
Abstract
Adolescent athletes with attention deficit hyperactivity disorder (ADHD) and oppositional defiant disorder (ODD) experience unique challenges that impact their sport performance, such as making errors due to poor concentration. The current multiple-baseline across behaviors case trial (i.e., positive assertion and negative assertion) is an evaluation of The Optimum Performance Program in Sports in an adolescent athlete diagnosed with ADHD and ODD. Intervention skill sets were targeted sequentially in a virtual format to safeguard against COVID-19 contraction. A battery of psychological measures was administered at baseline, post-intervention, and 1-month follow-up. Results indicated negative and positive assertion skills improved, but only when targeted, and severity of ADHD and ODD symptom severity, general mental health symptoms, and factors interfering with sport performance decreased from pre- to post-intervention and these improvements were maintained at 1-month follow-up. Similar improvements occurred in relationships with coaches, teammates, and family. Treatment integrity and consumer satisfaction were high.
Keywords
1. Theoretical and Research Basis for Treatment
Attention-Deficit/Hyperactivity Disorder (ADHD) is characterized by hyperactivity, impulsivity, and/or inattention, and affects at least 8% of adolescents (Poysophon & Rao, 2018). Oppositional Defiant Disorder (ODD) is characterized by patterns of anger or irritability and argumentative behavior, and up to 50% of youth with this disorder evidence ADHD (American Psychierican Psychiatric Association, 2013). Adolescent athletes with ADHD experience unique adverse consequences in performance (Nazeer et al., 2014), including negative feedback from coaches, teachers, and parents (Podolski & Nigg, 2001). Symptomology is exacerbated in youth athletes with ADHD when comorbid ODD is present. Indeed, in both school and sport environments these youth are often hostile and negatively reactive, leading coaches to more frequently report poor attitudes having them on their teams (Vargas-Tonsing et al., 2008), and officials more frequently disqualifying them from sport competition (Johnson & Rosen, 2000), than youth who do not evidence mental health symptomology.
Adolescents with ADHD tend to demonstrate poor motor performance (Harvey & Reid, 2003), resulting in difficulty learning game rules and strategies and applying them fluidly in game situations. Such errors frustrate teammates and coaches and negatively impact relationships (Pelham et al., 1990). Difficulty controlling emotions during sports competition can also adversely impact performance (Wagstaff, 2014), including forced removal from sports competition or practice (Friesen et al., 2013). Both ADHD and ODD adversely impact athletes’ academic performance, inherently affecting their eligibility to participate in school-based sports teams and increasing the likelihood of remediation (White et al., 2014).
1.1. Behavioral and Pharmaceutical Treatments for Adolescents Athletes With Attention Deficit Hyperactivity Disorder and Oppositional Defiant Disorder
Psychosocial treatments for ADHD, and ADHD comorbid with ODD, have been evaluated in controlled trials involving youth, but not in youth athletes (Stewman et al., 2018). Stimulant medications for ADHD are customarily prescribed when symptom impairment is moderate to severe, and considered the preferred treatment (Kutcher, 2011). Stimulant medications inhibit the reuptake of dopamine and norepinephrine, which improve attention span and concentration (Stewman et al., 2018). The physiological benefits of stimulant medications occur relatively soon after ingestion, however, there are disadvantages to using stimulant medications in the treatment of athletes with ADHD (e.g., stomachaches, decreased appetite, insomnia, headaches, and sudden cardiac death; Kutcher, 2011). These concerns have led sport organizations (e.g., International Olympic Committee (IOC) and National Collegiate Athletic Association (NCAA) to restrict stimulant drug use in competition to athletes with therapeutic use exemptions (Putukian et al., 2011). Atomoxetine is the only non-stimulant medication approved by the Food and Drug Administration (FDA) and not banned by the NCAA or IOC. The therapeutic benefit of non-stimulant medication for ADHD is usually not appreciated until 3–6 weeks of continual use (Parr, 2011). Lastly, while demonstrably effective, pharmacological treatment for ADHD has the potential to be abused (Putukian et al., 2011). Hence, behavioral interventions for ADHD are often attempted prior to medication management, and when behavioral interventions are insufficient, they are typically augmented with stimulant medications.
Pharmacological treatments are often discouraged in athletes with ADHD, especially those with aspirations to compete at national or international levels (Nazeer et al., 2014). Level-one therapies for ADHD include behavioral parent training, behavioral classroom management, behavioral peer interventions, and organization training, indicating that these therapies have been tested thoroughly and are well-established with adolescents with ADHD (Evans et al., 2014). While behavioral treatments have demonstrated efficacy in treating adolescents with ADHD, there are no controlled evaluations of behavioral treatments for adolescent athletes. However, O’Connor et al. (2014) evaluated a behavioral treatment program in young children with ADHD that included a sports training component (i.e., Summer Treatment Program; STP). This program has evidenced behavioral and academic improvements and parent and counselor reports of improved prosocial behavior and specific sports skills in children (O’Connor et al., 2014). While the Summer Treatment Program focuses on sport-participation benefits in young children with ADHD, it does not explicitly address sports performance in adolescent athletes.
There are many evidence-supported behavioral interventions to treat adolescents with ODD. These include combinations of parent-management training programs and family therapy, cognitive problem-solving skills training, social skills programs, and school-based programs (AACAP, 2009). Behavioral interventions for ODD have been shown to help youth achieve greater mastery in controlling their behavior and developing respect for authority figures (Conant-Norville & Tofler, 2005). Additionally, including parents in behavioral treatments have been shown to be the most effective way to reduce behavioral symptoms of ODD in all age groups (Brestan & Eyberg, 1998). Some of the most supported ODD interventions are family-based, such as Family Behavior Therapy (Azrin et al., 2001). Medication alone has not been supported as a treatment for ODD, however, it may be helpful (AACAP, 2009), particularly when ODD is comorbid with ADHD (Turgay, 2009).
1.2. Why Customize Evidence-Supported Interventions for Attention Deficit Hyperactivity Disorder and Oppositional Defiant Disorder to be Sport Specific?
Relevant to treatment development, the benefits of exercise and positive reinforcement make sport attractive for children with ADHD (Pujalte et al., 2019). However, evidence-based treatments for ADHD and ODD have not evolved to prescriptively incorporate sport in treatment planning. Therefore, it makes sense to adapt existing evidence-based behavioral interventions for ADHD and ODD to fit sport contexts, and in doing so, better promote their engagement, receptivity, and effectiveness in athletes (Geidne et al., 2013).
Athletes who evidence ADHD and ODD are presumed to be more interested in behavioral intervention when it addresses sports performance than traditional applications (Schinke et al., 2017). Such adjustments are hypothesized to improve attention, enhance working memory (Chai et al., 2018), establish stronger connections between new and existing information, and encourage greater interest in practicing therapeutic skill sets in a real-world context (Brewin, 1989).
Adolescents with ODD typically are brought to treatment by their parents and often demonstrate low motivation and reluctance to participate (Steiner & Remsing, 2007). Therefore, mental health service engagement is especially warranted (Karver & Caporino, 2010). However, sport-specific engagement strategies, such as those used in collegiate athletes (Donohue et al., 2020b), have yet to be evaluated in adolescent athletes.
While there are many benefits of sport-participation, there are stressors associated with competitive sports for adolescent athletes (Goyen & Anshel, 1998), including pressure to perform, conflicts with coaches or opponents, fear of injury, making errors, and poor coach–athlete relationships (Holt et al., 2005). Maladaptive coping strategies often exacerbate these stressors, which may exacerbate mental health symptomology (Tamminen & Holt, 2012). Therefore, there is a great need to develop and evaluate, using controlled methodology, sport-specific mental health intervention for adolescent athletes.
The Optimum Performance Program in Sports (TOPPS) has demonstrated significant improvements in collegiate athletes’ relationships, interferences with sports performance, and problems associated with mental health symptomology up to 8 months post-intervention in clinical trials (Chow et al., 2014; Donohue et al., 2020b; Donohue et al., 1999; Donohue et al., 2015; Donohue et al., 2018; Donohue et al., 2016; Pitts et al., 2015), and in one controlled trial particularly as mental health diagnostic severity increased (Donohue et al., 2018). Additionally, in an uncontrolled case trial involving an Asian American female adolescent diagnosed with social anxiety disorder, an adaptation of this intervention was determined to lead to similar improvements up to 1-month follow-up (Donohue et al., 2021).
The cancellation of athletic seasons and fear of contracting COVID-19 has negatively affected the psychological well-being of youth athletes (Sanderson & Brown, 2020). Further, COVID-19 has also impacted the delivery of traditional mental health services to be adapted to telehealth modalities (Pfender, 2020). Consequently, mental health providers must be mindful of the unique stressors that consumers experience due to COVID-19 while implementing psychologically-based interventions safely (Zhou et al., 2020). Along these lines, Merzon et al. (2020) determined untreated ADHD elevates risk for the contraction of COVID-19 through decreased ability to maintain COVID-19 safety precautions. Evidence has shown that the restrictions placed on children with ODD and ADHD have also exacerbated oppositional symptoms (Melegari et al., 2021). Thus, TOPPS is especially relevant to the improvement of these symptoms (Donohue et al., 2018), but with added COVID-19 precautions (i.e., video-conference intervention delivery). Zoom is a video-conferencing software that has been widely used by psychotherapists and shown to be efficacious in delivering behavioral therapies (Boelen et al., 2020), and its integration into TOPPS delivery is likely to be successful as teletherapies have been used previously to facilitate intervention engagement in FBT (Donohue et al., 2016; Donohue et al., 2020a).
The present study aim is to assess efficacy of TOPPS in an adolescent athlete evidencing comorbid ADHD and ODD. Dependent measures focus on psychiatric symptoms, factors that have been found to directly impact sport performance of this youth, and relationships with significant others.
2. Case Introduction
2.1. Participant
David was a 17-year-old White male high school varsity baseball player referred to a university-based sport optimization program by his assistant coach due to “behavioral outbursts” at baseball practices. David was screened to assure the following inclusion and exclusion criteria were met (a) participating in organized sports, (b) between 12 and 17 years of age, (c) enrolled in a public or private high school, and (d) not actively receiving psychotherapeutic intervention.
3. Presenting Complaints
During intake assessment, David reported behavioral outbursts and struggling with concentration in the baseball field (competition and training), at home, and school. David described these outbursts as explosive swearing and yelling, throwing objects (e.g., baseball equipment), frequent arguments, and punching walls. He emphasized these episodes occur when things do not go his way. Both David and his father described these outbursts happening as frequent as weekly (at least a few times a week). David reported that he was removed from baseball practices due to these issues, and frequent frustration with family, teachers, coaches, peers, and teammates. Regarding his concentration, David described having daily difficulties staying focused in class or when others are talking with him. He expressed being easily distracted by things in his environment (e.g., people walking by in the background) in situations where he is supposed to be attentive. These concerns were said to negatively impact his grades at school and baseball performance. David acknowledged his difficulties controlling his anger and concentrating and the impact they have on his academics, relationships, and sport performance, however, described having challenges in controlling these challenges. Overall, David expressed interest in gaining better self-control and concentration.
4. Case History
At the time of intake, David was living with his father and older adult sister. His father was employed as an electrician. His mother died when he was 7 years old due to an illicit drug overdose. David’s father reported that his son experienced significant inattention and difficulty controlling his temper. David’s father attributed these problems to verbal and physical bullying by his peers, and relationship difficulties in high school were said to include “explosive swearing” and punching walls. Additionally, David described having difficulty respecting coaches, umpires, and teachers.
5. Assessment
5.1. Diagnostic Assessment
Child and Adolescent Services Assessment (CASA; Ascher et al., 1996
5.2. Primary Outcome Measures
A comprehensive battery of assessment measures was administered by a trained assessor 1 week before intervention (baseline), 4 months post-baseline (post-intervention), and 5 months post-baseline. A sub-set of measures were administered consistent with multiple-baseline across behaviors methodology (Barlow & Hersen, 1988). The comprehensive battery included the following:Kiddie—Schedule for Affective Disorders and Schizophrenia for School Aged Children 6–18 years DSM-5 (KSADS; Kaufman et al., 2000
5.3. Secondary Measures
Time-Line Follow-Back interview (TLFB) (Sobell et al., 1996). This assessment measure uses a calendar with pre-recorded anchors to assist retroactive reports of alcohol and non-prescribed drug use frequency and number of days attending school and sport practice. The TLFB has demonstrated test-retest reliability and concurrent validity (Donohue et al., 2004).Youth Self-Report 11–18 (YSR) (Achenbach, 1991). This 112-item measure assesses adolescents’ competencies and problem behaviors. The Externalizing and Internalizing Behavior Problem scales will be used in the current study. The YSR has demonstrated acceptable internal consistency, test-retest reliability and content validity (Achenbach & Rescorla, 2001).Beck Depression Inventory-II (BDI-II) (Beck, 2011). This 21-item measure is one of the most widely used methods of assessing depressive symptoms. The BDI-II has demonstrated high internal consistency, test-retest reliability, and concurrent validity (Wang & Gorenstein, 2013).Student Athlete Relationship Instrument (SARI) (Donohue et al., 2007a). This 63-item measure assesses sport-specific problems in relationships with Family, Coaches, Teammates, and Peers. The SARI has demonstrated high internal consistency and criterion-related validity (Donohue et al., 2007a), and reliably predicts mental health symptom severity in collegiate athletes (Hussey et al., 2019).Overall Happiness with Family, Coaches, Teammates, and Peers (Donohue et al., 2007a). This 4-item measure utilizes a 0–100 scale of happiness (0 = completely unhappy, 100 = completely happy). Items assess overall happiness in four relationships, for example, coaches, teammates, family, and peers; these scales have demonstrated acceptable criterion-related validity (Hussey et al., 2019).Client Satisfaction Questionnaire-8 (CSQ-8) (Larsen et al., 1979). This 8-item (4-point scale) self-report questionnaire evaluates quality of services received, and has demonstrated high internal consistency and concurrent validity (Kelly et al., 2017).Overall Anger with Coaches, Teammates, Teachers, and Peers (Donohue et al., 2007a). This 3-item measure assesses overall anger with coaches, teammates, and teachers utilizing a 0–100 response format for each item (0 = not at all angry, 100 = completely angry; Donohue et al., 2007a).Average Anger over the Last 7 Days
Suicide Probability Scale (SPS) (Cull & Gill, 1982). This measure assesses suicidal risk/ideation. The SPS has demonstrated acceptable internal consistency (Eltz et al., 2006) and has established predictive validity in suicidal attempts and self-destructive behavior (Larzelere et al., 1996).
5.3.1. Pre-Intervention Assessment Results
Pre-, Post-, and Follow-Up Assessments of Mental Health.
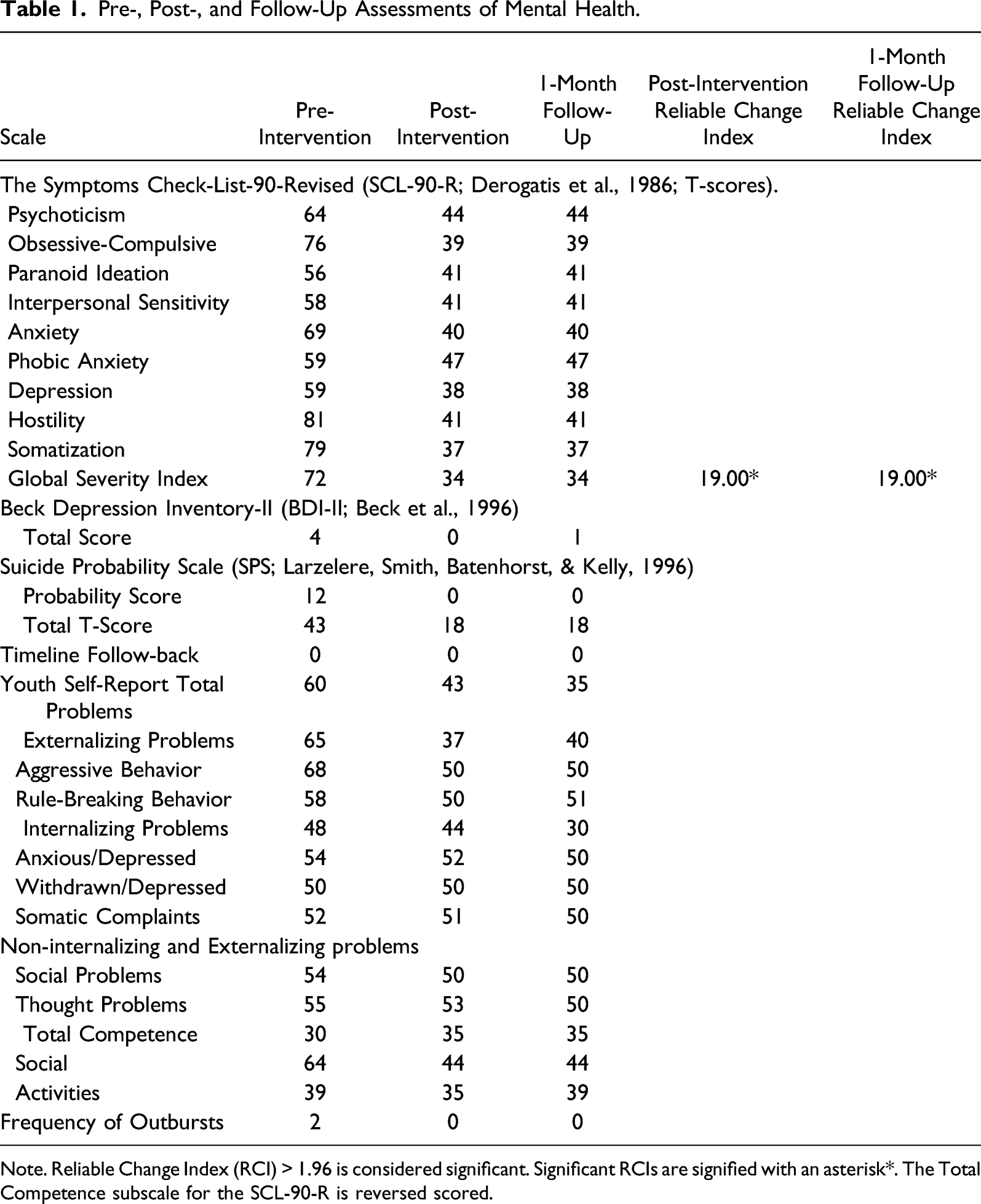
Note. Reliable Change Index (RCI) > 1.96 is considered significant. Significant RCIs are signified with an asterisk*. The Total Competence subscale for the SCL-90-R is reversed scored.
Pre-, Post-, and Follow-Up Assessments of Factors Interfering With Sport Performance.
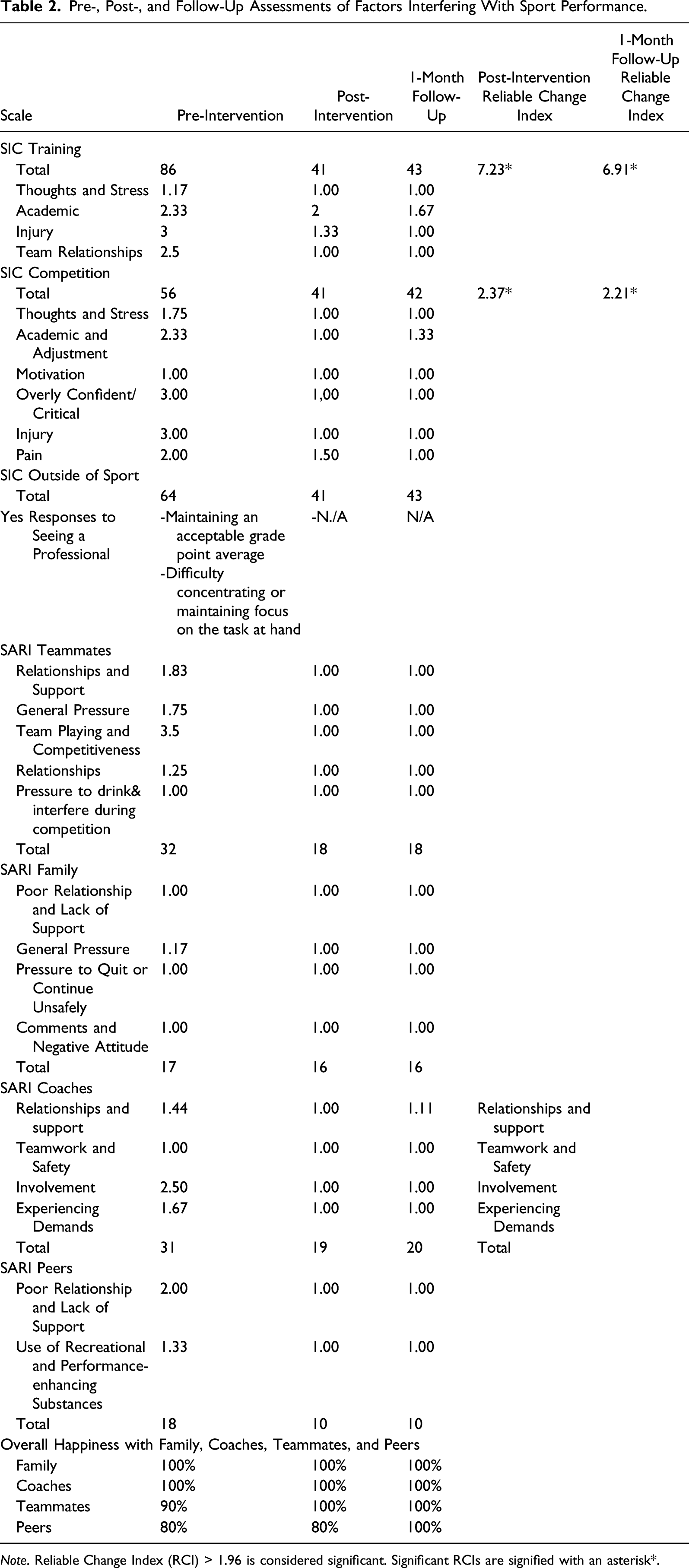
Note. Reliable Change Index (RCI) > 1.96 is considered significant. Significant RCIs are signified with an asterisk*.
He demonstrated elevations in several subscales of the SIC in both Training and Competition (i.e., Academic, Injury, Team Relationships, and Overly Confident/Critical), while his Thoughts, Stress, and Motivation subscale scores reflected relative strengths. Teammates and Coaches subscales were relatively high, indicating his relationships with coaches and teammates were negatively affecting his performance.
5.4. Study Design
In addition to the comprehensive assessment battery that was administered to assess changes in sport performance, relationships, and mental health symptomology across this study, a multiple-baseline across behaviors experimental design was used to assess the effects of specific intervention components in decreasing David’s frequency of outbursts, teachers, coaches, and teammate relationships, ADHD and ODD related symptoms, and positive and negative assertion skills in a controlled context (Barlow & Hersen, 1988). These behaviors were monitored immediately before each meeting throughout the study using probe assessments. Selected subscales from the SCL-90-R, SIC, and SARI (see Figure 1) were administered at each probe. It was predicted that David’s negative assertion skills (i.e., responding to an aversively perceived situation), as assessed in probe sessions, would improve once targeted in week four while his positive assertion skills (i.e., requesting something desired) would demonstrate minimal improvements. David’s positive assertion skills in probe sessions were predicted to improve once this skill set was targeted in week seven. Throughout positive assertion skills training it was predicted that his negative assertion skills would be maintained. David’s relationships, frequency of outbursts, and selected subscales from the SCL-90-R, SIC, and SARI were predicted to improve across time. Multiple-baseline figure for the role-play assessments for social skills.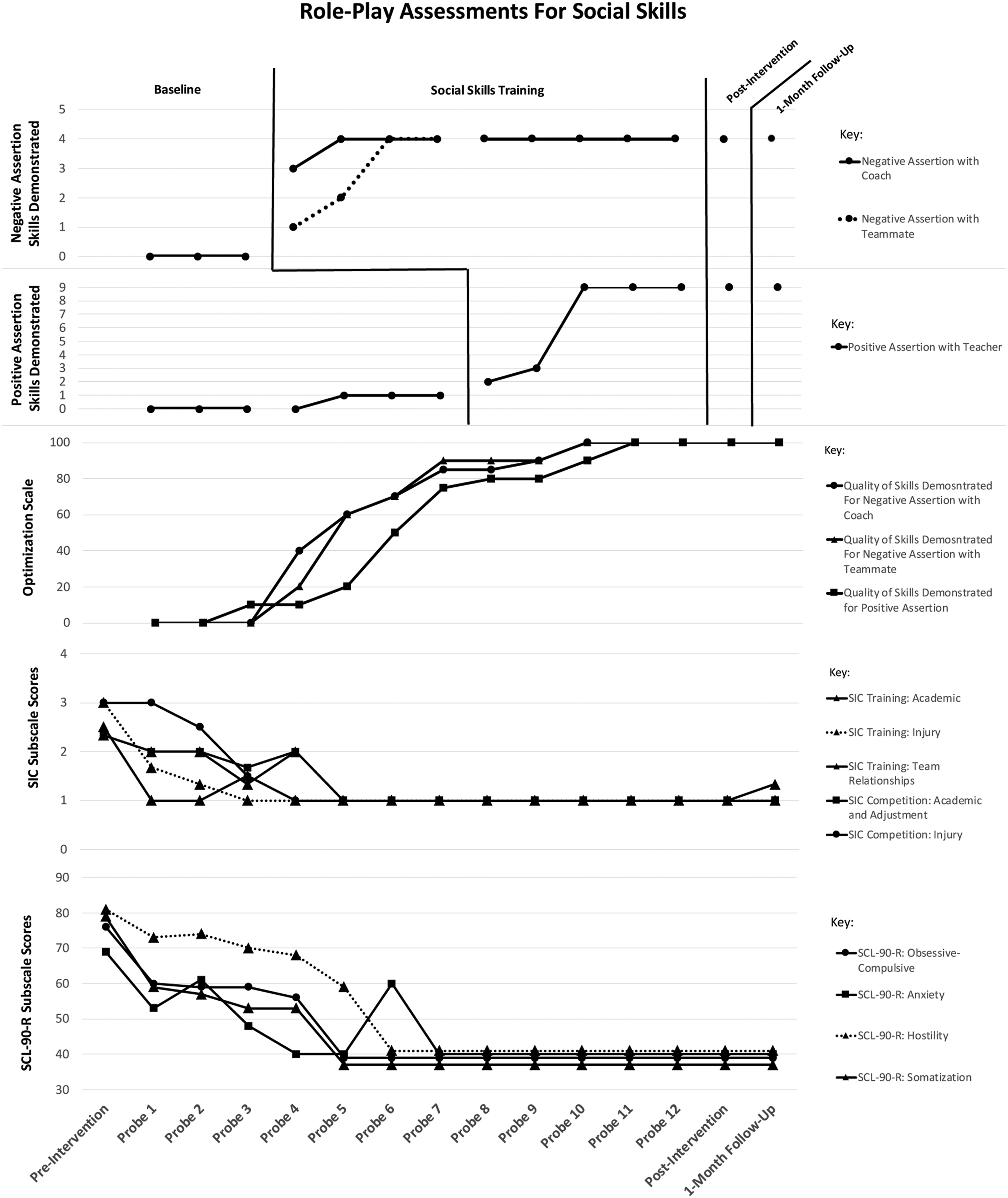
6. Case Conceptualization
David’s case was conceptualized from a cognitive-behavioral perspective. David and his father indicated that David evidenced severe difficulty sustaining attention since Elementary school. David described his mind “going blank” when others spoke and frequently responding to queries with “I don't know” due to self-reported difficulties thinking of a response. He reported being easily distracted by his surroundings and avoiding tasks that required sustained attention to avoid criticism from others. ADHD and ODD are influenced by frontal lobe dysfunction, and his beliefs about his concentration and executive functioning challenges are conceptualized as lack of cognitive coping skills because of his untreated ADHD (Nøvik et al., 2020). He approached events with elevated expectations for positive outcomes. For example, he solicited help from a teacher expecting that the teacher would help with is problem and when the teacher did not immediately help he reported thinking “I can’t rely on teachers” (Beck, 1995; Ramsay & Rostain, 2008). These elevated expectations also occurred in sport settings (e.g., “I don’t trust coach because he takes me out of games”).
His difficulties with attention were reported to negatively impact his school and sports performance (Harvey et al., 2003). He reported making careless errors, misinterpreting information from his coach, and forgetting to submit his assignments on time. These actions led to aversive consequences from others, which likely intensified symptoms associated with distractibility and stress and decreased his interest in skill development. David’s concentration was reported to become exacerbated following his mother’s sudden death due to substance use overdose when he was 9 years old.
After his mother died, David’s father reported having to manage extreme “anger outbursts” and argumentativeness, and that his son was “bullied” by his peers for not having a mother. David emphasized getting into arguments at school with others and often expressing his frustrations through outbursts involving explosive swearing and hitting or throwing “things.” His father described understanding and supporting his son’s emotional reactions and defiance towards his peers, and authority figures, as a way to “teach him how to stand up for himself.” Thus, his father may have inadvertently reinforced oppositional behaviors with empathy and support (Frick et al., 1992). David described himself as a person who “only focuses on himself” and is “critical of others,” which likely interfered with his ability to receive reinforcement from others. Reinforcement deprivation has consistently been found to increase aggressive behavior and interfere with rational thought (Azrin et al., 1965). His coach described him as a person who “shuts off” when he is receiving criticism, and he indicated having uncontrollable anger that likely distracted attention from his skill deficits. For instance, yelling at an umpire for calling a strike distracts attention of others from his inabilities to hit the ball. Anger is also reinforced with support (e.g., attempts to calm him after he throws a bat). The process of criticizing and arguing with others involves a similar reinforcement contingency (i.e., temporarily removes positive punishers, such as criticism or focus on poor performance). These behaviors prevent opportunities for skill development and experience of positive reinforcement for desired behaviors and generalize to other contexts (e.g., school) through stimulus generalization.
7. Course of Treatment and Assessment of Progress
Remediation was thus aimed at improving David’s concentration through cognitive and behavioral skill training (e.g., objective thinking, perspective taking, focusing on the task at hand rather than outcomes, thought stopping, solution generation, positive imagery, scheduling, note-taking, perspective taking, social skills specific to asking for reinforcers and responding to upset, and recognition of antecedent triggers to undesired behavior). Performance planning involved teaching his father and coach to reinforce desired behaviors while ignoring undesired ones. To address oppositional behaviors (e.g., arguing with authority figures and being critical of others) David was taught to effectively use compliments and ignore undesired behaviors, and to use problem-solving, objective thinking, diaphragmatic breathing, focusing on the task at hand rather than outcomes, and taking others’ perspectives.
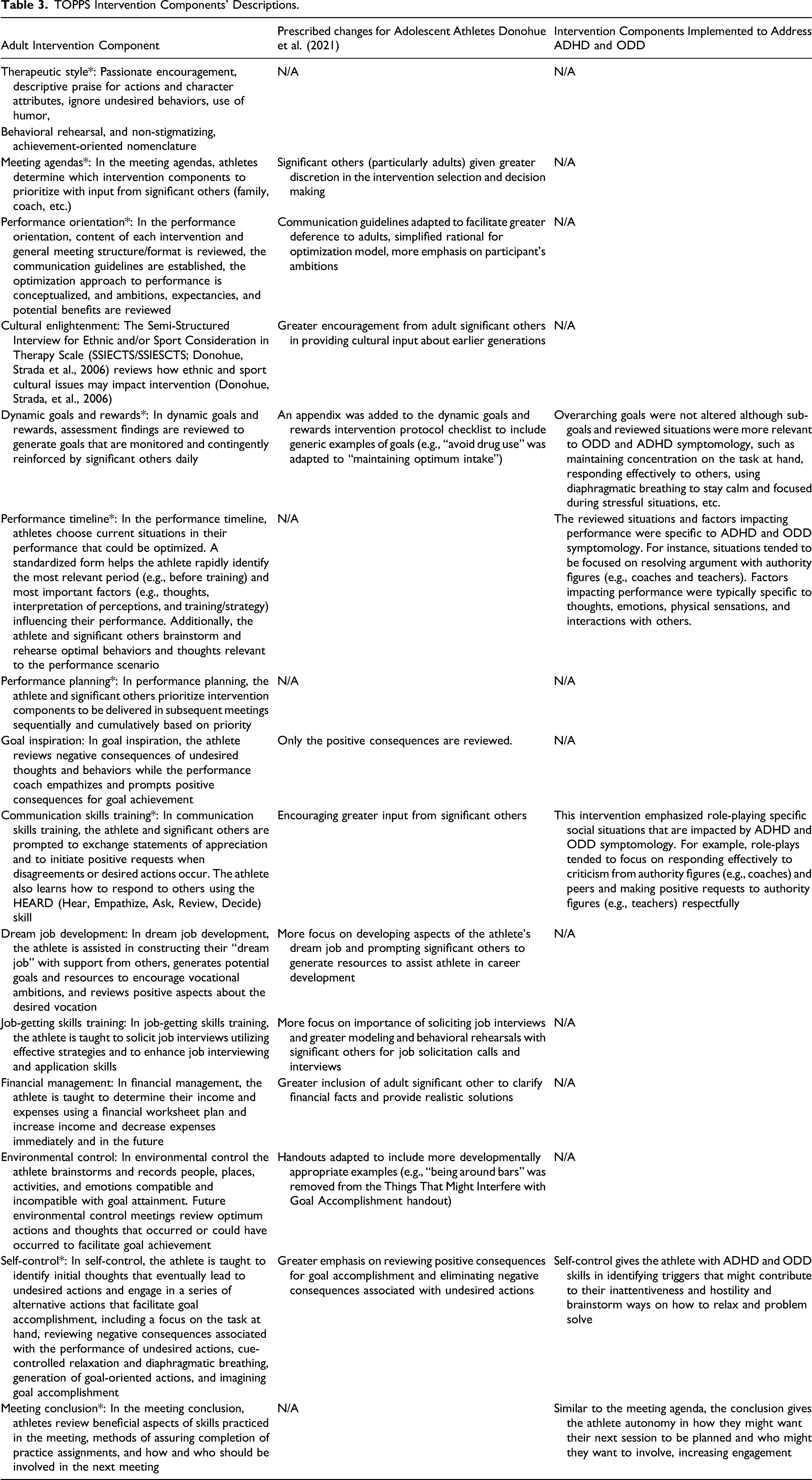
TOPPS Intervention Components’ Descriptions.
During Meeting 1, a standardized Program Orientation was conducted to provide an overview of the program, discuss expectations, and gather information regarding the referral. Additionally, David and the father discussed potential significant others to involve in future sessions (his sister and coach). The Performance Timeline component was subsequently implemented to build treatment engagement and allow David to take away skills from the first session. The performance scenario rehearsed in the performance timeline was optimizing his focus while running with teammates during training who distracts him. David required modeling to implement visual and verbal rehearsal of the scenario after brainstorming factors influencing his performance. The provider reviewed diaphragmatic breathing. David, his father, and the provider generated goals from the Performance Timeline, such as strengthening his legs, running ¾ of a mile each week, and practicing diaphragmatic breathing.
Meeting 2 involved reviewing pre-intervention assessment results for the SIC to identify David’s strengths and elevated goal-worthy items in preparation for establishing goals in the Dynamic Goals and Rewards intervention. David’s item elevations clustered around the program’s global goals of maintaining optimum mental wellness, maintaining optimum relationships with others, and maintaining optimum effort in school-related activities. Further, David and his father emphasized goals surrounding optimum effort in sport-related activities, given his motivations to play baseball at the collegiate level. Specific goals that were initially developed for maintaining optimum mental wellness included maintaining optimum focus, maintaining optimum sleep, and eating well. Specific goals that were initially developed for maintaining optimum relationships with others included being respectful to teachers and teammates, uplifting teammates at practice, and being praiseworthy to others. Specific goals that were initially developed for maintaining optimum effort in school-related activities included turning in schoolwork on time, asking teachers and peers for help if needed, and taking notes to promote focus in class. Finally, specific goals that were initially developed for maintaining optimum effort in sport-related activities included consistently attending hitting lessons, practicing breathing, and consistently working out. David and father both agreed on food (e.g., sushi dinner) as a reward for future goal accomplishment. Meeting 2 also involved prioritizing intervention components for the rest of the program. Notably, David and his father prioritized Self-Control to assist in his challenges in controlling his angry emotions.
David’s skills in negative assertion were targeted in Meetings 3–6 using the HEARD intervention component. In Meeting 3, the provider first modeled for David how to use the HEARD method in responding to criticism utilizing the scenario of a coach coming up to him on the mound and communicating that he should take a break (see Appendix 1 for prompt). The provider solicited what was liked about how the provider modeled HEARD and then allowed David to practice the HEARD steps in his style. At each meeting, the provider and father praised David for each of the steps David performed optimally. The provider and participant practiced the scenario about the coach for three sessions until mastery was demonstrated by achieving all the five HEARD steps. In meetings 5 and 6, the provider applied a different scenario about his teammate (see Appendix 1for prompt). Once mastery was demonstrated for this scenario, the provider transitioned to positive assertion training for Meetings 8–12.
In addition to HEARD training, Appreciation Exchange was implemented in Meeting 3 with David’s sister and father to develop David’s communication skills in expressing appreciation to supportive others. All expressed that it was a positive experience to hear appreciation from one another directly, and David reflected that it improved his mood. Dynamic Goals and Rewards were implemented in Meetings 3–6 as well. Each meeting, the provider would challenge David to brainstorm more optimal ways of achieving goals and including supportive others in assisting in goal development. In Meetings 3–6, David emphasized the benefits of diaphragmatic breathing, note-taking, utilizing online resources for schoolwork, healthier diet, completing assignments on time, increased class participation, consistency in working out and practices, keeping perspective, and visualization.
Meetings 5–6 focused on targeting David’s anger outbursts and inattention through Self-Control. The provider modeled the Self-Control steps for David using a scenario that David said had triggered his anger in the past (a bad call by an umpire). David and father expressed they liked having steps David can follow and practice in future situations. Another scenario practiced in Meeting 6 included taking exams. In Meeting 6, David reported using self-control outside of the meeting when playing video games, whereby he indicated the diaphragmatic breathing was the most helpful step.
Consistent with multiple-baseline methodology, the second phase of intervention (Meetings 7–12) continued to target social skills, with positive assertion being targeted for the first time. The Positive Request intervention was utilized in Meetings 7–11 to teach David how to make requests of others while avoiding arguments (e.g., succinct requests for specific actions, when actions are desired, offers to assist, statements of appreciation, acceptable alternatives). The provider first modeled the Positive Request steps for David, and then David engaged in role playing scenarios with his father (meetings 7–8) and coach (meetings 9–10). Examples included making requests from his dad, asking his teacher for help, and asking his coach to spend time with him after practice to assist in extra training. David mentioned using the positive request outside of sessions, such as asking his teacher for help on an assignment and making requests to his friends when playing videogames.
A conflict occurred in meeting 10. David missed a game without notifying his coach. The provider invited the coach with David’s permission to attend meeting 10 to address the conflict between David and his coach in session. While David was upset about the interaction in the session, the coach, participant, and provider were able to maintain therapeutic alliance. David utilized HEARD skills from phase 1 in this interpersonal conflict with his coach.
Dynamic goals and rewards were implemented each meeting to assess goal accomplishment and challenge David to improve his goals. The dynamic goals and rewards intervention was used to target David’s sport performance, academics, and relationships with others. Goals emphasized achieving were staying proactive on his schoolwork, eating healthier foods and making better meal choices, improved sleep habits, increased visualization of sport specific scenarios, increased frequency of sport specific training and strength training, and increased use of diaphragmatic breathing. David emphasized improvements in his sport performance where he described having increased physical strength and endurance because of meeting his training consistency goals each week. Both David’s father and coach described improvements in David’s athleticism in training and competition. David also described improvements in his academics where he reported turning in his assignments on time, asking questions when needed, and studying effectively for quizzes and exams. His father reported that David’s mathematics teacher commented on his improvements in the classroom. David’s report of his sport performance and academic improvements were consistent with his improvements on his scores on the SIC (see Table 2).
Self-control was also implemented in Meetings 7, 9, 10, and 11 to continue targeting David’s anger and inattention. David again emphasized how useful the diaphragmatic breathing component of the intervention has helped him outside of the session, especially regarding his focus during practices and competitions (e.g., during baseball practice after making an error).
7.1. Intervention Integrity
To ensure implementation integrity, several strategies were employed, including documentation of techniques used during each session, the participant’s ratings of engagement and progress towards personal and programmatic goals; ongoing clinical supervision by a licensed psychologist (i.e., review of audio recordings and corrective feedback); structured agendas and detailed protocol checklists to guide intervention and measure protocol adherence; reviews of audio recordings by independent raters to evaluate protocol adherence and measure inter-rater reliability; and the participant’s ratings of helpfulness with each intervention component during each session.
Intervention integrity scores were calculated in a two-step process: 1. The overall percentages of intervention protocol steps completed as per the provider’s self-report were computed, thus serving as validity estimates for protocol adherence. 2. Ten percent of the session audiotapes rated by the provider for intervention completion were randomly selected and reviewed by independent raters. Inter-rater agreement was computed by adding number of steps agreed upon by the provider and independent rater and dividing this result by the number of steps agreed upon and disagreed upon by the provider and independent rater × 100). 70% protocol adherence and inter-rater agreement is considered satisfactory.
Protocol Adherence. The overall protocol adherence across 12 sessions was 99% (SD = 3.34%, range = 84–100%), according to the provider. Inter-rater agreement between the provider and independent rater was 97.1% (range = 83–100%). Thus, the intervention components in this study were implemented with high reliability (see guidelines from Bellg et al., 2004).
Consumer Satisfaction and Engagement Ratings. Following completion of TOPPS, David reported high satisfaction with the intervention components, as indicated by the Athlete Helpfulness Rating Scale with an average score of 6.85 (SD = .36). The provider rated David’s engagement with each intervention component (based on attendance/promptness, participation, conduct, and home assignment completion) 98.5% optimal. The client also reported high satisfaction with the services received, as indicated by the CSQ-8 with a total score of 32. David attended 100% of the scheduled meetings.
Baseline. Figure 1 shows multiple-baseline data for his social skills assessment through role-plays and elevated SCL-90-R and SIC subscales. As hypothesized, Program Orientation, Dynamic Goals and Rewards, and Performance Planning did not affect his social skills.
Phase 1: Evaluation of HEARD, Self-Control, Dynamic Goals, and Rewards. A three-week baseline was established for David’s social skills in negative assertion and positive assertion. After implementing HEARD training, David’s negative assertion skills abruptly improved and reached peak performance in probe 6. David met four out of five criteria consistently for HEARD from probe 6 and onwards. While David did not “ask for solutions” in his role plays, he provided solutions in a respectful way. The quality of David’s skills demonstrated for negative assertion was evaluated using an optimization scale (0 = non-optimal, 100 = completely optimal) and was demonstrated to improve over time. Inter-rater agreement between the provider and independent raters for the quality of David’s skills demonstrated for negative assertion was 99.3% (range = 87.5–100%). David’s negative assertion skills improved while, as expected, his positive assertion skills demonstrated minimal improvement.
Phase 2: Evaluation of Positive Request Training, Self-Control, Dynamic Goals, and Rewards. After implementing Positive Request training, David’s positive assertion skills abruptly improved and reached peak performance in probe 10. David’s skills for positive assertion was evaluated using an optimization scale (0 = non-optimal, 100 = completely optimal) and demonstrated improvement over time. Inter-rater agreement between the provider and independent raters for the quality of David’s skills demonstrated for positive assertion was 92.3% (range = 80–100%). David’s positive assertion skills, as expected, improved while his negative assertions skills sustained throughout phase 2.
Post-Intervention and 1-Month Follow-Up. The reliable change index (RCI; Jacobson & Truax, 1991) was used to consider the significance of pre-intervention to post-intervention assessment score improvements for the SCL-90-R and SIC (primary outcomes). The RCI helps determine if the clinical change is significant beyond the standard error of measurement. It considers a participant’s pre-and post-test change while considering general measure reliability and standard error of measurement. RCI scores greater than 1.96 reflect changes in scores that are meaningful. As per the Reliable Change Index, David evidenced significant and meaningful reductions in his SIC Training and Competition total scores both pre- to post-intervention and pre- to 1-month follow-up. He evidenced reductions in SCL-90-R Global Severity pre- to post-intervention. Reliable Change Index scores are listed in Tables 1 and 2.
The post-intervention KSADS interview indicated no current clinically significant ADHD and ODD symptoms, and a blind rater determined the same after the 1-month follow-up KSADS interview.
Eyeballing procedures (Byrne, 2017) were used to estimate the magnitude of effect for all secondary measures (TLFB, YSR, SPS, SARI, Overall Anger with Coaches, Teachers, and Teammates, Overall Happiness with Coaches, Teammates, and Family, Frequency of Outbursts, and Average Anger during past 7 Days) from pre- to post-test and pre-test to 1-month follow-up. Post- and follow-up outcome measures demonstrated improvements from baseline for these measures (See Tables 1 and 2).
8. Complicating Factors
David initiated intervention with considerable motivation to improve his sports performance and regulate his anger. However, he initially lacked motivation to improve his social skills. To enhance his motivation, the provider incorporated the participation of his father, sister, and coach to model effective communication skills. David later acknowledged how learning these skills improved his mood, communication, and emotional regulation. Standardizing the provider’s prompts for the negative assertion role play assessments made it difficult to create a natural dialog in which HEARD is used. Thus, this latter method of assessment may have been insensitive to detecting skill improvement.
9. Access and Barriers to Care
As a method reducing COVID-19 contraction, video-conferencing was utilized. There were additional benefits of video-conferencing. First, given that adolescent athletes and their parents have busy schedules, video-conferencing facilitated access to care through limited travel time, and allowed David and the provider to search resources on the internet in real time. One of the challenges was that David and his father did not have access to printers at home. The provider was able to address limited access to printers through the use of e-mailing virtual documents prior to the meetings and using the screen share feature for worksheets and homework during the meetings. Lastly, the provider was able to address screen freezes through immediate telephone calls.
10. Performance Programming Implications of the Case
This case study permitted an evaluation of the effectiveness of a sport-specific FBT with an adolescent athlete diagnosed with predominantly inattentive ADHD and ODD. Multiple-baseline results revealed substantial reductions in problem behaviors and symptoms and improvements in social skills after being targeted with specific intervention components. Initiating Positive Request and HEARD was associated with improved social skills in positive and negative assertion, respectively. Initiating Dynamic Goals and Rewards and Self-Control was associated with improved mood, academic functioning, and focus. Consistent with prior research (Conant-Norville & Tofler, 2005; Evans et al., 2014), these findings suggest that social skills training and setting, monitoring, evaluating, and rewarding desired behaviors with the inclusion of significant others is effective for adolescents with ADHD and ODD in developing effective skills. David also expressed improvement in sports performance. These gains were reportedly maintained from pre- to post- and pre- to follow-up assessments. Given that David attended 100% of scheduled sessions and rated the program highly, this indicated that TOPPS’s sport-specific component demonstrated effective engagement for an adolescent athlete with ADHD and ODD.
TOPPS intervention components are capable of handling multiple cognitive and behavioral problems within ADHD and ODD. In choosing the respective treatment plans and modifying interventions to address the presenting diagnostic symptoms, the treatment provider must develop a treatment plan that optimally meets the client’s treatment goals. The treatment plan takes into consideration the client’s goals while addressing the presenting diagnostic symptoms. Therefore, the treatment provider would emphasize their client’s respective disorder, and when multiple diagnoses are present as in the current case, it is prudent to be inclusive of scenarios for the relevant diagnostics in each intervention component. Further, because TOPPS focuses on goals in both sports and life, the provider was able to teach David skills that could be applied in life outside of sports (e.g., communication skills with teachers or potential employers). Additionally, TOPPS was able to be delivered fully through video-conferencing, which was consistent with recommendations from Boelen et al. (2020). This indicates that TOPPS is an intervention that addresses the need for adaptable and effective behavioral interventions that minimize the risks of contraction of COVID-19 (Zhou et al., 2020).
11. Recommendations to Clinicians and Students
This case study describes a comprehensive approach to intervention with an adolescent student-athlete utilizing an evidenced-based intervention and integrating empirical research findings. Although David was initially ambivalent about improving his social skills, motivating factors unique to his athletic status were integrated into intervention planning, such as his sports performance and his coach’s involvement. Systematically involving his coach and sister improved David’s social skills and improved his ability to regulate his emotions when communicating with others. Additionally, clinicians and students are recommended to be familiar with the software they are using if they plan to implement this intervention through video-conferencing (Mace et al., 2018).
Thus, this case study supports the efficacy of a sport-specific adaptation of FBT in concurrently improving social skills, sport performance, and mental health. Therefore, given the limited support for mental health interventions in adolescent athletes, TOPPS offers great promise (Donohue et al., 2021), and supports the need to examine TOPPS in randomized clinical trials (Rounsaville et al., 2001).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.