
Abstract
Anorexia nervosa (AN) is a severe psychiatric disorder with high mortality and frequent relapse in adulthood. Although evidence-based treatments exist, their effectiveness remains limited, and few involve caregivers despite evidence supporting their role. This single-case study explored the feasibility and preliminary effectiveness of the ECHOMANTRA program—a brief, manualized, online intervention based on the cognitive–interpersonal model—as an adjunct to treatment-as-usual (TAU) for an adult woman with AN and her mother. The eight-session intervention included MANTRA-based modules for the patient and ECHO-based modules for the caregiver, supported by manuals and personalized workbooks. Assessments were conducted at pre-treatment, post-treatment, and three-month follow-up using validated self-report measures. Patient outcomes included eating disorder symptoms (EDE-Q), emotional distress (DASS-21), functional impairment (CIA 3.0), and quality of life. Carer outcomes included symptom accommodation (AESED), perceived illness impact (EDSIS), and caregiving skills (CASK). Results showed clinically meaningful reductions in eating disorder symptoms, emotional dysregulation, and functional impairment in the patient, with gains maintained at follow-up. A transient post-treatment increase in emotional distress likely reflected greater illness insight, which subsided by follow-up. The caregiver reported decreased accommodation, lower burden, and improved caregiving competence. Both participants adhered to and were highly satisfied with the intervention. Findings offer preliminary support for ECHOMANTRA as a feasible and potentially effective adjunct to standard care, highlighting the value of integrating caregiver-focused strategies into adult AN treatment.
Theoretical and Research Basis for Treatment
Anorexia nervosa (AN) is a severe psychiatric disorder characterized by persistent restriction of energy intake, intense fear of weight gain, and disturbance in body image, as defined by the DSM-5-TR (American Psychiatric Association [APA], 2022). It is associated with the highest mortality rate among mental health disorders—up to five times higher in women with AN than in the general population (van Eeden et al., 2021). In adulthood, treatment poses specific challenges, including greater resistance to change, heightened cognitive rigidity, and a higher risk of chronicity when the disorder is not addressed adequately or early (Abbate-Daga et al., 2013).
Despite the availability of several evidence-based treatments for adult AN, none has consistently demonstrated superiority in clinical trials. Among the most empirically supported therapies are Enhanced Cognitive Behavioral Therapy (CBT-E), Specialist Supportive Clinical Management (SSCM), and the Maudsley Model of Anorexia Nervosa Treatment for Adults (MANTRA) (Fonseca-Pedrero, 2021; Fonseca-Pedrero et al., 2021). CBT-E focuses on reducing eating disorder symptoms by targeting dysfunctional thoughts, rigid rules about food, and body-related anxiety, using structured behavioral and cognitive techniques (Fairburn et al., 2008). SSCM combines non-directive clinical support with psychoeducation and nutritional advice, and its flexibility often enhances patient engagement (McIntosh et al., 2022). MANTRA, developed specifically for adults with AN, is a manualized therapy that integrates cognitive, emotional, and interpersonal work to address maintaining factors of the disorder (Schmidt et al., 2014).
Meta-analyses and systematic reviews suggest that these three approaches produce comparable outcomes in weight restoration and symptom reduction, with generally modest effect sizes (Fernández-García & Quiles, 2024; Solmi et al., 2021). Given the lack of a clearly superior intervention, the choice of treatment often depends on factors such as patient preference, therapist expertise, and theoretical orientation. However, among these options, MANTRA stands out for its strong theoretical grounding and its comprehensive, individualized focus on emotional and interpersonal difficulties, traits frequently observed in adult AN and associated with poor treatment adherence and outcome (Schmidt & Treasure, 2006).
The MANTRA approach is built on the Cognitive-Interpersonal Maintenance Model, which conceptualizes AN as a disorder maintained by the interaction between premorbid traits (such as anxiety, cognitive inflexibility, and perfectionism), emotional avoidance, pro-anorexic beliefs, and problematic interpersonal functioning. These factors collectively reinforce restrictive behaviors and reduce motivation to recover. MANTRA aims to disrupt these maintaining mechanisms through a motivational, collaborative approach that incorporates reflective tasks, experiential exercises, and emotion-focused interventions. Importantly, the model acknowledges the social and relational context of the illness and emphasizes the potential role of close others in facilitating change (Schmidt et al., 2014).
Unlike many treatments that are solely patient-centered, MANTRA explicitly incorporates the role of carers within its theoretical framework. Increasingly, research has highlighted the importance of involving families and caregivers in the treatment of adult AN. As emphasized by Treasure et al. (2021), carers often experience high emotional burden, distress, and a sense of helplessness in their caregiving role. They may also engage in behaviors that inadvertently accommodate the illness, such as avoiding conflict or facilitating rituals. Such dynamics can maintain the disorder or undermine treatment progress. Including carers in interventions has been shown to reduce caregiver burden, improve coping strategies, and promote more autonomy-supportive communication, which in turn enhances the recovery process of the individual with AN (Quiles et al., 2026).
Building on these principles, Treasure and colleagues developed ECHOMANTRA, a brief, structured program that combines the MANTRA intervention for patients with the ECHO (Experienced Carers Helping Others) model for caregivers (Cardi et al., 2017). While the detailed structure of ECHOMANTRA is described later, it is worth noting here that the program operationalizes the cognitive-interpersonal framework in both individual and interpersonal components, addressing not only the patient’s internal maintaining mechanisms but also the caregiving environment.
Preliminary studies have shown encouraging results regarding the acceptability and potential effectiveness of ECHOMANTRA. For example, Adamson et al. (2019) reported that its implementation in inpatient settings was associated with faster weight gain, shorter hospitalizations, and better symptom maintenance at follow-up. Caregivers also showed reduced levels of expressed emotion and symptom accommodation. Similarly, Ruiz et al. (2024) found improvements in carer emotional well-being, communication patterns, and confidence in managing the disorder. More recently, Ruiz et al. (2026) extended these findings to adolescent populations, demonstrating that ECHOMANTRA not only improved motivation and emotion regulation in young patients but also enhanced treatment adherence and reduced carer distress and accommodation. These findings suggest that integrating carers through structured interventions may be a key factor in optimizing treatment outcomes, particularly in populations where motivation and engagement are often low.
The present study builds on this body of evidence, aiming to explore the feasibility, acceptability, and clinical impact of ECHOMANTRA in an adult outpatient context. By addressing the interpersonal and emotional factors that sustain AN, while simultaneously supporting carers with structured, evidence-based tools, ECHOMANTRA offers a promising adjunct to standard care in adult anorexia nervosa.
Case Introduction
The case concerns A., a 28-year-old Spanish woman diagnosed with AN, restrictive type (AN-R), according to DSM-5-TR criteria (APA, 2022). She was the third of six siblings and lived in a middle-class household with her retired mother and three siblings. A. had completed advanced vocational training in dance and was working as a teacher, occasionally participating in professional stage productions.
At the time of the intervention, she was receiving multidisciplinary care at a specialized day hospital program for eating disorders. This included medical monitoring, psychiatric evaluation, nutritional support, individual psychotherapy, and group interventions. In addition to TAU, she and her mother were enrolled in the ECHOMANTRA program, delivered online in eight parallel sessions.
The case was selected because it illustrates multiple clinical challenges typical of adult AN: a chronic illness course with relapses, entrenched perfectionism, and high levels of carer involvement. This profile provided an opportunity to explore the potential of ECHOMANTRA to enhance treatment outcomes by simultaneously addressing the patient’s intrapersonal maintaining factors and the carer’s burden and caregiving style.
Presenting Complaints
At baseline, the patient exhibited a pattern of severe dietary restriction, frequent nocturnal binge episodes, and occasional purging behaviors. These symptoms were accompanied by rigid food-related rituals, such as meticulous calorie counting and weighing of food, reflecting a high degree of cognitive control around eating. Additionally, she displayed pronounced irritability, progressive social withdrawal, and significant difficulties in identifying and expressing emotions.
She characterized her previous outpatient treatments as insufficient, indicating that despite multiple therapeutic attempts, she continued to struggle with symptom management and emotional regulation. Her referral to a specialized day hospital program was prompted by the worsening of her clinical condition and the limited response to prior interventions.
From the carer’s perspective, her mother reported high levels of emotional distress related to her daughter’s deteriorating health and the increasing tension within the family dynamic. She expressed uncertainty about how to support her daughter effectively and often felt overwhelmed by the demands of the caregiving role, highlighting the need for targeted guidance and emotional support.
History
A.’s eating difficulties began in 2019, at the age of 22, shortly after she completed her vocational dance training and began working professionally. Immersed in a highly competitive environment with rigid aesthetic expectations, she adopted restrictive eating patterns and intensive physical exercise routines. Initially framed as healthy lifestyle habits, these behaviors were socially reinforced and increasingly normalized within her professional context. Over time, however, they became more rigid and compulsive, resulting in significant weight loss, emotional distress, and a growing preoccupation with control over food and body image.
The COVID-19 pandemic, which struck when A. was 23, marked a pivotal escalation in her illness. Confinement at home disrupted her professional activities and social life, increasing her sense of isolation. Unable to engage in her usual dance routines, she intensified food control and began exercising compulsively within the home. These behaviors consumed most of her daily routine and led to emotional withdrawal even within her family circle. The lockdown thus reinforced cognitive rigidity and experiential avoidance, two central maintaining mechanisms of AN.
Following this period, A. engaged in outpatient treatment but reported limited benefit. While she achieved some behavioral improvements, full weight restoration was not reached. According to her account, attempts to gain weight provoked intense discomfort, which often led to relapse into restrictive behaviors. She eventually discontinued treatment, having attained only partial remission.
In 2022, at the age of 25, A. relocated abroad for work. The non-renewal of a dance contract, which she interpreted as a personal failure, triggered a major relapse. This event reactivated restrictive eating patterns, nocturnal binge episodes, and occasional purging behaviors. Her mood became increasingly unstable, and her social withdrawal intensified. These difficulties prompted her family to seek specialized care, leading to her referral to the day hospital program where the present intervention took place.
Developmentally, A. was raised in a large Catholic family affiliated with the Neocatechumenal Way, a context marked by strong religious and moral values, high expectations, and a structured approach to discipline. As the third of six siblings, she often perceived herself as overlooked and subjected to comparison. The family climate emphasized obedience, self-control, and achievement, which shaped her internal standards and contributed to the emergence of perfectionism and low self-worth. Her identity became increasingly tied to performance, both academically and artistically.
The relationship with her mother—her primary caregiver—was particularly influential. At the outset of therapy, her mother displayed a highly directive stance, often instructing A. on what to share in sessions or emphasizing unresolved family issues without allowing space for her daughter’s own pace or emotional readiness. While such involvement reflects cultural norms of close familial interdependence common in Mediterranean societies, it also hindered the development of autonomy and emotional differentiation.
These intersecting personal, familial, and sociocultural influences—ranging from early perfectionistic tendencies and body dissatisfaction to maternal overinvolvement and identity confusion—converged to sustain a chronic illness course. They underscore the complexity of A.’s case and highlight the need for a treatment approach that simultaneously addresses the intrapersonal functions of the disorder and the relational dynamics that perpetuate it.
Assesment
A comprehensive assessment protocol was administered at three time points: pre-treatment (baseline), post-treatment, and three-month follow-up. The battery was designed to evaluate both the patient’s clinical symptomatology and the carer’s emotional functioning and caregiving patterns. All instruments were self-report measures with adequate psychometric properties, validated in Spanish samples.
Patient Assessment Measures
• Ad hoc sociodemographic and clinical questionnaire. Collected basic information on age, educational level, and employment, as well as clinical data including diagnosis, illness duration, treatment history, hospital admissions, current medication, comorbidity, and body mass index (BMI). Data were provided by the clinician at the day-care centre. • Eating Disorder Examination Questionnaire (EDE-Q; Fairburn & Beglin, 1994). A 37-item self-report assessing eating disorder symptomatology across four subscales (Dietary Restraint, Eating Concern, Weight Concern, and Shape Concern). Each item is rated on a 0–6 scale, with higher scores indicating greater symptom severity. Global scores ≥2.5 are generally considered to reflect clinical-level symptoms in adult women. The Spanish version demonstrated good internal consistency (α = .74–.93; Peláez-Fernández et al., 2013). • Depression, Anxiety and Stress Scales (DASS-21; Lovibond & Lovibond, 1995). A 21-item self-report assessing psychological distress across three domains. Each subscale yields a score ranging from 0 to 42 (after multiplying raw scores by 2), with severity bands ranging from normal to extremely severe. For clinical interpretation, cut-offs for moderate severity are: Depression ≥14, Anxiety ≥10, Stress ≥19. The Spanish version showed adequate reliability (α = .70–.84; Bados et al., 2005). • Clinical Impairment Assessment (CIA 3.0; Bohn et al., 2008). A 16-item self-report evaluating psychosocial impairment due to eating disorder symptoms across personal, social, and cognitive domains. Items are rated on a 0–3 scale, with a total score ranging from 0 to 48. Scores ≥16 are typically interpreted as indicating significant functional interference. The Spanish validation showed excellent internal consistency (α = .90; Martín et al., 2015). • Eating Disorders Quality of Life Instrument (EDQoL; Engel et al., 2006). A 25-item disorder-specific measure assessing health-related quality of life across psychological, physical/cognitive, occupational/educational, and financial domains. Items are rated on a 0–4 scale; higher scores indicate poorer quality of life. The Spanish version showed high reliability (α = .91 overall; Quiles et al., 2023). • Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004). A 28-item self-report assessing six domains of emotion dysregulation: non-acceptance, goals, impulse, awareness, strategies, and clarity. Total scores range from 36 to 180, with higher scores reflecting greater difficulties. The Spanish version showed excellent reliability (α = .93; Hervás & Jódar, 2008). • Frost Multidimensional Perfectionism Scale (FMPS; Frost et al., 1990). A 35-item measure assessing concern over mistakes, doubts about actions, personal standards, parental expectations, parental criticism, and organisation. Items are rated from 1 to 5, with total scores ranging from 35 to 175. Although no standard cut-off exists, higher scores reflect greater maladaptive perfectionism. The Spanish version showed good reliability (α = .93 overall; Gelabert et al., 2011). • Motivation to Change Ruler (Miller & Rollnick, 1999). A two-item visual analogue scale assessing perceived importance and confidence regarding change, scored from 1 to 10. • Ad hoc satisfaction questionnaire. A 20-item measure developed for this study to explore the patient’s perceptions of the usefulness of the MANTRA program. It assessed dimensions such as understanding of the disorder, emotional regulation, motivation to change, and perceived relevance of the program content. This questionnaire was administered post-intervention.
Carer Assessment Measures
• Family Questionnaire (FQ; Wiedemann et al., 2002). A 20-item measure assessing expressed emotion through two subscales: Critical Comments (CC) and Emotional Over-Involvement (EOI). Each item is rated on a 4-point Likert scale. Clinical thresholds are typically set at CC ≥23 and EOI ≥27, with higher scores indicating elevated expressed emotion. The Spanish version showed good reliability (Sepúlveda et al., 2014). • Eating Disorder Symptom Impact Scale (EDSIS; Sepulveda, Lopez, et al., 2008). A 24-item self-report assessing the perceived impact of the disorder on carers across four domains: nutritional difficulties, guilt, social isolation, and dysfunctional behaviours. Scores above 50 may indicate clinically significant distress. The Spanish validation demonstrated good reliability (α = .74–.88; Carral-Fernández et al., 2013). • Accommodation and Enabling Scale for Eating Disorders (AESED; Sepúlveda et al., 2009). A 33-item scale evaluating the extent to which carers accommodate or enable eating disorder symptoms (e.g., allowing food avoidance, changing family routines). Items are rated on a 0–4 scale, with total scores ranging from 0 to 132. Scores above 90 may reflect excessive accommodation. The Spanish version showed good reliability (α = .74–.89; Quiles Marcos et al., 2015). • Caregiver Skills Scale (CASK; Hibbs et al., 2015). A 27-item scale measuring six key caregiving skills: emotional regulation, self-care, verbal containment, acceptance, cognitive flexibility, and frustration tolerance. Total scores range from 27 to 135; higher scores indicate stronger caregiving competencies. The Spanish validation showed adequate internal consistency (α = .70–.75; Vintró-Alcaraz et al., 2018). • DASS-21. Also completed by the carer to assess their own levels of emotional distress, following the same scoring and interpretation as described above. • Ad hoc satisfaction questionnaire. A 14-item tool developed for this study to assess carers’ perceptions of the ECHO intervention. It evaluated perceived improvements in understanding of the disorder, communication with the patient, emotional support, and conflict management skills. This measure was administered at post-intervention.
Case Conceptualization
The case was conceptualized using the cognitive–interpersonal model of anorexia nervosa (AN), which proposes that the interaction between specific personality traits and relational dynamics contributes to the development and maintenance of the disorder (Schmidt & Treasure, 2006). According to this model, individuals with AN often display a set of predisposing cognitive–emotional traits—such as perfectionism, cognitive rigidity, high levels of self-control, and emotional avoidance—that interact with stressful life events and interpersonal contexts to reinforce illness behaviors. These traits are frequently shaped by early developmental experiences and are maintained by interpersonal reactions that inadvertently support the disorder.
In A.’s case, several intrapersonal vulnerabilities were identified. From a young age, she exhibited traits of perfectionism, emotional inhibition, and an intense drive for achievement—features that aligned with the cognitive–emotional profile described in the model. These traits were reinforced within a familial context marked by strict discipline, religious conservatism, and high performance expectations. As the third of six siblings in a Catholic, Neocatechumenal household, she often experienced pressure to meet high moral and behavioral standards. Within this environment, she reported feeling invisible and compared to her siblings, internalizing a self-concept that linked approval and self-worth to performance and compliance.
These cognitive–emotional tendencies were further amplified by her immersion in the professional dance world, a setting that valorizes control, discipline, and aesthetic perfection. Here, her pre-existing vulnerabilities found a socially sanctioned outlet, reinforcing her need to regulate anxiety and self-worth through restrictive eating, overexercising, and rigid routines. Life events such as the COVID-19 lockdown and the loss of a professional opportunity abroad functioned as triggers, intensifying her perceived loss of control and prompting a relapse into disordered eating. In line with the MANTRA model—a clinical application of the cognitive–interpersonal framework—her symptoms served to manage internal distress while offering a sense of structure, identity, and predictability (Schmidt & Treasure, 2006).
Interpersonally, the patient’s close relationship with her mother played a central role in maintaining illness behaviors. Although emotionally supportive, the mother’s caregiving style was characterized by high involvement, overprotection, and difficulty setting boundaries—patterns often seen in families of individuals with AN (Treasure et al., 2021). For instance, during early therapy sessions, the mother would direct the patient to disclose specific personal content and insisted on controlling the therapeutic narrative, which undermined the patient’s autonomy and interfered with the therapeutic process. These behaviors reflected maladaptive family communication patterns, including role confusion, overinvolvement, and emotional enmeshment, which contributed to the patient’s difficulty in developing independence and emotional differentiation.
The dynamic between mother and daughter exemplified how well-intentioned caregiving responses—such as accommodating rituals or avoiding conflict—can reinforce the illness by reducing the patient’s exposure to corrective experiences and delaying emotional development. These observations aligned with evidence suggesting that interpersonal responses can serve as maintaining mechanisms by inadvertently validating disordered behaviors and diminishing the patient’s capacity for self-regulation (Schmidt & Treasure, 2006).
This formulation underscored the need for a dual-focus intervention targeting both intrapersonal vulnerabilities (e.g., perfectionism, emotional avoidance, rigidity) and interpersonal maintaining factors (e.g., carer accommodation, communication style). The ECHOMANTRA program was therefore selected as a suitable adjunct to standard care. Its structure integrates patient-focused modules from MANTRA—designed to enhance emotional awareness, cognitive flexibility, and identity development—with carer-focused ECHO sessions, aimed at reducing accommodation and improving caregiving strategies. By simultaneously addressing the complementary roles of both patient and carer in maintaining the disorder, the intervention sought to promote more adaptive coping and foster recovery within a relational framework.
Course of Treatment and Assessment of Progress
Treatment Context and Integration With Day Hospital Care
A. was enrolled in a specialized day hospital program for eating disorders, an intensive treatment modality involving attendance five days a week (Monday to Friday, 9:00 to 15:00). The program provided a structured daily schedule combining individual psychotherapy, psychiatric monitoring, nutritional support, and a variety of therapeutic groups, with breaks for snacks and lunch. During the first four months of treatment, the patient was unemployed and able to fully engage with the program; she later resumed part-time work as a dance teacher, coinciding with clinical improvement.
Group therapies targeted a wide range of areas relevant to eating disorder recovery, including body image, nutrition, dialectical behavior therapy (DBT), interpersonal conflict resolution, bibliotherapy, and psychoeducation (e.g., on ED and personality traits). In addition, several sessions focused on fostering autonomy and daily functioning through self-care, self-help strategies, and “adult life” skills, which encouraged reflection on key life domains (e.g., work, relationships, family, leisure) and goal-setting. Weekly individual psychotherapy initially integrated psychodynamic and behavioral strategies, focusing first on symptom containment and weight restoration, then exploring the symbolic meaning of symptoms and emotional defense mechanisms. After weight stabilization, the patient transitioned to transference-focused psychotherapy (TFP), aimed at addressing underlying narcissistic personality traits. Notable gains were made in emotional insight, relational depth, and goal-directed behavior.
Nutritional support involved weekly consultations with a dietitian to monitor weight, guide renourishment, and address distorted beliefs about food. Overall, the day hospital program targeted symptom stabilization and psychological insight through a combination of practical, cognitive, and affective interventions. The ECHOMANTRA program was delivered in parallel as an adjunct to treatment-as-usual (TAU), offering a complementary focus on maintaining mechanisms and the caregiving context.
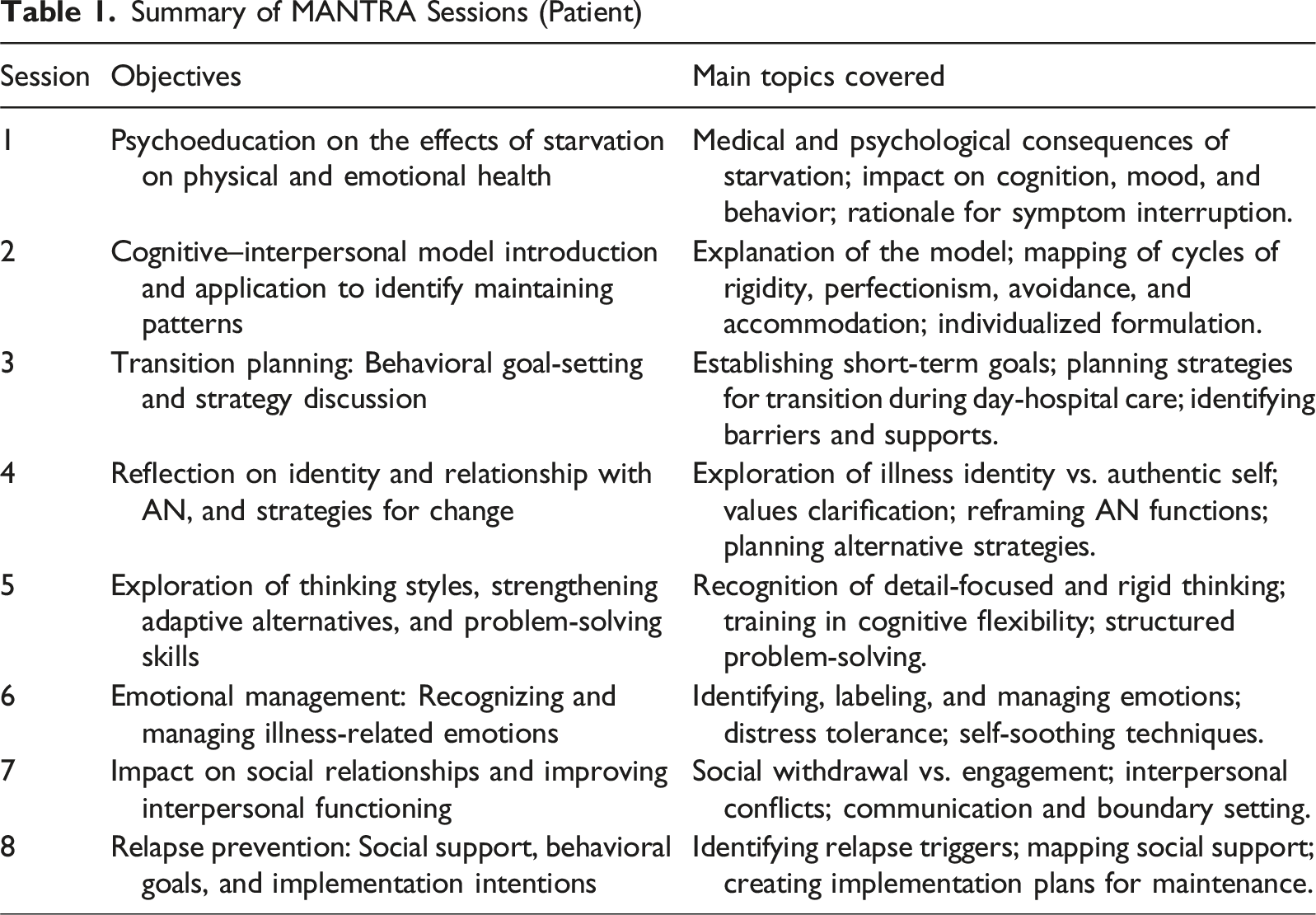
Overview of Intervention Content
Summary of MANTRA Sessions (Patient)
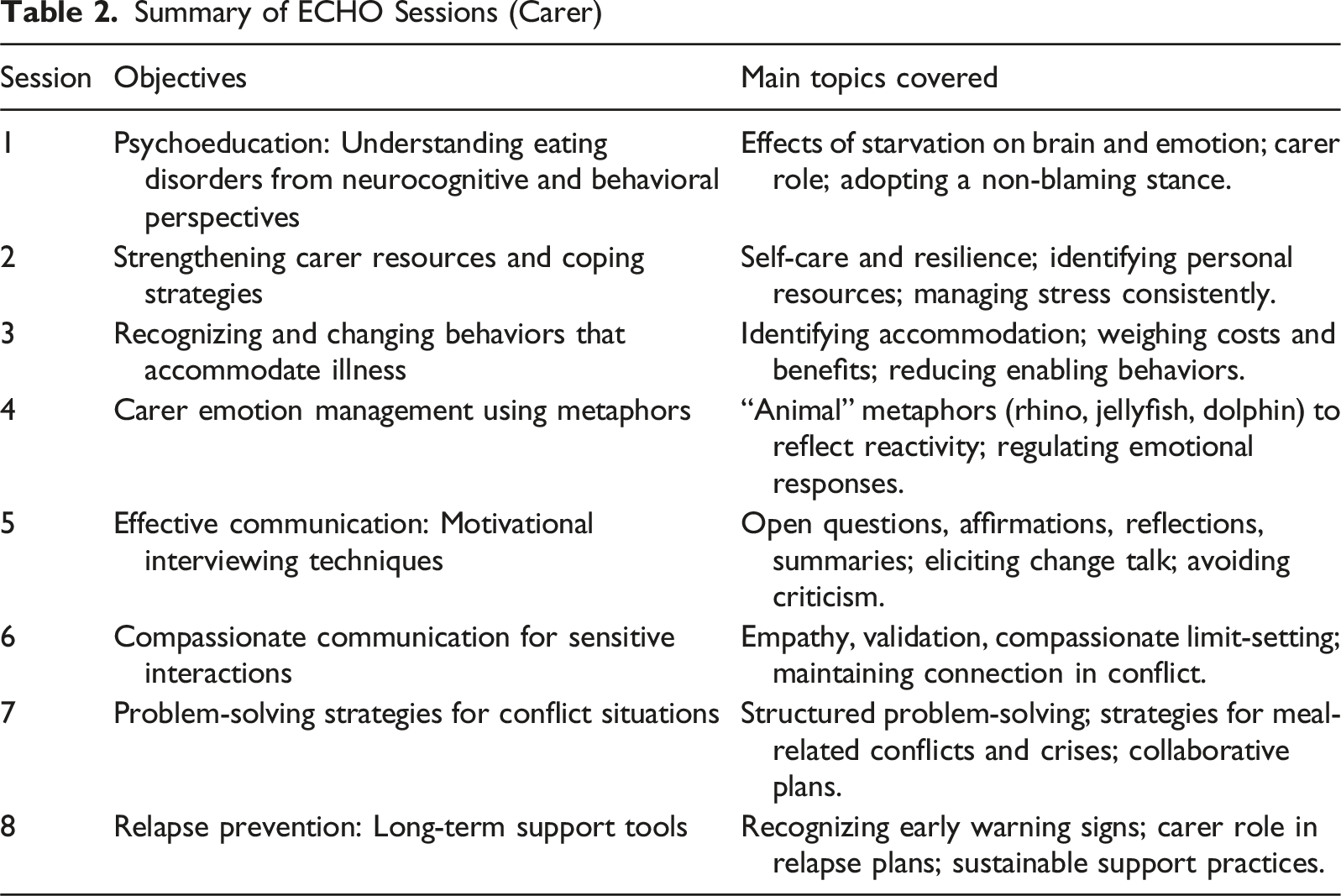
Summary of ECHO Sessions (Carer)
Session Structure and Materials
The ECHOMANTRA intervention followed a structured, session-by-session format for both patient and carer, guided by printed workbooks designed to support individualized reflection and gradual skill acquisition. Each participant received their own manual, tailored to their respective role (patient or carer), which served as both a roadmap for sessions and a tool for between-session practice.
Each weekly session adhered to a consistent structure: review of previous tasks, delivery of psychoeducational content, guided discussion, and assignment of new exercises. Materials combined written prompts, structured diagrams, and audiovisual components (e.g., clinical vignettes, real-life testimonies) that facilitated emotional engagement and normalization.
For the patient, the MANTRA workbook emphasized self-reflection on cognitive, emotional, and identity-related maintaining factors. One of the key tools used was the “hot cross bun” formulation (Session 2), which helped A. map how her thoughts, feelings, bodily responses, and behaviors interacted in self-perpetuating cycles of control and avoidance. In later sessions, she worked on setting short- and medium-term recovery goals (Session 3), including concrete steps and contingency plans, and completed emotion regulation tasks (Session 6), such as identifying helpful activities and using self-monitoring logs to explore emotional triggers and unmet needs.
For the carer, the ECHO workbook provided a parallel path of insight and change, focusing on understanding ED mechanisms, reducing accommodation, and practicing non-confrontational communication. Early sessions included reflective activities like distinguishing helpful versus unhelpful responses and identifying personal values (Session 2). Midway through the intervention, metaphors such as the “trampoline” or the “broken leg” were used to illustrate how carers could offer support while fostering autonomy (Session 4). Role-play exercises and written scripts later supported the development of more emotionally attuned and boundaried communication.
While the patient’s sessions fostered internal change—emotional literacy, cognitive flexibility, and self-compassion—the carer’s sessions targeted external factors that reinforced illness behaviors, such as enabling patterns or emotional overinvolvement. This dual approach allowed each participant to work on their respective domains, while moving toward shared goals of recovery and relational repair.
In both cases, the structured yet accessible format of the materials was cited as instrumental in facilitating engagement. The workbooks encouraged active participation beyond the sessions, and the audiovisual content increased motivation and emotional resonance. Together, these elements provided a scaffolded learning process that blended education, self-awareness, and behavioral experimentation.
Engagement and Adherence
The patient attended all eight sessions, actively engaging in reflective exercises and discussions. She consistently completed the assigned homework and reported that the structured content and personal formulation enhanced her understanding of the illness. The carer also attended all sessions but completed fewer between-session tasks (approximately 37.5%).
Quantitative Outcomes and Patient Progress
To evaluate the effectiveness of the intervention, changes in scores from the scales administered at three assessment points (T0 = baseline, T1 = post-treatment, T2 = follow-up) were analyzed. Clinical change was first examined by comparing scores to established cutoff points for each instrument, identifying transitions between clinical and non-clinical ranges. Subsequently, the Reliable Change Index (RCI) was calculated following Jacobson & Truax (1991) to determine whether score differences between time points exceeded expected measurement error. Changes with an RCI ≥ ±1.96 (p < .05) were considered statistically reliable. This approach enabled the assessment of both the statistical significance and the clinical relevance of observed changes throughout the intervention period.
Scores and Reliable Change Index Results for the Patient
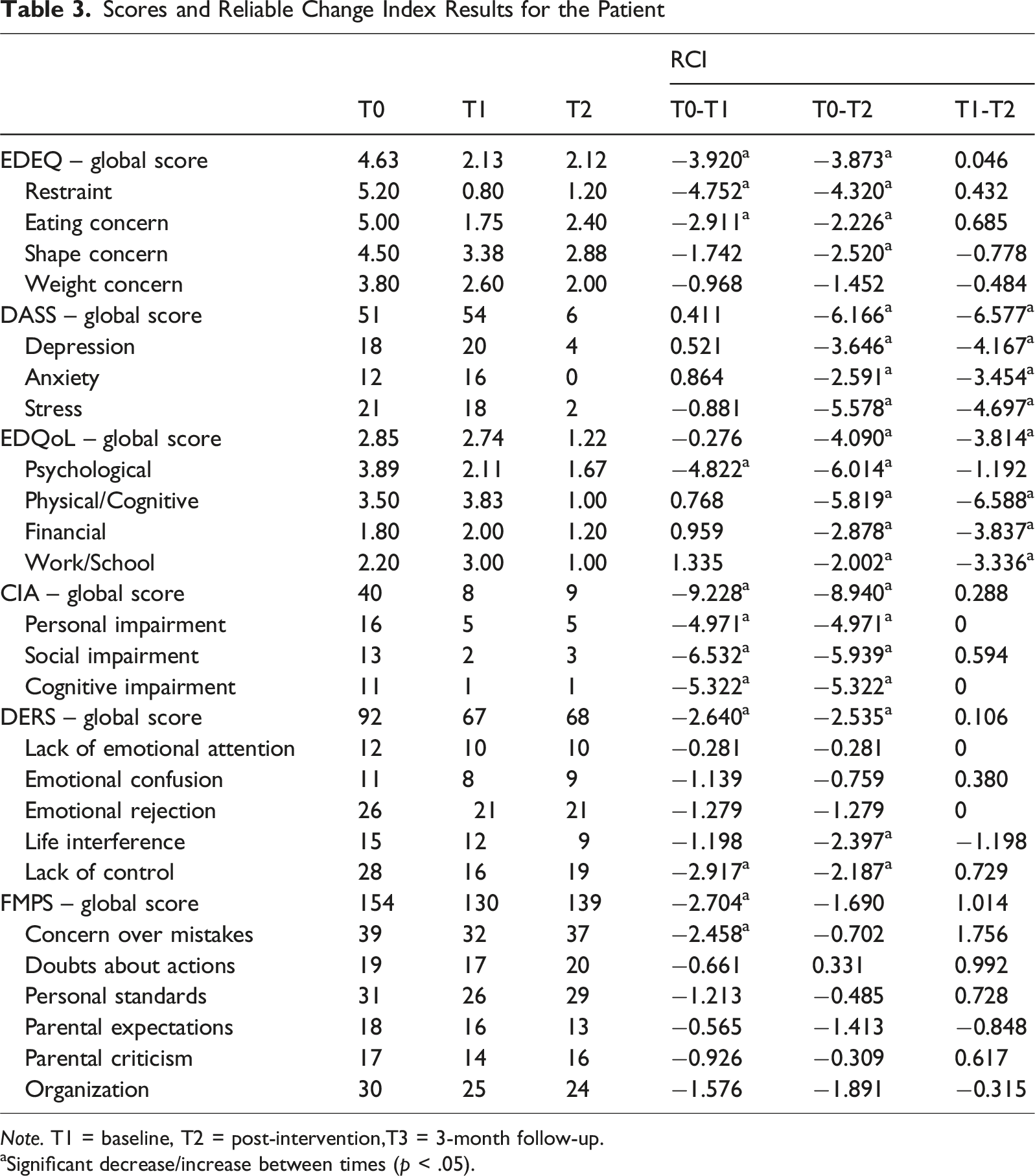
Note. T1 = baseline, T2 = post-intervention,T3 = 3-month follow-up.
aSignificant decrease/increase between times (p < .05).
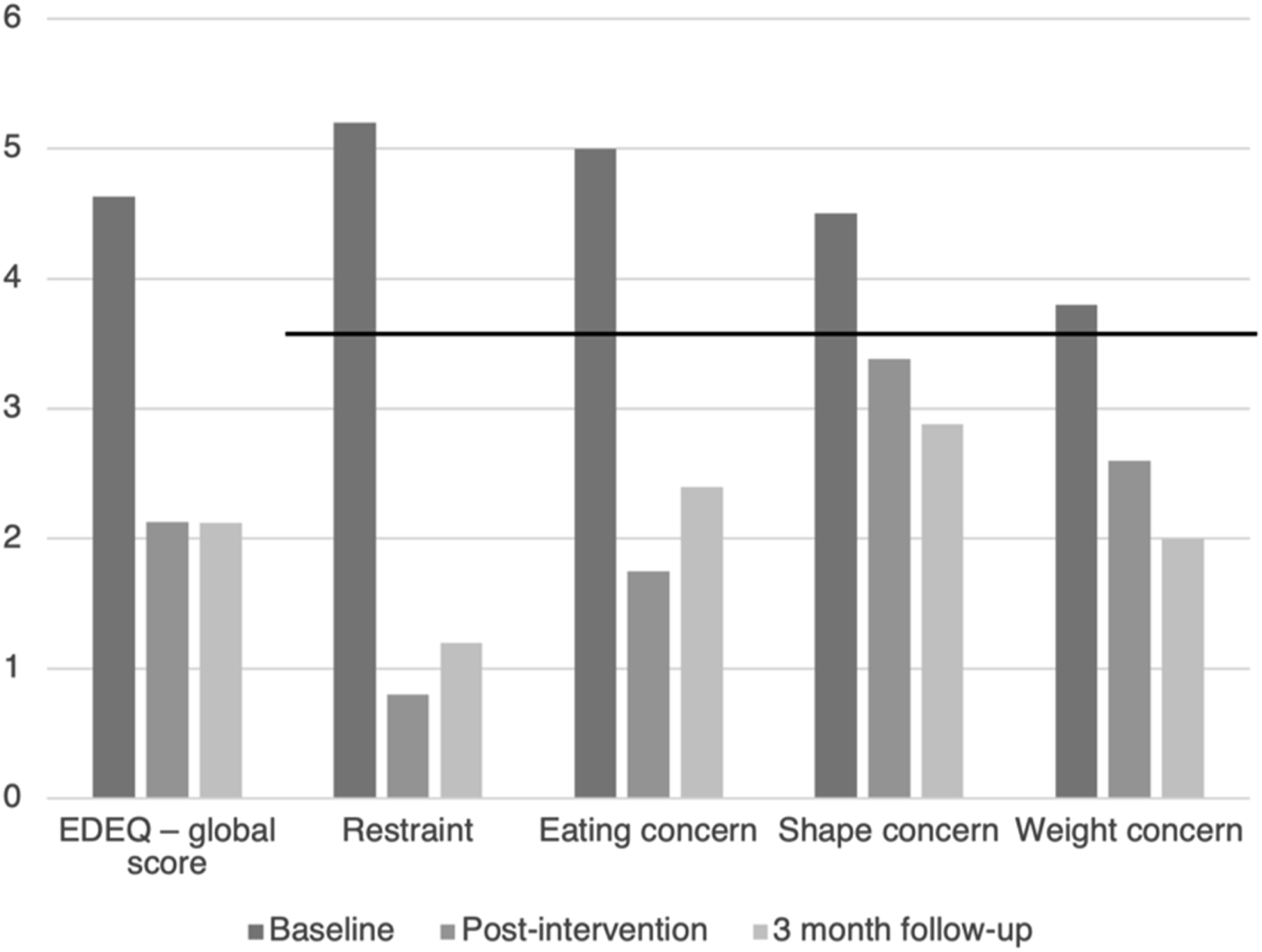
EDE-Q scores with cutoff points for the subscales
In addition to self-report outcomes, clinically relevant changes were also observed in weight and BMI. At baseline, the patient had a BMI of 17.8 and weighed 46.2 kg. By the end of treatment (ECHOMANTRA + TAU), her BMI had increased to 21.7 with a corresponding weight of 56.2 kg, indicating full weight restoration and supporting the clinical significance of symptom reduction.
Emotional regulation capacities, assessed through the DERS, improved significantly, suggesting enhanced ability to identify, tolerate, and express emotional states. Interestingly, scores on the DASS-21 revealed a temporary increase in psychological distress immediately following treatment (Figure 2). This pattern was interpreted as a reflection of greater emotional contact and illness insight, a phenomenon previously described in the literature (Gorwood et al., 2019), and occurred in parallel with continued progress in core AN symptoms and reflective capacity. DASS-21 scores with cutoff points for the subscales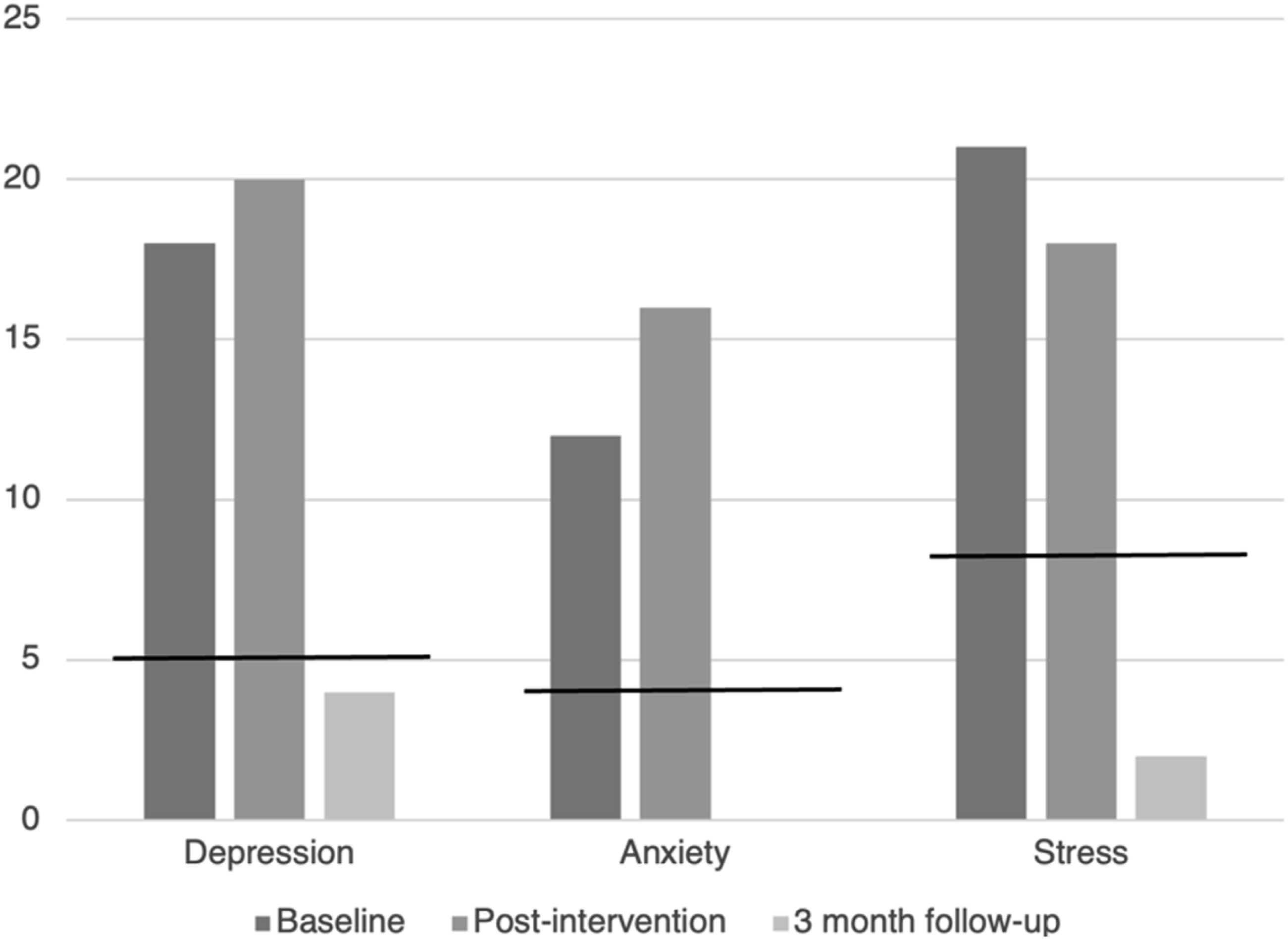
Regarding perfectionism, FMPS scores demonstrated significant post-treatment improvement, indicating increased cognitive flexibility and reduced self-critical thinking. Qualitative feedback further supported these findings: the patient reported feeling “more in touch” with her emotional needs and perceived greater control over binge–purge episodes. Taken together, these outcomes suggest that the intervention effectively addressed several of the core cognitive and emotional maintaining mechanisms outlined in the MANTRA model.
Carer Outcomes
Scores and Reliable Change Index Results for the Carer
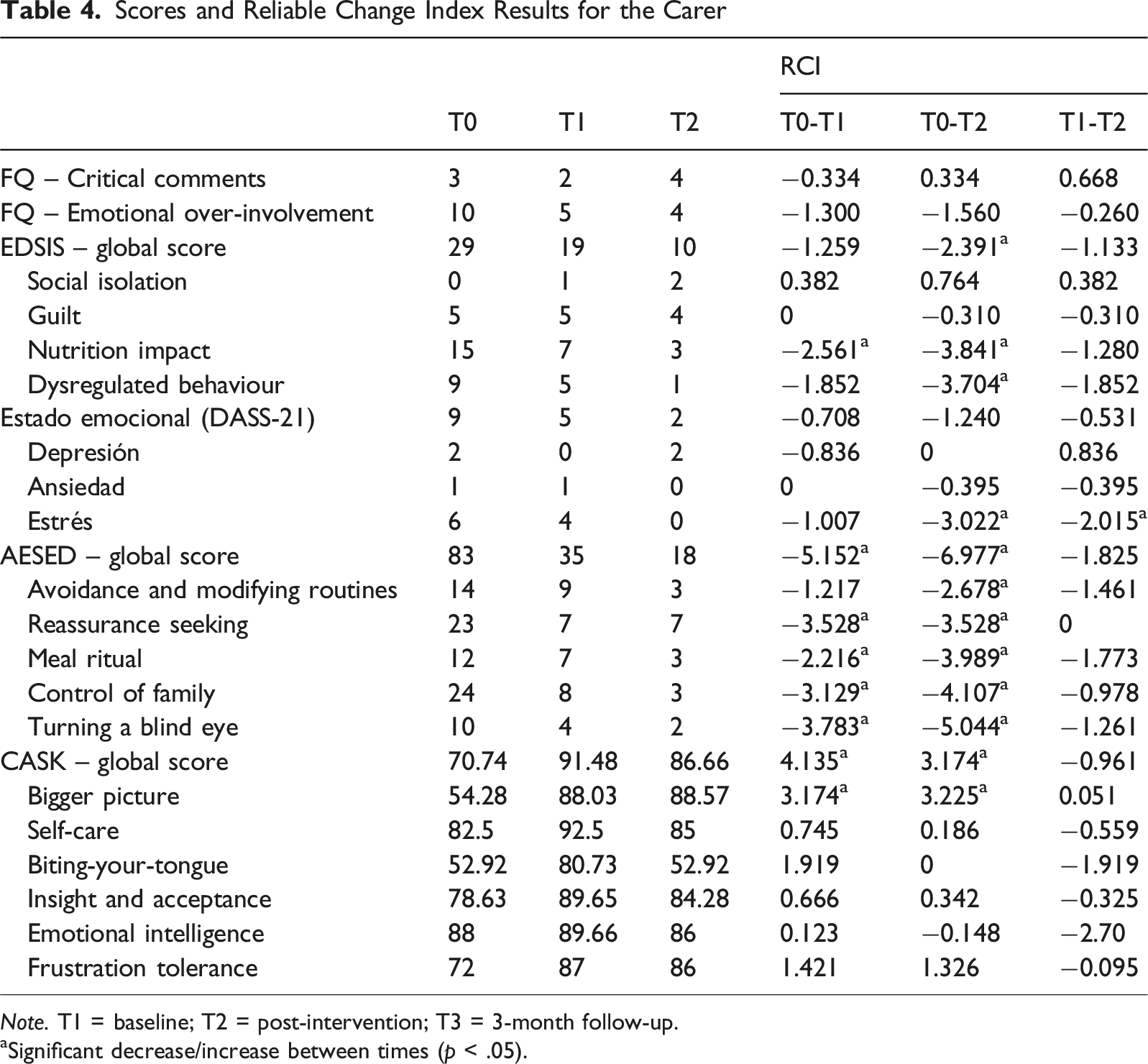
Note. T1 = baseline; T2 = post-intervention; T3 = 3-month follow-up.
aSignificant decrease/increase between times (p < .05).
Taken together, these patterns are consistent with recent findings suggesting that ECHO-based interventions can facilitate shifts in carers’ emotional responses, enhance empathic understanding, and promote a more supportive and less controlling caregiving stance (Ruiz et al., 2024).
Participant Feedback and Program Evaluation
In addition to quantitative measures, both participants provided structured feedback on their experience with the program. These evaluations offered insight into the perceived usefulness, relevance, and acceptability of the intervention content. Overall, ratings reflected high satisfaction and perceived benefit, suggesting that the materials and session structure were accessible and meaningful for both participants.
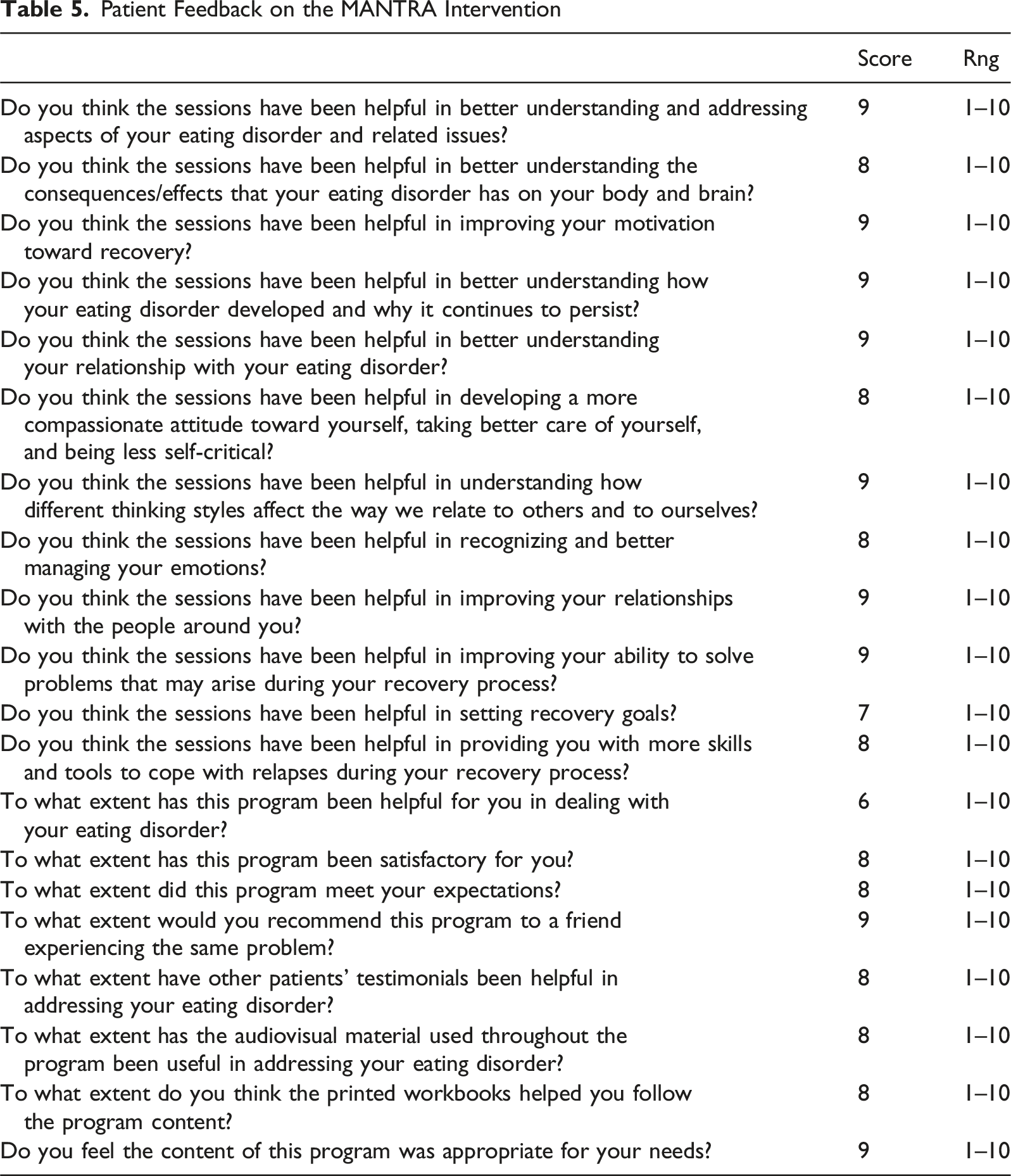
Patient Feedback on the MANTRA Intervention
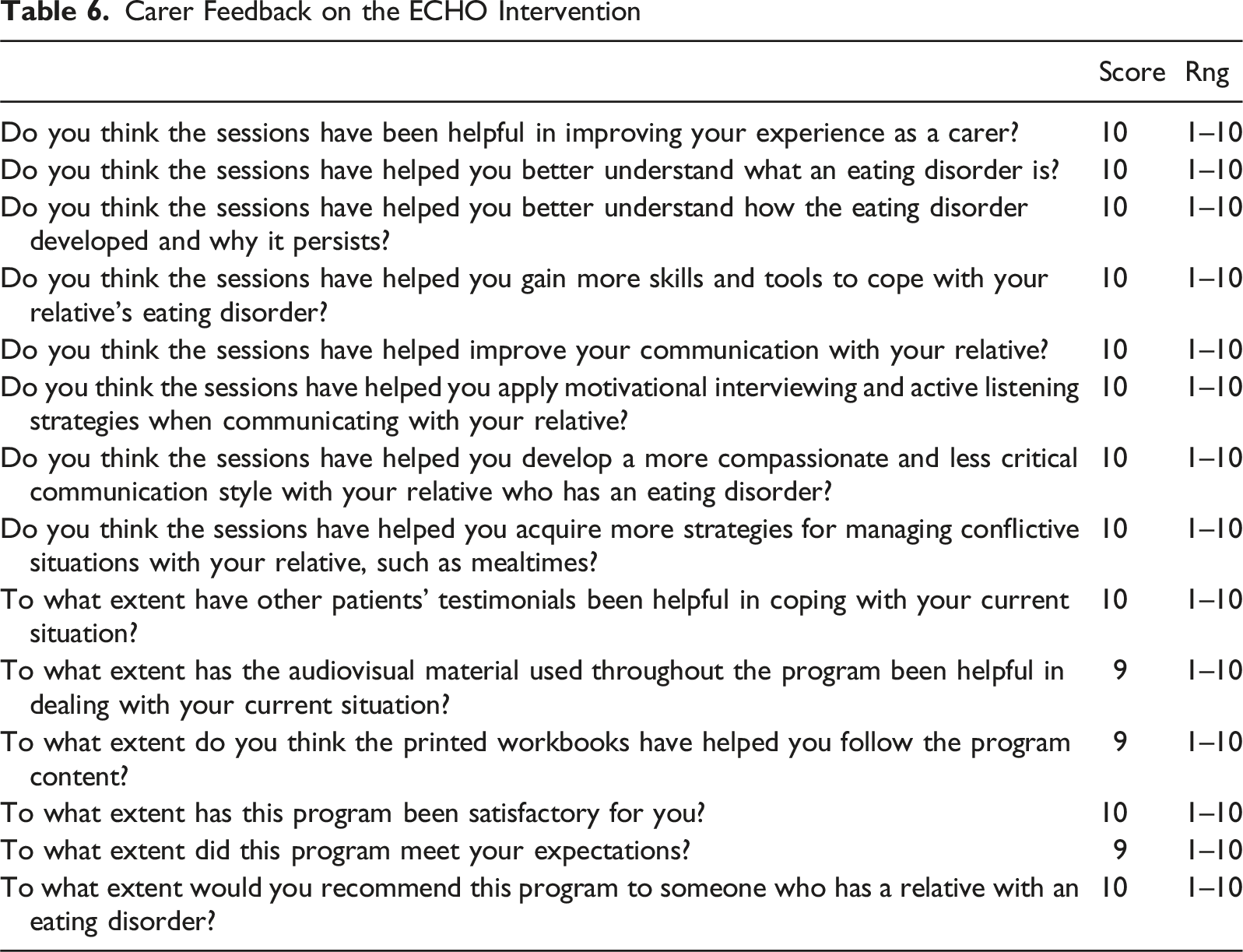
Carer Feedback on the ECHO Intervention
Together, these results suggest that ECHOMANTRA was not only effective in promoting measurable changes but also well-received and meaningful, reinforcing its acceptability and clinical feasibility.
Complicating Factors
Several clinical and contextual factors complicated the therapeutic process by intermittently interfering with engagement, flexibility, and emotional tolerance.
A central challenge was the patient’s entrenched perfectionism, which extended beyond symptom expression and permeated her professional identity and self-evaluation. This tendency frequently emerged in therapy as rigid goal setting and an intolerance for incremental progress. For example, she often framed recovery in dichotomous terms (e.g., “either I do this perfectly or I have failed”), which increased self-criticism following minor setbacks and, at times, led to urges to re-engage in restrictive or compensatory behaviors. Clinically, this pattern required ongoing reformulation of goals into process-oriented and values-based targets, as well as repeated emphasis on flexibility and self-compassion to maintain therapeutic momentum.
Maternal overinvolvement constituted a second complicating factor at the interpersonal level. Although driven by concern, the mother’s caregiving style initially involved close monitoring of eating behaviors, frequent reassurance, and attempts to direct therapeutic content. These responses occasionally reduced the patient’s opportunity to experience and manage distress independently, reinforcing dependency and limiting the development of autonomy. During moments of heightened tension—such as meal-related conflicts or emotional withdrawal—the clinician worked with both participants to slow down interactions, clarify roles, and practice non-directive, emotionally attuned communication, thereby reducing escalation and preserving engagement.
An additional challenge emerged in the form of increased emotional distress during the middle phase of the intervention. As the patient developed greater awareness of her cognitive and emotional patterns, she reported heightened anxiety, sadness, and self-doubt. Rather than interpreting this as clinical deterioration, the treating clinician framed these reactions as part of an adaptive process of emotional contact and insight development. Sessions were adjusted to include greater emotional validation, grounding strategies, and pacing of reflective exercises, which helped prevent disengagement and supported continued participation.
Finally, broader contextual influences—particularly the performance-oriented culture of professional dance and strong family interdependence—periodically reinforced high standards, fear of failure, and ambivalence toward recovery. These external pressures sometimes reactivated core beliefs linking self-worth to achievement and control, requiring repeated integration of real-life stressors into the therapeutic formulation.
Taken together, these complicating factors highlight the dynamic interplay between intrapersonal traits, interpersonal responses, and sociocultural context in adult AN. Their management required a flexible, formulation-driven approach that balanced emotional containment with the gradual promotion of autonomy, reinforcing the value of dual-focus interventions that address both patient vulnerabilities and caregiving patterns.
Access and Barriers to Care
The patient initially pursued outpatient treatment on her own initiative, motivated by a growing awareness that her restrictive eating behaviors and emotional distress were no longer manageable without professional support. While this outpatient care led to a partial remission, its limited intensity—alongside systemic constraints in adult eating disorder services—likely contributed to her vulnerability to relapse.
Her subsequent referral to a specialized day hospital provided access to a more comprehensive, multidisciplinary treatment framework. This included medical, nutritional, psychiatric, and psychotherapeutic components, which allowed for a more sustained therapeutic engagement. Importantly, the concurrent implementation of the ECHOMANTRA program was made possible through online platforms, which minimized logistical barriers and enabled both the patient and her primary carer to participate regularly despite their respective daily obligations.
However, broader structural limitations within the healthcare system continued to pose significant challenges. Access to specialized services for adults with eating disorders remains scarce, and evidence-based interventions that formally integrate carers are seldom available outside the scope of research. These systemic barriers highlight the ongoing difficulty faced by many adult patients in accessing comprehensive, family-inclusive care. They also reinforce the relevance and potential value of structured programs like ECHOMANTRA in bridging gaps in current service provision.
Follow-Up
Three months after completing the ECHOMANTRA program, both the patient and her mother participated in a follow-up assessment to evaluate the maintenance of therapeutic gains.
At this stage, the patient continued to show marked improvement relative to baseline (Table 4). Reductions in eating disorder symptomatology, as measured by the EDE-Q, were sustained (Figure 1), and improvements in functional impairment (CIA 3.0) remained stable. Notably, illness-related quality of life (EDQoL) showed further enhancement compared to post-treatment levels, indicating ongoing recovery in daily functioning. Emotion regulation difficulties (DERS) also continued to decrease, suggesting a progressive consolidation of emotional regulation skills over time (Adamson et al., 2019; Byrne et al., 2017).
Importantly, the temporary increase in psychological distress observed immediately after treatment, as reflected in the DASS-21 scores, had subsided by follow-up. These scores fell below baseline levels, indicating not only symptom reduction but also improved adjustment to emotional awareness developed during the intervention (Figure 2).
Physical health indicators also demonstrated continued stability. The patient’s BMI remained at 21.7, with a slight increase in weight from 56.2 kg at post-treatment to 56.3 kg at follow-up, indicating successful maintenance of full weight restoration. This consistency in nutritional status reinforces the clinical significance and durability of the therapeutic gains achieved.
In contrast, scores on the Frost Multidimensional Perfectionism Scale (FMPS) revealed a partial rebound. Although this increase did not coincide with a deterioration in core eating disorder symptoms, it pointed to the persistence of underlying perfectionistic tendencies. This finding aligns with previous literature highlighting perfectionism as a stable cognitive vulnerability that may persist even in the context of clinical improvement (Bardone-Cone et al., 2007; Hewitt & Flett, 1991), and supports the need for continued therapeutic attention in this domain.
The carer’s outcomes also demonstrated sustained progress (Table 5). Reductions in accommodation and enabling behaviors (AESED) and perceived illness impact (EDSIS) were maintained, while improvements in caregiving skills (CASK) remained elevated (Sepulveda et al., 2008). Emotional distress, as measured by the DASS-21, was either stable or slightly reduced compared to baseline, reflecting greater emotional balance and confidence in her caregiving role.
Taken together, these findings indicate a stable maintenance of treatment effects across both patient and carer domains. Improvements in symptomatology, psychosocial functioning, emotional regulation, and caregiving competence were preserved three months after the intervention. While some intrapersonal vulnerabilities—such as perfectionism—remained, the overall pattern supports the durability of ECHOMANTRA’s therapeutic impact and the potential for sustained family-level adaptation beyond program completion.
Treatment Implications of the Case
This case illustrates the potential benefits of integrating both patient- and carer-focused components in the treatment of adult anorexia nervosa (AN). The combined use of MANTRA and ECHO within the ECHOMANTRA framework offered a structured yet adaptable intervention that targeted maintaining mechanisms across individual and relational domains. While MANTRA specifically addressed cognitive rigidity, emotional avoidance, and motivational ambivalence in the patient, ECHO supported the carer in understanding the illness, developing more effective coping strategies, and reducing unhelpful caregiving responses. This parallel structure fostered complementary progress, contributing not only to symptom reduction but also to improvements in autonomy, communication, and mutual understanding.
One notable implication of this case is the feasibility and acceptability of delivering ECHOMANTRA in an online format. The program was implemented in parallel with a day hospital treatment and demonstrated high levels of engagement and adherence. Its telehealth delivery, supported by structured workbooks and audiovisual materials, facilitated learning and continuity—especially for participants managing other responsibilities. These findings suggest that online adjunctive modules may be a viable strategy to enhance intensive treatments for adults, particularly in contexts where logistical or emotional barriers hinder access to face-to-face care (Blalock et al., 2025).
The inclusion of carers as active participants in the recovery process represents another important contribution. In this case, the mother’s involvement helped reduce symptom accommodation and foster more compassionate and consistent communication. These changes were associated with a perceived reduction in caregiver burden and an increase in her confidence to support her daughter. At the same time, they appeared to promote greater autonomy and engagement in the patient. These observations are consistent with emerging evidence supporting the value of family-inclusive interventions in adult populations (Treasure et al., 2021), where carers often remain key sources of emotional and practical support.
Despite these encouraging outcomes, certain limitations must be acknowledged. As a single-case study, the findings cannot be generalized to broader populations or cultural contexts. Moreover, the patient’s simultaneous participation in a structured day hospital program complicates attribution of outcomes solely to the ECHOMANTRA intervention. She had been enrolled in the day hospital and remained in phase 1 throughout the intervention and follow-up period, receiving multidisciplinary support alongside our sessions. While we believe that ECHOMANTRA contributed meaningfully to the therapeutic gains observed, the role of continued intensive treatment must also be recognized in shaping clinical improvements. Additionally, the three-month follow-up period limits conclusions about the long-term sustainability of observed changes. Future research should focus on larger and more diverse samples, employ controlled designs, and include extended follow-up assessments to better determine the program’s efficacy and durability.
Ultimately, this case contributes to the growing literature supporting dual-focus approaches that integrate individualized cognitive–interpersonal models with structured carer interventions. Systematic reviews and meta-analyses have documented that MANTRA shows moderate to large effects on symptom reduction and emotional functioning in adults with AN (Fernández-García & Quiles, 2024), while ECHO has been found to reduce caregiver distress, improve caregiving skills, and enhance perceived support across diverse settings (Quiles et al., 2026). Recent findings from Ruiz et al. (2026) further support this dual-focus model, showing that ECHOMANTRA—when delivered as a combined intervention to adolescent patients and their carers—was associated with significant improvements in motivation, emotional regulation, and therapeutic engagement, alongside reductions in carer accommodation and psychological burden. These results suggest that the integration of both components, as demonstrated in this case, may not only promote intrapersonal recovery but also foster relational resilience across developmental stages. Taken together, these findings highlight ECHOMANTRA’s potential as a promising adjunct to standard care for individuals with complex and enduring forms of AN.
Recommendations to Clinicians and Students
This case demonstrates that structured, mechanism-focused interventions such as ECHOMANTRA can be effectively integrated into intensive treatment settings for adult patients with anorexia nervosa (AN), provided that patient and carer participation are actively coordinated. Therapists should strive to maintain consistent communication between the parallel sessions and ensure alignment of therapeutic goals. This coordination helps translate individual insights into meaningful changes within day-to-day family interactions, reinforcing progress in both members of the dyad.
It is also essential for clinicians to acknowledge the emotional toll that AN imposes on carers. Including carers in the therapeutic process—through psychoeducation, reflective exercises, and skills training—can reduce unhelpful behaviors such as symptom accommodation while promoting empathy, patience, and more adaptive communication. When carers are viewed as partners in recovery, treatment adherence and emotional resilience often improve, benefiting the patient’s recovery trajectory as well as the carer’s own wellbeing.
Furthermore, this case supports the feasibility and acceptability of delivering interventions like ECHOMANTRA in an online format. The use of digital platforms allowed both the patient and carer to engage with the treatment consistently, despite external demands. For clinicians and students, this highlights the importance of developing digital competencies and adapting evidence-based interventions to flexible delivery formats. Mastering the use of structured online tools and maintaining therapeutic presence in virtual settings are increasingly valuable skills in contemporary clinical practice.
Overall, clinicians and trainees are encouraged to adopt a collaborative, system-informed perspective when treating adult AN. Incorporating both individual and relational mechanisms into the treatment plan can enhance outcomes and promote a more holistic recovery process.
Footnotes
Acknowledgments
We thank the patient and her mother for their participation and trust.
Ethical Considerations
The study was approved by the Research Ethics Committee of Miguel Hernández University and by the Ethics Committee of the Biomedical and Health Research Institute of Alicante (ISABIAL). All procedures were conducted in accordance with the ethical standards of the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from both the patient and her primary carer prior to participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science, Innovation and Universities of the Government of Spain under Grant PID2022-138078OB-I00.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.