
Abstract
Cervical cancer is the fourteenth most common cancer in the United Kingdom, with a national screening programme offered to women aged 25–64. Autistic women are significantly less likely than non-autistic women to engage in cervical screening, yet there is limited research examining psychological barriers to uptake. Illness Anxiety Disorder (IAD), characterised by excessive health-related worry alongside checking or avoidance of medical investigation, offers one possible explanatory mechanism. Despite a strong evidence base for cognitive behavioural therapy (CBT) in the treatment of IAD, there is minimal literature addressing its development, maintenance, or treatment in autistic adults, and none focused specifically on autistic women. This clinical case study describes the assessment, formulation, and treatment of an autistic woman presenting with gynecologically focused IAD centred on fears of cervical cancer. An adapted CBT intervention was delivered within a community post-diagnostic autism service over twelve sessions, incorporating structured visual formulation, imagery rescripting, integration of special interests, and targeted family involvement to address interpersonal reassurance processes. Change was monitored using the Short Health Anxiety Inventory alongside goal-based and behavioural indicators. Reliable improvement in health anxiety was observed, with marked reductions in checking behaviours, increased engagement in valued activities, and cessation of crisis service use, although health anxiety scores remained above clinical threshold at treatment end. The case highlights key adaptations required when delivering CBT for IAD in autistic women and discusses clinical implications, limitations, and directions for future research.
Keywords
Theoretical and Research Basis for Treatment
Illness Anxiety Disorder (IAD), often referred to more broadly as ‘health anxiety’ is characterised by excess preoccupation and anxiety about developing serious illness, despite the absence of significant somatic symptoms, and is associated with avoidance and/or pursuance of healthcare investigations. Autism, as a neurodevelopmental difference, is recognised via persistent difficulties with social communication, often alongside restricted and repetitive behaviours and interests, and reported cognitive rigidity and sensory sensitivities (NICE, 2021). Autistic people are more likely to experience co-occurring mental health conditions, including 20% prevalence of anxiety disorders (Lai et al., 2019). Alongside typical experiences of anxiety, qualitative research has identified experiences which appear to reflect autism-specific anxiety symptomology. These include areas of particular relevance to IAD, such as sensory hypersensitivity, elevated intolerance of uncertainty, and ‘somatic anxiety’ – wherein physiological anxiety sensations are experienced either before, or in absence of, anxious cognition (Halim et al., 2018).
Despite links between autism and anxiety disorders, literature on the presentation and treatment of IAD in autistic people is severely limited. When associations between these conditions are examined, autistic adults appear to demonstrate greater health anxiety than non-autistic controls (Galvin & Richards, 2023; Huang et al., 2025). Where both sex differences and autistic traits are studied, women are found to experience IAD more acutely than men (Galvin & Richards, 2023).
It is suggested that autism-specific traits and anxiety symptomology may play a role in IAD in this population. Due to the rigidity of thought often experienced by autistic people, intolerance of uncertainty appears frequently in anxiety focused literature related to this population, and whilst intolerance of uncertainty also plays a significant role in IAD, little research formally connects the two (Kikas et al., 2024). Existing evidence suggests that autistic individuals may demonstrate higher confidence, yet poorer accuracy, in tests of interoceptive awareness when compared with non-autistic people, supporting the hypothesis that autistic people may struggle to differentiate between benign and concerning bodily sensations, and this low sensory registration appears positively associated with IAD (Huang et al., 2025; Williams et al., 2023).
When considering gynecologically focused IAD, it is important to situate psychological processes within a health service context. A small pool of research dedicated to autistic women’s experience of gynaecological healthcare has highlighted the potential impacts that sensory difference, communication difficulties and lack of perceived control may have on gynaecological care in pregnancy, childbirth and when experiencing dysmenorrhea (Gray & Durand, 2023; Samuel et al., 2022). It is likely therefore that settings related to routine gynaecological care such as cervical cancer screening may also present unique and underrecognized challenges for autistic women, with a need to balance benefits against potential traumas, including exacerbation of health-related distress and/or anxiety (Byrnes, 2022). Overall, the identification of research which explores gynaecological health as a specific trigger or maintaining factor in IAD, for both autistic or non-autistic women, proves challenging, and appears to present a gap in current understanding.
When considering potential modalities of formulation and intervention for gynaecological IAD, it is important to note that NICE guidelines for this - and for IAD more broadly - do not currently exist. However a robust evidence base is available for use of cognitive behavioural therapy (CBT) and antidepressant medications (Bailey, 2024). The CBT model for IAD hypothesises that misinterpretations of health information can lead to anxiety, safety seeking behaviours and attentional bias, which maintain the psychological problem (Salkovskis et al., 2003). Intervention involves behavioural experiments targeting feared symptoms, addressing persistent reassurance seeking, reducing rumination and addressing intrusive imagery. Both healthcare and family systems can play a significant role in maintaining IAD, and attention to interpersonal processes is a core feature of many recommended interventions (Halldorsson & Salkovskis, 2017). Links have been established between attention to detail and greater need for reassurance in autistic adults with IAD, hypothesising that difficulty shifting attention may result in increased desire for detailed explanations and psychological support from others (Huang et al., 2025). As such, there have been some developments in the use of systemic therapies for IAD, primarily in child and adolescent patients, however the evidence base for CBT currently dominates literature.
Qualitative research around use of CBT with autistic people notes difficulties with generalisation of in-session strategies to daily life, and implementing core techniques such as identifying and challenging cognitions (Mazurek et al., 2023). Current guidance advises adaptation, including use of concrete, structured approaches, emphasis on behaviour change, involving support systems and incorporating special interests (NICE, 2021). There are no studies or published case examples to date which examine the effectiveness of CBT for IAD in autistic adults or note problem-specific adaptations for this population. This case study aims to explore the efficacy of cognitive behavioural therapy for illness anxiety disorder when adapted for autism.
Case Introduction
Lily (pseudonym) was the subject of an in-house referral for psychological therapy in a post-diagnostic autism support service. She was referred due to high levels of distress related to her physical health, which significantly impacted her daily functioning. This case report follows the clinical cycle for this individual over eight face-to-face and four remote sessions in a community setting.
Presenting Complaints
Lily reported recurring intrusive thoughts about cervical cancer, with associated checking behaviours and distress. She was not engaging with activities she enjoyed due to a fear that this would interfere with her ability to perform frequent, manual, cervical checking. Her healthcare providers were concerned that this self-examination could cause self-inflicted internal damage. She was highly distressed by health-related anxieties and had presented to crisis services with suicidal thoughts. Lily’s distress and risk escalated in response to being offered medical examination, such as receipt of cervical cancer screening letters, or when she encountered information related to cancer.
History
Lily was a cisgender woman in her twenties during the sessions detailed in this case report. She had received her autism diagnosis in adulthood. Her parents were separated, and both were supportive of her, as she lived with one and had regular contact with the other. She was not in education, employment, or training. Lily had previously experienced medical investigation and surgical intervention for a non-cancerous gynaecological health problem. She had a documented history of non-specific anxiety and had previously undertaken CBT for harm-related OCD, which she reportedly had not found helpful, however she was not reporting intrusive OCD thoughts or related compulsions during the assessment and intervention described here. For six months prior to referral Lily was regularly contacting crisis services for suicidal ideation. She was a skilled artist and passionate about dogs and creative pursuits.
Assessment
A trainee clinical psychologist completed a detailed CBT assessment which identified a one-year history of IAD, precipitated by an incident of vaginal bleeding. In response to her anxiety around this event Lily began engaging in her own cervical checking behaviours. Via Socratic questioning across multiple assessment sessions, Lily identified the following goals for therapy: 1. ‘Stop checking my cervix’. For Lily, this would involve both no longer physically investigating her body, and not visually checking toilet paper for blood after using the bathroom. 2. ‘Get my life back’. When explored further, Lily stated that this would mean she had resumed her attendance at a weekly art group by the time therapy finished, and that she would be walking outdoors for at least ten minutes a day, building up to hour-long walks. These were valued activities that were inaccessible to her at the time of assessment, due to her desire to be close to a ‘safe place’ where she could perform body checks.
Risk was monitored regularly via discussion with Lily and her parents. When risk assessed, Lily consistently demonstrated a clear desire to continue her life, as her thoughts around suicide were framing this as an acceptable alternative to losing her life to cancer.
Case Conceptualization
Psychological formulation took place across four sessions and was based on the Salkovskis et al. (2003) model of IAD. This was used to collaboratively develop Lily’s personal ‘vicious flower’ of IAD, with integrated autism-specific factors, as presented diagrammatically in Figure 1 (adapted from Hill & Watts, 2024). Given the centrality of reassurance-seeking within this model, formulation emphasised the ways in which personal and interpersonal reassurance processes served as key maintaining mechanisms in Lily’s presentation. A linked formulation of the interpersonal processes within her family that were contributing to this cycle was later constructed with Lily’s parents, seen in Figure 2. Lily's idiosynctatic ‘vicious flower' of health anxiety, with integrated autism-specific factors.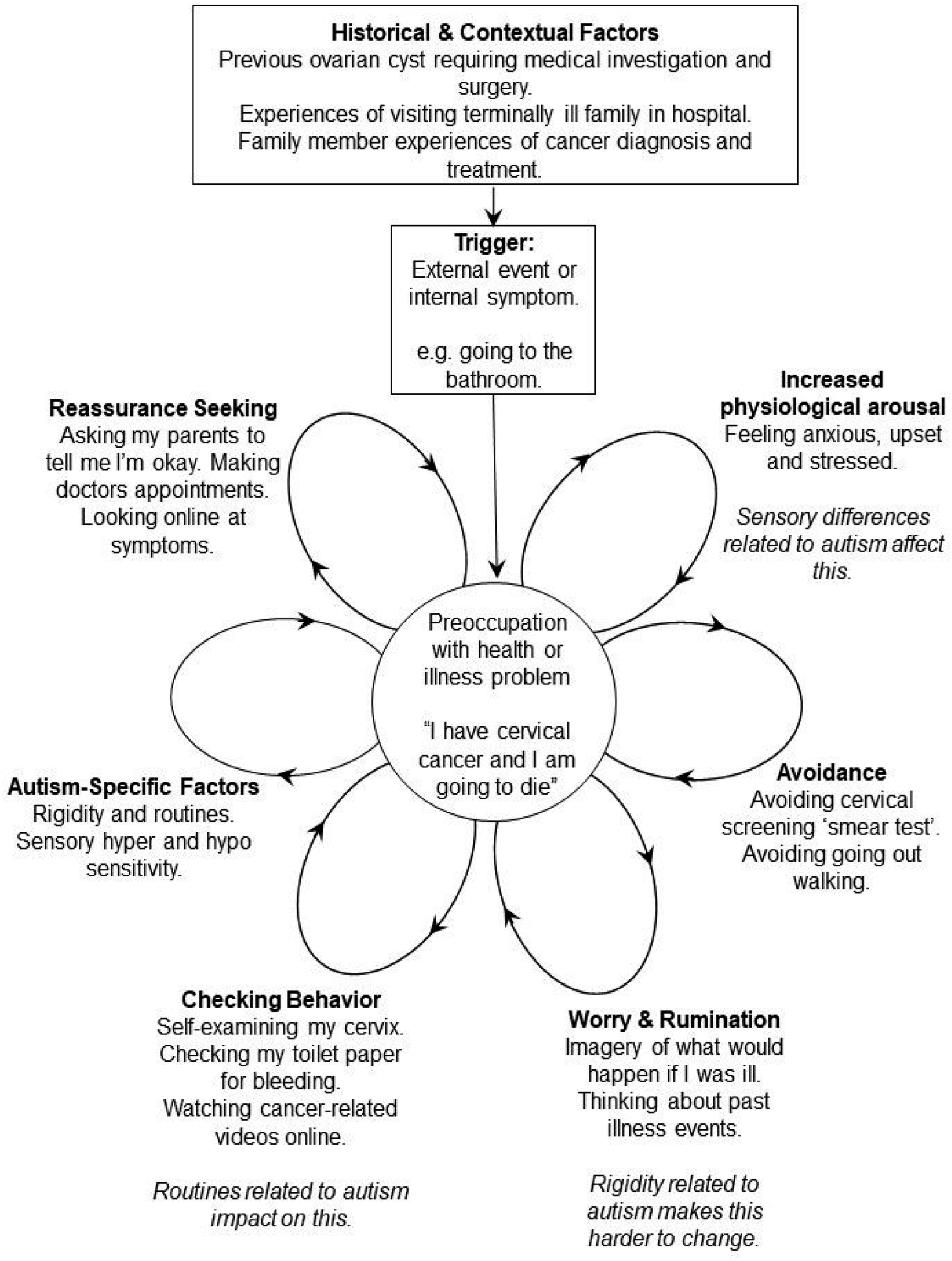
Lily had experienced the death of a family member from gynaecological cancer and had previously undergone gynaecological surgery. Approximately six months prior to therapy referral she experienced unexplained vaginal bleeding, unrelated to her normal menstruation, after which she became certain she had developed cervical cancer. This precipitated a pattern of self-examination and increased doctor appointments. Lily felt unable to undertake a cervical cancer screening test, and discussion of this prompted panic attacks. It appeared that Lily’s needs around both her initial surgery and current anxiety were poorly met within the healthcare system, which contributed to the formation and maintenance of her anxiety. She reported that procedures and appointments related to her previous surgery were not communicated in a way she found accessible, and that medical environments were sensorily overwhelming.
Lily’s family and healthcare staff struggled to understand the relationship between her worries about cervical cancer and her distress related to undertaking a screening test. Lily found that this amplified feelings of isolation, disempowerment, and difference experienced as a result of her broader struggles with social communication. Rigidity of thought related to autism meant Lily found it difficult to redirect herself from these worries. She began watching cancer-related content online, exposing her to health misinformation. She withdrew from pleasurable activities due to a desire to remain close to locations where she could self-examine. Autism-related cognitive rigidity and heightened intolerance of uncertainty appeared to intensify Lily’s difficulty disengaging from threat-based interpretations, making reassurance-seeking particularly compelling and increasing her reliance on behaviours that provided temporary certainty.
Lily began seeking frequent reassurance from medical professionals and family members, typically requiring detailed explanations of gynaecological health to feel briefly reassured, and ultimately reinforcing her belief that only complete certainty could neutralise danger. Interpersonally, Lily’s parents were her primary social contacts, and their responses of either frustration toward persistent reassurance seeking, resulting in dismissal of Lily’s worries, or provision of detailed reassurance related to gynaecology and physiology appeared to play a significant role in the maintenance of Lily’s concerns (Figure 2). Inconsistent responses appeared to function as intermittent reinforcement, thus maintaining the reassurance-seeking cycles. These persistent interpersonal miscommunications appeared to result in Lily feeling increasingly isolated and further craving certainty around her health. Information often used in providing Lily reassurance was that she had received the HPV vaccine in adolescence, had never been sexually active, and was not taking contraceptive medication, meaning her chances of developing cervical cancer were extremely low. Parental formulation of reassurance seeking in illness anxiety disorder.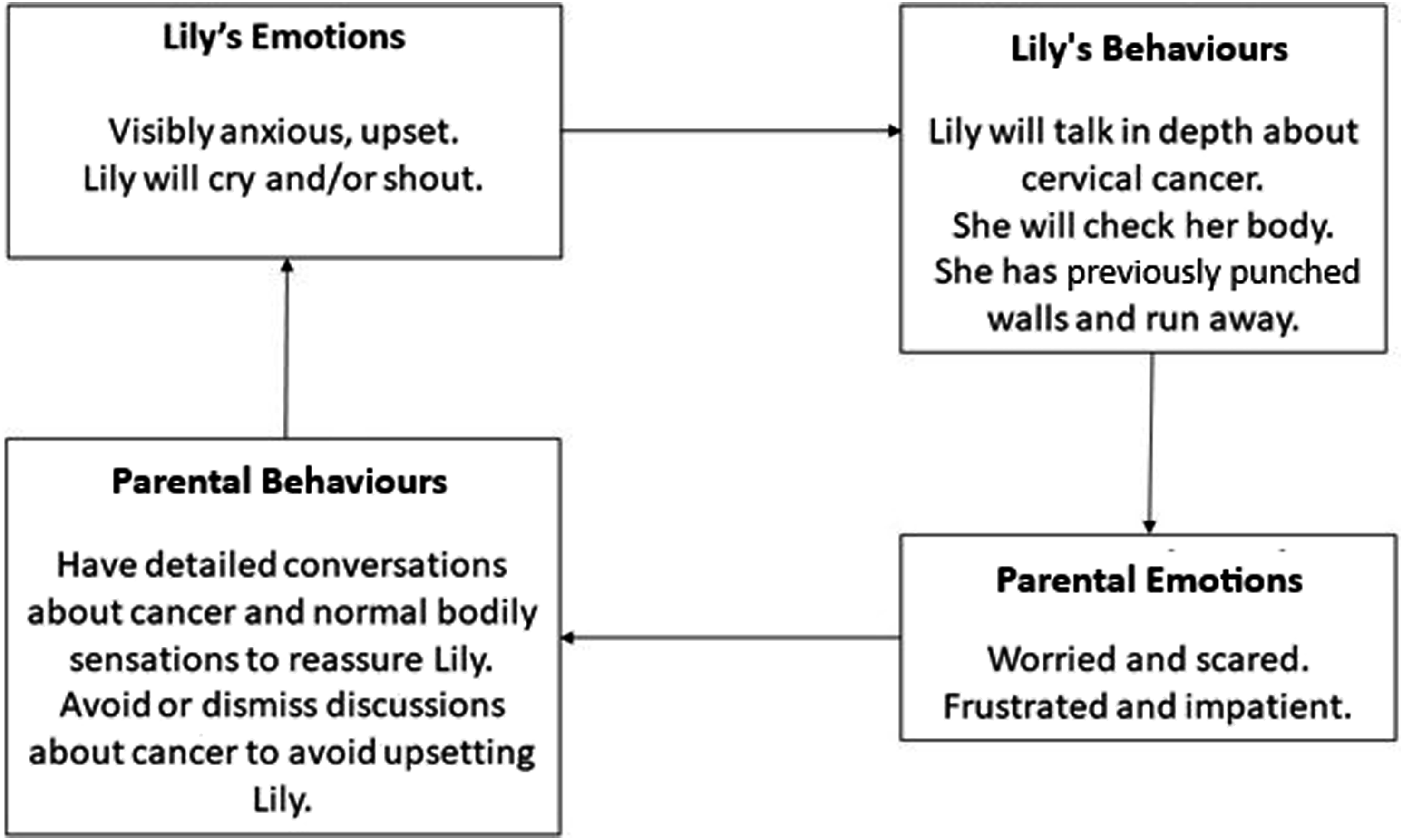
As reassurance became increasingly difficult to obtain or failed to provide lasting certainty, Lily experienced heightened distress and hopelessness. Her withdrawal from valued activities and increased isolation contributed to feelings of despair, which were closely linked to episodes of suicidal ideation. Therapy proceeded with the hypotheses that reducing Lily’s checking and reassurance seeking behaviours, alongside increasing her social contacts, would decrease her levels of health-related anxiety, which would subsequently reduce suicidal ideation.
Course of Treatment and Assessment of Progress
Lily attended 12 appointments over the course of five months; her parents also attended a total of three sessions. These were conducted by a trainee clinical psychologist, under the supervision of an accredited CBT supervisor and a qualified psychologist. Time between sessions was typically one week, and sessions were conducted both in person and virtually. Intervention followed suggested CBT interventions for IAD as constructed by Salkovskis et al. (2003) with adaptations for autism in line with NICE guidelines (2021). A psychological outcome measure was taken at the beginning and end of therapy to monitor change, as Lily could not tolerate weekly measures. A lower total on the Short Health Anxiety Inventory (SHAI; Salkovskis et al., 2002) would be indicative of a reduction in preoccupation with health-related worries. Goal-based outcomes were also used, via monitoring the amount of self-examination Lily performed per day and her degree of re-engagement with valued daily activities, changes in crisis service contact were additionally used to monitor outcomes.
Early sessions focused on risk assessment, as Lily had reported ‘planning her own funeral’ to crisis services. This was identified to be linked to her intense fear of dying from cervical cancer, which had led to extensive rumination about death. Lily disclosed that she thought of suicide as a potential alternative to dying of cancer but was ‘desperate to continue living’. Reflecting this, Lily’s SHAI score demonstrated high levels of health-related anxiety and high perception of the negative consequences of developing a health condition. This was used to inform Lily’s goals for therapy and integrated into a CBT formulation to demonstrate the link between thoughts (worries and images related to cancer), behaviours (planning funeral, checking her body) and emotions (anxiety and fear). Assessment also explored individual adaptions for autism. As Lily found it challenging to move her attention away from rumination on cancer when it was discussed, it was agreed that five minutes at the end of each session would focus on special interests which brought her pleasure, to assist in shifting focus. This was contracted in session one, and a rough visual reminder of session structure which included this adaptation was visible each session.
Theory A and Theory B
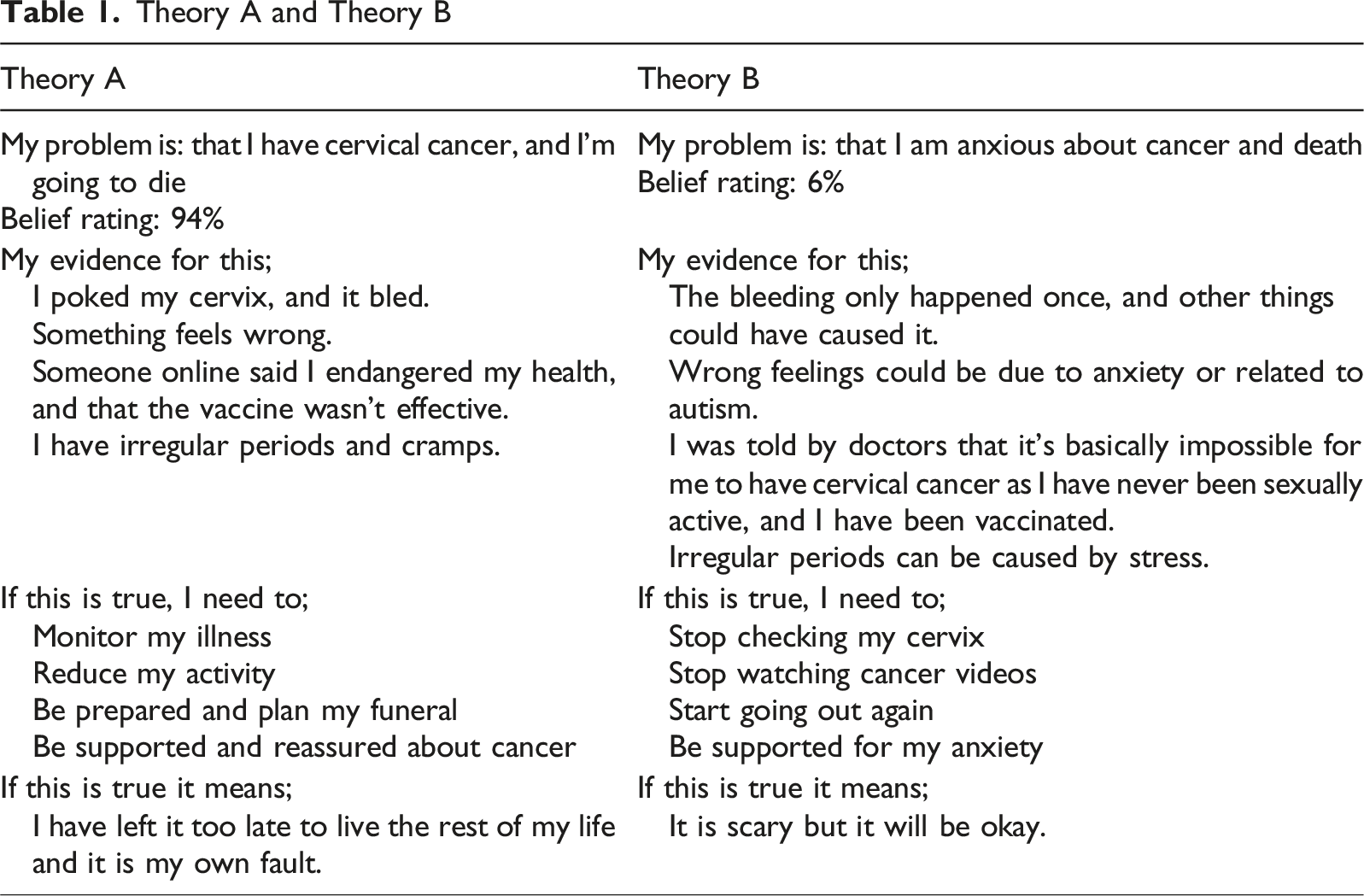
These techniques opened up therapeutic discussion and opportunities for psychoeducation, enabling Lily to begin to identify her physiological symptoms of anxiety. This was accomplished by using body maps, signposting to sources of reliable health information, and using these resources to normalise female bodily experiences and sensations. These techniques guided a decision to reframe anxious thoughts as an ‘anxiety bully’ - helping Lily begin to change her relationship with these through providing a more clear, visual characterisation of her worries.
Lily believed it would be valuable to involve key individuals in her system. Sessions were held separately with each parent to talk through Lily’s formulation and discuss supporting Lily to meet her goals. Both parents had been facilitating access to community activities and were encouraged to continue this, but they expressed worry around Lily’s reassurance seeking.
Lily’s parents were introduced to Theory A/B as a method of understanding the function of providing support versus reassurance. A brief formulation of reassurance seeking in IAD was constructed with each parent as seen in Figure 2 and alternative ‘support’ responses were brainstormed, informed by previous discussions where Lily stated what she would find helpful. Each parent agreed to trial validating the emotional experience of distress, with phrases similar to the following: ‘feeling like that is terrible, I’m here for you no matter what, you can count on me, I will give you a hug.’ One parent strongly expressed that they felt criticised by this intervention, feeling this blamed them for Lily’s distress. Specific psychoeducation around reassurance in health-related anxiety disorders was shared, ensuring that parents’ emotions were validated, and their experiences were normalised alongside Lily’s. Systemic implementation of emotional validation and support in place of reassurance was reviewed with Lily in a later session, where she felt this significantly improved her anxiety. When explored further she stated that this approach made her feel that ‘if the worst happened, I would be okay.’
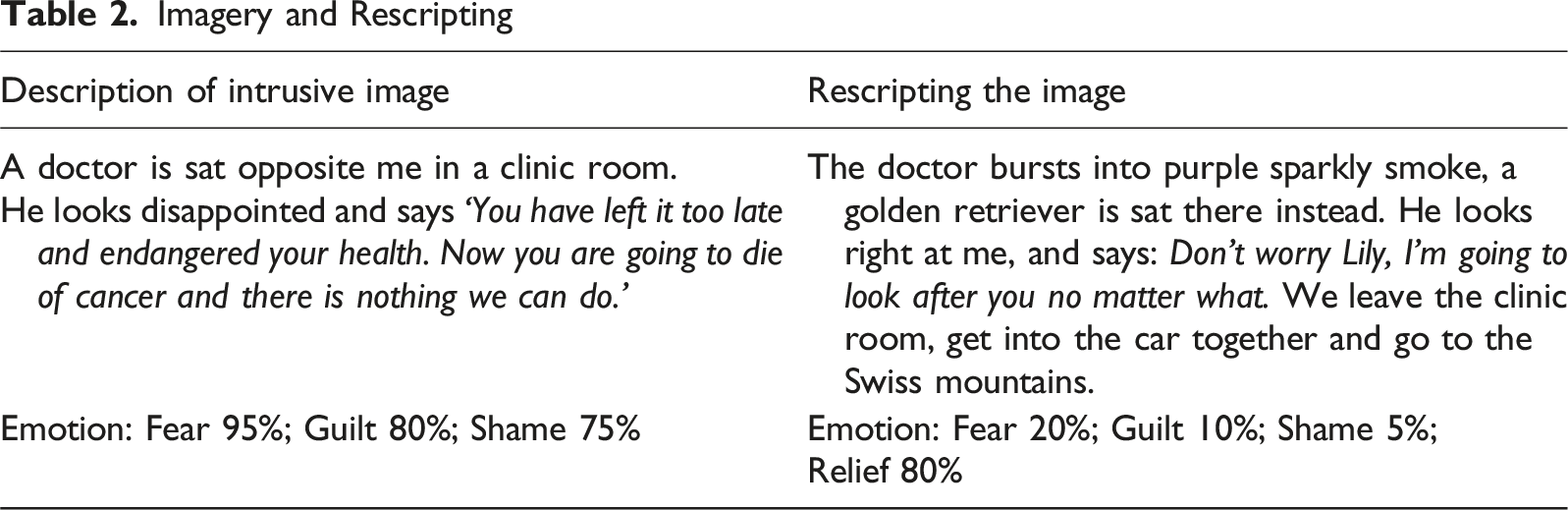
Imagery and Rescripting
The final session involved collaborative development of Lily’s relapse prevention plan with Lily and a parent. An ending letter was written and shared, and the SHAI repeated and reviewed. The concluding half was dedicated to discussing Lily’s special interests, to mirror the format of preceding therapy sessions, and mark the end of the intervention. An onward referral was made to the autism service social prescribing team to enable Lily to continue toward her goal of ‘getting her life back’ and becoming more involved in activities outside home.
Raw SHAI scores can be seen in Figure 3. Lily’s score remained above clinical threshold; however, the difference was indicative of reliable change, exceeding the calculated RCI of 8.23 (Alberts et al., 2013). Goals were monitored to track therapy progression and formally reviewed in the final session. Her first goal, ‘stop checking my cervix’ showed marked improvement. At the beginning of therapy Lily was performing four routine checks and approximately ten spontaneous checks per day, including two occasions where she left the therapy room to do this. At the final session, Lily was completing one routinised check per day and had reduced her spontaneous checks to twice per day. Summary of raw pre- and post-intervention measures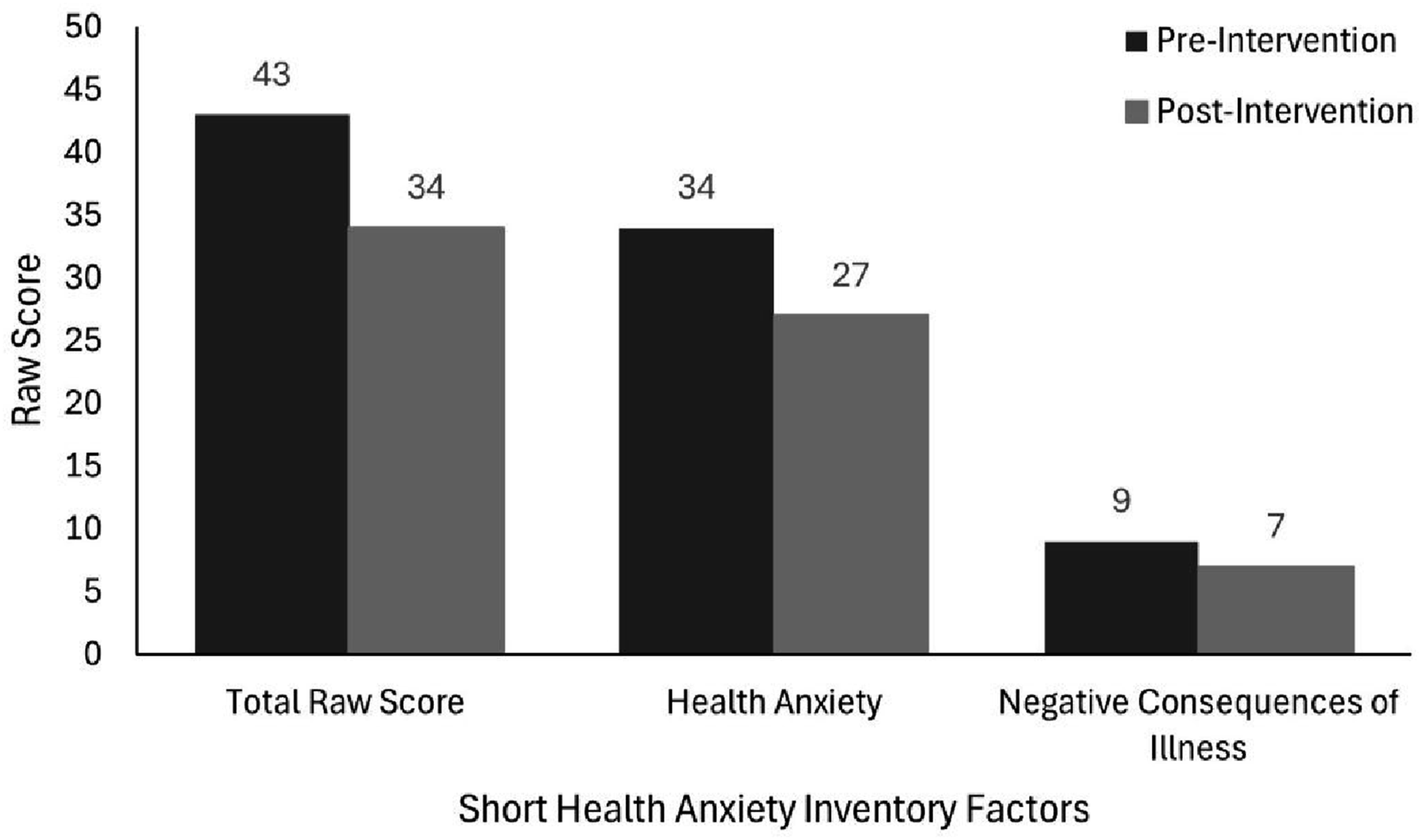
Lily considered her second goal, ‘get my life back’ partially completed. At the conclusion of therapy, she had holidayed abroad with a parent, gone on short walks, and accepted referral to a social prescribing service to progress further. For results not explicitly linked with her goals, Lily had ceased to utilise local crisis services and had demonstrated a decreased belief rating in the statement ‘I have cervical cancer’ from 94% to 35%, alongside a reduction in distress ratings associated with intrusive health-related imagery as shown in Table 2. Qualitatively, Lily reported that she felt ‘understood and listened to’ and that ‘sessions really helped’. She specifically cited the adaptations for autism, such as inclusion of special interests, as integral to this. A parent fed back to the therapist that the approach taken during this intervention ‘was the best fitting one [Lily] had ever had’ and expressed their disappointment that similar adaptations were not available sooner.
Complicating Factors
The principal complicating factor is that this model was untested in autistic populations, with no evidence supporting the acceptability and feasibility of this approach. As a result, it remains unclear which component parts of the intervention were effective, or which can and should be adapted to meet the needs of autistic people receiving this therapy. This is linked to the issue of effective outcome measurement. The SHAI was used at the beginning and end of therapy, due to the level of distress Lily initially experienced when completing it. As a result, it is difficult to determine which specific techniques used were most valuable or precipitated change. This measure has also not been validated in an autistic population, and it is unclear how accurately it was able to identify and monitor IAD for this individual.
Online health information and its role in IAD - dubbed ‘cyberchondria’ - has been shown to exacerbate distress related to health anxieties (Muse et al., 2012; Starcevic et al., 2020). Lily reported that due to her social communication difficulties related to autism, she had struggled to build and maintain a peer group with whom she could discuss ‘normal’ health and bodily experiences, impacting her reliance on internet mediated forms of information. She reported being affected by health misinformation online and using the internet to seek reassurance. As a similar-age therapist working with Lily, consideration of social power and balance in light of this was therefore essential.
Building a therapeutic relationship with Lily required several considerations which were explored by the therapist in supervision. Nuanced discussions of power and difference reflected on Lily’s limited social contact with same-age peers, and the benefits of being able to discuss her presenting problem with a similarly aged female therapist. It was hypothesised that this may be normalising and validating for Lily, utilising the similarities between patient and clinician to allow for a more ‘equal’ discussion of Lily’s fears. However, discussions also considered the therapist’s position of power as a professional operating within the same health system that Lily found highly distressing, and this was exemplified by Lily’s expressed worry in initial sessions that the therapist would ‘just tell me I have to get the test’.
Access and Barriers to Care
Efforts were made to limit barriers to care, Lily’s sessions were held in the local area at a time that suited her, when she was unable to attend in person virtual sessions were arranged, including those with her parents. Autism-related adaptations were seen as core to facilitating access to CBT as a therapeutic approach.
Follow-Up
A follow-up was unable to be conducted, due to the therapist’s departure from the service following the end of their placement in this area.
Treatment Implications of the Case
This case study outlines formulation and intervention for a presenting problem of illness anxiety disorder, to establish the efficacy of CBT for IAD when adapted for an autistic woman. The subject of this case report was able to meet her goals around reduction of checking behaviours and health related anxiety. Lily’s personal goals for therapy were to cease repeatedly checking her cervix for signs of cancer and to ‘get her life back’ - which would involve going to a local art group, taking frequent walks, feeling able to holiday abroad, and no longer ruminating on death. These were deemed to be partially met at the conclusion of the intervention, as she had significantly reduced her checking, increased her activities outside the home, accepted a referral for social prescribing and ceased to require crisis care.
Lily reported two specific parts of this intervention as helpful - first was the use of imagery rescripting. Rescripting intrusive imagery is a technique typically used as part of gold standard treatment for social anxiety, however it has also shown good results as a single session intervention for IAD, where the presence of illness-related imagery is well established (Arntz, 2012; Benke et al., 2024; Muse et al., 2010; Nilsson et al., 2019; Wells & Hackmann, 1993). There is evidence that autistic people may have greater ability to maintain mental images, think more visually in daily life, and benefit from visualisation in therapy (Bled et al., 2021, 2024; Ekman & Hiltunen, 2015). Further exploration of imagery rescripting for autistic people with IAD could therefore be valuable.
The second element Lily valued was the involvement of her parents. For psychological therapists delivering interventions to autistic adults, successfully integrating family members can be considered challenging, with concerns about differing goals or therapy interference (Riches et al., 2023). Parental reassurance seeking formed a significant component of Lily’s formulation, correlating with findings that those with IAD primarily seek reassurance rather than support from loved ones (Halldorsson & Salkovskis, 2017). Techniques which promote a shift between reassurance and support fit well within Theory A/B models of working with IAD, and appeared to have a notable impact on Lily’s experience, aligning with the reported benefits of family involvement (Ainsworth et al., 2020). Further parental involvement may have been helpful, but was not possible, with the fortunate exception of the final session, which helped assuage concerns about generalising techniques post-therapeutically (Mazurek et al., 2023).
Recommendations to Clinicians and Students
This case study indicates that cognitive behavioural therapy for IAD can be effective for autistic adults with illness anxiety disorder, but its delivery requires careful consideration of contributing systemic factors, and an understanding of how autistic traits can impact both formulation and intervention in this population. Whilst this work can and should be done in generic mental health settings, seeking supervision or consultation from clinicians working in neurodiversity services can aid in delivering effective care and implementing the recommendations below.
Clinicians working with autistic individuals who experience IAD should attend to the influence of autism-specific factors such as sensory difference, routines and rigidity of thought on the maintenance of distress, and ensure these processes are well integrated within psychological formulations, including the vicious flower model. In practice, this includes routinely assessing how intolerance of uncertainty, sensory sensitivities, and cognitive rigidity may influence reassurance seeking, checking, and avoidance behaviours.
Introducing structured visual tools including visual formulations and predictable session agendas may further support engagement for autistic adults who benefit from concrete and visually anchored information. Within this, practitioners should consider the therapeutic value of creatively incorporating an autistic individual’s area of special interest, as grounding strategies or motivational tools to optimise engagement.
Thoughtful involvement of family members or key supporters can also be valuable. Collaborative development and sharing of individual and systemic formulations is recommended, particularly with regard to identifying the maintenance cycles of reassurance-seeking. Providing support for systems around the individual to shift their own behaviours from reassurance to emotion-focused support can reduce inadvertent maintenance of anxiety and facilitate change for those struggling with IAD. Where possible clinicians should offer structured guidance to family members, and potentially to wider healthcare networks, to help ensure consistent responses to reassurance seeking outside sessions.
Clinical attention and research are warranted regarding the presentation of illness anxiety disorder in autistic adults, to better develop understanding of the role autistic traits may play in the development and maintenance of IAD and increase the evidence base for intervention when working with autistic people.
Further practice-based evidence and research around the potential value of imagery-focused approaches for autistic people in the application of CBT for IAD is needed. Imagery rescripting may be particularly useful where conventional cognitive techniques prove less accessible, and may leverage visual thinking strengths in this population. To support effective evaluation of this and other clinical work with IAD in autistic adults, further research should also evaluate which outcome measures are acceptable and valid for this population, given potential limitations of existing instruments. Systematic investigation is needed to refine these adaptations, identify active therapeutic components, and develop clearer guidance for clinicians working at the intersection of IAD and autism.
Footnotes
Acknowledgements
Dr Cathy Randall-Phillips, University of Bath & Avon and Wiltshire NHS Foundation Trust.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Informed, written consent was gained for the writing and publication of this case study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analysed during this case report are included in this published article.