
Abstract
We report a case of a patient seen within Integrated Primary Care at a collegiate health center for treatment of comorbid idiopathic urticaria and anxiety. Following medical consultation within Primary Care, Emergency services, and Asthma and Allergy Specialists, Primary Care Behavioral Health services were consulted. Here, we describe the Behavioral Health Consultant (BHC) model within primary care and the collaborative nature of the model. The benefits of this collaboration allowed the patient’s primary care provider (PCP) to use appointment times efficiently and to rely on the BHC to address the complexities of the patient’s underlying stress and anxiety. We detail the ways in which the BHC model contributed to significant decreases in the patient’s symptoms of anxiety and depression. Finally, we recommend expansion of programs providing opportunities for training in the integrated primary care model.
1 Theoretical Background and Basis for Treatment
Integrated Primary Care
The integration of mental health services into primary care can improve access to care for individuals who may otherwise not seek mental health treatment (Phillips et al., 2022). Recent models for integrating mental health services into primary care have been pioneered in community-based (Kroenke & Unutzer, 2017; Ramanuj et al., 2019; Reiter et al., 2018) and Veterans Affairs primary care clinics (Leune et al., 2018). These models have demonstrated effectiveness for diagnosing and treating mental health problems (Caldwell & Patterson-Kane, 2014) in addition to improving outcomes in the treatment of acute illness and chronic medical problems (Hunter et al., 2018; Wilfong et al., 2022).
College students with mental health concerns are highly likely to utilize primary care for treatment (Kessler et al., 2005). Thus, provision of mental health services within college primary care clinics may reduce inequities and enhance access to mental health care (Alschuler et al., 2008; Turner et al., 2018).
The clinical care model used at our university primary care practice is based on the Primary Care Behavioral Health (PCBH) model (Reiter et al., 2018), a prominent model of integrated care in which BHCs are embedded members of the health care team. This embeddedness allows BHCs to assist with any health condition across the entire range of patients, thus becoming an accepted and routine aspect of the biopsychosocial model of patient care. BHC’s share office and exam room space with other clinic providers and staff, which promotes both team cohesion and BHC accessibility. The PCBH model promotes enhancement of quality and efficiency of patient care, as well as staff and provider support, via ‘curbside consultations’ to help PCPs with treatment planning, doing appropriate administrative tasks that reduce PCP workload, and by developing strategies to enhance psychological safety on the team. The overarching goal of the BHC is to improve a primary care team’s ability to manage chronic and acute health conditions (Reiter et al., 2018). In this model, providers initiate referrals to the BHC, often occurring as a “warm hand-off”, wherein the BHC sees the patient in the exam room alongside the primary care provider (PCP) or following the PCP appointment. Per the PCBH model guidance, XU BHCs provide brief, time-limited behavioral interventions that address a multitude of presenting problems including depression, anxiety, insomnia, ADHD, medication adherence, substance use, and acute or chronic disease management. Visits are typically 15–30 minutes in length, and an episode of care typically ranges from one to five sessions. BHCs provide real-time communication with other clinic team members (e.g., physicians, nurse practitioners, registered nurses, and medical assistants) via in-office consultation and through the EMR. All XU BHCs are doctoral trainees who provide services under the direct supervision of a licensed clinical psychologist faculty.
Urticaria
Urticaria is a common skin condition requiring medical consultation in primary care medical practice. It is disease characterized by itchy and sometimes painful wheals (hives) which cover the skin and mucous membranes. Between 8.8%–20% of individuals experience an attack of urticaria at least once in their lifetime (Darlenski et al., 2014). Allergic urticaria (AU) can last from a few hours to six weeks and is more common in children and young adults. The cause or trigger is associated with a definable exposure, such as foods, medications, infections, insect stings or blood transfusions. Non-allergic urticaria is ‘the label given when the allergic source can’t be found’. Non-allergic urticaria is more prevalent than allergic urticaria and is caused by many things, including cold temperatures, food dyes and additives, medication, exercise, anxiety, constricting clothing, and the sun (Bernstein et al., 2014).
Chronic urticaria (CU) lasts for more than six weeks, can come and go for months or years and can disappear on its own, and is more common in middle-aged women. In CU, the trigger is identified only 20% of the time; in cases where the trigger remains unidentified, the condition is referred to as Chronic Idiopathic Urticaria (CIU). CIU significantly affects patients’ health-related quality of life. Patients often suffer from sleep disorders, depression and emotional distress (Gimenez-Arnau et al., 2016; Staubach et al., 2011; Vietri et al., 2015) that result in a high emotional burden, psychiatric disorders and other comorbidities. Also, personality traits have been shown to be associated with some dermatological conditions. For example, patients with urticaria, psoriasis or alopecia were reported to demonstrate higher hostile and neurotic traits than people with other dermatological conditions, while others report more interpersonal sensitivity in patients with CIU.
The international guidelines for treating CU recommend use second-generation H1-antihistamines (AH) as first- and second-line treatment options, respectively, with administration of omalizumab and ciclosporin as third- and fourth-line therapy, respectively. Corticosteroids (CS) are only recommended as a short course for exacerbations, but reports suggest that longer-term us of CS occurs routinely in clinical practice (Weller et al., 2022).
Anxiety
Individuals with CU report significantly higher rates of depression and anxiety, lower quality of life, and worse physical health than those without CU (Engin et al., 2008). Research suggests that CU and anxiety often co-occur (Barbosa et al., 2011; Engin et al., 2008; Hashiro & Okumura, 1994), with almost half of individuals with CIU experiencing severe anxiety levels (Barbosa et al., 2011). The relationship between anxiety and CU may be bi-directional. For instance, several of the physical symptoms of CU can give rise to anxiety and emotional distress (Barbosa et al., 2011; Engin et al., 2008; Hashiro & Okumura, 1994). The presence of CU and its accompanying discomfort and health concerns, alongside the intricacies of treatment that might impact quality of life, could lead to a higher prevalence of anxiety symptoms (Barbosa et al., 2011). Alternately, psychological stress and mood changes may activate and exacerbate urticaria via an underlying dysregulated inflammatory process (Bansal & Bansal, 2019).
Anxiety is a general survival response to threats in one’s environment and is characterized by worried thoughts and physical changes, like body tension and increased heart rate (American Psychological Association; Arroll & Kendrick, 2018). Anxiety is necessary for human survival but can become maladaptive when the symptoms of anxiety are out of proportion or disrupt daily living (Arroll & Kendrick, 2018). Anxiety disorders appear to be caused by a combination of biopsychosocial factors, including genetic vulnerability, which interact with stressors to give rise to clinically significant syndromes (American Psychiatric Association, 2022). In the case of CU, those same situational stressors may also trigger histamine as a part of the body’s inflammatory response. Histamine is a chemical mediator released by the immune system, which causes blood vessel expansion and fluid release, resulting in skin redness, swelling, and itching (Kolkhir et al., 2022).
Anxiety disorders are the most prevalent psychiatric disorders in the college student population, with approximately 12% of college students are managing symptoms of an anxiety disorder (Pedreilli et al., 2015). However, most recent literature suggests that the global prevalence of anxiety disorders has significantly increased among college students (Li et al., 2022). Li and colleagues (2022) conducted a meta-analysis examining the global prevalence of anxiety and depression among college students. They discovered that the global prevalence of anxiety among college students was 39%, a stark increase since 2015. North American college students had a prevalence rate of 48.3%--the highest prevalence rate compared to other countries.
Anxiety in college students is demonstrated to be positively associated with irregular eating, poor sleep, low self-confidence, use of alcohol, and academic struggles (Li et al., 2022). Moreover, the COVID-19 pandemic has contributed to a surge in anxiety among college students as the prevalence rate of anxiety among college students has increased by roughly 2% since the pandemic’s start (Li et al., 2022). Adverse childhood experiences (ACEs) have also been associated with anxiety disorders (Watt et al., 2020), and college students with four or more ACEs are more likely to develop anxiety than students without ACEs. Systemic bodily inflammation has been associated with anxiety and other mental health disorders in college students who experience four or more ACEs (Watt et al., 2020).
Considering the high prevalence rate of anxiety among college students, several treatments have been developed to help college students manage anxiety symptoms. Cognitive behavioral therapy (CBT) has been demonstrated to be effective and efficacious in treating anxiety disorders (Kaczkurkin & Foa, 2015). CBT is a structured treatment focused on teaching individuals how to change maladaptive thoughts and expose themselves to anxiety-provoking situations. Exposure techniques have been widely demonstrated to be effective at reducing anxiety; however, the effectiveness of cognitive restructuring is more variable (Kaczkurkin & Foa, 2015). In addition to CBT, relaxation techniques that activate the parasympathetic nervous system have been demonstrated to reduce anxiety symptoms effectively (Conrad, 2007). Specifically, diaphragmatic deep breathing and progression muscle relaxation, two interventions geared to activate the parasympathetic nervous system, have been demonstrated to be effective at reducing anxiety symptoms (Dolbier & Rush, 2012). Moreover, mindfulness-based interventions, like body scans and mindful meditations, have been demonstrated to reduce anxiety (Gallego et al., 2014).
Specific to behavioral health treatment in primary care, the PCBH model generally assumes that a brief number of sessions (e.g., 1-4 sessions) is effective at reducing anxiety (Hunter et al., 2017). A brief CBT model can be utilized to effectively treat mild to moderate anxiety in primary care (Shepardson et al., 2020). Since episodes of care are shorter in primary care behavioral health services than traditional mental health services, interventions used to treat anxiety in primary care are more targeted and behaviorally based. The most common intervention used to treat anxiety in primary care is psychoeducation. Other common interventions used to treat anxiety in primary care are relaxation techniques (e.g., deep breathing, progressive muscle relaxation), problem-solving, pleasant activity scheduling, cognitive restructuring, and mindfulness (Shepardson et al., 2018, 2020). An episode of care for a patient presenting to primary care for anxiety treatment could look like the following: A patient struggling with anxiety schedules an appointment with their primary care provider to discuss treatment options. The primary care provider introduces the patient to the BHC to work on behavioral strategies to manage anxiety symptoms. During this first visit, the BHC provides psychoeducation about anxiety and teaches the patient a relaxation technique, deep breathing, to manage physical symptoms of anxiety. The patient follows up with the BHC at their next appt with their PCP. During the second appt, the BHC teaches the patient cognitive restructuring to manage maladaptive thoughts. The patient follows up with the BHC in one month. The patient reports a significant decrease in anxiety symptoms and agrees to follow up with the BHC as needed.
2 Case Introduction
Tara (a fictitious name) was an 18-year-old woman who presented to the campus primary care clinic with complaints of red, itchy ‘macular’ skin rash on her neck, feet and legs along with a sore throat. The rash had been present for one day, and she denied any known exposures. Chart review revealed that she had a history of Generalized Anxiety Disorder (GAD) and had been taking Buspirone (Buspar) 5 mg twice daily, hydroxyzine 10 mg PRN, and fluoxetine 40 mg daily. During the course of medical treatment in primary care, the providers took into consideration Tara’s prior diagnosis of anxiety, her anxious presentation in the office, and the impact of the condition on her sleep, academic and interpersonal functioning, and her overall quality of life (QOL). These struggles led to a referral to the on-site BHC for mounting anxiety about her current condition.
3 Presenting Complaints
Upon history taking and examination at her initial office visit, the primary care provider (PCP) determined that Tara’s rash was of unknown origin. She denied any history of allergies or eczema, and she denied any other physical complaints such as pain, chills, or fever. Tara had tried an over the counter anti-itch cream with no relief. She tested negative for strep. She was diagnosed with irritant contact dermatitis, unspecified trigger, and was prescribed Diphenhydramine (Benadryl) 25 mg every 4 hours and hydrocortisone 2.5% cream 2–4 times daily. Tara was told to follow up with the PCP if her condition did not improve in a few days.
Later that same day, Tara presented to a local hospital emergency room (ER) with the same complaints that had been reported at the university health clinic earlier that day. ER staff also noted increased blood pressure (BP) (137/83) and heart rate (HR) (113), which they suggested was related to her level of emotional distress over her dermatological condition. The ER physician diagnosed the patient with acute, allergic urticaria, and she was given intravenous Methylprednisolone (IV Solu-Medrol), which is a systemic corticosteroid designed to reduce inflammation. She was then discharged to home and told to follow up with her PCP.
The patient presented to the university primary care clinic again the next day. Chart notes revealed that the PCP noted that Tara presented with lip/hand/feet swelling in addition to the original rash. The patient reported that the symptoms had briefly improved with the IV steroid treatment given at the ER the prior night, but that the symptoms were worsening again. The rash was observed to have now spread to the back of both knees. Tara again denied use of any new soaps, lotions, detergents, foods, or substances. She denied having a sore throat, cough, congestion, fever, or chills. The PCP then added 20 mg of twice daily oral prednisone (another corticosteroid) to the existing medication regimen. The patient was then referred to a local Asthma and Allergy specialist.
Two days after initial presentation to PC, Tara presented to the Asthma and Allergy specialist’s office. The specialist determined that there were ‘no pertinent environmental exposures’ and ultimately diagnosed Tara with idiopathic urticaria. An antihistamine [Cetirizine (Zyrtec) 10 mg twice daily] was added to her medication regimen. At this time, the physician also ordered a ‘urticaria blood panel’ which included a complete blood cell (CBC) count with differential, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), liver enzymes, and thyrotropin (TSH) levels. Interpretation of the blood panel was that values were ‘consistent with inflammation or infection’. The patient was recommended to continue the course of her current medications and to follow up with the Allergy specialist in one month.
The day after the visit to the Allergy specialist, Tara again presented to campus primary care with continuing rash but was now exhibiting both lower extremity and upper extremity swelling and tenderness. The patient reported that she had not started on the prescribed prednisone and she was encouraged to do so.
Due to the patient’s prior diagnosis of anxiety, her anxious presentation in the office, and the impact of her condition on the patient’s sleep, functioning, and quality of life (QOL), the PCP referred the patient to the on-site BHC for help with managing the mounting anxiety about her current condition.
4 History
Tara’s medical and personal history was gathered through chart review, discussions with the PCP, and face-to-face interviews with the BHCs. The initial interview was conducted by a licensed psychologist BHC who also supervised the treatment conducted by a BHC trainee. Tara’s past medical history included diagnoses of GAD, depression, and seasonal allergies. She had undergone a surgical removal of small but painful subcutaneous lipoma (a non-cancerous fatty tumor) two years prior. The surgeon’s report from that procedure indicated that Tara had been experiencing ‘significant emotional distress’ related to the node because of its unknown etiology, and that she had been ‘less responsive to reassurance’ than expected by the surgeon.
Tara resides in a Midwest state with her father, stepmother, and younger siblings. She attends a Midwestern private university, where she lives in campus accommodations during the academic year. She reports having generally positive relationships with her immediate family, and spending time with them has been an effective means of managing her depression and anxiety in the past. She reports some intermittent tension with her stepmother that she defines as ‘generally manageable’.
Tara has irregular contact with her biological mother due to her mother’s reported longstanding history of a severe substance use disorder (SUD). Tara recognized this is a significant source of ongoing distress and worry, but she had not pursued any counseling or psychological services to address this. She reported attending two counseling sessions the previous semester after losing a family member to homicide, which was reportedly related to that family member’s severe SUD. Tara reports worrying that she will lose her mother to the same fate. She reported that her mental health diagnoses had been managed through medications prescribed by her PCP from home and that she had not participated in any other counseling or psychological services until the current BHC encounters.
5 Assessments
Tara completed the Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001) and the Generalized Anxiety Disorder Scale (GAD-7; Spitzer et al., 2006) at each BHC appointment. The PHQ-9 and GAD-7 are commonly used screening tools in primary care. During her first BHC appointment, the patient endorsed four symptoms of depression for a total score of 6 on the PHQ-9. This score is indicative of a mild level of depressive symptom severity (Kroenke et al., 2001). Her endorsed symptoms included anhedonia and difficulties with attention which were present for several days of the previous two weeks, as well as depressed mood and fatigue which were present for more than half the days in the previous two weeks. She endorsed that these symptoms made her daily functioning somewhat difficult.
On the GAD-7, Tara endorsed seven symptoms of anxiety for a total score of 11, which indicates a moderate level of symptom severity (Spitzer et al., 2006). She endorsed having trouble relaxing, feeling restless, and irritable for several days for the previous two weeks. She also endorsed feeling anxious, being unable to control her worrying, worrying about many different things, and feeling as though something awful may happen for more than half the days over the previous two weeks. As with her symptoms of depression, her anxiety symptoms made her daily functioning somewhat difficult.
During the second appointment, Tara endorsed three symptoms of depression that were not interfering with her daily functioning, for a total score of 3 on the PHQ-9. The endorsed symptoms included depressed mood, poor appetite, and difficulties with attention that were present for several days over the previous two weeks. Her PHQ-9 score showed a 3-point decrease between appointments. On the GAD-7, the patient also endorsed three symptoms of anxiety that were not interfering with her daily functioning, for a total score of 3 on the GAD-7. The endorsed anxiety symptoms included restlessness, irritability, and worries that something bad will happen and were present several days over the previous two weeks. Her GAD-7 scores showed a 7-point decrease between appointments suggesting her anxiety symptoms shifted from moderate severity into the minimal severity range.
6 Case Conceptualization
Treatment in this case was delivered from a CBT orientation. When considered from the perspective of Beck and Haigh’s (2014) generic cognitive model (GCM), the interaction of cognitive, behavioral, emotional, physical, and interpersonal factors was conceptualized to have contributed to the development and maintenance of a heightened state of anxiety. A central cognitive component, that of focus, suggests that Tara was exhibiting an attentional bias toward threatening information regarding the potential causes and consequences of her condition and away from information that might disconfirm her negative beliefs.
Specifically, Tara’s maladaptive cognitions included catastrophizing (interpreting the presence of hives as a sign of a serious underlying health issue, belief that her condition would never improve) and a sense of helplessness in management of her condition. Her attentional bias restricted her ability to broaden her awareness of additional possibilities (the potentially temporary nature of the condition, the likelihood of treatment options, past similar experiences that had resolved). Interpersonally, she struggled between a desire to seek comfort from family members while not wanting to burden them, and this also exacerbated her sense of distance from her mother, from whom she was already estranged. Behaviorally, Tara began to engage in more frequent skin checking, triggering an increase in symptom focus, and was consistently seeking new treatments and reassurance from medical providers. These physical symptoms of anxiety exacerbated an already sensitized stress response, creating a negative cycle.
To break this cycle, Tara’s mounting distress was approached from a bi-directional perspective. Within the GCM, clinicians attempt to assist the patient in shifting their perspective to promote broader awareness of more accurate or helpful information. The clearest starting point was to address Tara’s current anxiety surrounding her physical discomfort, as well as her uncertainty about the underlying cause (and subsequent best treatment for) her dermatologic condition. The maladaptive belief (that an emerging health problem was a sign of grave danger) intensified her emotional response to the skin condition, leading to exaggerated worry and rumination as a form of control. For these targets, identifying maladaptive conditions surrounding her health condition (i.e. catastrophizing) was thought to be a useful intervention point to reduce her distressing emotional reactions, which were altering her current self-care (i.e. sleep, class attendance) and overall quality of life. Using this conceptualization, the change intervention focused on gaining an accurate perspective about her concerns about the potential causes and consequences of the dermatological condition. The integration of the behavioral health provider into the same practice as her PCP allowed the health care team to address Tara’s medical concerns using language (after coaching by the BHC) sensitive to her anxiety (i.e. not just a typical psychoeducation visit).
However, the patient’s prior anxiety and depression diagnoses, and her ACES (parental divorce, parent with substance use disorder) were noted as predisposing factors for a state of chronic stress, which we hypothesized could heighten her vulnerability for inflammatory dysfunction. We hypothesized that this history of familial instability may have contributed to negative core beliefs surrounding a lack of safety, a lack of control, and a sense of helplessness and powerlessness. These core beliefs may have become activated by recent stressors such as her mother’s worsening substance use and subsequent lack of contact and her uncle’s recent death from the same disorder, leading to negative automatic thoughts such as “I might lose my mother and there is nothing I can do”. Her attempting to navigate these issues as a first-year college student in a new environment were also believed to contribute to her sense of disconnection and helplessness. We hypothesized that this sense of vulnerability and worry then increased when her skin condition first appeared, leading to a downward spiral of catastrophizing (“I am losing control of my body”) and sympathetic nervous system (SNS) activation. During the collaborative discussion of this conceptualization, Tara resonated with the BHC’s approach as they moved toward developing a treatment plan that would address these cognitive and physiological factors.
Thus, although the brief nature of the BHC model does not lend itself to processing past traumatic events, we were attuned to how her SNS may be playing a role in exacerbating her dermatologic condition and prioritized reducing the physiological activation as a way to enter the anxiety spiral and move toward ‘breaking the cycle’. See Figure 1 for Case Conceptualization diagram. Tara’s case conceptualization (modeled after Cully et al., 2020).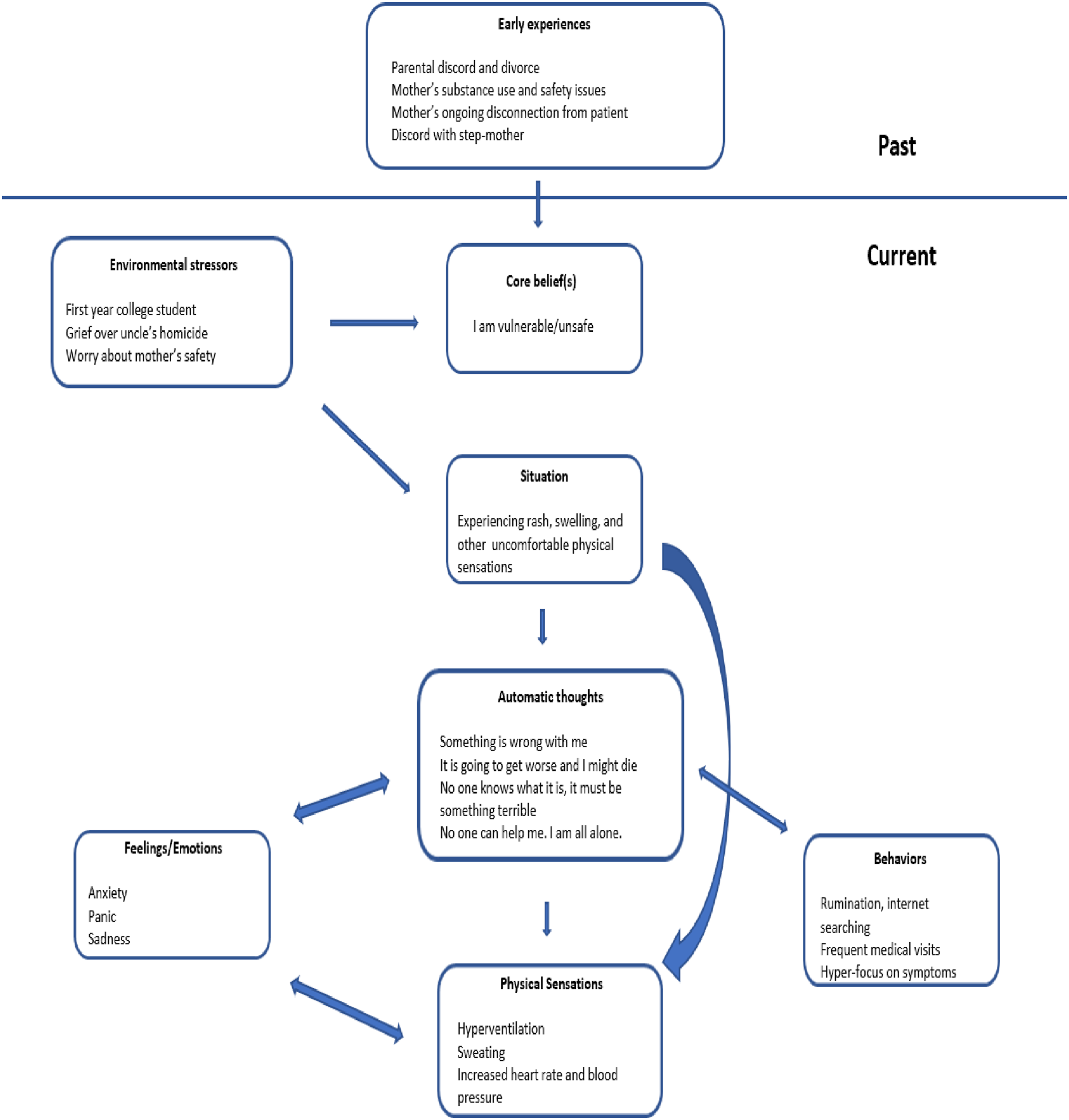
7 Course of Treatment and Assessment of Progress
Tara was first seen by BHCs the day following her third appointment with the PCP. She reported experiencing anxiety and depression related to the recent onset of unknown physical symptoms six days prior. She said that her anxiety symptoms had increased as the severity of her physical symptoms increased. She reported frequent rumination on her current health issues, the potential meaning of her symptoms, and the potential results of her bloodwork. She reported a history of anxiety and depression that had been well managed on Buspar and Fluoxetine for the last year. The patient completed the Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001) and the Generalized Anxiety Disorder scale (GAD-7; Spitzer et al., 2006) during the appointment and endorsed mild symptoms of depression and moderate symptoms of anxiety.
Due to the brief episodes of care within the PCBH model, the patient was shown multiple behavioral and cognitive strategies, based on the CBT conceptualization noted above, to help manage her anxiety during her first appointment. It was recommended that the patient practice diaphragmatic breathing with progressive muscle relaxation three times a day for the next two weeks in order to reduce activation of her sympathetic nervous system. She was also encouraged to track her thoughts related to her current stressors. She was given the option to challenge those maladaptive thoughts if she felt ready to take the next step. It was recommended that the patient also consider initiating services with the university counseling center to receive more long-term support regarding her distressing and conflictual relationship with her mother. The patient was planning to return home that afternoon following the appointment to spend time with family while awaiting the results of her blood work. She scheduled a follow-up with the BHCs for two weeks after to discuss how the techniques utilized during the visit impacted her anxiety levels and the management of urticaria.
One week after that visit, consultation with PCP and chart review revealed that Tara’s condition was improving, with some ‘waxing and waning’ of her rash, but overall improved. Within this particular practice, BHCs share office space with PCPs which allows for valuable brief, efficient face-to-face consultation in between patient visits and during breaks. This enhances the ongoing written communication conducted via chart reviews and direct EMR messaging.
Tara was seen for a BHC follow-up two weeks after her first BHC appointment. She reported significant decreases in her anxiety and depression in the two weeks between appointments. In that time, she had practiced diaphragmatic breathing three times a day, kept a log of her anxious cognitions and began to verbally challenge her catastrophic thinking by talking with her sister. She did not practice the progressive muscle relaxation but found the breathing exercises and thought logs to be helpful in reducing her anxiety. During this time, she also met with her provider to review her blood work results and her physical symptoms, which had continued to improve. She stated that ‘finally having an explanation’ for the onset of her physical symptoms, as well as relief from the symptoms, contributed to reductions in her anxiety.
During this second BHC visit, Tara’s progress was evaluated via use of the PHQ-9 and the GAD-7 as well as behavioral observations and assessment of her progress in daily functioning and reported quality of life. On the PHQ-9 and GAD-7, she endorsed minimal symptoms of both anxiety and depression, supporting the significant improvement since her last appointment. She was encouraged to continue practicing diaphragmatic breathing and to incorporate progressive muscle relaxation, as well as continuing to track and challenge her anxious cognitions. The patient was agreeable to this plan of action. The patient was unsure whether it would be more beneficial to pursue ongoing counseling or psychological services through the university or through a community provider in her hometown. The BHC discussed the pros and cons of initiating services in both settings and the patient ultimately decided to initiate services with the university counseling services. The patient’s initial appointment with the counseling center was made at the conclusion of this appointment. The BHC and patient had scheduled a final follow-up appointment for the following week, however the patient did not attend the appointment.
Chart review revealed that Tara attended her one-month follow-up with the allergy specialist to complete skin prick allergy tests and review a plan for managing chronic urticaria. The patient had been taking Cetirizine (Zyrtec) 10 mg daily but had stopped use a week prior in preparation for the allergy testing. The patient’s urticaria was mostly controlled with daily Cetirizine (Zyrtec), however she was still experiencing breakthroughs that would last 1–2 hours and generally go away with or without the additional use of Diphenhydramine (Benadryl). Her additional physical symptoms of joint aches and swelling that accompanied the urticaria in previous episodes were no longer present. The patient had not reported any breakthroughs in the days leading up to the appointment while she was not taking Cetirizine (Zyrtec). Allergy testing showed positive reactions for grass and cockroaches. The patient’s family resides on a farm, and she has exposure to grass and cockroaches when home. The allergy specialist provided information on control measures for managing her allergies and advised her to follow measures as much as possible. To manage chronic urticaria, the patient will continue taking Cetirizine (Zyrtec) 10 mg and start Fluticasone nasal spray (Flonase), one puff per nostril once a day. The patient is set to follow-up with the allergy specialist in one year.
8 Complicating Factors
The nature of integrated primary care mental health inherently differs from ‘traditional’ mental health services in several ways, including the typical number of treatment visits. For patients navigating problems of mild to moderate severity, a brief intervention may be sufficient to help the patient develop and strengthen coping skills, address specific symptoms, or provide support during a stressful time. The majority of patients benefit from an average of four or fewer visits (Bryan et al., 2012; Bryan et al., 2009; Cigrang et al., 2006; Corso et al., 2009; Ray-Sannerud et al., 2012). This was the case with Tara. Although she did not return for the third (and likely final) visit for the specified episode of care, this is an expected feature built into the PCBH model. In PCBH, the focus in on improving function within the patient’s life context and not on full elimination of symptoms (Robinson & Reiter, 2016). Because the goal of primary care integration is to provide patients with the right level of care at the right time, this level of flexibility is a key factor in helping to improve patient outcomes.
9 Access and Barriers to Care
Common barriers to mental health care include stigma, cost, and ease of access (Cunningham, 2009; Eisenberg et al., 2007; Mojtabai et al., 2011). Integrated primary care seeks to overcome these barriers by facilitating same day visits to an on-site BHC, thus reducing the need for frequent outside referrals and the complicated logistical issues that can arise. Because of the collaborative nature of the PCBH team model, patients benefit from providers that can freely share information that can accelerate the pace of providing effective treatment. Tara benefitted from each of the aspects of integrated care detailed above. In addition, because the BHC’s in this clinic were funded by the university, her services were provided at no added cost.
10 Follow Up
As noted previously, Tara was recommended to return for a third BHC visit which she did not attend. This is expected in primary care and is an advantage of the model. If the patient has experienced sufficient relief and improved functioning, they are generally assumed to have gotten what they came for. The model allows for consistent access to same day services for new patients in need of care.
Should Tara request additional services in the future, she knows that the BHC services are available. Her chart information will be readily available and she will benefit from that continuity of care. Should she return with concerns that prove to be of a more severe nature that necessitate a more intensive level of mental health care, the BHC will coordinate a referral to a specialty clinic within the local community.
11 Treatment Implications of the Case
The integration of mental health services into primary care can result in a range of benefits for patients and health care providers. In addition to providing comprehensive and collaborative care to address mental health concerns that may contribute to physical symptoms, BHCs can effectively help patients cope with common medical concerns. In Tara’s case, addressing her escalating anxiety in the face of unexplained physical symptoms appeared to enhance her current quality of life, and potentially prevented a worsening of her mental (and, perhaps, physical) health. Programs such as this can enhance patient outcomes and reduce longer-term health care costs. In addition, Tara has now had the positive experience of working with a mental health care provided as recommended by her trusted PCP; this may have led to an enhanced willingness to seek psychotherapy in addition to medication alone for her mental health symptoms and ongoing family stressors. This may also encourage her to seek care earlier in the course of symptom exacerbation. Finally, the collaboration between Tara’s BHC and her PCP allowed her health care provider to use appointment times efficiently and to rely on the BHC to address the complexities of Tara’s underlying stress and anxiety.
12 Recommendations to Clinicians and Students
Integrated primary care is designed to improve the effectiveness and efficiency of the PC clinic by helping a wide range of patients with a multitude of concerns. We recommend continued implementation of these services across the primary care system. This requires an expansion of programs providing opportunities for training in the integrated primary care model. Training of this nature offers a unique opportunity for trainees to gain experience working in a collaborative, multidisciplinary healthcare setting. By increasing the availability of mental health providers who are prepared to work in this setting, we can work toward addressing the shortage of mental health providers and improve access to care for patients. Overall, expanding this training in integrated primary care is an important step towards improving the delivery of mental health care and promoting overall health and wellbeing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.