ST. In the present case, ST provided experiential treatment interventions that lent themselves to both cognitive and affective learning to shape a more positive and realistic view of the self, others and the world.
The present study, despite its limitations, provides a preliminary example of the effective use of ST for a young woman with SAD and comorbid MDD. Case studies can be useful clinical and empirical tools to explore treatment efficacy in naturalistic settings (Kazdin, 1981); however, larger scale replication studies are needed to determine if the results of this novel treatment approach for SAD are generalizable and to better refine which specific components hold the most efficacy for this condition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.