
Abstract
This case study summarizes the assessment and treatment of a nine-year-old girl, Layla, with separation anxiety and school refusal. The initial assessment indicated that challenging behavior served both to access and avoid stimuli from the environment, rather than to escape or avoid an aversive stimulus. Treatment consisted of teaching and then differentially reinforcing the use of appropriate behaviors that serve the same function as the challenging behaviors for which the family was seeking treatment. These strategies included functional communication training and differential reinforcement of other and alternative behaviors using a cumulative duration schedule of reinforcement and a habituation paradigm. The treatment was successful in reducing school refusal and increasing compliance with adult directions. We discuss treatment- and assessment-related recommendations for clinicians and students.
Theoretical and Research Basis for Treatment
Parental accommodation (i.e., the ways in which family members modify their behavior in an effort to lessen or avoid distress; Phillips et al., 2020) was originally investigated in adults suffering from Obsessive Compulsive Disorder (Calvocoressi et al., 1995) but has since been found in many families of children and adolescents with an anxiety disorder (Kagan et al., 2017). Accommodation can include facilitating avoidance, providing items that reduce anxiety, adhering to rigid child-determined rules around anxiety provoking stimuli, providing excessive reassurance, or modifying the family routine to reduce anxiety (Johnco et al., 2022). Parental accommodation is most prevalent in youth with a primary diagnosis of separation anxiety (Phillips et al., 2020). Although intended to improve distress caused by anxiety, accommodation has been linked to increased anxiety symptom severity, functional impairment, and caregiver burden (Phillips et al., 2020). Indeed, instead of allowing the child to have corrective experiences to either realize the anxiety provoking outcome is unlikely to occur or that they can cope when it does, parental accommodation provides short term relief of anxiety but maintains anxious behaviors long term by modeling avoidance (Strohmeier et al., 2020). Parental accommodation is also associated with poorer treatment response (Salloum et al., 2018).
Behaviorally, parental accommodation operates through a mutually reinforcing negative reinforcement cycle. Accommodation allows children to avoid aversive situations, temporarily reducing their anxiety and increasing future expectations of accommodation. Simultaneously, caregivers experience immediate relief from distress when their child is calm, making them more likely to accommodate avoidance again. Similarly, anxiety disorders stem from respondent and operant conditioning (Thyer & Sowers-Hoag, 1988). For instance, in separation anxiety, previously neutral situations (separation) become paired with life stressors, evoking anxiety alone (respondent). Avoidance or escape behaviors are then maintained because they successfully reduce that anxiety (operant).
More broadly, separation anxiety is characterized by developmentally inappropriate or excessive fear or anxiety concerning separation from an attachment figure (e.g., caregiver) expressed through three or more symptoms (e.g., recurrent excessive distress when anticipating or experiencing separation, persistent and excessive worry about losing major attachment figures, persistent reluctance or refusal to sleep away from home or go to sleep without being near a major attachment figure) (American Psychiatric Association [APA], 2013). This fear must persist for at least four weeks in children and adolescents. Separation anxiety is most prevalent in children under 12 years old; the 6–12-month prevalence is approximately 4%. It often develops after a life stressor, such as a loss, and may include worry about specific dangers to parents or caregivers (APA, 2013). Traumatic events (e.g., domestic violence) can precede separation anxiety (Socolar, 2000), which often fluctuates in severity and can persist into adulthood. Associated behaviors include aggression during separations and school refusal. This refusal creates problematic attendance and emotional distress, ultimately impairing academic achievement and social adjustment (Maynard et al., 2018), which may warrant therapeutic intervention.
Behavior therapy relies on identifying environmental variables that evoke and maintain challenging behavior to inform an individualized, function-based treatment plan. As children display similar behaviors during separations for different reasons, such as escaping separation or gaining caregiver compliance, a data-based understanding of the specific function is critical for effective intervention. Exposures (i.e., real or imaginal confrontation with an anxiety provoking stimulus in a controlled environment) have been noted as an especially important mediator of anxiety treatment, particularly when implemented in close succession and multiple contexts to optimize inhibitory learning (Mohr & Schneider, 2014). Exposure therapy is effective for behaviors maintained by escape from an aversive context because it involves confronting an anxiety provoking stimuli and preventing escape or avoidance until distress reduces (Bouchard et al., 2004). Behaviorally, the escape or avoidance behavior is put on extinction (i.e., prevented from contacting reinforcement) until the anxiety provoking stimulus no longer evokes an anxiety response and other more appropriate behaviors are reinforced instead. Family involvement in treatment, especially when caregivers play an integral role in the maintenance of anxiety, is often recommended (Ehrenreich et al., 2008). Exposures are also an important technique for behavioral approaches to school refusal, hypothesizing that a quick return to attendance prevents reinforcement through avoidance (Maynard et al., 2018).
Importantly, not all separation-related challenging behavior may be maintained by escape. Challenging behavior at separation may also serve as precurrent behavior (i.e., a behavior that increases the likelihood of a subsequent behavior obtaining reinforcement) by increasing the effectiveness of requests made to caregivers (Edelstein et al., 2025). For example, a child’s use of precurrent disruptive behavior following the announcement of a separation may result in caregivers allowing the child to dictate parameters of the separation. This pattern may generalize over time, such that the child may begin to expect that all requests will be honored (i.e., their reinforcer is choice and control over the environment), and caregivers may become distressed when they are unable to accommodate their children’s increasingly complex requests (Edelstein et al., 2025). Therefore, rather than only negative reinforcement through escape, the mechanism of their challenging behavior may be multiply maintained by social negative (e.g., avoidance) and social positive (i.e., access) reinforcement.
Recently published research suggests that requiring engagement in a task for a fixed duration of time (i.e., a cumulative schedule of reinforcement) may be an effective means to promote habituation (Edelstein et al., 2025). A cumulative duration schedule involves providing reinforcement after a duration of appropriate responding (Mellott & Ardoin, 2023); for example, a parent may allow a child to end a chore they have persisted at for 5 minutes. During the cumulative duration, children are systematically habituated to complying with others’ preferences in play and work contexts (Edelstein et al., 2025). The duration of abiding by others’ preferences is gradually increased and is reinforced by intervals when others comply with their preferences, within reason (see Edelstein et al., 2025 for an example). Although both employ a habitation paradigm, exposures continue until internal, subjective criteria have been met (e.g., anxiety has decreased) and cumulative duration schedules continue until an objective, behavioral criteria have been met (e.g., appropriately tolerating another’s preferences for a given period of time).
For this case study, we utilized a behavioral approach by first conducting a functional assessment to identify the drivers of challenging behaviors. We then implemented an idiographic, function-based treatment program to reduce these behaviors and increase functionally equivalent, appropriate alternatives. This approach prioritized addressing major functional impairments over standard separation anxiety diagnostic criteria. By assessing behavior through both contrived and natural means, we avoided assuming a single function (like escape), addressing a gap in the literature and highlighting the value of comprehensive functional assessments in outpatient treatment plans.
Case Introduction
Layla Hunter (pseudonym), an 8-year-old third grader with age-appropriate functioning, lived with her mother and three sisters. The local Emergency Department referred her for treatment due to school refusal, elopement, suicidal ideation, and physical aggression. Her diagnoses included separation anxiety, school avoidance, and a trauma and stressor-related disorder linked to undisclosed levels of domestic violence exposure. Layla took daily psychiatric medication for dysregulation. Treatment was provided by a first-year post-doctoral fellow specializing in behavioral and cognitive-behavioral therapy, supervised by a licensed psychologist experienced in internalizing and externalizing behaviors.
All assessment and treatment appointments were conducted in treatments rooms (approximately 5 m × 5 m) at an outpatient clinic for challenging behavior. The treatment rooms were equipped with a one-way observation window and audio-video recording capabilities. Each appointment lasted approximately 2 hours. Treatment appointments were scheduled twice a week for five weeks; at the family’s request, one appointment was rescheduled to the sixth week.
Presenting Complaints
Layla’s mother, Ms. Hunter, reported that during separations, Layla engaged in disruptive behaviors (e.g., crying, yelling, hitting, and eloping) and refused safety instructions. These behaviors escalated in third grade, driven by Layla’s worry that her mother would be injured. Transitions to school or her mother going to work typically triggered these episodes. While Layla usually remained calm once inside school, transitioning to a virtual setting led to similar disruptive behavior during online classes. To appease her, Ms. Hunter promised not to work alone at the office. Layla tolerated short errands when left with preferred relatives. The treatment team initially hypothesized that her challenging behavior was maintained by escape from aversive stimuli or demands.
History
Layla met all developmental milestones and performed at grade level without accommodations. She had no mental health concerns until late second grade, when an alleged domestic violence incident left Ms. Hunter severely injured. Following this, Layla first refused school by eloping from her home; she was allowed to stay home, and the local crisis center recommended outpatient therapy. That summer, an art therapist diagnosed her with separation anxiety, a trauma and stressor-related disorder, and school avoidance. In third grade, Layla refused school twice by eloping to the parking lot and making suicidal statements, resulting in same-day crisis center evaluations and discharges. A third elopement into the road outside the school prompted emergency services involvement. Ms. Hunter then took Layla to a pediatric Emergency Department. Consequently, Layla was placed on a virtual Home & Hospital education plan for 6 hours of weekly instruction. Over the next two months, she intermittently attended a partial hospitalization program (PHP), which implemented token economies to reinforce “brave behavior” and prescribed 25 mg of Sertraline and 1 mg of Guanfacine daily to address her dysregulation. The family reported that both the token economy outside the PHP and the medication had mixed results (e.g., Layla did not always seem interested in earning the offered prizes, the family did not routinely implement the procedures).
Assessment
The initial clinical evaluation consisted of a semi-structured functional interview completed by Ms. Hunter, parent report measures, and direct observation of Layla and Ms. Hunter in contrived and natural contexts. Ms. Hunter consented to all assessment and treatment procedures, and Layla provided her assent.
Semi Structured Functional Interview
Ms. Hunter completed a semi-structured interview aimed at identifying, operationally defining, and understanding contexts in which Layla’s challenging behavior occurred (Edelstein et al., 2023). Layla was invited to participate and share her perspective; she primarily chose to allow her mother to speak on her behalf. Ms. Hunter identified Layla’s target behavior as emotional dysregulation and defined it to include elements of physical aggression (i.e., hitting, kicking, pulling on clothing) as well as noncompliance (i.e., vocal or verbal refusal, ignoring an adult directive), elopement, and tantrums (i.e., yelling, crying, name calling, threats directed at others). Contexts likely to occasion challenging behavior included perceived imminent separation from her mother (e.g., school drop off, doctor’s appointments) and completion of school related tasks. Removing the perceived separation or compliance with Layla’s requests (e.g., not to go to school) were identified as likely to reinforce the target behavior.
Functional Assessment and Direct Observations
Informed by the interview with Ms. Hunter, a functional assessment was conducted to examine possible environmental determinants of the target behavior using functional analysis methodology (Iwata et al., 1994). Escape and request compliance conditions were employed. Although testing only escape and request compliance conditions does not rule out the possibility that other functions contributed to the behavior, these were determined to be the most salient conditions for the assessment based on the functional interview. Efficiency in assessment was emphasized given the brief format of a treatment course (i.e., 20 hours). Data were collected via paper and pencil using a frequency count and latency to target behavior.
To test the escape function, the clinician and Ms. Hunter covertly arranged four trial separations. Each trial lasted until Layla exhibited the target behavior or 5 minutes elapsed. Trials began when Ms. Hunter announced her intention to leave. If Layla displayed the target behavior, Ms. Hunter immediately stayed or returned, whereas appropriate requests were ignored. The clinician guided Ms. Hunter using written instructions and a bug-in-the-ear device, while deceptively telling Layla she was doing paperwork nearby. Instead, the clinician observed via a one-way mirror. To compare responses to known versus unknown separation lengths, Ms. Hunter left without specifying a timeframe in two trials and specified a five-minute absence in the other two. Five-minute intervals between trials, featuring toys and Ms. Hunter’s presence, served as control conditions. Unexpectedly, Layla calmly tolerated her mother’s departures (see Figure 1, trials 1-4). Behavior During In-Clinic Practice Trials.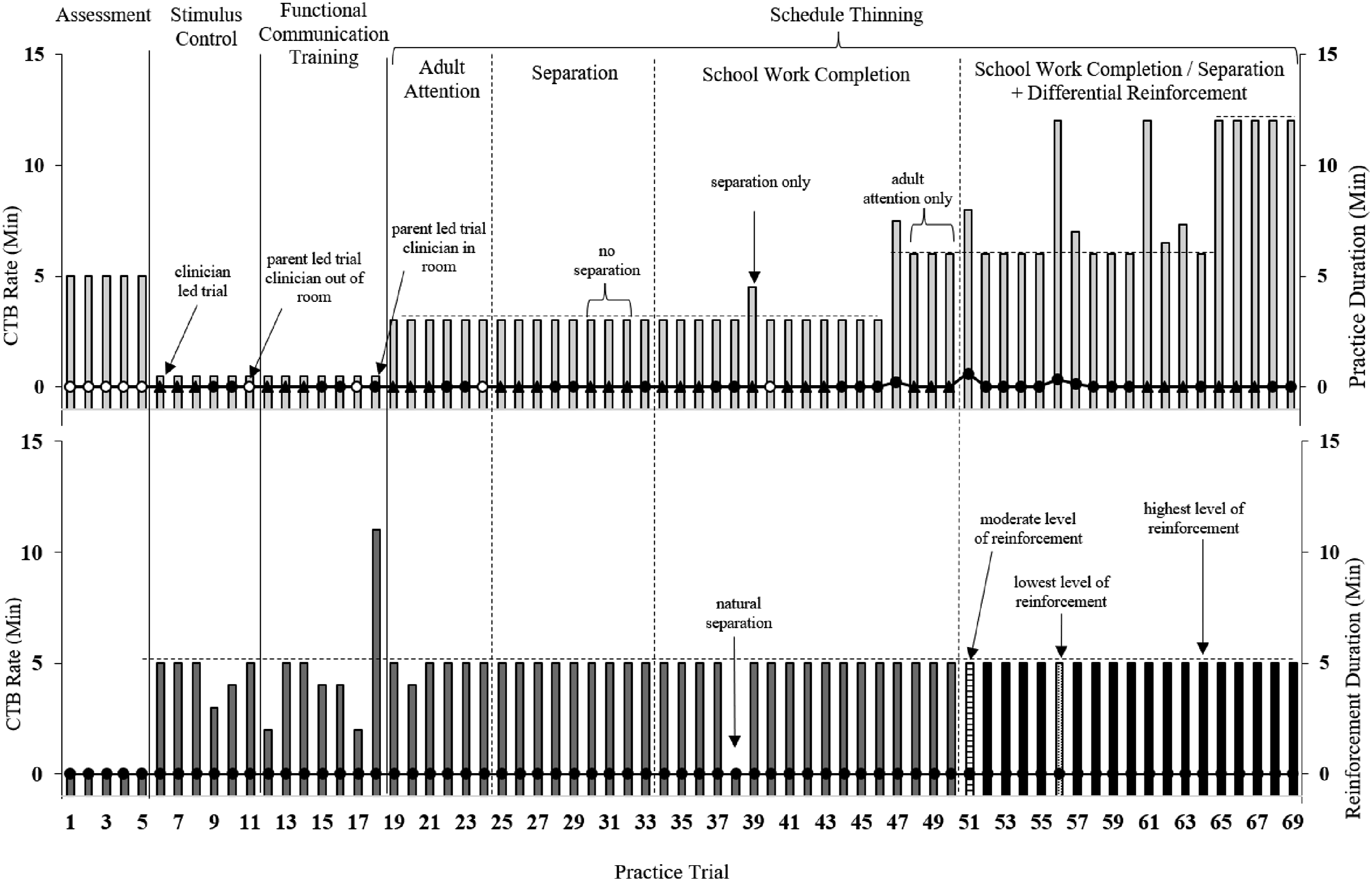
To test the request compliance function, the clinician used a choice/control-based functional analysis (Edelstein et al., 2025). Ms. Hunter repeatedly interrupted Layla’s preferred toy play by directing the interaction. If Layla displayed challenging behaviors, Ms. Hunter immediately yielded control, returning to Layla’s preferences for 30 seconds before interrupting again. Appropriate requests were ignored throughout the five-minute trial. Ultimately, Ms. Hunter issued nine interruptions, but Layla responded playfully rather than demonstrating any disruptive behavior (see Figure 1, trial 5). Ms. Hunter reported that her daughter’s behavior was typical of behavior at home when schoolwork was not involved.
Beyond contrived observations, clinicians directly observed Layla’s target behaviors during clinic transitions (e.g., checking in or moving from the waiting to the treatment room). Observed during intake and appointments 1, 7, 9, and 10, transition times ranged from 6 to 28 minutes due to aggression, noncompliance, elopement, and tantrums (see Figure 2). When denied requests to leave, Layla initially chose to transition independently but required physical assistance from staff during the final two sessions. Occasionally, Layla made idiosyncratic requests (e.g., texting someone) after exhibiting target behavior; complying with these requests correlated with an immediate reduction in challenging behaviors. Transition Time into Appointment.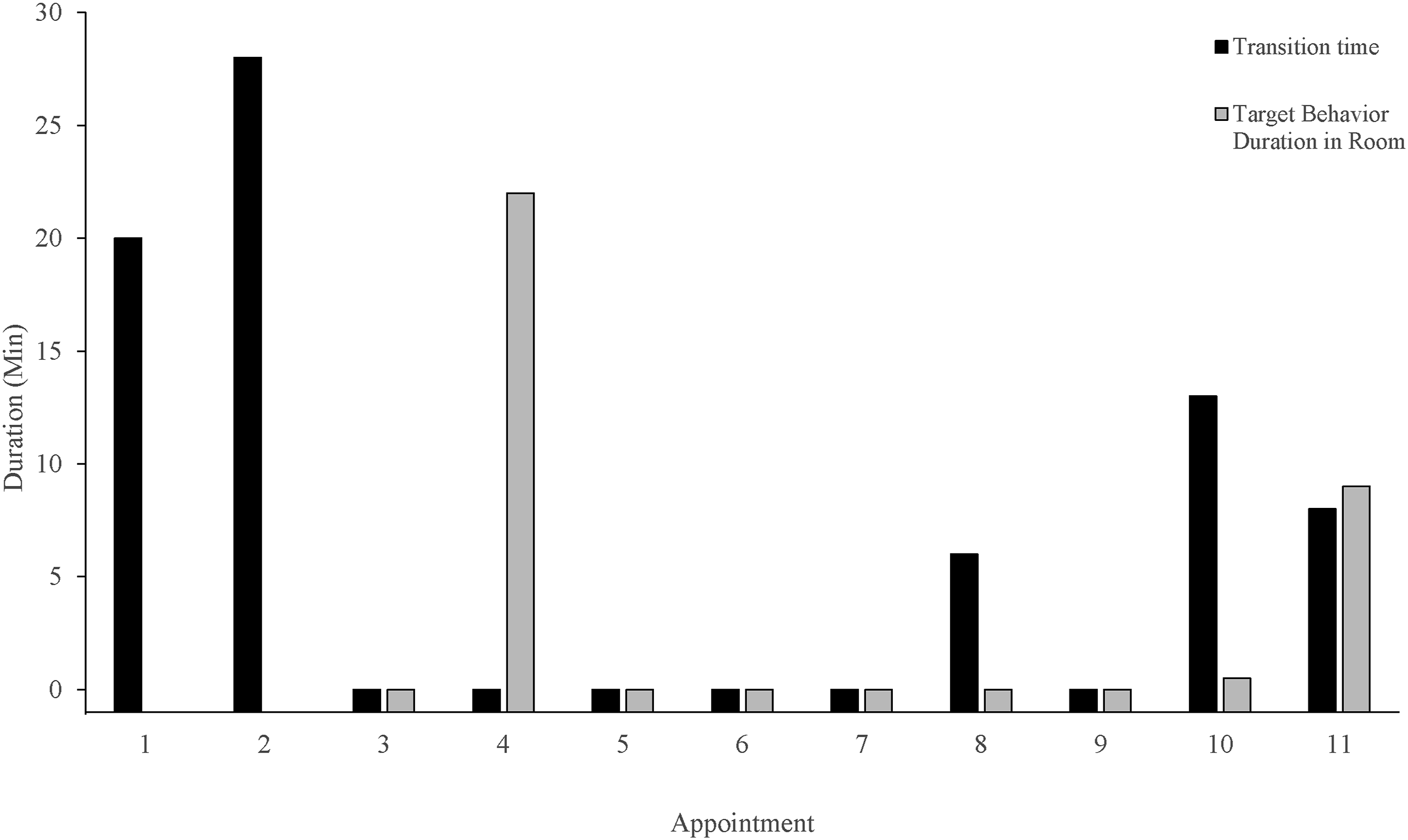
Parent Report Measures
Parent Report Measures
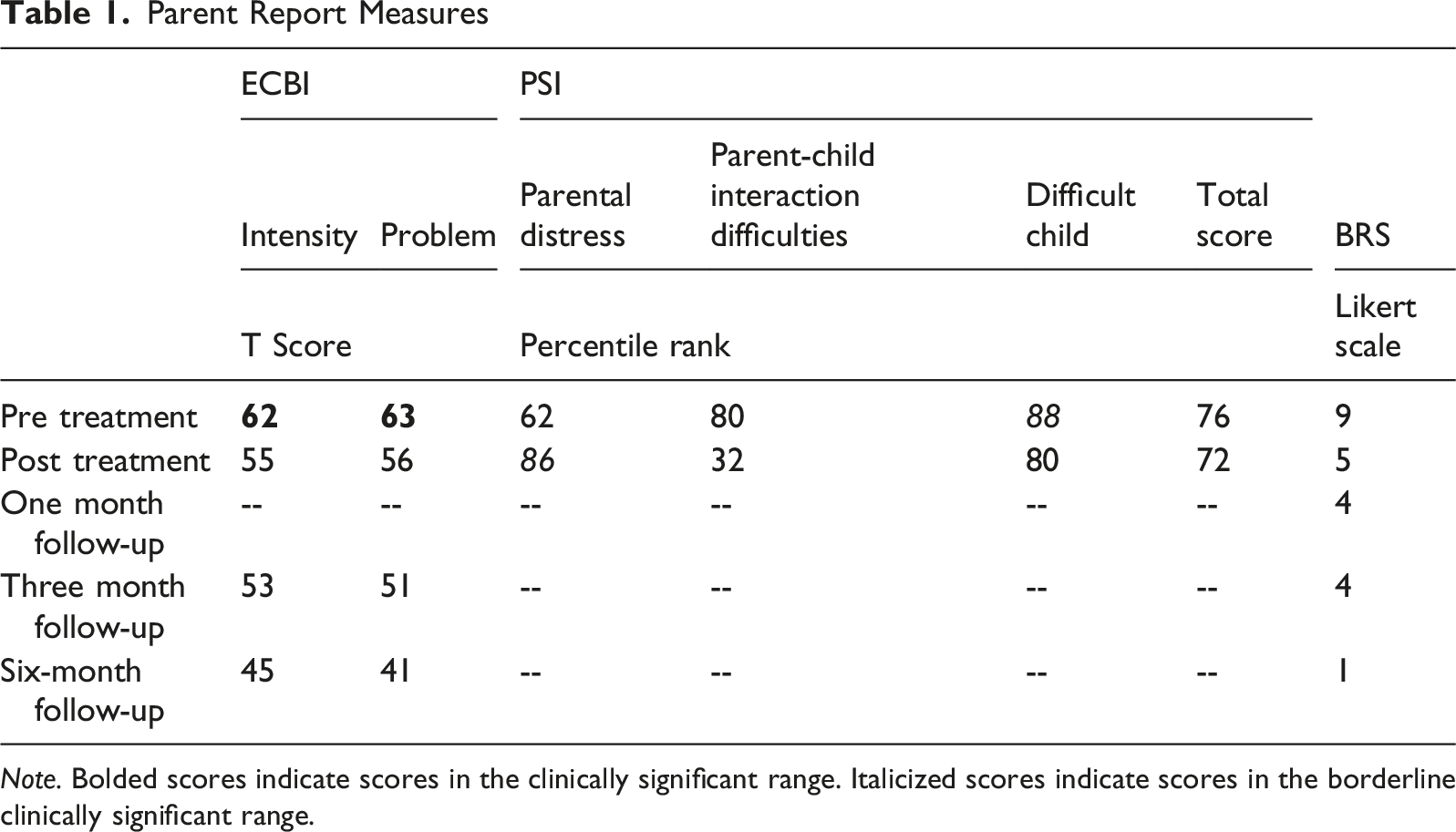
Note. Bolded scores indicate scores in the clinically significant range. Italicized scores indicate scores in the borderline clinically significant range.
Ms. Hunter also completed the Parenting Stress Index-Short Form Fourth Edition (PSI-SF) before the initiation of and at the end of treatment (Abidin, 1990). This questionnaire measures the degree of stress parents experience in the parent-child relationship and in their role as parents. It yields a Total Stress score and three subscale scores: Parental Distress, Parent-Child Dysfunctional Interaction, and Difficult Child. The test–retest and internal consistency reliability ranges from 0.68 to 0.84 (Abidin, 1990). Ms. Hunter’s pretreatment Difficult Child score was in the borderline clinical range; her other pretreatment scores were average (see Table 1).
Finally, Ms. Hunter provided a Behavior Rating Scale (BRS) rating at each appointment indicating the degree of impairment the target behavior had on Layla’s daily functioning (Edelstein et al., 2025). This subjective rating scale ranges from 0-10, with 0 representing no impairment, 1-3 representing minimal impairment, 4-7 representing moderate impairment, and 8-10 representing severe impairment. Ms. Hunter’s pretreatment score was in the severe range (see Table 1).
Case Conceptualization
Layla demonstrated no challenging behavior during the contrived direct observation conditions in clinic and, as a result, no differentiation between test and control assessment conditions. A lack of differentiation would typically make a functional interpretation of the data impossible. However, naturalistic observations related to appointment attendance suggested that the presentation of non-preferred demands acted as a trigger of the target behavior. Ms. Hunter did not allow escape or avoidance of the therapy appointments, but she strongly suspected that escape from an appointment would have reinforced the target behavior. When avoidance could not be achieved, Ms. Hunter accommodated Layla’s challenging behavior by ceding control; for example, allowing her to dictate the terms of separation (e.g., requiring mid-separation check-ins). Therefore, it was hypothesized that Layla’s target behavior was maintained via negative reinforcement by avoiding non-preferred situations and/or positive reinforcement of complying with Layla’s specific requests. Adult accommodation of the escape-maintained and/or precurrent behaviors was also hypothesized to play a prominent role.
Layla’s greatest functional impairment was related to failure to access her education and her deteriorating relationship with her mother. At the time of the intake, she had not attended school in-person in two months and her participation in the virtual Home & Hospital education plan was intermittent. By engaging in target behavior, Layla was often able to avoid schoolwork. Teachers were inadvertently complicit in this reinforcement-cycle; they were scheduled for 6 hours each week and could not extend their time if Layla refused to initiate the school meeting or complete work tasks during the assigned time. Thus, as a result of her failure to engage with school tasks, Layla was sometimes able to escape them entirely. Similarly, Ms. Hunter’s efforts to ameliorate distress led to a decreased number of demands, poor follow through with stated expectations and acquiescing to Layla’s requests in the midst of challenging behavior. Ms. Hunter also had few strategies for handling Layla’s distress and often attempted to verbally soothe her or offer assurances, even while being the target of physical aggression and threats. These experiences served to maintain the cycle of challenging behavior and parental accommodation.
Overall, although certain aspects of Layla’s presentation were consistent with a separation anxiety diagnosis (e.g., worries about terrible things happening to the caregiver), there were also aspects of her presentation that were atypical (e.g., noncompliance with non-separation adult directives). However, results of the assessment (i.e., direct observation, functional assessment, and parent report) suggested that all of Layla’s functionally impairing behavior was maintained by the same underlying mechanism: negative reinforcement. More specifically, the precurrent behaviors occur before a target behavior to increase its effectiveness or likelihood of reinforcement. As such, they can serve multiple operant functions and are often shaped by context. Layla’s precurrent behaviors served to ensure demands made to prevent or lessen the aversiveness of separation were followed, thus resulting in negative reinforcement. In fact, Layla’s challenging behavior appeared to be overgeneralized; that is, her target behavior was maintained by escape from any non-preferred demand rather than separation only. When Layla determined that escape was unavailable, precurrent behavior led to gaining choice/control over some aspects of the inescapable situation. Thus, while the previous separation anxiety diagnosis highlighted the maintenance of challenging behavior through negative reinforcement, the broader clinical picture warranted a treatment approach beyond the specificity of separations. In other words, Layla’s separation anxiety diagnosis was contextual but not essential to the developed treatment plan. The broader focus led to treatment of target behavior across all contexts in which it was evoked and included elements of differential reinforcement of alternative and other behaviors.
Course of Treatment and Assessment of Progress
Treatment was initiated to address the hypothesized mechanisms maintaining Layla’s challenging behavior. The primary goal of treatment was to return Layla to full-time, in-person school. The school proposed an attempt to return to school prior to the final treatment appointment. Additionally, there were secondary goals related to increasing Layla’s compliance with adult directives and reducing Ms. Hunter’s accommodation of target behaviors. All appointments were co-attended by Layla and Ms. Hunter. Ms. Hunter was identified as the change agent with the treating clinician in the role of teacher and coach. Using Ms. Hunter as the change agent increased the ecological validity of treatment and promoted generalization of skills outside of the clinic context.
Following the initial two-hour intake session, Layla and her mother participated in ten two-hour appointments in the clinic over the course of six weeks. These appointments were video recorded for data collection purposes. Virtual follow-up appointments were offered one month, three months, and six months later and were conducted over HIPAA compliant web-conferencing software. A single school consultation meeting was conducted over web-conference software between the ninth and 10th treatment appointments.
Each appointment was structured so that there were four to seventeen practice trials (m = 8.13, SD = 4.02) for Ms. Hunter and Layla to demonstrate learned skills in relevant contexts. The number of practice trials varied depending upon the length of the practice trial (range: 0.25 to 12 minutes) and whether target behavior occurred during the session. Practice trials alternated with periods of reinforcement, such that Layla earned a timed free choice activity following successful completion of the adult-directed practice trials. Details on practice activities are listed below. As additional skills were taught, the free choice activities were differentially offered based on how Layla completed the adult-directed practice trial. For example, completion of a practice trial with no target behavior earned the highest level of choice whereas completion with the presence of target behavior earned lower levels of choice. Bug-in-ear coaching was not provided during any of the treatment trials.
Using paper and pencil, the clinician recorded data on the frequency of target behavior during each practice trial, duration of each practice trial, activity completed during practice trials, duration of time in reinforcement, and the duration of target behavior during transitions into the clinic. As it became relevant, the clinician also tracked the differential outcomes earned for Layla’s reinforcement intervals. These data were compared across trials and appointments to assess behavioral outcomes. Specifically, rates of target behavior during practice trials were used to determine when to increase the response effort for Layla. As data on school attendance was not possible (Layla was not attending in person school at the time of treatment) and could not be replicated in session, data on the secondary goals were used as proxies for the primary goal. This substitution was deemed reasonable given that Layla would need to follow non-preferred adult directives and Ms. Hunter would need to stop accommodating challenging behavior in order for school attendance to be achieved. Following each appointment, Ms. Hunter was assigned home practice activities to assist with generalization of skills in the home context. Of note, the treatment course recommendations did not alter pre-existing token economies for reinforcing “brave behavior” (e.g., sleeping alone) set up by the PHP.
Establishing Stimulus Control
The clinician introduced the concept of “Adult’s Way/Layla’s Way,” such that sometimes during sessions it would be “Layla’s Way” when they could do and talk about things that she wanted to do/talk about, and at other times it would be “Adult’s Way” (Edelstein et al., 2025). “Layla’s Way” and “Adult’s Way” were signaled via a visual stimulus card. The card was used to create clear expectations around when Layla would be able to access social positive and social negative reinforcement in her environment, provided she remained engaged in appropriate behavior. Appropriate behavior was defined as following the clinic rules. The rules were vocally introduced to Layla (e.g., “My rules for clinic are that kids have a calm body, hands to self, and a quiet voice. When they do these things, fun things can be available.”). A visual aid depicting the rules was placed prominently in the room. If at any time target behaviors were observed, it automatically became “Adult’s Way,” and fun activities ceased, until Layla demonstrated the clinic rules again. Additionally, discrete stimulus control trials were conducted by the clinician and Ms. Hunter.
For the six discrete stimulus control trials, reinforcement was provided at a 1:1 fixed ratio schedule. The trial began when the clinician or Ms. Hunter announced that it would be “Adult’s Way,” flipped the visual stimulus card, and paused previous activities. When Layla appropriately disengaged from the previous activity and demonstrated the rules, the adults immediately provided a brief praise statement for remaining calm, flipped the stimulus card to indicate it was “Layla’s Way,” and provided 5 minutes of reinforcement according to Layla’s preferences (e.g., playing board games). The clinician modeled the first three trials, then Ms. Hunter conducted the next two trials with the clinician in the room providing direct coaching and feedback. The final trial was conducted by Ms. Hunter with the clinician observing from the observation room. Layla engaged in no challenging behavior during stimulus control trials (see Figure 1, trials 6-11).
Functional Communication Training for Access to Reinforcement
The clinician conducted functional communication training (FCT) to teach Layla to request access to social positive and social negative reinforcement in her environment. Layla’s functional communication response (FCR; i.e., “my way”) was paired with the previously established “Adult’s Way/Layla’s Way” visual stimulus card. The modified version of functional communication training (Carr & Durand, 1985) reinforced appropriate ways to indicate wants and needs, replacing challenging behavior with an adaptive, low effort response. In the case of Layla, the objective of functional communication training was to replace impairing and unsafe target behavior with an efficient communication tool. A request for “Layla’s Way” was hypothesized to be the most appropriate communication response as sometimes Layla desired an end to or break from an adult directive (i.e., negative reinforcement, separation) and sometimes she desired that specific requests be honored (i.e., positive reinforcement, access).
Reinforcement was provided at a 1:1 fixed ratio schedule. For the six FCT trials, the trial began when the clinician or Ms. Hunter announced that it would be “Adult’s Way,” flipped the visual stimulus card, and paused previous activities. When Layla appropriately used her FCR, the adults immediately provided a brief praise statement for the appropriate request, flipped the stimulus card to indicate it was “Layla’s Way,” and provided 5 minutes of reinforcement according to Layla’s preferences. As before, the clinician modeled the first three trials, then Ms. Hunter conducted the next three trials with the clinician out of the room for the final trial. Layla engaged in no challenging behavior during FCT trials (see Figure 1, trials 12-18).
Schedule Thinning
Following successful demonstration of replacement behaviors, the clinician implemented a schedule thinning procedure based on a cumulative duration schedule. This built tolerance for delayed reinforcement, making appropriate behaviors more applicable to real-world settings. Reinforcement intervals (“Layla’s Way”) remained at 5 minutes, while work intervals (“Adult’s Way”) systematically increased, starting at 3 minutes. To begin “Adult’s Way,” a clinician or Ms. Hunter announced the transition, flipped a visual stimulus card, and paused current activities. If Layla used her functional communication response (FCR), she was instructed to wait or complete a task monitored by a visual timer. Successful completion yielded praise, a card flip back to “Layla’s Way,” and 5 minutes of reinforcement. Challenging behaviors paused the timer. Each criterion required three successful trials with both the clinician and Ms. Hunter before escalating demand difficulty or duration.
During the first six trials of the cumulative duration schedule of reinforcement, Layla was provided access to toys and told she could play independently while the clinician and her mother completed psychoeducation. Psychoeducation lasted 3 minutes. The clinician led the first three trials, then Ms. Hunter led the next three. Layla demonstrated no challenging behaviors, and the timer was never paused (see Figure 1, trials 19-24).
The next series of trials were separation trials. Ms. Hunter was instructed to leave the room for the duration of “Adult’s Way.” Ms. Hunter and the clinician collaboratively determined that the clinician should remain in the room and be available as Layla was never left entirely alone at home or school. Toys were also available. The clinician never initiated play during separations but would comply with Layla’s appropriate requests. Separations lasted 3 minutes. The clinician led the first three trials, then Ms. Hunter led two trials. The next three trials were led by the clinician and did not include separation in order to allow for additional psychoeducation to Ms. Hunter about the next steps in treatment (see Figure 1, trials 30-32). Ms. Hunter then led the final separation trial. Layla demonstrated no challenging behaviors, and the timer was never paused (see Figure 1, trials 25-33). Separation trials were deemed necessary as separations were required for the ultimate goal of returning to school.
The third series of trials were related to schoolwork completion. Layla was instructed to complete both preferred and less preferred school related tasks for a specific period of time. The clinician and Ms. Hunter were available to assist or correct the work as needed. Schoolwork completion lasted 3 minutes. The timer began when Layla initiated schoolwork. The clinician and Ms. Hunter each led three trials for the preferred and the lesser preferred tasks. Layla demonstrated no challenging behavior, and the timer was never paused (see Figure 1, trials 35-46). School work completion trials were deemed an approximation of attending school and thus related to the ultimate goal of treatment. Following twelve schoolwork trials with no challenging behavior, Ms. Hunter increased the length of “Adult’s Way.” Layla demonstrated some passive noncompliance, delaying task initiation (see Figure 1, trial 47). This led to three trials (trials 48-50) without a schoolwork completion task for Layla, but during which the clinician and Ms. Hunter collaborated on ways to quicken task initiation. Finally, trial 39 did not include schoolwork but included a longer separation as Ms. Hunter had to step out of the treatment room. This was deemed a practice trial as it recreated a previous practice context.
Finally, the fourth series of trials combined the previous versions for a series of mixed separation and schoolwork trials; this mixed presentation was deemed the closest in clinic approximation to attending school. The clinician always remained in the room and available for help or corrective feedback. Additionally, the length of time for each trial was increased to six and then 12 minutes as mastery was demonstrated. The timer began when Layla initiated schoolwork. Ms. Hunter led the majority of the trials. Layla demonstrated occasional passive noncompliance (e.g., laying on the ground and refusing to initiate work), resulting in a delayed start to the work interval timer or a work interval timer pause (see Figure 1, trials 51-69).
Differential Reinforcement
As the final skill, the clinician taught Ms. Hunter how to implement a proactive contingency management system, such that Layla earned different levels of preferred items/activities during “Layla’s Way” based on her behavior during “Adult’s Way.” For safe, calm, and quick initiation of tasks, Layla earned the highest level of access. For disruptive behavior (e.g., whining) and/or mild delays in initiating tasks (i.e., 1-3 minutes to begin), Layla earned a moderate level of access – her most preferred activities were not available. For unsafe behavior (e.g., eloping, hitting) and/or long delays in initiating tasks (i.e., more than 3 minutes to begin), Layla earned low levels of access (i.e., only drawing or relaxing). The reinforcement system reset every “Adult’s Way” interval, such that Layla need only complete the next practice trial safely and calmly to earn back her most preferred reinforcers during “Layla’s Way.” This system was paired with the fourth series of trials. As noted above, minimal target behavior was observed during these practice trials, and Layla typically earned the highest level of reinforcement during “Layla’s Way” (see Figure 1, trials 51-69). The clinician and Ms. Hunter also discussed how this system could be generalized to school transitions outside of clinic.
Parent Training
Throughout treatment, Ms. Hunter was provided psychoeducation. During the first few appointments, psychoeducation focused on the functions of behavior and the role of antecedents and consequences in evoking and maintaining behavior. The clinician explained that a child may avoid separations for a variety of reasons and behavior change was most likely to occur if Layla was taught an appropriate replacement behavior that served the same function. Habituation and gradually building tolerance for non-preferred adult directives were also discussed as the rationale for the treatment procedure. These topics were juxtaposed with accommodation of child challenging behavior and the negative reinforcement cycles faced by the parents and children alike. The negative reinforcement cycles were emphasized as maintaining factors of challenging behavior. Ms. Hunter and the clinician completed exercises to help Ms. Hunter understand the level of accommodation she was providing and to allow her to make strategic choices about when to accommodate.
To strengthen Ms. Hunter’s ability to follow through with instructions, effective instruction delivery and contingency management were discussed. Providing brief, clear, statements was emphasized (e.g., sit in that chair, complete 6 math problems). Instructions were paired with contingencies, and the clinician explained how to use contingencies for spontaneous instructions that occurred throughout the day.
Differential attention, including minimally attending to aggressive and unsafe behaviors, was also discussed and practiced in sessions. Specifically, Ms. Hunter was encouraged to provide minimal attention (sufficient to maintain safety) during challenging behavior and to provide more opportunities for discussion and interaction when Layla was demonstrating safe behaviors.
Safety Planning
Due to Layla’s physical aggression, age and size, Ms. Hunter was provided with coaching and hands-on practice with behavior management strategies for blocking hits and kicks. She was also taught to create physical space during moments of physical aggression without compromising her ability to provide direct supervision. Ms. Hunter was encouraged to use these techniques at home since concerns with elopement prevented Ms. Hunter from fully separating when Layla engaged in physically aggressive behavior. Elopement also occurred during the transition into the appointment on two occasions. During the first elopement, Ms. Hunter pursued Layla, and they returned to the treatment space together and the appointment carried on with no further interruptions. During the second elopement, Layla required physical assistance from the clinician and supervising psychologists to enter the treatment space. Physical assistance was provided with the consent of Ms. Hunter. Ms. Hunter was also provided with the options of going home or going to the nearest pediatric Emergency Department. Ms. Hunter chose to continue the appointment in an effort to reduce the negative reinforcement of escaping the appointment. The clinician helped Ms. Hunter plan for elopement in the community. Hand holding whenever transitioning between spaces and wearing a GPS tracking device in case they were separated were specifically recommended.
Exposures
During the sixth appointment, in addition to continuing with schedule thinning, the clinician and Ms. Hunter began to discuss school-based exposures that could be completed. The goal was to habituate Layla to aspects of the school environment prior to full re-entry. All recommendations made by the clinician were qualified with the precaution that Ms. Hunter discuss exposures on school grounds with school personnel before completing them. Ms. Hunter brainstormed a few options that did not require school collaboration (e.g., driving by the school, parking in the school parking lot). Throughout the remaining appointments, Ms. Hunter coordinated with the school to complete school-based exposures that required entering the building (e.g., returning a library book). When exposures were completed, the “Adult’s Way” language was used. The family reported success with the school-based exposures. However, Layla shared that she did not like the amount of attention her visits garnered from the other students. The clinician advised Ms. Hunter to speak with the school about reducing the amount of attention Layla’s re-entry received.
School Consultation
Between the ninth and 10th appointments, the clinician virtually joined a school meeting to plan Layla’s school re-entry. Present at the meeting were Layla’s school counselor, lead teacher, assistant principal, special educator, and Ms. Hunter. The re-entry plan included an immediate reward in the morning for a safe transition into the school building (e.g., one-on-one time with a preferred school counselor) as well as clear contingencies for when the school would call crisis services (e.g., elopement, physical aggression directed at school personnel or peers). The team collaboratively determined who would provide supervision during all parts of the transition into the school building. Ms. Hunter stated a preference that, if Layla could not enter the school building safely and did not reach the behavioral threshold requiring crisis services, she and Layla be allowed to sit in the school parking lot together to prevent reinforcement through escape. The school team agreed to Ms. Hunter’s request.
Outcomes
Direct observation of the target behavior was based on Layla’s transitions into appointments and during practice trials. Transition time into appointments decreased during the first half of treatment from 20 minutes at intake to instantaneous transition by the seventh appointment (see Figure 2). However, challenging behavior during transitions resurged during three of the final four appointments. Physical assistance into session was provided by the clinician and an assisting licensed psychologist for the last two appointments. Even so, transition into session decreased from 20 minutes at intake to 8 minutes at the final appointment. During the last appointment, in addition to challenging behavior impeding the transition into session, Ms. Hunter managed challenging behavior in the treatment room for approximately 29 minutes. She correctly waited for compliance and then provided an agreed upon contingency. These steps demonstrated a decrease in parental accommodation of challenging behavior.
As reported above, occurrences of target behavior during practice trials were rare. The observed behaviors only ever reached mildly challenging levels (mostly passive noncompliance), indicating that Layla did well when she was given specific instructions with contingencies that were followed through on. For instance, Layla earned the highest level of reinforcement on approximately 90% of the final 19 practice trials. See Figure 1.
Results from Ms. Hunter’s endorsements on the four separate administrations of the ECBI are depicted in Table 1. At pre-treatment Ms. Hunter’s scores for the Intensity and Problem scales were both above the clinical cut off (T ≥60). By post treatment, the scores had dropped below the clinical cut off and they remained lower than the cutoff at the three-month and six-month follow-ups. These scores suggest that, according to Ms. Hunter, both the frequency of the behaviors and her perception of how challenging they were to manage decreased over the course of treatment and in the months following.
Similar reductions were observed in most of the PSI scores (see Table 1). Pre-treatment scores were higher than post-treatment scores for all scales except for Parental Distress. The largest reduction was in the Parent-Child Difficult Interaction subscale. Overall, the lower scores reflect reduced behavioral challenges and parenting stress, alongside improvements in the quality of parent-child interactions. The increase in Parental Distress suggests that Ms. Hunter reported a greater amount of stress due to personal factors affecting her parenting by the end of treatment. The clinician did not further probe Ms. Hunter’s reasons for this increase in stress.
Ms. Hunter’s subjective BRS score did not change until the final treatment appointment. She reported during treatment that the score was unlikely to change until Layla returned to school. Prior to the final appointment, Layla had attended one day of in person school and then two virtual school days due to inclement weather. Although there had been mild protesting, Layla was successful in transitioning into and remaining in school. As a result, Ms. Hunter reported that her BRS score had dropped (see Table 1). It dropped further as Layla demonstrated an increased tolerance of attending school. By the six-month follow-up, Layla had only missed school due to illness, although, per Ms. Hunter’s report, it sometimes took them 2 hours to transition into school. Each time, Ms. Hunter followed through with the expectation that Layla attend school. As a result, Ms. Hunter reported low BRS ratings at the follow-up appointments.
Complicating Factors
One complicating factor of the case was Layla’s continued exposure to the other individual allegedly involved in the domestic violence incident. Layla saw this individual most weekends, and Ms. Hunter noticed a pattern of increased challenging behavior in the days preceding and following visitation. While the impact of the contact on Layla’s treatment progress could not be empirically derived, it seemed reasonable that exposure to this individual was not insignificant. Although a clear pattern did not emerge, clinicians took into consideration the potential for contact to have influenced behavior during treatment appointments.
An additional complicating factor in the case was Layla’s elopement. It is not uncommon to recommend that parents physically separate from their children, when children are targeting them for physical aggression. However, because of Layla’s history of eloping from the home, the family was unable to create separation and provide the necessary supervision to prevent elopement. Ms. Hunter also expressed reluctance to separate from Layla during therapy appointments where separation and prevention of elopement could both be managed. Therefore, recommendations had to be tailored to maximize both Ms. Hunter’s and Layla’s safety.
Access and Barriers to Care
Layla attended 20 hours of treatment over the course of six weeks, a time-consuming and potentially costly investment for many families. Ms. Hunter’s employment situation permitted her a high degree of flexibility, allowing her to attend 4 hours of appointments per week. Additionally, once Layla returned to school, Ms. Hunter was able to follow through with school attendance expectations even on days when the transition into school took more than an hour. Some days she worked remotely from the school parking lot. This degree of flexibility may be atypical but facilitated success with the family’s goals. Additionally, although appointments were covered by insurance, Ms. Hunter expressed some financial hardship related to costs associated with clinic attendance (e.g., gas for a 30-45 minute commute). When offered information on financial support, she shared that they had already been connected with resources and declined further services. Although an upfront commitment, the condensed, high intensity treatment regimen helped the family efficiently maximize their treatment goals, ultimately reducing accrued costs over a prolonged period of time.
Just as there are barriers to families attending treatment, there may be barriers to clinicians offering the type of treatment provided to Layla and her family. The outpatient clinic was staffed with psychologists trained in behavior management strategies that allowed them to continue treating Layla despite the degree of her challenging behavior. Not every outpatient clinic may be equipped to handle the difficult transitions into appointments. However, Ms. Hunter’s ability to follow through with decisions to attend non-preferred appointments with staff assistance likely contributed to their positive outcomes. Similarly, the school coordination meeting was not a billable hour, and many clinicians may be unable to provide pro bono care coordination services. Coordinating the transition of treatment recommendations from the clinic to other relevant environments is an important direction for future treatment research.
Follow-Up
Follow-up appointments were held one, three, and six months after the final treatment appointment. The purpose of these visits was to collect behavioral data to monitor the effects of treatment and its maintenance.
At the one-month follow-up, Ms. Hunter reported that Layla had attended school every day except for once due to illness. Mondays and Fridays continued to be the hardest days for Layla to transition to school, but school personnel were following through with the differential reinforcement plan for safe entry into the school building. Ms. Hunter continued to provide substantial support during the transitions, staying with Layla in the parking lot until successful entry. She also worked remotely from the school parking lot or home (within a short drive of the school) most days instead of her office. Layla occasionally aggressed toward her mother during the transition, but it was milder and of shorter duration than what was witnessed in clinic. Ms. Hunter’s subjective rating of distress/impairment remained low (see Table 1). Ms. Hunter also expressed a desire to see Layla receive trauma services; the clinician provided referral recommendations.
At the three-month follow-up, Layla was on the waiting list of a trauma therapist recommended by the clinician. She continued to demonstrate success at transitioning into school. Some days, Ms. Hunter was able to enter the drop-off lane and Layla entered school without her mother’s assistance. Other days, Ms. Hunter parked in the parking lot and transitioned with Layla over the course of 15 minutes. There were occasional instances of elopement from the school building during the transition; Layla never left her mother’s line of vision and thus the safety plan necessitating crisis intervention services had not been activated. Ms. Hunter was working from home more frequently but had not made a full-time transition to working from home or the office yet. She stated this was a goal for the next school year. Ms. Hunter’s ECBI scores continued to trend downward and her BRS score demonstrated a 56% reduction from baseline and a 20% reduction since the end of the six-week treatment course (see Table 1). Additionally, Ms. Hunter shared that she had seen improvements in her own ability to handle Layla’s challenging behavior as a direct result of therapy.
At the six-month follow-up appointment, Layla remained on the waiting list for trauma therapy but reportedly was discussing her experiences with her individual art therapist. She had not missed a day of school for behavioral reasons, and Ms. Hunter continued to successfully use the drop-off lane in the morning. During summer vacation, which had commenced prior to this appointment, Ms. Hunter had returned to work in her office. Although Layla occasionally checked in with her mother via the phone during the day, there was no set check in schedule and Layla did not check in consistently. Moreover, there had been no aggression or elopement in the last two months; these objective behavioral markers were also noted in the subjective rating scales (see Table 1). In consultation with a psychiatrist, Layla had stopped taking the Sertraline and Guanfacine. The family retained a fast-acting medication for emergency use as needed. Ms. Hunter reported optimism for the next school year, including Layla expressed interest in riding the bus to school. The clinician and Ms. Hunter collaboratively determined to end follow-up appointments given the continued success.
Treatment Implications of the Case
This case study is an example of assessment and treatment of a nine-year-old girl using challenging behavior to gain social negative (e.g., preventing separation) or social positive (e.g., certain levels of attention during a separation) reinforcement. We began with a functional assessment that indicated her challenging behavior was maintained by escape from or avoidance of non-preferred situations or acquiescing to her demands when escape/avoidance were not possible. Challenging behavior occurred primarily when faced with non-preferred adult directions. Treatment was tailored to a multi-operant function by providing periods of time in which she could have access to social positive and social negative reinforcement, within reason, following cumulative periods of ceding control and following adult directives. Our treatment approach resulted in very low rates of challenging behavior during appointments, potentially suggesting that Layla was responsive to clear contingencies and found earning access to toys/activities and attention as well as a break from non-preferred instructions reinforcing.
The main clinical implication of this case report is that function-based treatment makes clinical care more precise and effective. Without considering the function of challenging behavior, clinicians may provide recommendations that are ineffective at best and inadvertently reinforcing at worst. While initial observations suggested that Layla’s challenging behavior functioned for avoidance, systematic assessment revealed that social positive reinforcers (e.g., attention, preferred activities) were also key factors. This information was vital for the selection of treatment components and practice contexts (e.g., following adult directives broadly rather than separations only). By tailoring treatment, we were able to target all contexts that evoked challenging behaviors, rather than narrowly targeting behaviors that occurred within the context of a specific diagnosis.
Recommendations to Clinicians and Students
To ensure accuracy, clinicians should use functional assessments that evaluate both what triggers and what maintains a behavior targeted for reduction. The assessment process can inform which treatment components to include as well as current skills. For example, our cumulative duration schedule of reinforcement began at 3 minutes because Layla had been observed to tolerate potentially aversive stimuli at least that long during the escape condition of the functional assessment. Without those data, the starting point of the cumulative duration schedule may have over or underestimated Layla’s current skills.
Second, it is recommended that data are collected on both the primary and secondary goals of treatment. Clinicians should collect both types of data whenever possible as the data can provide evidence of progress and treatment effectiveness. For example, the primary goal was for Layla to return to school, but she did not attempt a return until after the ninth treatment appointment. Having collected data on secondary goals (e.g., compliance with nonpreferred adult directions in clinic) the clinical team had greater confidence in Layla’s ability to be successful with the primary goal and had specific recommendations for the school team about how to ease the transition. Data collection on the secondary goals also allowed the family to demonstrate mastery of skills and strategies in an efficient way, moving them to the follow up phase of treatment even though they had only just re-entered school. In fact, pulling Layla from school to continue with therapy appointments may have inadvertently made the return to school harder if therapy was viewed as preferrable to school attendance.
Third, when the primary goal is a return to school, clinicians should attempt to provide coordinated care with the school team whenever possible. For Layla, a single re-entry meeting toward the end of treatment, when specific strategies based on treatment progress could be provided, was sufficient. It is possible that other families may need more or less support. Additionally, Ms. Hunter and Layla had taken steps outside of session to complete exposures to the school building (e.g., parking in the parking lot, returning a library book to the school library) prior to full re-entry. These exposures were critical for slowly habituating Layla to returning to school as well as identifying other components that may make re-entry more difficult (e.g., attention from peers). Although clinicians cannot dictate the policies, procedures, and strategies implemented by school, sharing successful strategies from the clinic and helping the school and family to craft a specific plan for how to respond to various outcomes can only help with the transition.
This case study has four primary limitations. First, contrived functional assessments did not clearly reveal the behavior’s function, which was instead derived from home descriptions and clinic transition observations. Given time constraints, the team forewent further assessment, though repeating the request compliance condition using schoolwork rather than play may have clarified the pattern. Second, the lack of an experimental design prevents establishing a true causal relationship between the intervention and Layla’s symptom reduction, leaving alternative explanations like maturation possible (Kazdin, 2021). Future replications should employ reversal, multiple baseline, or alternating treatments designs. Third, the absence of systematic data collection on Layla’s Home & Hospital attendance limited information on treatment generalization. With consent, clinicians could have taught teachers to implement the FCR and cumulative duration reinforcement schedule to improve school participation. Finally, a single rater observed the dependent variables and procedural fidelity of Ms. Hunter’s implementation. The lack of a second observer precluded inter-observer agreement, potentially limiting confidence in the intervention’s reliability and integrity.
In conclusion, this case study demonstrates the effectiveness of an assessment-based approach to challenging behavior in a child diagnosed with separation anxiety. It highlights the importance of understanding the function of the behavior, breaking cycles of caregiver accommodation of challenging behavior, and the utility of skills practice with secondary goals when the primary treatment goal is unable to be replicated in clinic. These approaches can help clinicians develop and provide efficient and effective treatments to families.
Footnotes
Acknowledgements
We thank the family for making this case study possible.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and has been deemed exempt by the Johns Hopkins Institutional Review Board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data is available upon reasonable request.