
Abstract
The present case details a successful treatment response to 21 sessions of Acceptance and Commitment Therapy (ACT) delivered via teletherapy for mixed anxiety and depressive symptomology during the COVID-19 pandemic. The client (“Natalie”), a 19-year-old, White, cisgender female, presented to a university training clinic reporting primary problematic anxiety consistent with a diagnosis of Generalized Anxiety Disorder. The therapist conceptualized Natalie’s anxiety through the ACT psychological flexibility model, wherein Natalie’s challenges appeared to be maintained by experiential avoidance and lack of committed action. This case highlights (a) the unique challenges of treating someone with pervasive anxiety amid the uncertain context of the COVID-19 pandemic, (b) repeated assessment of transdiagnostic processes to inform intervention focus, and (c) the process of ACT teletherapy. Symptom, process, and outcome measures taken bi-weekly throughout therapy suggested theoretically consistent and reliable treatment responses. Clinical implications of the case are discussed.
Keywords
1 Theoretical and Research Basis for Treatment
Acceptance and Commitment Therapy (ACT; Hayes et al., 2012) is an empirically supported, transdiagnostic form of cognitive-behavioral therapy (Hayes & Hofmann, 2017). Unlike traditional Cognitive-Behavioral Therapy (tCBT), ACT does not consider unpleasant private events, such as anxiety-related physiological responses or so-called negative thoughts, to be problems in and of themselves. Rather, these internal experiences are regarded as a natural and inevitable part of the human condition. Accordingly, ACT conceptualizes anxiety disorders as resulting from rigid and inflexible attempts to control and avoid anxious thoughts, feelings, and sensations. The attempted solutions to anxiety become the true problem, not the anxiety itself. This conceptualization is also supported by emotion science, where efforts to suppress or control distressing thoughts and feelings often paradoxically potentiate their occurrence and severity (e.g., Campbell-Sills et al., 2006; Wegner et al., 1987), resulting in problematic avoidance behaviors and life impairment (Forsyth et al., 2006). In line with this view, ACT aims to change an individual’s relationship with internal experiences from one of avoidance or control to one that is open and accepting in the service of choosing values-consistent behaviors with whatever one might think or feel (Eifert et al., 2009). Accordingly, overarching targets of ACT are to increase psychological flexibility (PF) and decrease psychological inflexibility (PI).
Psychological flexibility is defined as the ability to behave congruently with freely chosen values, in the present moment, even while experiencing unwanted thoughts, feelings, and sensations (Hayes et al., 2012). ACT influences psychological (in)flexibility by targeting the six interrelated processes that theoretically comprise the overarching construct. These processes include: acceptance (i.e., willingness to nonjudgmentally contact and make space for unwanted private events as they are), contact with the present moment (i.e., directing attention to the here and now), defusion (i.e., viewing thoughts as mental experiences that need not be trusted or believed in guiding choices and actions), self-as-context (i.e., flexible perspective taking ability to notice a distinction between the “you as observer” and the “you as identified with your learning or conditioning history and lived experience”), values clarity (i.e., getting and staying in touch with what matters most in life), and committed action (i.e., acting in ways that align with values). Conversely, psychological inflexibility is defined as “the rigid dominance of psychological reactions, over chosen values and contingencies, in guiding action” (Bond et al., 2011, p. 678). Inflexibility processes are associated with a vast range of mental health syndromes (e.g., anxiety and mood disorders), and other psychological problems.
As a transdiagnostic approach, ACT is designed to target the common psychological processes that theoretically underpin this wide range of seemingly disparate mental health conditions, including common daily challenges. Indeed, a recent meta-analysis of meta-analyses (i.e., Gloster et al., 2020) showed that ACT, through targeting the same small set of processes, is effective for anxiety, depression, substance misuse, distress from chronic pain, psychosis, problematic stress, somatic complaints, eating disorders, transdiagnostic combinations of conditions, and improving quality of life. These findings support the notion that various mental health concerns share common underlying processes (e.g., psychological inflexibility), which ACT effectively addresses. Thus, clients with comorbid and complex presentations are likely to benefit from transdiagnostic therapies such as ACT.
ACT is also a flexible therapy, and can be delivered in face-to-face individual therapy, group therapy, teletherapy, and self-help formats. Flexibility is a hallmark of the ACT model, as is its pragmatic and contextually sensitive approach which aims to treat a range of behaviors that potentiate suffering and get in the way of living a full, rich, and meaningful life. ACT’s flexibility, pragmatic approach, and focus on treating behaviors that hinder a meaningful life make it well-suited for the dynamic challenges that arise during public health crises such as the COVID-19 pandemic. For instance, Cordaro et al. (2021) found that those with generalized anxiety disorder (GAD) experienced heightened stress, loneliness, fatigue, and reduced quality of life during the COVID-19 pandemic. This work suggests that pandemic-specific problem sequelae extended beyond the typical symptom-based boundaries of a mental health disorder, indicating a flexible treatment approach with wide-ranging effects.
ACT is also a model rather than a fixed set of techniques. As such, techniques from various approaches may be integrated into therapy while maintaining fidelity to the ACT model. The present case highlights this point by describing the use of techniques commonly associated with Motivational Interviewing (MI; see Rollnick & Miller, 1995), such as scaling questions and envisioning exercises, in an ACT-consistent manner. ACT and MI have also been described as distinct yet complementary interventions aiming to promote valued living (Bricker & Tollison, 2011), with examples of their clinical integration emerging in the literature (e.g., Ehman & Gross, 2019; Thurstone et al., 2017). Lastly, the telehealth context of the case provided unique challenges and opportunities which are discussed in light of best practice telepsychology guidelines (see APA, 2013) within the extreme extenuating circumstances of the pandemic and with special consideration to telemental health measurement-based care (tMBC; Douglas et al., 2020).
2 Case Introduction
“Natalie” (pseudonym), a 19-year-old White cis-gender undergraduate female, sought treatment after the onset of the COVID-19 pandemic at a university-affiliated community psychology clinic in the northeastern United States. Referred by her psychiatrist, she presented with primary complaints of life-impacting anxiety and worry about various issues. Her therapist, a White cis-gender male clinical psychology doctoral student, was supervised by licensed clinical psychologists. To protect her identity, identifying details and specific daily life activities were altered or replaced with alternatives.
3 Presenting Complaints
Natalie described herself as being “always an anxious person” and presented with heightened anxiety, which she described as worsening since the COVID-19 pandemic began. Her worries centered on health, virus transmission, adhering to pandemic guidelines, and concerns about others’ perceptions, her physical appearance, and time management. In response to worry, she experienced somatic symptoms like tension, lightheadedness, and nausea, along with feelings of anger and resentment. Based on her account, the above symptoms were exacerbated by not being able to have a “normal” college experience because of the pandemic.
She also endorsed feelings of loneliness and isolation, having few and unsatisfying close relationships, and being out of touch with interests she used to enjoy. She isolated herself from friends, avoided running due to fears of injury or judgment, wore modest clothing to avoid attention, and limited driving to essential trips out of fear of accidents. At work, she felt constantly stressed about contracting or spreading the virus, leading to physical and mental tension. Natalie expressed feeling controlled by her worries, unable to break free from ruminative thoughts, and found her previous coping strategies ineffective. Natalie reported that her anxiety and worry substantially interfered with her functioning in important domains of her life. Despite these struggles, she denied any suicidal ideation at intake and throughout treatment.
4 History
Natalie was born without complication to married parents in the northeastern United States and described her family as generally supportive. She denied experiencing any physical or emotional abuse, significant hardships, or traumatic life events. She endorsed a lengthy mental health history in her biological family including anxiety and depression, though she denied any personal or family history of substance abuse. Natalie described herself as an anxious person from a young age, preoccupied with schoolwork, perfectionism leading to excessive time on assignments, difficulty concentrating due to worry, and rigid rule-following that sometimes caused conflicts with peers. The early stages of the COVID-19 pandemic had significant social and behavioral health impacts globally. During this time, Natalie completed her senior year of high school virtually. As an essential worker in a public-facing job, her fear of contracting and spreading COVID-19 grew. To avoid spreading the virus, she avoided non-essential in-person socialization, leading to increased isolation, bitterness, and heightened anxiety and worry.
Natalie also experienced depressive symptoms after the pandemic began, including low mood and energy, anhedonia, irritability, and appetite fluctuations. She hoped starting college would help, but when she arrived, the ongoing pandemic increased her stress. She struggled to focus on studies due to worries about COVID-19 and felt at odds with her peers over their responses to mitigation rules.
Consequently, Natalie sought therapy at her college counseling center. Despite this, her anxiety continued to negatively impact her daily life, leading her to distance herself from peers. She described this period as a low point, rarely leaving her room, halfheartedly attending online classes, and feeling isolated and hopeless about the future. She reported hypersomnia, overeating, and weight gain. She also met with a psychiatrist who diagnosed her with Generalized Anxiety Disorder and prescribed an antidepressant. While the antidepressant improved her sleep and appetite, her anxiety, somatic symptoms, and lack of engagement persisted. After returning home, she felt less depressed but feared slipping back into isolation and disengagement. Thus, her psychiatrist referred her to our community-based clinic for further treatment.
5 Assessment
Overview
Assessment involved collecting and synthesizing data throughout treatment. The first session featured an unstructured clinical interview to gather psychosocial history and information about her presenting problems, leading to preliminary diagnostic impressions. The second session focused on collaboratively conceptualizing the functional interrelation of symptoms, processes, and anticipated outcomes using the ACT Matrix (Polk et al., 2016). Dimensional symptom, transdiagnostic process, and life satisfaction measures were administered in sessions one and two to establish a baseline and ensure consistency in Natalie’s reporting. These self-report measures were then administered and discussed at the beginning of every other session for the remainder of therapy. To administer measures virtually, the therapist screen-shared the measures, Natalie provided verbal responses, and the therapist recorded them. The therapist then scored the measures and reviewed the results with Natalie to guide clinical decision-making and collaborative care (Douglas et al., 2020; Scott & Lewis, 2015).
Symptom Assessment
To assess and monitor symptoms across treatment, Natalie was given the 21-item, self-report Depression, Anxiety, and Stress Scale, 21 (DASS-21; Henry & Crawford, 2005) at baseline (i.e., at sessions one and two), then again, every other session throughout the course of treatment. The DASS-21 is a widely used short version of Lovibond and Lovibond’s (1995) 42-item Depression Anxiety and Stress Scale. The DASS-21 contains three, 7-item subscales measuring dimensions of depression, anxiety, and stress over the past week. Each item is rated on a Likert type scale anchored from 0 = “Did not apply to me at all” to 3 = “Applied to me very much, or most of the time.” Scale totals are calculated by adding the scale items and then multiplying by a factor of two (Henry & Crawford, 2005; Lovibond & Lovibond, 1995). The measure retains sound psychometric properties when administered virtually (Peters et al., 2021). This measure was chosen from various symptom screeners because it includes a validated stress subscale, which was valuable for monitoring stress alongside anxiety and depression in the context of the pandemic.
Transdiagnostic Process Assessment
To monitor ACT-specific processes across treatment, Natalie completed the 12 psychological inflexibility items from the Multidimensional Psychological Flexibility Inventory 24 (MPFI-24; Grégoire et al., 2020), a virtual-administration-validated short form of the original 60-item MPFI (Rolffs et al., 2018). The MPFI-24 assesses six psychological flexibility and six inflexibility processes from the ACT Hexaflex model (Hayes et al., 2012). Each of the twelve subscales has two items rated from 1 = “never true” to 6 = “always true,” evaluating flexibility and inflexibility processes over the past two weeks. Subscale scores are averages of the two items, and the six flexibility and six inflexibility subscale scores can be averaged to create global composite scores, with greater scores indicating more flexibility or inflexibility. Only the 12 inflexibility items were given in the present case. This decision was made to reduce assessment time and burden, and to focus on processes where Natalie was getting ‘stuck’. Psychological flexibility was evaluated through alternative means, such as Natalie’s report of flexible, values-based behavioral engagement outside of therapy and observations of her behavior in session.
Outcome Assessment
To monitor satisfaction with life, Natalie completed the 5-item Satisfaction with Life Scale (SWLS; Diener et al., 1985) in sessions one and two, and then every other session throughout treatment. The SWLS contains five items (e.g., “In most ways my life is close to my ideal”) which map onto one factor representing global life satisfaction. Each item is rated on a Likert type scale from 1 = “Strongly disagree” to 7 = “Strongly agree.” Validated for online use (e.g., Howell et al., 2010), the SWLS was the primary therapy outcome measure, aligning with broader aims of ACT; namely, to help Natalie to be living a richer, more meaningful life, thereby increasing her life satisfaction.
The proportion of values-guided (approach) versus avoidance-motivated (avoidance) behaviors in daily life is a key indicator of change in anxiety and depressive disorders (Grosse Holtforth, 2008; Struijs et al., 2018). In session two, while completing the ACT Matrix, Natalie was asked to estimate the percentage of her daily behaviors aimed at avoiding unwanted internal experiences (i.e., the top left quadrant of the Matrix), and similarly those aimed at approaching her values and living as the person she wants to be (i.e., the top right quadrant of the Matrix). This metric provides insight into how much Natalie perceived approach or avoidance as guiding her choices and actions.
6 Case Conceptualization
In ACT, the main outcome criterion is ‘successful working' based on the client’s values and goals (Bach & Moran, 2008). As such, Natalie’s presenting problems, behavior patterns, and relevant learning history were explored in relation to (a) her values (i.e., is this working for you?) and (b) the six psychological inflexibility processes (Hayes et al., 2012) that are thought to maintain her problems and interfere with desired changes.
From the start of therapy, Natalie clearly articulated how she wanted to live her life, identifying core values such as assertiveness, spontaneity, fun, independence, intimacy, authenticity, presence, and fitness. Thus, there was not a need to guide Natalie through a formal values clarification exercise (e.g., values card sort). Natalie also easily identified behaviors aligned with her values, such as taking spontaneous trips, running with others or alone, going to the gym or dining hall alone, wearing preferred clothing, and being open and authentic with others. Her engagement in these values-consistent behaviors, when practical and life-enhancing, defined successful working in this case.
Though Natalie was clear about her values and able to articulate actionable ways to move forward, she was not engaging in these behaviors consistently. Much of her suffering appeared to stem from the gap between the life she wanted and the life she was living (see Rogers, 1950). Using the psychological inflexibility model of ACT helped identify where Natalie was stuck and guided targeted interventions to promote effective change. Each of the psychological inflexibility processes were evaluated for their role in maintaining her suffering.
Despite Natalie’s value clarity, she faced significant barriers to acting on her values. When Natalie considered taking actions aligned with her values, she was confronted with anxious thoughts about feared outcomes, which pulled her out of the moment and into her head (i.e., lack of contact with the present). Natalie bought into these worries and entertained them for long periods (i.e., fusion), leading to somatic sensations such as stomach upset and tension. Because Natalie was focusing on worries rather than her values, and saw the somatic symptoms of anxiety as unwelcome, she often opted out of activities that she knew could bring her joy and fulfillment (i.e., inaction). This inaction appeared to be linked to her desire to escape the feared outcomes she imagined and to reduce unwanted sensations associated with her anxiety (i.e., experiential avoidance). As a result, she felt stuck, powerless, and often resorted to behaviors that were not aligned with her values, including scrolling social media or watching TV (i.e., inaction).
Holding onto rigid stories about how things “should be” and how her life should look (i.e., self-as-content) further illuminated the gap between her desires and inaction, leaving her feeling angry, bitter, and eventually depressed. She noted that this cycle would often repeat on a loop as she bought into and fused with those thoughts. Her rigid relationship with these anxious and depressive thoughts and sensations led her to choose behaviors that offered short-term relief from anxiety (i.e., negative reinforcement) but conflicted with her long-term values. Living predominantly under aversive control (i.e., choices and actions influenced by the presence of, and desire to avoid, aversive thoughts and feelings) evoked more anger and depressive symptoms and low motivation to engage in subsequent desired activities, leading to downward spirals.
7 Course of Treatment and Assessment of Progress
The psychological processes which maintained Natalie’s suffering and kept her from taking action were the primary targets for intervention. Natalie’s psychological inflexibility was targeted by addressing each of the six psychological (in)flexibility processes. Natalie’s treatment consisted of learning to be present with her history and current lived experience (i.e., present moment awareness, self-as-context), opening up to and developing a harmonious relationship with her private events (i.e., acceptance, defusion), and choosing and persisting in behaviors which move her toward the life she wants, even in the presence of anxiety, worry, and other difficult internal experiences (i.e., values clarity, committed action). The implementation of ACT is nonlinear and is akin to a fluid “dance” between processes (Eifert & Forsyth, 2005). However, core ACT intervention strategies have been articulated for the treatment of anxiety-related suffering (e.g., Eifert et al., 2009), which were loosely followed in the present case. As noted above, the MPFI-24 also helped focus the interventions on relevant processes that could be targeted for change.
Course of Treatment
Intake Assessment and Alliance Formation (session 1)
Apart from information gathering for purposes of case conceptualization, the initial therapy session also focused on strengthening “common factors” known to impact outcomes (e.g., Wampold, 2015). The therapist actively listened, was nonjudgmental, worked to ensure goal alignment, and instilled optimism about therapy (Constantino et al., 2018). To enhance virtual teletherapy interactions, the therapist aimed to maximize the perception of eye contact by raising his seat and lowering the webcam to reduce gaze angle between the webcam and the therapist’s eye gaze (see Grondin et al., 2020 for detailed guidance). Natalie did not initiate therapy to rid herself of symptoms associated with her diagnoses. Rather, she hoped to improve her life and to act more like the person she knew she wanted to be. Thus, therapy began with an idiographic functional analysis of factors keeping Natalie from living as she desired.
Phase 1. Creating the Context for Acceptance (sessions 2-4)
This phase focused on a collaborative formulation of Natalie’s problems and establishing acceptance as an alternative to controlling internal experiences (Eifert et al., 2009). In session two, the therapist guided Natalie through the ACT Matrix (Polk et al., 2016) to illustrate the interrelation of ACT processes linked with Natalie’s private and public events. The ACT Matrix (AM) served three main functions in this case. First, it aided ACT case formulation, simultaneously assessing Natalie’s ability to distinguish private events and think functionally about behavior. Second, the AM functioned as a creative hopelessness intervention by helping Natalie see where she was getting stuck despite trying various strategies to control unwanted private events. Third, the therapist used the completed AM to facilitate informed consent, goal alignment, and to discuss treatment targets and expected outcomes from an ACT framework.
Natalie demonstrated an excellent ability to distinguish her private events and reported surprise upon realizing how her escape behaviors both functioned to keep her from living the life she wanted and did not work to control her private experiences in any durable way. This surprise encouraged her to align with the ACT conceptualization and consent to ACT-guided treatment. Natalie estimated that 80% of her behaviors fell in the top left quadrant of the AM (i.e., attempts to escape or avoid private events), whereas only 20% of her behaviors fell in the top right quadrant (i.e., values-guided approach behaviors). This realization and reflection motivated Natalie to try something new which created the context for acceptance. Moreover, the therapist offered psychoeducation about the survival functions and adaptivity of anxiety to lay the groundwork for a more accepting relationship with anxiety. At the end of the second session, Natalie was invited to notice towards and away moves (i.e., approaching values or avoiding internal pain; Polk et al., 2016) throughout the week to develop a functional understanding of behavior and build awareness of her choices.
Sessions three and four focused on cultivating mindfulness skills to help Natalie develop a new relationship with her challenging internal experiences. Interventions introduced in these sessions included “mind watching” (Forsyth & Eifert, 2016) and simple defusion exercises such as adding “I notice I’m having the thought that…” (Harris, 2021) before her thoughts. While mind watching, she was guided through a brief eyes closed exercise and instructed to imagine herself in a blank room, with thoughts entering in one door and exiting out a door on the other side of the room. Upon completing this exercise, Natalie reported “there’s something else inside me other than my thoughts,” indicating a positive response to recognition of the self as observer being separate from the self as her thoughts. Natalie imagined her thoughts were like visitors whom she could choose to interact with or not, and that they all eventually came and went. Natalie was invited to keep a “visitor log” between sessions to practice noticing the coming and going of her thoughts. The therapist guided Natalie through perceiving recurring themes of thoughts as stories told by the mind, which Natalie called “frequent visitors” (e.g., “here’s the ‘rule breaking’ visitor”).
Natalie was later guided through adding defusing statements at the beginning of her thoughts (e.g., “I notice I’m having the thought that…”) or thanking her mind for ‘inviting the visitor,’ as a means of fostering a non-judgmental, defused, and observer stance toward her internal experiences. Natalie was also guided through applying the same techniques to her somatic sensations. Despite increased work stress from layoffs and heightened COVID-19 uncertainty, Natalie consistently practiced developing defusion skills between sessions and reported that they were helpful in allowing her to sidestep unhelpful ruminative cycles. Given her progress with mindfulness and defusion interventions, treatment shifted to focus on values and committed action.
Phase 2. Connecting with Values and Engaging in Flexible Exposure (sessions 5-8)
The second phase of therapy aimed to get Natalie in touch with what mattered most to her in life and to cultivate skills to act flexibly in the presence of fear and anxiety (Eifert et al., 2009; Eifert & Forsyth, 2005). The main interventions introduced in sessions 5-8 included personifying the mind, developing a flexible and informal values-based exposure hierarchy, and engaging in in-vivo, imaginal, and emotional exposure. First, Natalie was guided through mind personification (Forsyth & Eifert, 2018). She identified her mind as a separate individual with its own name (“Sarah”) and offered a detailed visual description. Personifying the mind allowed the therapist and Natalie to talk about her anxious thoughts and feelings as coming from a separate entity that Natalie could choose to listen to or not. Natalie responded well to this intervention and reported feeling greater distance from her thoughts and feelings after considering they came from her mind, “Sarah.” Natalie was next guided through developing a values-guided exposure hierarchy.
The goal of exposure in ACT is to increase willingness to experience unpleasant private events in service of engaging in values-consistent behavior (Twohig et al., 2015). Because reducing symptoms of fear and anxiety is not the goal in ACT, the hierarchy is based on behaviors that align with how the client wants to be in their life. Progress through the hierarchy is based on willingness to experience unpleasant private events which arise alongside values-based actions (see Twohig et al., 2015). Here, the process of developing a hierarchy was organic, informal, and responsive to Natalie’s priorities and the changing contexts.
In multiple sessions, Natalie was guided through imagining herself engaging in valued behaviors she identified while the therapist encouraged her to be in contact with anxious thoughts and feelings that arose during the imagery. She was prompted to stay with, mindfully notice, describe, and differentiate her thoughts and feelings in session. For emotional sensations, this included defining the shape, boundaries, color, texture, temperature, and other perceived properties of the internal sensations she was experiencing. Between sessions, she engaged in at least one valued behavior per week. The target behavior for the week was determined by Natalie based on her priorities and changing contexts and aligned with her initial behavioral goals. Examples of these behaviors included wearing brightly colored clothes to a shopping mall and exercising in the presence of other people. In subsequent sessions, Natalie reported what sensations she noticed and what Sarah, her mind, was telling her during the experiences. We focused debriefs on why, and for what greater purpose, she chose to persist in the behavior in the presence of these anxious thoughts and sensations. Natalie reported being excited to move back to school and was feeling positive momentum in therapy. She received her first COVID-19 vaccine in the early wave of vaccination efforts due to qualifying as a front-line worker, which she said gave her a feeling of relief. Her self-report measures at this time reflected a decrease in symptoms and a modest increase in life satisfaction.
Phase 3. Rolling with Environmental Challenges (sessions 9-10)
After arriving back on campus, Natalie realized she was one of few vaccinated people in her dormitory. She also reported that most of her peers were not abiding by safety protocols and attended large gatherings without masks. Infections of COVID-19 spread quickly through her campus community causing the university to enforce strict mitigation measures. Students were told to remain in their dorm rooms, attend class online, and leave only for essential activities.
Natalie struggled to manage the flood of fear, anxiety, and anger associated with being back in isolation. She reported increased anhedonia, fatigue, apathy, and difficulty engaging in activities of daily living. She reported thoughts that the “pandemic was never going to end” and there was “no point in working hard” on herself if she could not do what she wanted to be doing. Despite these feelings, she felt pressured to maintain a facade of being “fun and carefree” for her roommate and peers, adhering to the verbal rule that sharing feelings with others would burden them. As she fused with these thoughts, she masked her feelings and felt inauthentic. Therapy then focused on addressing her depressive symptoms and applying ACT principles to her new college and pandemic circumstances.
The therapist aimed to normalize and validate Natalie’s reactions to her environmental constraints. Consistent with the ACT concept of aligning with clients in the challenges of the human condition, the therapist disclosed his own experiences of feeling and thinking many of the same things Natalie was describing. Natalie reported this disclosure helped her feel more connected to the therapist and less guilty or embarrassed for her reaction. The therapist reflected this to Natalie as an analogue for how Natalie was acting with her roommate and others. Natalie ultimately valued authenticity with others. Yet, she found her behavior was guided by how she thought others wanted her to be. The focus of these sessions turned to recognition and pursuit of the opportunity for value-guided (i.e., more authentic) interpersonal behavior.
Natalie was invited to tell her close peers about how she was feeling and to show her sadness, disappointment and frustration in response to the pandemic mitigation measures and behavior of other students. She was invited by the therapist to notice thoughts and feelings which arose during this imaginal exposure, and to nonjudgmentally name and describe them. Natalie then increased her authentic communication with her close peers between sessions with apparent good effect. Natalie’s openness resulted in a sense of increased intimacy and connectedness. This closeness strengthened Natalie’s social support and reinforced that emotional authenticity can lead to deeper interpersonal connection. Importantly, Natalie also felt connected to a new sense of living authentically for herself rather than for the perceived wants or needs of others.
Phase 4. Living a Valued Life With Anxiety (sessions 11-18)
Sessions 11-18 focused on increasing Natalie’s engagement in valued behaviors and troubleshooting barriers and challenges while generating self-compassion. During this phase, the therapist also incorporated Motivational Interviewing (MI; Rollnick & Miller, 1995) techniques to increase Natalie’s motivation and willingness to engage in valued behaviors and implement her ACT skills between sessions. In each session, Natalie identified specific behaviors that aligned with her values and that she wanted to engage in. These behaviors were those she previously avoided and/or continued to fear. The therapist introduced simple self-compassion-enhancing components to the interactions in these sessions by validating frustration and asking perspective-taking questions. The therapist modeled mindfulness skills by also using defusing reflections. For instance, when Natalie said something like, “I want to go on a run, but I am still worried about getting injured,” the therapist, in turn, responded by stating “It seems that your mind is telling you that if you run you might get injured.” These reflections functioned to create distance between Natalie as observer and the products of her mind, to remind her to implement defusion skills, and as MI-consistent reflections to evoke change talk.
As Natalie moved toward committing to engage in a value-guided behavior, the therapist worked with her to construct specific behavioral goals and employ behavioral activation techniques (e.g., identifying and scaffolding behavior toward engaging in the process, scheduling the day and time for this engagement, anticipating barriers, and managing contingencies; Kanter et al., 2010). If these conversations evoked self-critical thoughts (e.g., “I shouldn’t still care about this because I know it’s just in my head”), the therapist encouraged compassion (e.g., “What might you say to a friend in response?”). The therapist also normalized Natalie’s process of change and disclosed shared experiences when Natalie became self-critical (e.g., “My mind says stuff like that to me sometimes, too – I think this is our minds’ attempt at getting us to make changes”; Harris, 2021). MI techniques used here also included evocation about importance of the behavior, assessing willingness for engagement in behavior on a 1-10 scale, and revising weekly behavioral goals as needed. This phase of therapy became highly useful as indicated by Natalie’s report and the therapist’s observations.
Over this phase, Natalie regularly engaged in behaviors she said were once difficult for her to imagine at the outset of therapy and evolved as the pandemic context shifted. She went running alone, spontaneously called up friends to meet for lunch, went grocery shopping alone, resumed artmaking, attended social events on campus, and joined the university running club. Natalie encountered numerous barriers during this time as well, though her flexibility and burgeoning self-compassion in the presence of these barriers demonstrated to her and the therapist that Natalie was internalizing and applying the skills learned in ACT. Overall, Natalie was increasingly engaged in previously avoided but highly valued behaviors. She was able to navigate real-world barriers with increasing flexibility and with reduced guilt and self-criticism. Her qualitative report, the therapist’s observations, and Natalie’s self-report measures indicated progressive improvement across this phase of therapy.
Phase 5. Doing it alone – Preparing for Termination (Sessions 19-21)
In session 19, Natalie brought up thoughts regarding termination. Natalie reflected on the progress she had made and expressed confidence in her ability to maintain progress. She also reported anxious thoughts about ending therapy. She said introducing the topic of termination felt like an application of what she learned during therapy (i.e., noticing her fears about going without therapy but electing to do it anyway due to her trust in herself). Natalie and the therapist collaboratively agreed to taper sessions, such that two weeks passed between the final sessions. During the remaining sessions, the therapist mainly reinforced Natalie’s independent application of skills and maintenance of gains and provided supportive reflection, gratitude, and admiration for her work during therapy. In the final session, the therapist showed her the ACT Matrix diagram she completed in session two. This sparked a conversation and reflection about her growth during therapy. In stark contrast to the start of therapy, Natalie reported feeling like 70% of her behavior was now values-guided (i.e., top right quadrant of AM), and around 30% was aimed at escaping private events. She considered this a success, and the therapist agreed.
Assessment of Progress
Natalie’s treatment was considered successful based on convergent evidence across quantitative self-report measures, Natalie’s qualitative report, and therapist observation of in-session behavior. Clinically significant changes in satisfaction with life, symptoms, and processes were evident to Natalie and the therapist and are elaborated upon below.
Satisfaction with Life
Session by Session Data, First-to-Last Session Change Scores, and Calculated Reliable Change Indices.
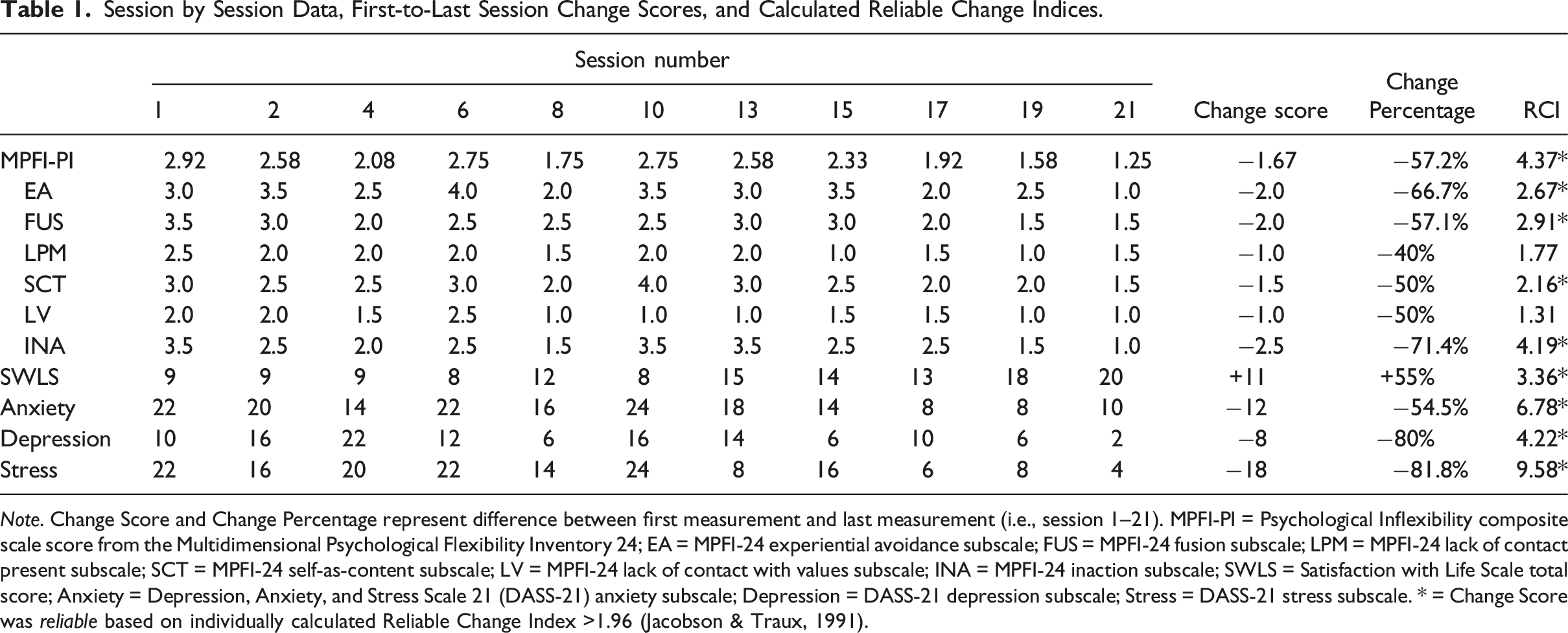
Note. Change Score and Change Percentage represent difference between first measurement and last measurement (i.e., session 1–21). MPFI-PI = Psychological Inflexibility composite scale score from the Multidimensional Psychological Flexibility Inventory 24; EA = MPFI-24 experiential avoidance subscale; FUS = MPFI-24 fusion subscale; LPM = MPFI-24 lack of contact present subscale; SCT = MPFI-24 self-as-content subscale; LV = MPFI-24 lack of contact with values subscale; INA = MPFI-24 inaction subscale; SWLS = Satisfaction with Life Scale total score; Anxiety = Depression, Anxiety, and Stress Scale 21 (DASS-21) anxiety subscale; Depression = DASS-21 depression subscale; Stress = DASS-21 stress subscale. * = Change Score was reliable based on individually calculated Reliable Change Index >1.96 (Jacobson & Traux, 1991).
Symptoms
Natalie demonstrated reliable reductions in anxiety, depression, and stress as measured by the DASS-21. Based on cutoffs established for the DASS-21 comprising a sample of 2914 (64.2% female) university students and community workers (Lovibond & Lovibond, 1995), Natalie’s anxiety moved from “extremely severe” at pre-treatment to “moderate” at post-treatment. Natalie’s depression was “mild” at pre-treatment and “normal” at post. Her stress was “moderate” at pre-treatment and “normal” at post. From pre-to-post treatment Natalie demonstrated clinically significant reliable change (Jacobson & Traux, 1991) on indices assessing anxiety, depression, and stress (see Table 1). These scores converged with Natalie’s report of feeling less anxious, depressed, and stressed. Though Natalie still reported moderate anxiety at post-treatment on the DASS-21, she evidenced increased flexibility in the presence of her internal experiences consistent with anticipated treatment response to ACT. The therapist also observed that Natalie appeared less distressed about her anxiety, suggesting that her anxiety could naturally fluctuate without derailing her engagement in valued behavior or evoking the downward spiral indicative of Natalie’s pre-treatment presentation.
Processes
Natalie demonstrated theoretically consistent and statistically reliable reductions in psychological inflexibility overall, as well as reductions in each of the six underlying processes, as measured by the MPFI-24 (see Table 1). Without established cutoffs, normative data in the literature can provide some context for these scores. Grégoire et al. (2020) reported normative data from the MPFI-24 among 2688 English speaking adults. Natalie’s global inflexibility composite score at pre-treatment (i.e., 2.93) was above that normative mean (M = 2.73; SD = .90; Grégoire et al., 2020) and fell over one standard deviation below the normative mean at post-treatment (i.e., 1.25; see Table 1).
Natalie’s varied subscale scores demonstrate the clinical utility of the MPFI-24. Specifically, identifying elevated process scores at pre-treatment aided the therapist in selecting targeted interventions for those processes. By taking these measures at the beginning of every other session, we tailored intervention focus of that session toward processes with elevated scores. Natalie also qualitatively reported improvements in flexibility. She described numerous situations she believed would have “derailed” her in the past due to evoking anxious thoughts and feelings, but which she increasingly navigated with ease. In the final session, Natalie further estimated that her value-guided approach behaviors dominated her actions compared with behaviors under aversive control. By all accounts, Natalie responded well and in a theoretically expected manner.
8 Complicating Factors
Complicating factors in the present case included the COVID-19 pandemic, Natalie’s change in environment during therapy, and medication usage. The evolution of the COVID-19 pandemic coincided with large-scale fluctuations in physical and mental health, which complicated causal attribution of the outcomes described here. For instance, Natalie’s university implemented restrictions because of the community spread of COVID-19. This change in environmental circumstances limited Natalie’s range of functioning and coincided with a spike in anxiety and depressive symptoms. Such occurrences can be grist for therapy and, as described earlier, provide opportunities for flexible application of therapeutic interventions. Natalie’s change in environment over the course of therapy was useful in terms of generalization of therapy skills, but it also complicated assessment of progress using teletherapy. Though therapy continued uninterrupted, changes in Natalie’s environment likely influenced her behavior and well-being, thus complicating attribution of therapeutic change to the therapy alone.
Natalie’s medication usage while in therapy also complicates causal attribution of therapeutic change. Natalie reported beginning antidepressant medication prior to intake and did not report changing dosages during therapy. The precise timelines of when Natalie began medication in relation to beginning therapy was unfortunately unclear. It is possible that Natalie’s early and positive engagement with therapy was more accessible to her because her symptoms were managed, in part, by her medication. She noted her sleep and appetite improved because of medication alone, before beginning therapy. Yet, she was still highly anxious and stressed at the outset and for a good portion of therapy. This does not discount the benefits of either therapy or medication but highlights their potential synergistic effects. While an ACT conceptualization indicates that symptom reduction is not a necessary precursor for therapeutic success and life change, medication might have functioned to increase Natalie’s willingness to assume an accepting stance toward her internal experiences because they were somewhat reduced by medication and therefore felt less threatening or daunting. In any case, the unclear contribution of medication to the observed intervention outcomes is a limitation, albeit a common occurrence in outpatient mental health settings.
9 Access and Barriers to Care
Natalie owned a laptop and had access to private WIFI in her home, and password protected university WIFI while on campus. This enabled easy and secure access to teletherapy. Ethical issues and potential barriers most relevant to this case included therapeutic privacy when delivering telehealth and balancing COVID-19 exposure risk with in-vivo public behaviors. The therapist discussed benefits and risks of teletherapy with the client at length to ensure informed consent (see Guideline 2 for the practice of telepsychology; APA, 2013). Throughout therapy, discussion included Natalie’s privacy in remote environments. This included brief role-plays of conversations the client could have with her roommate about her need for privacy during the hour without disclosing that she was in therapy, use of headphones for sessions, and seeking out private locations around her dormitory she could go for virtual sessions. At each session, Natalie was asked to confirm physical location for emergency management purposes if needed, to confirm the privacy of her environment, and consent to continuing treatment for that day. The benefits of maintaining contact outweighed the potential privacy risks in the virtual therapeutic environment. This approach aligned with balancing best practices and reasonable flexibility given the extreme extenuating circumstances of the pandemic.
An additional ethical consideration revolved around balancing the client’s goal of increased behavioral engagement with her university policy and public health guidance to mitigate risk of COVID-19 exposure. The therapist did not want to collude with Natalie’s excessive avoidance resulting from health anxiety, but also aimed to carefully evaluate whether Natalie’s treatment goals and exposures were in alignment with CDC guidelines and her university’s policies. Furthermore, Natalie emphasized the desire to engage in more outdoor activities, and these were reinforced throughout treatment. Overall, the therapist and Natalie agreed that sensible, values-guided actions aligning with CDC guidelines were a necessary part of the treatment (e.g., Sheu et al., 2020).
10 Follow-up
Follow up was not conducted per clinic policies and procedures.
11 Treatment Implications of the Case
The present case adds evidence to a small body of literature demonstrating ACT’s effectiveness when delivered over teletherapy and in the context of the COVID-19 pandemic (e.g., Rhodes et al., 2020; Smith, Coe, & Meyer, 2021Smith et al., 2021). Though the pandemic is no longer in an acute crisis phase, other public health crises are unfortunately inevitable. Therefore, this case provides an example of treatment process through such a public health crisis and highlights the utility of a transdiagnostic and flexible approach. Specifically, this case aligns with the conceptualization of heterogeneous anxiety and mood symptomology as responding well to a process-based treatment delivered virtually. Namely, the theoretically consistent outcomes, which targeted transdiagnostic processes rather than symptoms, also aligned with the conceptualization of Acceptance and Commitment Therapy as a unified approach to behavior change (e.g., Hayes, 2019; Hayes et al., 2012) and with empirical evidence demonstrating psychological inflexibility underlies various mental health concerns (e.g., Levin et al., 2014).
This case further exemplifies ACT’s efficacy when assimilating techniques commonly attributed to Motivational Interviewing. Natalie’s increase in behavioral engagement and subsequent decrease in symptoms and inflexibility followed the introduction of MI-like techniques. This suggests that MI techniques may have facilitated good outcomes within an ACT intervention context in this case. This understanding aligns with theoretical comparisons of ACT and MI (outlined in Bricker & Tollison, 2011) as well as clinical case evidence of their assimilative potential (e.g., Ehman & Gross, 2019). Likewise, the flexibility of the ACT model was further evidenced in the present case by the limited use of metaphor (commonly associated with ACT), suggesting that ACT can be applied in different ways yet align with a functional contextual approach targeting the same core processes.
The case detailed here also incorporated a relatively new, multidimensional measure of psychological inflexibility processes (i.e., MPFI-24; Rolffs et al., 2018) which enabled a very fine-grained examination of the six theorized ACT processes of change across the course of therapy and helped to prioritize specific process targets for intervention. The benefits described here of repeated assessment demonstrated the utility of this type of measurement-based care (Scott & Lewis, 2015) and in a process-based therapy context.
12 Recommendations to Clinicians and Students
The present case yields multiple recommendations for clinicians and students. First, teletherapy poses unique benefits and challenges for the provision of psychological services. In an ideal world, the client would always have access to a private space free of distractions. Such luxuries are often not possible, crisis or not. If determined that the benefits of teletherapy outweigh the risks, the therapist is encouraged to model flexibility with teletherapy-specific intrusions. This functioned in the present case to align the therapist with the client, demonstrate shared dilemmas, and model flexibility in the face of challenges. The therapist can also take steps to ensure that their teletherapy setup maximizes connectedness by approximating eye contact with camera positioning (see Grondin et al., 2020). Beyond teletherapy, the present case points toward recommendations for the treatment of anxiety and mood comorbidities from an ACT framework.
This case describes how ACT worked to address a complex anxiety and mood comorbidity, which generally became more severe during the height of the COVID-19 pandemic (e.g., Cordaro et al., 2021). Getting client buy-in early in treatment (e.g., through use of the ACT Matrix) may contribute to good outcomes, particularly in crisis contexts where increased health anxiety is normative, and the range of activities is often restricted to prevent disease spread. Along those lines, the present case highlights the use of exposure and behavioral engagement amid the pandemic with reasonable precautions and in alignment with public health guidance.
This case also demonstrates the utility of repeated assessment of transdiagnostic processes. If done consistently and with theoretically and psychometrically sound measures, self-report measures given at the beginning of sessions can guide therapist intervention focus for that session to maximize intervention efficiency and precision. Consistent with Scott and Lewis (2015), we recommend widespread adoption of measurement-based, evidence-guided care (Boswell et al., 2023). Utilizing the MPFI-24 is an excellent tool from which to begin incorporating process-level data into clinical decision making within an ACT context.
Lastly, MI techniques can be assimilated into ACT even in later stages of treatment depending on their functional purpose in therapy. Clinicians and students interested in incorporating MI with ACT are encouraged to develop competency with both approaches alone, and to consult literature (e.g., Bricker & Tollison, 2011) which details their integration. ACT is a flexible therapy and emphasizes “doing what works.” If the techniques incorporated into ACT are used in alignment with ACT’s underlying philosophical framework, drawing techniques from other therapy systems to move the needle with a stuck client seems entirely appropriate.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.