
Abstract
Practical functional assessment and skill-based treatment (PFA/SBT) is increasingly recognized as a safe and efficient behavioral assessment and treatment approach for severe challenging behaviors commonly exhibited by children with autism spectrum disorder (ASD). Few studies, however, have evaluated the safety, efficiency and acceptability of implementing PFA/SBT procedures by coaching caregivers via telehealth, particularly for caregivers with no prior experience and training. In this pilot single-case investigation, the mother and father of a 6-year-old autistic girl who exhibited severe challenging behaviors were individually coached in weekly one-hour sessions via telehealth to implement PFA/SBT procedures with their child over 12 weeks in their home. The child’s father was subsequently coached to implement a treatment extension with the child in weekly one-hour telehealth sessions conducted over an additional 12-week period. Neither parent had prior training or experience implementing behavioral interventions with their child. Results showed that both parents implemented the intervention with high fidelity and that dangerous forms of challenging behavior rarely occurred during the treatment period. Both parents rated the intervention as highly acceptable. These results demonstrate that parents with limited knowledge and experience of behavioral principles can be successfully coached to implement PFA/SBT procedures via telehealth safely, efficiently, and with high fidelity.
Theoretical and Research Basis for Treatment
A significant proportion of children with autism spectrum disorder (ASD) exhibit challenging behaviors such as aggression, self-injury, and/or property destruction that can result in exclusion from educational and social opportunities, as well as increase the risk of trauma and significant social stigma (Hodgetts et al., 2013; Rajaraman, Austin, et al., 2022; Stack & Lucyshyn, 2019; Swaab et al., 2023). Given the impact of these behaviors on family functioning, there is a clear and critical rationale to evaluate targeted behavioral interventions for children with ASD that are grounded in behavioral principles (Roane et al., 2016). Over the past four decades, researchers have demonstrated that behavioral treatments based on the functions of challenging behavior identified in a pre-treatment functional analysis can result in significantly improved outcomes (Saini et al., 2020). During the functional analysis, the individual is systematically exposed to antecedent and consequent events (e.g., escape from demands, access to preferred items) that typically evoke and maintain levels of dangerous challenging behavior (Iwata et al., 1994).
Once the function(s) of the behavior has been identified, studies have shown that teaching the child to emit functionally equivalent alternative responses that serves the same function(s) as the challenging behavior can result in positive outcomes (Carr & Durand, 1985; Ghaemmaghami et al., 2021; Wacker et al., 2013). For example, if the function of the child’s challenging behavior is to escape from difficult tasks, teaching the child to say “break, please” while simultaneously placing the challenging behavior on extinction, can result in increased levels of communicative behavior and decreased levels of challenging behavior. Although these assessment and treatment studies have resulted in successful outcomes, questions remain concerning the ethical ramifications of the standard assessment and treatment process, given that in many cases, the child may display levels of behaviors that are dangerous or unsafe to both the child and their family members (Fiani & Jessel, 2022; Jessel et al., 2022).
To limit the potential for dangerous forms of challenging behavior to occur during the assessment and initial treatment process, over the past decade, there has been a shift toward prioritizing client assent and safety, leading to significant advances in traditional assessment and treatment procedures for challenging behaviors (Layman et al., 2023). The practical functional assessment and skill-based treatment (PFA/SBT) approach, originally developed by Hanley and colleagues (2014), is an assessment and function-based treatment approach that has gained recognition in the behavior analytic literature as a safe and efficient method for reducing severe challenging behaviors across a variety of contexts, populations, and response classes (Coffey et al., 2019; Layman et al., 2023). The PFA consists of an open-ended functional assessment interview (Hanley et al., 2014) and a functional analysis known as an interview-informed synthesized contingency analysis (IISCA) (Ghaemmaghami et al., 2015; Jessel et al., 2016) to identify the function(s) of the child’s challenging behavior. During the interview, information is obtained concerning the forms of challenging behavior that typically occur, behavioral precursors or indicators that reliably precede the child’s challenging behaviors, specific situations that tend to trigger the child’s challenging behavior, and putative reinforcers or specific types of consequences that may follow the child’s challenging behaviors. The interview is also employed to identify items and activities that are reinforcing for the child.
An IISCA is then conducted to verify the underlying functions of the child’s challenging behavior. Specifically, the IISCA is designed to test the effect of synthesized reinforcement contingencies on levels of dangerous and non-dangerous problem behaviors that typically occur in the natural environment. During an IISCA, the child is exposed to two experimental conditions administered in an alternating treatments design (Rajaraman, Hanley, et al., 2022; Slaton et al., 2017). In the Test condition, an establishing operation (EO) is presented that reliably evokes the child’s challenging behavior (e.g., removal of reinforcing activities and preferred items such as an iPad or parental attention) and if challenging behavior occurs, the child is immediately provided with access to all reinforcers (e.g., preferred items such as an iPad or parental attention). During the Control condition, the child is given continuous and free access to multiple reinforcing items and activities identified in the interview. Each condition is typically conducted for 5 mins and alternated until there is differentiation between the conditions. Throughout the assessment, the focus is on providing synthesized consequences for non-dangerous forms of challenging behavior, rather than presenting consequences for dangerous forms of challenging behavior in isolation, toward the goal of simulating real-life situations that typically occur in the child’s natural environment. This assessment has been reported to take less than an hour to complete, thus decreasing the potential for severe forms of challenging behavior to occur during the assessment (Jessel et al., 2022).
Although the standard IISCA has been deemed a safer and more efficient alternative to the traditional functional analysis, researchers have continued to refine the procedures to further enhance safety and efficiency (Saini et al., 2020). More recently, some clinicians have adopted a shorter and even more efficient “performance-based” IISCA that may be safer for parents to implement with their child, thereby increasing ecological validity (Metras & Jessel, 2021). During a performance-based IISCA, the child is exposed to the EO only after a period of time in which the child appears to be happy, relaxed, and engaged (HRE) and no challenging behaviors have occurred. When the EO is presented, any non-dangerous or dangerous behaviors immediately result in restoration of the items, and the interventionists wait for another period of HRE before the EO is presented again. In this way, the test and control conditions are alternated more rapidly in a trial-based format. In a study evaluating the utility of the performance-based IISCA, Canniello et al. (2023) reported that the performance-based IISCA could be completed in under 20 minutes on average and noted a potential reduction in the risk for individuals to engage in severe and dangerous behaviors during the assessment. The results of this research are encouraging as they demonstrate the potential for enhancing safety measures and facilitating quicker initiation of treatment protocols.
Once the performance-based IISCA has been completed, the results of the assessment can be used to develop the SBT protocol. This treatment package includes teaching the child alternative and socially meaningful functionally equivalent responses based on the function(s) of challenging behavior identified in the IISCA. For example, SBT typically involves teaching a sequence of adaptive responses, including a simple functional communication response (sFCR) (e.g., “my way”), a complex functional communication response (cFCR) (e.g., “my way, please”), a tolerance response (TR) (e.g., “Okay” or thumbs up), and then progressively introducing more complex tasks that have ecological validity to the child and family members (Jessel et al., 2018; Rajaraman et al., 2021). These contextually appropriate behaviors (CABs) may include relinquishing reinforcement, transitioning to a previously non-preferred activity, and completing an activity or multiple activities. The safety, feasibility, and acceptability of the PFA and SBT procedures have been demonstrated in diverse settings such as schools, clinics, and homes (Cervi et al., 2024).
One consideration for increasing access to specialized assessment and treatment of severe challenging behavior is a shortage of providers trained in PFA and SBT protocols, which may place a heavy burden on families to locate specialized care. Telehealth allows for the remote implementation of assessment and treatment procedures for challenging behaviors, such as self-injury and aggression, commonly exhibited by children with autism when in-person services are not feasible (Lindgren et al., 2016, 2020; Monlux et al., 2019; Wacker et al., 2013). A commonly utilized model involves remotely coaching caregivers to implement the therapy directly with their child in their own home. This eliminates the need for family and provider travel, reduces disruption in the family home, and addresses provider shortages (Lerman et al., 2020). However, limited research has examined whether PFA/SBT procedures can be implemented effectively by coaching caregivers to implement the procedures with their child via telehealth (Edelstein et al., 2021; Metras et al., 2023; Rajaraman et al., 2024).
In a study conducted by Metras et al. (2023), for example, mothers of three children diagnosed with ASD, aged 5, 7, and 9 years, were coached to implement PFA/SBT procedures with their child in their home via telehealth during one-hour visits, which occurred three to five times per week over three to four months. Two of the caregivers had prior experience with behavior analytic service implementation and one caregiver had no experience with ABA. Prior to delivering the intervention, each parent watched a 4-h instructional video detailing the procedures that would be implemented. Each caregiver received coaching from a Board Certified Behavior Analyst (BCBA®) to implement a standard IISCA and SBT package with their child. All three children demonstrated a reduction in challenging behavior to zero or near zero levels, and all acquired targeted skills of communication responses and contextually appropriate behaviors.
In another study involving telehealth-enabled implementation of IISCA and SBT procedures, Rajaraman et al. (2024) coached the mother of an adolescent who displayed severe challenging behaviors to implement standard IISCA and SBT procedures with her child in one-hour visits that were conducted via synchronous video conferencing conducted two to three days per week. Although the mother of the child held a Board Certified Assistant Behavior Analyst (BCaBA®) credential, she needed help to implement the procedures correctly with her son. These authors showed that the child acquired functional communication skills and was able to cooperate with over 40 discrete tasks, in the absence of any challenging or precursor behaviors. The studies by Metras et al. (2023) and Rajaraman et al. (2024) demonstrate that coaching parents to implement PFA/SBT procedures via telehealth in their home can effectively decrease challenging behavior while developing functional skills to levels that are meaningful to individuals and families. However, further research is needed to determine whether parents with no prior experience can be successfully coached to implement these procedures via telehealth. Additionally, both studies by Metras et al. (2023) and Rajaraman et al. (2024) trained a single parent to implement the procedures with their child and it is therefore unclear whether other caregivers involved in the child’s care were also implementing the procedures. To date, no studies have evaluated whether coaching both parents of the child to implement PFA/SBT procedures in their home can result in efficient, safe and acceptable outcomes, particularly for those with no prior training or experience.
In this pilot single-case demonstration, we evaluated whether the child’s mother and father who had no prior experience or training in PFA/SBT procedures could be coached via telehealth to implement the procedures safely and efficiently with their child. The aims of the study were 1) to examine the extent to which PFA/SBT procedures could be implemented efficiently via telehealth while minimizing the risk for severe or dangerous challenging behavior 2) the degree to which the procedures could be implemented with fidelity across caregivers, and 3) the acceptability of these procedures reported by each parent. The study was designed to provide pilot data for a randomized controlled trial of PFA/SBT for severe challenging behaviors in children with ASD via telehealth. All study procedures were approved by the Stanford IRB and conformed to recognized standards by the US Federal Policy for the Protection of Human Subjects. Both parents gave their informed consent prior to their inclusion in the study.
Case Introduction
Mila was a 6-year-old female diagnosed with autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder (ADHD) who was referred to a university-based clinic to address her severe challenging behavior, including aggression, and self-injurious behavior. Mila was reported to have limited expressive language skills and would often talk to herself and employ scripts from movies such as Disney’s Moana. Mila was able to say approximately 20 functional words, however, her vocal speech was reported to be generally echolalic although she could sometimes use 3-word sentences for example, “I want juice,” “I want swimming.” Mila liked to play by herself with figurines of Disney characters and would set them up in certain ways, build a fort by herself and engage in imaginative play with stuffed animals. She would sometimes engage in parallel play with her older sister, however, she generally preferred to be on her own and didn’t want to play with other children and liked to hide in small tight spaces. Mila’s father, a 41-year-old Caucasian male, held a Bachelor’s degree, worked 35-h per week and owned his own business. Mila’s mother, a 39-year-old Caucasian female, held an Associate’s degree and worked 40 hours per week outside the home. Neither of Mila’s parents had any prior experience implementing behavior analytic procedures with their child. Mila lived approximately 190 miles away from the nearest treatment center with expertise in challenging behavior for children with ASD with limited availability of providers in her local area.
Presenting Complaints
During initial interviews conducted with Mila’s parents, Mila was reported to engage in several forms of challenging behavior including aggression, self-injurious behavior, property destruction, and excessive climbing behaviors. Mila’s aggressive behaviors were reported to take the form of pulling her mother’s hair and scratching her father on the neck and back. Mila’s mother stated that she would typically react by grabbing Mila’s arm and attempting to release her fingers while saying “Let go, let go. That’s not nice.” Mila was reported to primarily target her mother but would also sometimes pull her sister’s hair. These behaviors typically occurred when Mila was denied something she wanted such as a favorite toy, food item, or to move to a preferred location. Mila’s self-injurious behavior was reported to take the form of biting her lip or arm and pulling her own hair. She was reported to pick at her lip and bite her arm when she couldn’t get her own way. Parents reported trying various chewing necklaces but Mila would often break them, and would not not wear them consistently. Mila would also sometimes chew her hair so parents would often tie her hair back. Mila would often put things in her mouth - toys, dirt, sand, and rocks – and parents would try to discourage this by saying “no mouth” and she would generally spit the item out into their hand. It was unclear whether Mila might be swallowing these items. Mila’s excessive climbing behaviors were reported to occur almost continuously throughout the day. Mila would climb onto surfaces (tables, couches) or climb up trees and then jump off without regard to her safety. It was reported that Mila had broken her arm when she was 4 years old after falling from a window seat onto a tiled floor. She was also reported to have tripped and hit her head against a metal pole. Mila was reported to constantly climb onto the vanity in the bathroom and kitchen counters in the kitchen and parents reported that they will typically say “get down” and Mila would stop for a brief period. Mila was reported to climb onto something very quickly and therefore needed to be watched continuously. It was reported that Mila’s constant climbing was emotionally and physically draining. On the Behavior Problems Inventory-Short Form (Rojahn et al., 2012), Mila’s behaviors were reported to occur on a daily basis and to be severe (i.e., minor or major medical intervention was often required).
History
Mila was diagnosed with ASD and a speech delay when she was three years old. She subsequently received 20 hours per week of home-based applied behavior analysis (ABA) therapy implemented by behavior technicians four days per week. The supervising clinician would come out to the house once per month. Both parents had full-time jobs during this time and hired a babysitter during therapy hours. Mila’s parents reported that behavior technicians failed to build rapport with Mila, there was high staff turnover, behavior technicians did not have adequate training with challenging behavior, and Mila did not make progress towards independent responding. Given lack of progress and the onset of the COVID pandemic, parents decided not to continue with ABA after Mila had received ABA for only one year. Prior to enrollment in the study, Mila attended kindergarten at her local elementary school, however, due to behavioral challenges at school and lack of academic progress, Mila’s parents had taken her out of school and opted to provide home instruction. Mila received an ADHD diagnosis when she was five years old. At the time of her participation in the study, Mila received 60 minutes per week of speech and language pathology treatment, 60 minutes of occupational therapy, and one hour per month of parent consultation from a Doctoral-level Board Certified Behavior Analyst ® (BCBA-D®) at the university-based clinic. Genetic testing revealed that Mila was negative for fragile X syndrome (29 CGG repeats on the FMR1 gene). Trio exome sequencing conducted at the time of the study was uninformative. Further testing indicated that Mila was negative for DDX3X syndrome.
Assessment
Mila’s parents completed the Vineland Adaptive Behavior Scales, Third Edition (Vineland-3) (Sparrow et al., 2018), and Mila received an overall Adaptive Behavior Composite standard score of 56. This score indicated that her overall level of adaptive behavior skills was approximately 3 standard deviations below the mean. She obtained a standard score of 42 on the Communication Skills domain, a score of 59 on the Daily Living Skills domain, a score of 52 on the Socialization Skills domain and a score of 73 on the Motor Skills domain. These data show that Mila exhibited a relative weakness in communication skills and a relative strength in motor skills.
The PFA was conducted with each parent one week prior to the start of treatment. The interview was conducted by the BCBA-D® who also provided the parent coaching. Additional questions were included to determine an appropriate therapeutic space, the placement of cameras for video recording sessions, and information about typical parent-child interactions. The interview lasted approximately 2 hours with Mila’s father and 90 minutes with Mila’s mother.
After the interview, the clinician conducted a 10-min observation as described by Jessel (2022). This brief observation served to probe Mila’s responses to environmental events and contingencies, helped to better define the topography of dangerous and non-dangerous behaviors, and provided the opportunity for caregiver input on relevant contexts in which challenging behavior was most likely to occur. Additionally, the clinician observed Mila’s verbal and imitation skills, her responses to physical touch, the environmental arrangement of the home space, and possible safety factors. Information from the interviews and observations were then used to develop safe conditions for the performance-based IISCA.
The performance-based IISCA was designed to demonstrate that Mila’s dangerous and non-dangerous behaviors were subject to functional control of the identified reinforcers, similar to procedures outlined by (Jessel et al., 2024). At the beginning of each performance-based IISCA, Mila had access to preferred items and activities in her living room including the TV being on, an iPad, a physioball and trampoline, and several other toys in the control condition. After an initial 4 minutes of synthesized reinforcement, the parent was coached to begin the test condition by presenting an establishing operation (EO) (i.e., standing up, clapping their hands, moving closer to Mila, and saying, “iPad all done”). If Mila displayed any dangerous or non-dangerous topographies of challenging behavior, the parent was coached to immediately say, “You can have your way,” and to move away from Mila and sit down to allow Mila to resume access to synthesized reinforcement. The clinician instructed the parent to present the test EO again only after Mila demonstrated 30 seconds of HRE. For Mila, HRE meant a period of time when she was not only free of challenging behavior but using her favorite toys and activities that could include engagement with a parent. This trial-based procedure was repeated a total of four times with each parent.
Measurement and Interobserver Agreement
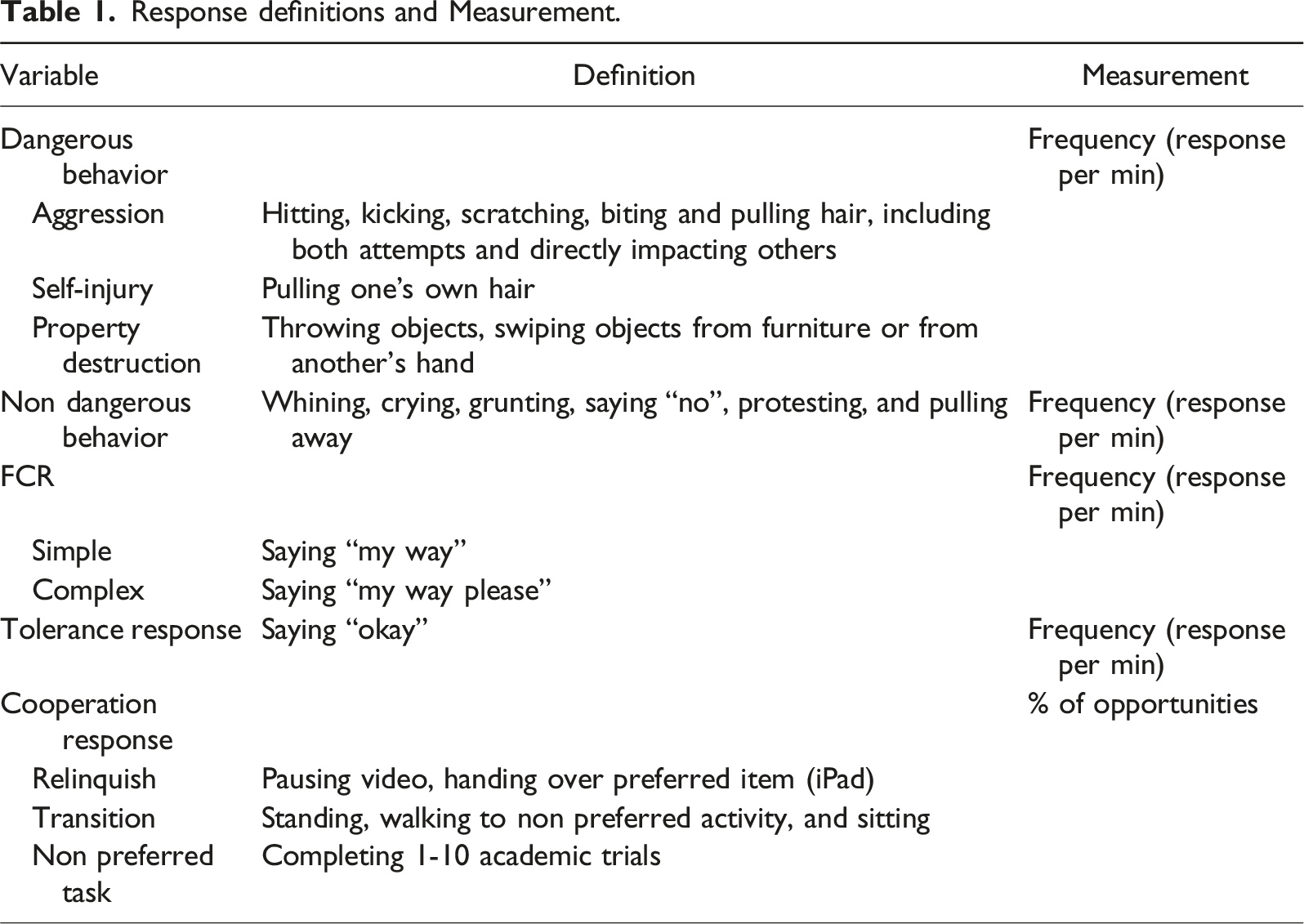
The clinician used the IISCA+ app (Garage94, 2023) to collect child behavior data synchronously via telehealth during the performance-based IISCA as outlined by Canniello et al. (2023). Child behavior data and parent performance data were later reviewed asynchronously. The following dangerous topographies of challenging behavior were recorded: biting, hitting, kicking, pulling out other’s hair, scratching and destroying things. Non-dangerous topographies of challenging behavior that often predicted more severe challenging behaviors were also recorded and included pulling away, whining, grunting, protesting, and saying “no.” Table 1 shows the response definitions and measurement.
Case Conceptualization
The performance-based IISCA was conducted with Mila’s father during the first visit, and then with Mila’s mother during a separate visit conducted two days later within the same week (see Figure 1). During the IISCA conducted by her father (top panel), Mila engaged in both dangerous and non-dangerous challenging behaviors upon interruption of preferred activities and removal of preferred items (i.e., approaching Mila and saying “iPad all done”). However, Mila did not engage in further challenging behaviors when synthesized reinforcement (SR) was presented contingent on problem behavior (i.e., Mila’s father said, “You can have your way” and allowed Mila to resume engaging in preferred activities). During the IISCA by her mother (bottom panel), Mila engaged in dangerous topographies of challenging behavior (e.g., kicking and hair pulling) upon interruption of preferred activities but displayed no further challenging behavior following the presentation of synthesized reinforcement. In the final presentations of the test condition, Mila engaged in non-dangerous challenging behaviors only (whining and grunting) upon presentation of the EO. Taken together, these data suggest that Mila engaged in challenging behavior primarily to retain contact with preferred items/activities. Results of the performance-based IISCA conducted with Mila’s father and her mother conducted in separate visits.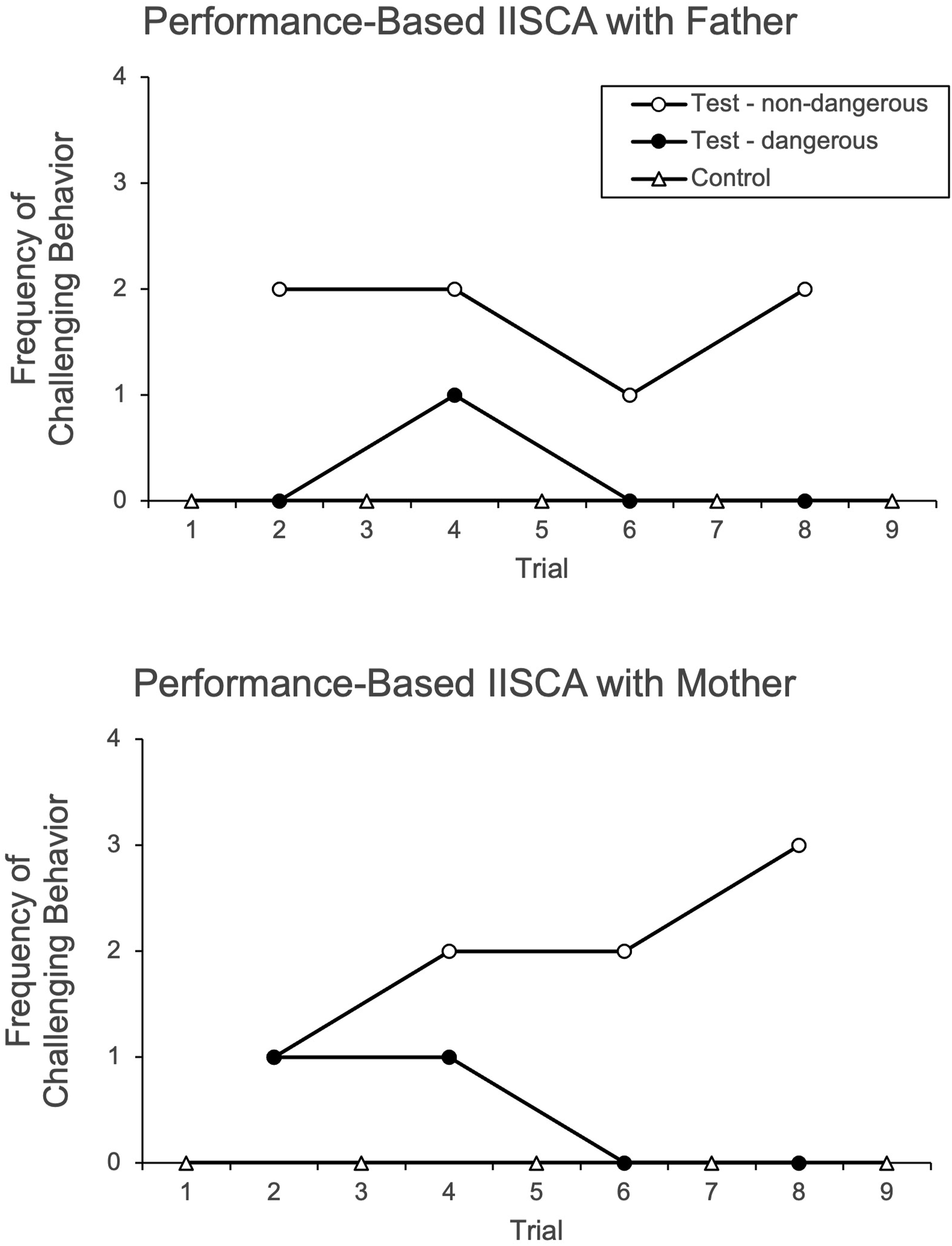
The results of the performance-based IISCA suggested Mila’s challenging behavior was socially maintained and a synthesized reinforcement contingency could be used to develop an intervention for Mila. Following the review of the functional assessment results with the caregiver and with caregiver input, the research team designed Mila’s SBT protocol to use the evocative events from the IISCA and target teaching alternative communication and cooperation responses. As part of a focused intervention, each caregiver met separately with the doctoral-level BCBA clinician and received individual coaching in one-hour weekly sessions via telehealth to implement SBT procedures with Mila over 12 weeks.
Each one-hour telehealth visit began with an initial check-in with the parent followed by behavioral skills training (BST; Lloveras et al., 2022) with the parent. Once the parent demonstrated procedural fidelity during role play and expressed readiness to proceed, the parent implemented treatment with Mila. Sessions consisted of five-trial blocks and one to five blocks were completed in each visit. If dangerous or non-dangerous challenging behavior occurred on a trial, the parent was coached to either prompt the correct response or wait until challenging behavior subsided and modify the environment and represent the instructional prompt (i.e., saying “all done” and prompting the target response). If Mila demonstrated three correct independent responses with no challenging behavior in a five-trial block, training was moved to the next phase. Sessions were terminated if Mila engaged in dangerous topographies of challenging behaviors on three trials within a five-trial block, if she left the room, or if she did not achieve HRE after a trial. Sessions were resumed once Mila showed indications of being HRE for a minimum of 4 minutes.
At the end of each visit, the parent had the opportunity to discuss any concerns and review skills. The clinician then provided the parent with a practice log adapted from Ruppel et al. (2021) and instructed the parent to practice the skills they had learned with Mila to encourage future independent practice. During the next visit, the clinician asked each parent if they had practiced and helped each parent troubleshoot any difficulties they had encountered. While the frequency of homework practice was not recorded, in general, each parent self-reported practicing 1-2 times between consult sessions.
All treatment sessions took place in the family’s home. Parents identified the open concept living space (living room, dining, and kitchen area) as the location for Mila’s preferred items and activities including movies on the television, iPad, and trampoline. Favorite snacks were available throughout each session. Sessions were conducted individually via synchronous videoconferencing using a 9th generation Apple iPad that was provided to the family with Center Stage and the Zoom platform installed. To communicate with the therapist during sessions, Mila’s father used his own bluetooth earbuds, and Mila’s mother preferred to use the text function on her Apple watch. The clinician used an Apple laptop with built-in webcam and microphone. All performance-based IISCA and SBT sessions were video-recorded and saved automatically in Zoom.
Course of Treatment and Assessment of Progress
A multiple baseline across skills design was used to evaluate the effects of the SBT intervention. Mila was first taught to emit a simple functional communication response (sFCR) (i.e., “my way”). On initial sFCR training trials, the parent was coached to present the EO in a progressing sequence (e.g., standing up, clapping their hands, approaching Mila, and saying “time to turn off your iPad”) and then immediately prompted Mila to point to a 4 inch × 4 inch picture card containing the words “my way” using most-to-least prompting. Within one visit, however, it quickly became clear that Mila could vocally say the words “my way,” and trials were adjusted for parents to use most to least verbal prompts for a vocal “my way” response. When Mila said “my way” either independently or with prompting, the parent was coached to immediately say “Ok, you can have your way” and provide access to reinforcement. If Mila displayed dangerous or non-dangerous challenging behavior during a trial, the parent was instructed to remain neutral and prompt Mila to say “my way” instead. After a session during early sFCR training when Mila engaged in moderate rates of both dangerous and non-dangerous behaviors, the session structure was modified to increase the quality of parent attention. These modifications included: 1) the clinician provided feedback only after the 5-trial block, and 2) instructing the parent to stay close to Mila.
Once Mila was emitting the sFCR reliably on each trial, training progressed to a complex functional communication response (cFCR) (i.e., “my way, please”). On each cFCR training trial, the parent was coached to present the EO in a progressing sequence (e.g., standing up, clapping hands together, approaching and saying “time to turn off your iPad”) and immediately prompting Mila to say the words “my way please.” When Mila said “my way please” either independently or with prompting, the parent was coached to immediately say, “Ok, you can have your way” and to allow her to play with her toys. If Mila said the simple FCR (i.e., “my way”), she was not provided with reinforcement and prompted to use the cFCR instead.
Once Mila was reliably saying the cFCR (i.e., “my way please”), she was taught to accept disappointment by saying “ok” as a tolerance response (TR). During TR training trials, the parent was coached to signal the end of reinforcement by saying “[item/activity] all done.” When Mila said “my way please,” the parent was coached to deny Mila access to reinforcement by saying “no, not right now” and then prompting Mila to say “ok.” If Mila said “ok,” the parent was coached to say, “you can have your way” and Mila received access to reinforcement as usual. During this phase, parents were coached to present a tolerance training trial on three out of every five training trials to minimize the predictability of trial order and maintain Mila’s communication responses. As with teaching FCRs, the clinician only provided feedback between trial blocks to minimize reactivity and increase parent independence.
Once Mila independently emitted the TR without exhibiting challenging behavior and was able to tolerate delays to reinforcement, she was taught progressively more complex contextually appropriate behaviors (CABs). During CAB1 training, Mila was taught to relinquish reinforcement across multiple items and activities, such as giving up her iPad or pausing a movie. Once CAB1 training was mastered, CAB2 training was introduced and consisted of teaching Mila to transition from preferred play to a lesser preferred activity, such as walking to the work table. CAB1 and CAB2 were taught using three-step least-to-most prompting (i.e., “Tell them,” “Show them,” “Help them”), similar to the method outlined by Ruppel et al. (2021). As with the previous stage, CAB session blocks consisted of five randomized trials (60% CAB, 40% cFCR) with clinician feedback provided in between blocks. Once Mila cooperated with instructions, the parent immediately resumed synthesized reinforcement and waited a minimum of 30 s before implementing the next trial block.
Treatment Extension
A treatment extension was conducted for an additional 12 weeks with Mila’s father because Mila’s mother’s work schedule did not permit her participation and Mila’s father had recently committed to teaching Mila on a full-time basis. The treatment extension consisted of completing three branches of academic goals outlined in Mila’s Individualized Education Plan (IEP). These included labeling (i.e., “tacting”) objects and action verbs, discriminating between different objects, and imitating motor actions. At baseline, these behaviors were not observed and were goals in Mila’s IEP. Mila’s father requested conducting treatment in various environments during this phase to replicate naturally occurring contexts, however, data for CABs in novel contexts suggested Mila’s skill acquisition was slower in novel situations. Therefore, sessions were occasionally relocated to previous settings when necessary. During CAB3 chaining, Mila’s father was coached to implement most-to-least prompting for training new skills, and least-to-most prompting for learned skills. Coaching for the majority of CAB2 and CAB3 was implemented either in Mila’s living room or a closed-off room with toys and sensory items.
Response Measurement
In addition to dangerous and non-dangerous forms of challenging behavior, target skills recorded during SBT included the simple functional communication response (sFCR) (i.e., saying “my way”), the complex functional communication response (cFCR) (i.e., saying “my way, please,“) and the tolerance response (TR) (i.e., saying “ok.“). Contextually appropriate behaviors (CABs) consisted of relinquishing reinforcement (e.g., an iPad) or a preferred activity (CAB1), transitioning to a workspace (CAB2), and cooperating with tasks (CAB3) (see Table 1).
During SBT, the clinician collected data in vivo to guide treatment, and asynchronously to collect child behavior, child performance, parent performance and total session time. During the IISCA and SBT, the frequency of dangerous and non-dangerous forms of challenging behaviors and taught responses (FCR, TR, CAB) as prompted or independent were recorded via paper and summarized as rate. Parent fidelity data were collected for each session using the IISCA and SBT teaching integrity worksheets adapted from Metras (2021). Parent fidelity was reported as the number of events correctly implemented divided by the total number of events and multiplied by 100 to obtain the percent correct. The mean fidelity of treatment implementation was 91.49% (range 73.33%–100%) for Mila’s father and 88.77% (range = 60%–100%) for Mila’s mother. Overall, the mean treatment fidelity for both caregivers was 90.53% (range 60–100%) (See bottom panel of Figure 2). Mila’s Treatment Data. Note BL is baseline, FCT is functional communication training, CAB is contextually appropriate behavior. The dashed lines denote phase changes.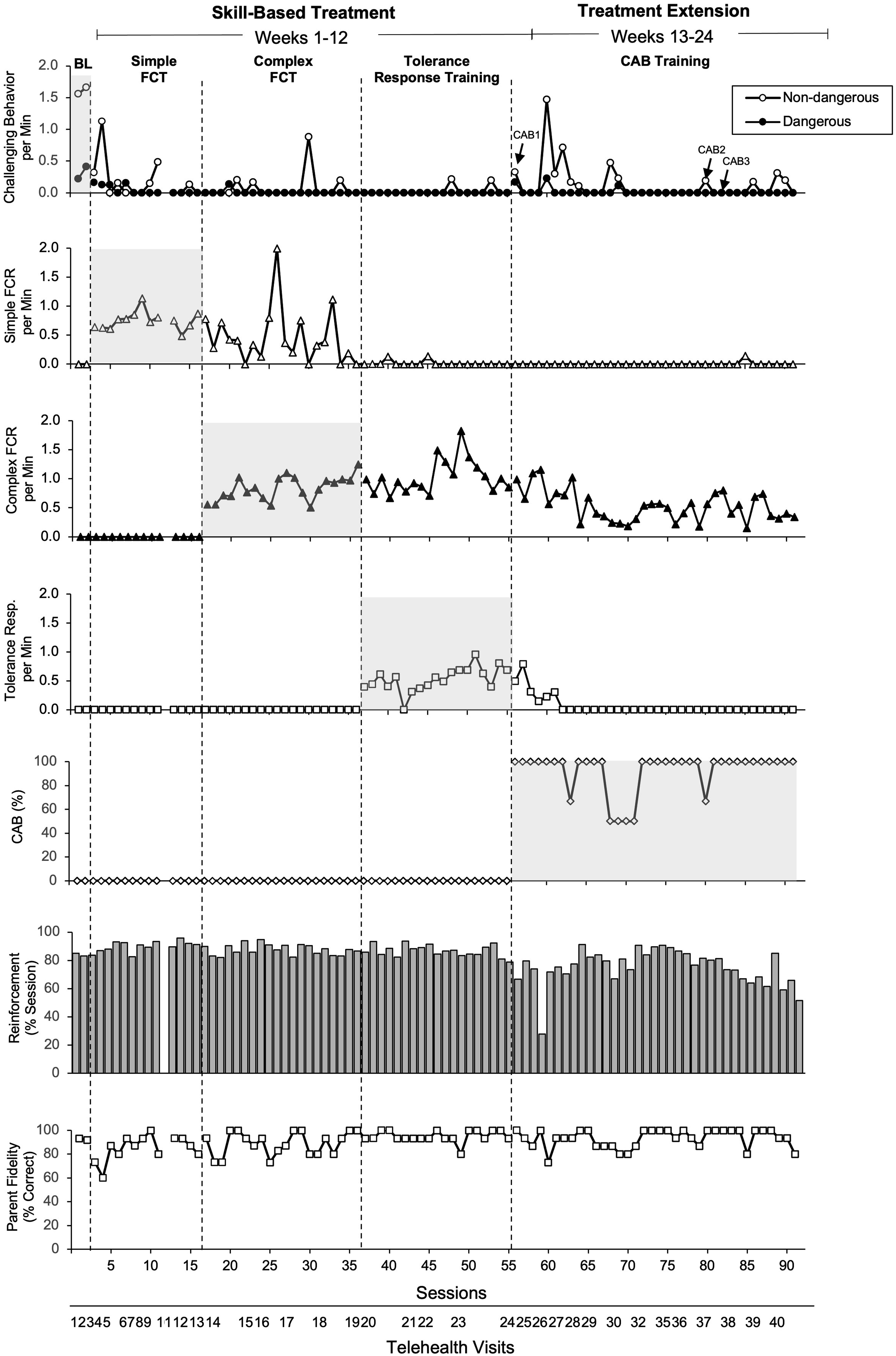
A second observer asynchronously collected data on child performance measures and parent fidelity on 25% of sessions to determine interobserver agreement. For child performance measures, trial-by-trial IOA was calculated by dividing the number of agreements by the number of trials in a session block, then multiplying the quotient by 100. An agreement was scored if both observers scored the same number of behaviors in a trial. For parent fidelity, total count IOA was calculated by dividing the number of agreements by the total number of events in each session block and multiplying by 100. These were averaged across sessions. The mean percentage agreement for dangerous and non-dangerous behaviors for the PFA and SBT sessions were 97.92% and 99.17% (range, 50–100%) respectively. The mean percentage agreement for sFCR, cFCR and TR behaviors were 100%, 80% (range, 40–100%) and 100% respectively. The mean percentage agreement for CABs was 100%. The mean percentage agreement for IOA of parent fidelity of implementation was 97.71% (range, 86%–100%) for Mila’s father and 100% for Mila’s mother.
The results of the treatment are summarized in Figure 2. The top panel shows the rate of dangerous and non-dangerous forms of challenging behavior observed during each session of the IISCA baseline (BL), during 12 weeks of SBT with both parents, and the 12-week treatment extension conducted with Mila’s father only. During the IISCA baseline, the first data point represents the mean rate observed during the IISCA conducted with Mila's father and the second data point represents the mean rate observed during the IISCA conducted with Mila's mother. The mean rate of dangerous forms of problem behavior observed across both parents was .32 r/min whereas the mean rate of non-dangerous forms of problem behavior observed across parents was 1.61 r/min. Both forms of challenging behavior were progressively reduced during subsequent sessions of functional communication training. During sFCR training, the mean rate of non-dangerous forms of challenging behavior was .20 r/min whereas the mean rate of dangerous forms of problem behavior was .09 r/min. During cFCR training, Mila continued to exhibit fewer dangerous (M = .01 r/min) and non-dangerous (M = .07 r/min) behaviors compared to baseline. Mila acquired both simple (“my way”) and complex (“my way, please”) responses with both parents. Similarly, the rate of non-dangerous and dangerous challenging behaviors remained at low levels during TR training although forms of non-dangerous challenging behavior increased when CAB1 training was introduced at the beginning of the 12-week treatment extension. However, as the 12-week treatment extension progressed with her father, Mila’s dangerous and non-dangerous forms of challenging behavior continued to occur at low rates, and Mila was subsequently able to transition to a work table and cooperate with completing tasks (CAB3) at the table without an increase in either dangerous or non-dangerous forms of problem behavior.
Complicating Factors
SBT typically includes teaching a tolerance response (TR) to help the child accept temporary denials of reinforcement and adjust to gradual increases in the evocative condition (Ghaemmaghami, 2016). However, following 12 weeks of treatment, Mila was less consistent with maintaining the tolerance response, and caregivers indicated a preference for focusing on CAB training instead. It is worth noting that in one of the few studies of PFA and SBT implemented by caregivers via telehealth, Metras et al. (2023) reported that two of the three caregiver-child dyads also opted to forgo TR training. Despite the potential advantages of TR training, caregivers may find extending delays naturally with increasingly more complex CABs more relevant. When designing SBT, clinicians should consider factors including the available treatment time, ecological validity, and social validity with parents, when deciding to incorporate a tolerance response. Additionally, encouraging parents to practice outside of treatment may have further promoted skill acquisition of the child and the parents as implementers.
Several precautions were taken to mitigate the challenges in delivering telehealth services. These were based on recommendations by recently published guidelines (CASP, 2021; Lerman et al., 2020). These measures included providing parents with all necessary technology for treatment implementation (e.g., iPad with Zoom installed), evaluating internet connectivity in advance, instructing parents on how to optimize the view of the child, and removing disruptions in the child’s environment. Because Mila’s preferred items were mainly available in the open space of the living room and kitchen, we experienced challenges specific to implementing SBT protocols via telehealth. Even with the placement of the camera from a distance, Mila sometimes wandered off camera, and the clinician was unable to hear Mila’s vocal functional communication responses. This was resolved by moving to another smaller room in the home, which provided Mila with more freedom to move around the room while staying within video boundaries.
We note that we were unable to provide treatment to both parents simultaneously because parents were not available for scheduled sessions at the same time. This provided an added complication because Mila could not be supervised during 1:1 parent coaching and sessions could therefore be disrupted. This was managed by providing frequent breaks to allow the parent to attend to Mila as needed. We mitigated potential misunderstandings between parents by providing the same instructional materials to both parents and measuring parent fidelity data in each session to ensure each parent implemented the procedures with high fidelity.
Access and Barriers to Care
Opting for telehealth coaching rather than in-person coaching has unique advantages for families, making treatment more accessible. Telehealth coaching provides families access to highly qualified practitioners, has lower costs in terms of time and travel expenses, and allows the child to receive treatment when services are not locally available (Lerman et al., 2020). In the case of the present family, traveling to the nearest specialist required a 380-mile round trip and over 7 hours of drive time, significantly increasing the cost and decreasing the feasibility of treatment. While our findings suggested that parent-mediated PFA and SBT via telehealth is a feasible model, our investigation also revealed some limitations and opportunities for improvement, indicating potential avenues for further research. Specifically, these relate to challenges with the tolerance response, technology challenges, and limited generalization of skills outside of treatment sessions.
Response definitions and Measurement.
Follow-Up
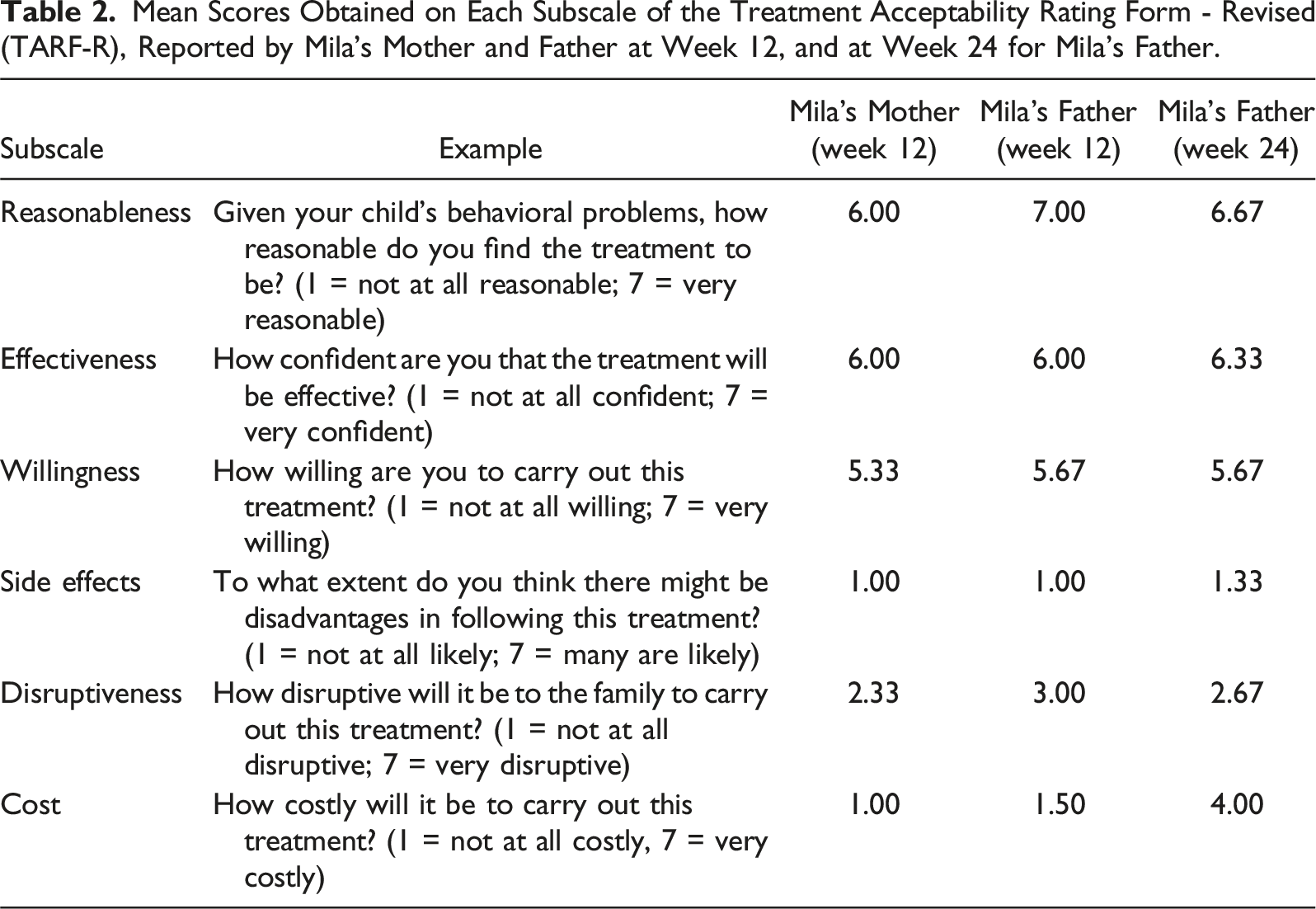
Mean Scores Obtained on Each Subscale of the Treatment Acceptability Rating Form - Revised (TARF-R), Reported by Mila’s Mother and Father at Week 12, and at Week 24 for Mila’s Father.
Treatment Implications of the Case
Our study builds on previous studies investigating the effectiveness of parent-mediated functional analyses and skills training via telehealth in children with ASD (Hall et al., 2020; Lindgren et al., 2020; Metras et al., 2023; Rajaraman et al., 2024; Wacker et al., 2013). Specifically, we evaluated the effectiveness of the performance-based IISCA and SBT when implemented by novice parents via telehealth coaching, focusing on managing challenging behaviors and promoting appropriate replacement behaviors. Notably, this is the first known study where two parents without prior experience with behavioral treatment protocols were coached via telehealth to implement the performance-based IISCA and SBT with their child. Differentiation was successfully achieved during the performance-based IISCA, and safety was maintained by both parents. Previous research has shown that control may be evident within one test session (Jessel et al., 2018). The goal of the performance-based IISCA is to reduce escalation by providing reinforcement at the first indication of problem behavior, typically when the child engages in minor precursor behaviors. We believe that obtaining two baseline data points from two separate IISCAs were representative of the rates of challenging behavior observed across both parents. Mila engaged in a few attempted dangerous behaviors (e.g., kicking and hitting) during the performance-based IISCA with both caregivers, however, these behaviors did not escalate and Mila quickly ceased when synthesized reinforcement was presented. The IISCA was conducted in 8 minutes for Mila’s father and 12 minutes for Mila’s mother. During the IISCA with Mila’s mother, Mila demonstrated a decrease of dangerous behaviors with a shift toward non-dangerous behaviors. During the IISCA with Mila’s father, non-dangerous behaviors remained stable with only one occurrence of dangerous behavior. These results suggest that the performance-based IISCA is a safe and efficient protocol when implemented by caregivers without prior training.
During SBT sessions, Mila consistently exhibited low levels of challenging behavior, with dangerous topographies being minimal, typically surfacing only when new skills or contexts were introduced. Indeed, dangerous topographies of challenging behaviors were minimal across all phases. In instances where challenging behaviors occurred during sessions, potential contributing factors typically included lower parent fidelity of implementation, limited access to reinforcement during programmed synthesized reinforcement periods, increased time spent in the EO condition, and naturally occurring delays or denial of access to reinforcement. Consistent with findings from previous studies examining parent-mediated treatment via telehealth (Lindgren et al., 2020; Wacker et al., 2013), Mila’s challenging behavior decreased by 91.78% (Baseline = 1.46 r/min, 12th Week = .12 r/min). Moreover, within 12 weeks of treatment, Mila acquired functional communication responses, tolerance responses, and engaged in prompted CAB targets.
During the treatment extension with Mila’s father, Mila developed CAB targets and independently demonstrated increasingly complex CAB chaining despite a reduction in treatment time to 1 hour per week working exclusively with her father. By week 24, Mila willingly relinquished multiple types of reinforcement, successfully transitioned across varying distances (e.g. up to 10 feet and to different rooms) and demonstrated the ability to complete three activities, each containing between three to thirty steps, within a single trial. Taken together, these data and observations suggest that the performance-based IISCA and SBT can be implemented safely and efficiently by parents via telehealth, resulting in meaningful behavior change.
Recommendations to Clinicians and Students
Our pilot study informs the feasibility, safety, and acceptability of parent implementation of the performance-based IISCA and SBT for a prospective randomized controlled trial and further contributes to the telehealth coaching literature. With the performance-based IISCA, we successfully reduced assessment time to less than 15 minutes for each caregiver and minimized exposure to harmful behaviors. This not only increased the safety of the procedure within one visit with each parent, but also yielded effective results in identifying the functions of challenging behavior and developing a treatment protocol that significantly reduced problem behavior. To our knowledge, this study is the first to train two parents independently, neither of whom had experience with the protocols, to implement the performance-based IISCA and SBT through a telehealth coaching model. The findings of this study provide evidence that parent-mediated treatment, facilitated by a telehealth coaching model, can effectively and safely address behavioral challenges, representing a significant advancement for families with limited access to in-person services. As the field continues to advance its understanding of PFA and SBT, we encourage further studies on the impact of parent implementation and telehealth modalities in safely treating challenging behavior.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the U.S. Department of Defense; W81XWH-22-1-0321.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.