
Abstract
Although outcomes are modest, extant studies for bipolar disorder have supported comprehensive behavioral treatments and medication management. These treatments are customarily focused on psychiatric symptom reduction, which may be stigmatizing and overlook the optimal spectrum of functioning. As a novel alternative to traditional treatment, we examined the implementation of Performance Optimization-Focused Family Behavior Therapy (POFFBT) in a performance artist who evidenced bipolar I disorder with psychotic features, social anxiety, and cannabis use disorder as well as psychiatric symptoms and performance anxiety. POFFBT meetings occurred within the context of Coordinated Specialty Care (CSC). In clinical trials POFFBT has decreased psychiatric symptom severity and improved sport performance and relationships in adolescent and emerging adult athletes. However, POFFBT has yet to be evaluated in performance artists or within the context of CSC, which appears to enhance intervention engagement and outcomes for individuals with early serious mental illnesses. A battery of assessment measures was administered at baseline and six-month follow-up. Results indicated a substantial decrease in mental health symptom severity and increased social engagement. Future directions are discussed in light of the results.
Theoretical and Research Basis for Treatment
Bipolar disorder (BD) is characterized by cyclic manic, depressive, and often psychotic symptoms; affecting approximately 40 million individuals worldwide (Nierenberg et al., 2023). Individuals living with BD often experience functional decline in various life domains, such as education and vocational absenteeism, financial independence, social performance, and executive functioning. Persons with BD frequently evidence comorbid disorders, most often including substance use and anxiety disorders (Ostacher, 2011).
Treatment for BD customarily involves comprehensive psychological evaluation to ensure diagnostic accuracy and determine symptom presence across various mood states, such as euthymia, depression, hypomania, or mania. Once illness timeline and current mood state are established, pharmacological intervention is typically employed to stabilize mood fluctuations across time utilizing mood stabilizers or antipsychotic medications. Individuals who receive psychotherapy in addition to pharmacological management have evidenced better outcomes than those who receive pharmacological management alone (Swartz et al., 2018). Therefore, after acute symptoms are sufficiently reduced, intervention focus shifts to long-term illness management through psychotherapy, and whenever possible, psychological interventions are implemented within the context of Coordinated Specialty Care (CSC). Early intervention is critical to the proactive success of CSC, as this period has the greatest potential to limit illness progression and facilitate positive life outcomes (Lieberman et al., 2013).
Clients enrolled in CSC programs receive individualized care from a cross functional team of mental healthcare workers who provide standardized pharmacological medical services, psychotherapy, family psychoeducation, and employment and education support, with some programs also offering peer support and case management. These programs are strength-based, resilience focused and determine services that are appropriate to individual clients using shared decision-making, a model that has shown significant success in lowering conflict, stigma, regret, and increased involvement in treatment planning (Langer et al., 2022). The CSC approach addresses biological, social, familial, and community contributors to early serious mental illness and recovery. Additionally, studies have found that CSC programs lead to improved medication adherence, fewer hospitalizations and overall better quality of life in patients displaying psychosis (Gafoor et al., 2010). CSC increases treatment engagement in clinical populations that are typically difficult to engage, increase occupational and social functioning, and reduce symptom severity over time (Dixon et al., 2015). Originally developed for the treatment of individuals experiencing first episode psychosis (Kane et al., 2016), CSC has since been adapted for individuals at clinical high risk for psychosis (CHR-P) (West et al., 2021) and, in the current examination, for individuals experiencing early BD.
A Novel Performance Optimization-Focused Family Behavior Therapy Within the Context of Coordinated Specialty Care
Clinical trials generally support medication management and behavioral therapies, particularly when they are implemented within the context of CSC. However, the focus of traditional psychotherapies on pathology has led many patients with BD to feel stigmatized, which has influenced them to decrease their adherence to medication, evidence diminished social support, and avoid therapeutic programing (Perich et al., 2022). To promote a positive perspective in patients with BD, researchers recently developed a Performance Optimization Focused Family Behavior Therapy (POFFBT) within the context of family-based medicine, peer support and CSC. Derived from Family Behavior Therapy (FBT) (Azrin et al., 1994) and inspired by Positive Psychology (Seligman & Csikszentmihalyi, 2000), POFFBT is a non-pathological, cognitive-behavioral intervention that focuses on performance optimization rather than personal deficits. POFFBT generally involves (1) soliciting from patients what they did, thought or perceived optimally in performance situations throughout the week, given their current resources, skills and demands from the environment, (2) descriptively praising patients for these efforts, and (3) challenging patients to optimize their thoughts, perceptions and actions for future use. Clients are assisted in this process using various cognitive and behavioral interventions. Both uncontrolled (Donohue et al., 2014, 2016, 2021; Gavrilova et al., 2017; Phrathep et al., 2022a, 2022b, 2023; Pitts et al., 2014), and controlled (Chow et al., 2014; Phrathep et al., 2021), evaluation studies have shown this intervention consistently demonstrates reduced psychiatric symptoms, and improved relationships and sport performance in athletes, with and without mental health disorders, particularly as psychiatric symptomatology increase (Donohue et al., 2018, 2020).
The current case examines the application of POFFBT within a CSC program for a client presenting with comorbid bipolar I disorder and performance anxiety. The client, a performance artist, represents a novel application of POFFBT, as the intervention has traditionally been implemented as a standalone strategy and has not previously been applied to populations with early serious mental illness or to performance artists.
Case Introduction
Alex is a biological male Caucasian adult who was referred to intervention by a family member for a manic episode that resulted in hospitalization three months prior. Consistent with program requirements, Alex was required to (a) evidence bipolar I disorder, bipolar II disorder, or related manic-depressive disorders, (b) evidence less than 12 months of lifetime treatment with antipsychotic or mood stabilizing medications, (c) be at least 15 years old, and (d) evidence no lifetime history of traumatic brain injury, neurodevelopmental disorder, seizure disorder, schizophrenia-spectrum, or other psychotic disorder.
Presenting Complaints
Verbal consent for program involvement was obtained to establish presenting complaints in a phone screen, and written consent for program involvement was obtained prior to baseline neuropsychological testing administration. Alex reported that he was seeking treatment because of manic symptoms (expansive mood, grandiosity, psychomotor agitation, risky behavior, and pressured speech), depressive mood symptoms (sadness, feeling miserable, asociality, and suicidal ideation), psychotic symptoms (delusions and tactile, visual, and somatic hallucinations), and anxiety symptoms, primarily surrounding social and performance situations. Alex indicated that these experiences were clinically distressing and negatively impacted his functioning (e.g., decline in college coursework, dropping out of college classes, financial impact after giving away thousands of dollars, strained relationships with family members). He reported that some of these symptoms began in childhood but were becoming more frequent, distressing, and negatively impactful in the most recent months prior to his hospitalization and referral to the current program.
Additionally, Alex reported a lifetime history of social anxiety as related to both prosocial relationships and performance success, namely fine arts performance. Alex indicated (a) marked fear of social situations such as performing for people outside of the family unit, (b) being afraid of making mistakes for fear of failure or ridicule, and (c) having excess fear that is out of proportion to the actual threat (i.e., performing in public), symptoms congruent with social anxiety disorder. These situations historically provoked fear and caused significant distress, leading the client to actively avoid participation in public performance and prosocial activities.
History
At the time of intake, Alex was prescribed oxcarbazepine (300 mg PO BID) and risperidone (2 mg PO QD) for treatment of his psychiatric symptoms and indicated he was taking the medications as prescribed. Alex’s family psychiatric history includes depression and anxiety. He denied a history of bipolar disorder, schizophrenia-spectrum disorders, or other serious mental illnesses in first-degree relatives.
Assessment
Diagnostic Assessment
The Structured Clinical Interview for DSM5 Disorders Research Version (SCID-5-RV)
The Wide Range Achievement Test 5 (WRAT 5) is utilized to assess academic achievement in all age and ability groups (Wilkinson & Robertson, 2017). Three subtests (Word Reading, Sentence Comprehension, and Coding) were utilized for the study’s purposes to assess baseline academic functioning relevant to educational avocational outcomes, which are central targets within CSC.
Wechsler Adult Intelligence Scale – Fourth Edition (WAIS-IV). The gold standard cognitive assessment for intellectual performance (Weschler, 2008), comprising ten psychometrically validated (Sadeghi et al., 2011) core subtests yielding four index scores. The Digit Span and Coding scaled scores were utilized to provide an estimate of baseline cognitive functioning in domains relevant to treatment engagement and performance optimization (i.e., working memory and processing speed). Deficits in these areas influence functioning outcomes and responsiveness to behavioral interventions and thus were used to contextualize Alex’s ability to engage in and benefit from POFFBT.
Secondary Measures
The Brief Psychiatric Rating Scale (BPRS) is one of the most frequently used instruments used to determine the severity of psychopathology in patients exhibiting psychotic symptoms. The Likert scale from 1 (not present) to 7 (extremely severe) assesses 18 psychotic symptom subtypes such as suspiciousness, positive symptoms, and grandiosity (Overall & Gorham, 1962), and has expressed satisfactory sensitivity and specificity in psychiatric and nonpsychiatric settings (Lee et al., 1990).
The Hamilton Depression Rating Scale (HDRS) is a widely used clinician-administered depression assessment scale, containing items measuring the severity of depressive symptoms in the past week relative to clinical interview (Hamilton, 1960), and has been shown to express good reliability and consistency (Trajković et al., 2011).
Young Mania Rating Scale (YMRS) is an 11-item clinician-rated scale to assess observations of mania (elevated mood, increased motor activity/energy, sexual interest, sleep, irritability, speech, language/thought disorder, content, disruptive/aggressive behavior, appearance, and insight) during a clinical interview (Young et al., 1978), that has exhibited appropriate psychometric properties in assessing the severity of mania in bipolar disorder (Mohammadi et al., 2018).
The Scale to Assess Unawareness of Mental Disorder (SAUMD) is one of the most widely utilized assessments to measure insight into psychological disorders and has been shown to exhibit good reliability and validity (Amador et al., 1993). The current study employed the abbreviated version of the SAUMD measure.
The Outcome Questionnaire (OQ), version 45.2 (OQ-45.2; Lambert et al., 1996) is a comprehensive overview of overall mental health and perceptions designed to examine treatment related changes in symptoms. The OQ measures symptoms along three subscales; (1) Symptom Distress and Discomfort, intrapsychic functioning with an emphasis on depression, stress, and anxiety; (2) Interpersonal Relations, conflict with others, loneliness, inadequacy, and difficulties with loved ones; and (3) Social Role, difficulties with school, work, or home. A score of 64+ is categorized as “dysfunctional range.” Risk assessment for critical items relating to suicidal ideation, substance abuse, and anger and violence at work or school are also included. Changes in OQ total and subscale scores can be interpreted using the reliable change index (RCI) that allows for objective determination of improvement (decrease) or worsening (increase) of symptoms over time and is represented by the difference between a client’s baseline and follow-up score (Shimokawa et al., 2010). Previous studies support validity of the correlations between clients’ presenting concerns and OQ total scores (Boswell et al., 2013).
Baseline Assessment Results
Psychological Assessment and Symptom Ratings Results
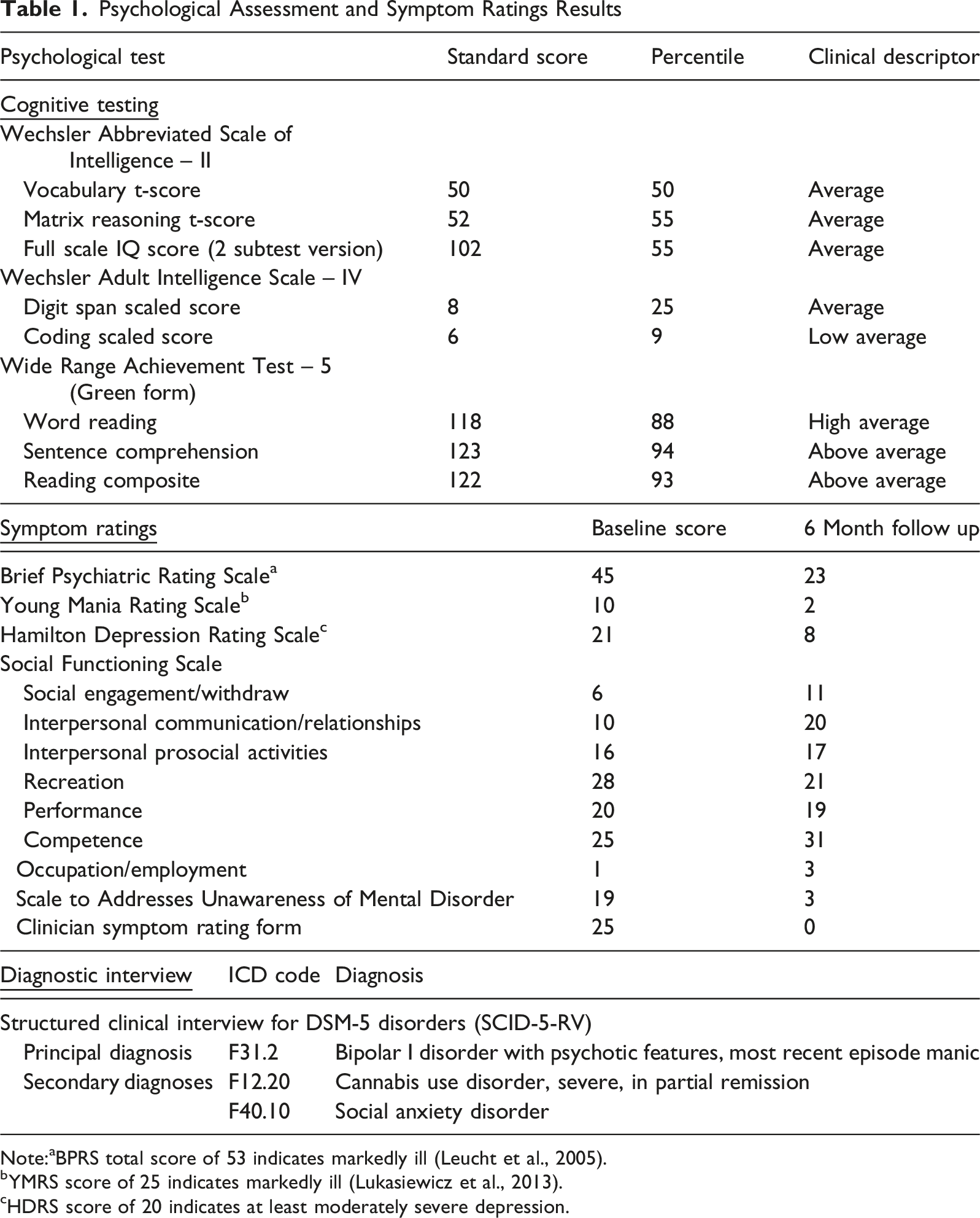
Note:aBPRS total score of 53 indicates markedly ill (Leucht et al., 2005).
bYMRS score of 25 indicates markedly ill (Lukasiewicz et al., 2013).
cHDRS score of 20 indicates at least moderately severe depression.
Case Conceptualization
Alex’s case was conceptualized in accordance with Performance Optimization Theory (Donohue et al., 2018), which is presented in Figure 1. The triangle illustrates that optimal functioning across thoughts/perceptions, actions and emotions is associated with optimal mental health and performance outcomes. The optimal state demonstrates high resistance to various environmental stressors. As the bottom section of the figure indicates, cognitive and behavioral skills are distributed along a continuum from non-optimal to optimal. Adapted from the widely used Cognitive the Behavioral Therapy Triangle, the tenets of Performance Optimization Theory are employed to teach patients to use cognitive behavioral skills to facilitate optimal thoughts, perceptions and actions in targeted performance situations (i.e., mental strength, relationships, creativity, physical health, work/school). Optimal is defined as thinking, perceiving and doing in the best way possible given current skills, available resources and demands from the environment. In this way, performance optimization is dynamic, and patients are consistently challenged to optimize their thoughts, perceptions and actions using various skill sets that are later taught in treatment. POFFBT optimization model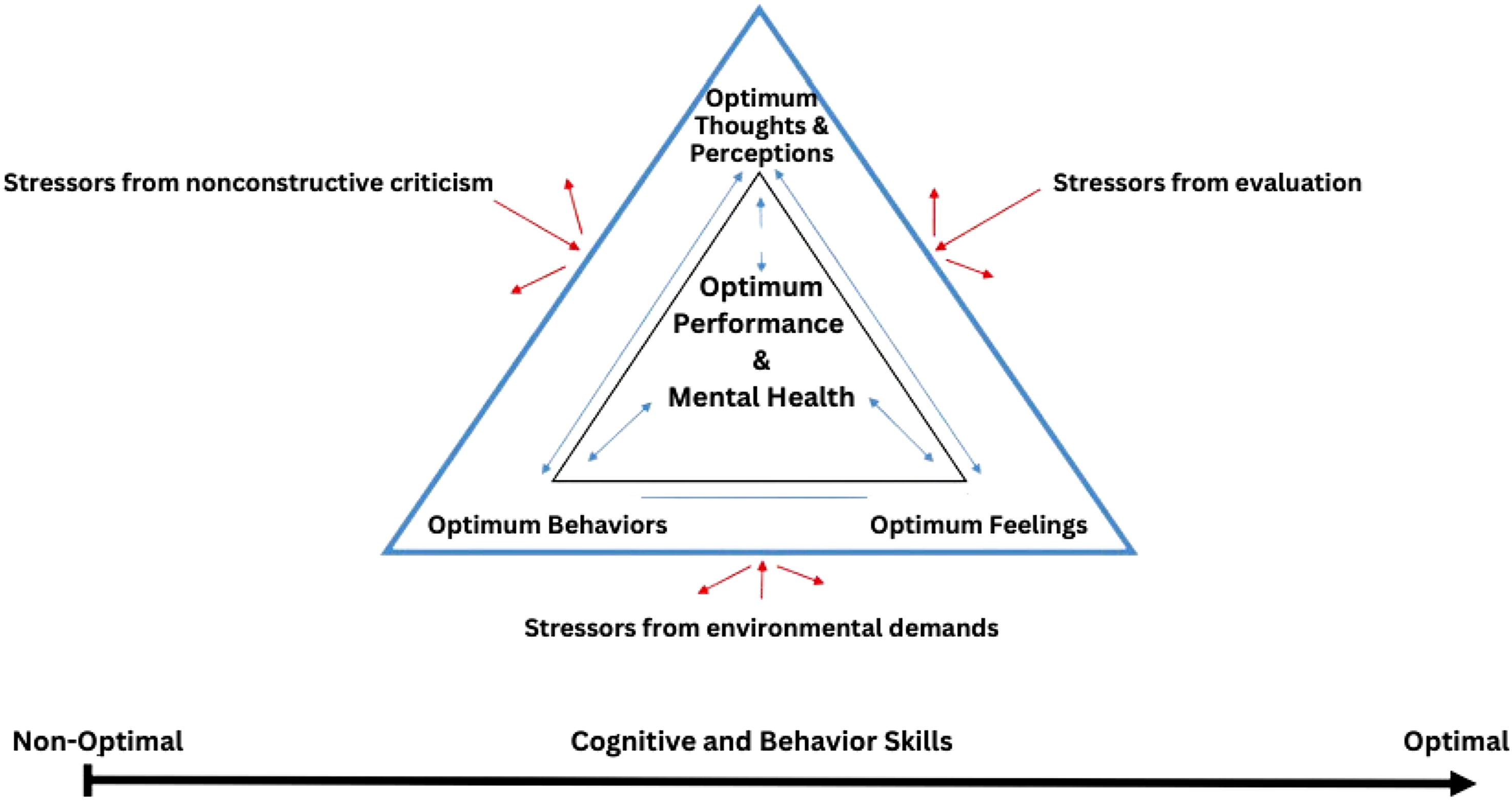
Prior to treatment, Alex would focus on potential negative outcomes of social engagement, which in turn would discourage social connectedness with others. Specific to performance arts and ability, Alex approached performance situations with negative expectations and maladaptive self-talk (“I’m going to mess up”) and avoided activities in which public performance could potentially occur. Alex’s avoidance of social interactions and performances led to nonoptimal behaviors (e.g., restricted training in the arts, low levels of feedback); thus, negatively impacting mental health and positive performance in these domains. Adverse interpersonal interactions exacerbated repetitive negative thinking and self-criticalness, which has been purported to predict expression of bipolar manic, depressive, anxiety symptoms (McEvoy et al., 2018), and excessive cannabis use to relieve acute anxiety. Therefore, Alex’s bipolar symptoms, negative thinking, social isolation, and lack of community and social connectedness were primary targets in treatment/performance planning with the aim of optimizing social, educational and artistic performance and reinforcement of positive thinking patterns.
Course of Treatment and Assessment of Progress
In alignment with the shared decision-making model of CSC, Alex was provided with a comprehensive list of all program services and, through collaboration with both supportive others and therapeutic team, selected the services he wanted to prioritize, which included POFFBT, medication management, and peer support. Alex’s family also received a list of available family services, including family education and peer support groups.
Weekly collaborative check-ins between supervising psychologists, psychiatrists, and peer support teams ensured that the POFFBT therapeutic model was consistently applied across all aspects of care. Providers actively integrated the optimization language and framework in individual sessions, reinforcing the optimization approach into every stage of treatment.
Performance Optimization-Focused Family Behavioral Therapy (POFFBT)
POFFBT was administered by a graduate student clinician under the supervision of a licensed clinical psychologist for 25 sessions across 6 months. The initial POFFBT appointment (i.e., Program Orientation) was utilized to (a) discuss performance related goals and expectations, (b) review general information about the CSC program, (c) solicit commitments to incorporate individuals who could support Alex in the programming (i.e., his mom), (d) define optimal performance (i.e., doing, thinking and perceiving in the best way possible given available skills and resources while managing demands in performance situations; perceptions are conceptualized to be important sensations that are interpreted as beneficial, such as hearing a mother’s voice leading to comfort), (e) review Performance and Mental Health Optimization Theory (i.e., demonstrating how optimal mental health and performance occur when thoughts, perceptions and actions occur optimally; which in turn resist stressors due to nonconstructive criticism and environmental demands), (f) review examples of nonoptimal and optimal thoughts, perceptions and actions, (g) review strategies that are relevant to the optimization of thoughts, actions and perceptions, and (h) solicit personal examples in which optimal values were recently demonstrated. In order to destigmatize clinical language, Alex was referred to as an “optimizee” and his therapist was referred to as an “optimizer.”
The
Cultural Domains Menu (CDM) and Semi-structured Interview for
Psychiatry
Although medication is not a requirement for program participation, it is necessary for individuals to attend appointments with a psychiatrist to discuss psychiatric symptoms, medication options, potential side effects of medications, and overall physical well-being. Subsequent psychiatry appointments occur monthly to assess ongoing medication efficacy, adjust prescription dosages, provide ongoing support, and monitor concerns and symptoms. Alex attended five total medication management appointments. Prior to psychiatric intake, Alex was prescribed 300 mg of oxcarbazepine, 2 mg risperidone, and carvedilol for high blood pressure. After program enrollment, supervising psychiatrists raised the original risperidone dosage from 2 mg to 3 mg to increase medication efficacy and decrease mood destabilization. Within six weeks of taking the increased risperidone dosage, Alex reported ten pounds of weight gain. With consideration to clinical concerns regarding previous disordered eating habits and maladaptive self-image, the psychiatric team instructed Alex to discontinue risperidone and instead was prescribed 10 mg of aripiprazole at the fourteen-week follow-up to prevent further weight gain and lessen symptomatology severity.
During weekly treatment case rounding, the supervising psychiatrist and primary optimizer collaboratively reinforced the optimization-focused coordinated specialty care model by reporting maladaptive thinking patterns disclosed during psychiatry appointments, such as artistic performance anxiety and difficulties with interpersonal relationships. These cognitive themes were then systematically integrated into ongoing weekly POFFBT sessions by utilizing the Optimal Mindset and Positive Requests exercises. These exercises provided Alex with the skills to discuss medication adjustments in psychiatry appointments, improve his performance skills despite previous anxieties, and develop more positive relationships with family and friends. As reported by Alex:
“I think that it (i.e., POFFBT) has helped me be more resilient…. The experience adds more depth to me. When I listen to music, it just reminds me of how resilient I am because I do not let depression take me. I am in a much better place, I am doing great, I am much more positive. I am not always happy, but I am much more positive… I think that a lot of what I used to deal with was nihilism, like I used to think that there is no point to anything at all, and it was really debilitating.”
Peer Support
A certified Peer Recovery Support Specialist (PRSS) was available to assist in accessing, scheduling, and providing social and community resources for care outside the CSC network of providers. This branch of the CSC is critical to increasing support networks, reducing stigmatization of mental illness, and bolstering individual autonomy in the client (Blajeski et al., 2021), as well as education and support of family members and loved ones. This family-integrated community approach fosters strength and resiliency in support systems, developing meaningful understanding of serious mental illness, and generating social support systems such as community outreach programs, group therapy, and identity- and culturally informed mental health services.
Alex and Alex’s family engaged in peer support from the current program in multiple ways. The PRSS provided resources for mental health support groups conducted both in person and virtually, social events and community building classes, community computer gaming classes, as well as resources for text lines and crisis phone numbers. Alex’s mother completed a recovery-focused, evidence-based 8-week Family Education course through the National Alliance of Mental Health (NAMI), which provides mental health education and strategies for assisting loved ones with mental illness. Classes are led by individuals with lived experiences and formal education, and include presentations, interpersonal discussions, and interactive exercises.
Complicating Factors
Several complicating factors must be considered when interpreting this case. First, this report describes a single individual receiving comprehensive CSC. As such, given the multimodal nature of CSC and concurrent pharmacological treatment, symptom reduction cannot be attributed solely to POFFBT. However, this care demonstrates that an optimization-focused, strengths-based framework can be successfully and safely implemented within early serious mental illness services and may compliment stabilization for BD. The integration of optimization language across psychiatry, psychotherapy, peer support, and family involvement appeared to promote consistency in treatment messaging and reinforce adaptive cognitive and behavioral patterns across settings. Further, improvements may partially reflect the natural course of recovery following acute manic hospitalization, regression to the mean, or the client’s remission from cannabis use disorder. Thus, further research is necessary to determine the individual contributions to recovery of POFFBT in BD.
Access and Barriers to Care
Throughout the treatment course, Alex lacked reliable methods of transportation to appointments and would often employ ride sharing services. The financial burden associated with employing transportation services resulted in reduced engagement in CSC resources, including intervention and psychiatry appointments, and most notably, peer support opportunities. For example, the PRSS provided Alex with several in person opportunities—such as community engagement to help foster autonomy and social connectedness—to apply the skills learned in POFFBT sessions. However, these opportunities were declined due to the client’s limited transportation options.
Follow-Up
Clinician Ratings
Monthly reassessments to monitor progress were collected at medication management appointments through a clinician symptom rating form that encompassed a variety of somatic and psychological symptoms, including depression, anxiety, mania, suicidal ideation, hostility, and insight. Additionally, the SAUMD, YMRS, BPRS, and HDRS instruments were utilized at six-month follow up to assess treatment effectiveness (Table 1). Standardized clinician ratings completed at follow up indicated trends toward improvement in recovery and remission across all measures.
Social Functioning
The Social Functioning Scale (SFS) has demonstrated strong reliability, validity, and sensitivity in adult psychosis samples (Birchwood et al., 1990) and provides an overview of functioning for seven domains of social behavior: (1) Social Engagement/Withdrawn, (2) Interpersonal Communication/Relationships, (3) Interpersonal Prosocial Activities, (4) Recreation, (5) Performance, (6) Competence, and (7) Occupation/Employment.
Alex’s SFS subtest scores for baseline and follow up are outlined in Table 1, with all subtest domains illustrating positive trends with intervention, except for Subtest 4. Recreation (decrease of −7) and Subtest 5. Performance (decrease of −1).
Outcome Questionnaire, Version 45.2
The OQ was administered at baseline and at each therapy session. Alex’s OQ scores across the 25 POFFBT appointments are outlined in Figure 2. Alex’s baseline total OQ score (pre-intervention) was 111, indicating high distress and dysfunction. At 6-month post-intervention follow-up, Alex reported an OQ score of 37, indicating a “low” distress level and normal functioning. His positive response to treatment was marked as “in recovery” and with a suggestion to consider termination of intervention services. A Reliable Change Index (RCI) was calculated using Alex’s total baseline and follow-up scores on the OQ-45.2 to evaluate whether clinically significant change occurred over the course of treatment. According to established publisher criteria, a change of ±14 points on the OQ-45.2 indicates reliable change. Alex’s RCI was −26 at the time of 6-month follow-up, reflecting a reliable improvement in overall psychological functioning. All subscales indicated a negative trend towards recovery. OQ-45.2 Domain and Total Scores Across 25 POFFBT Sessions. 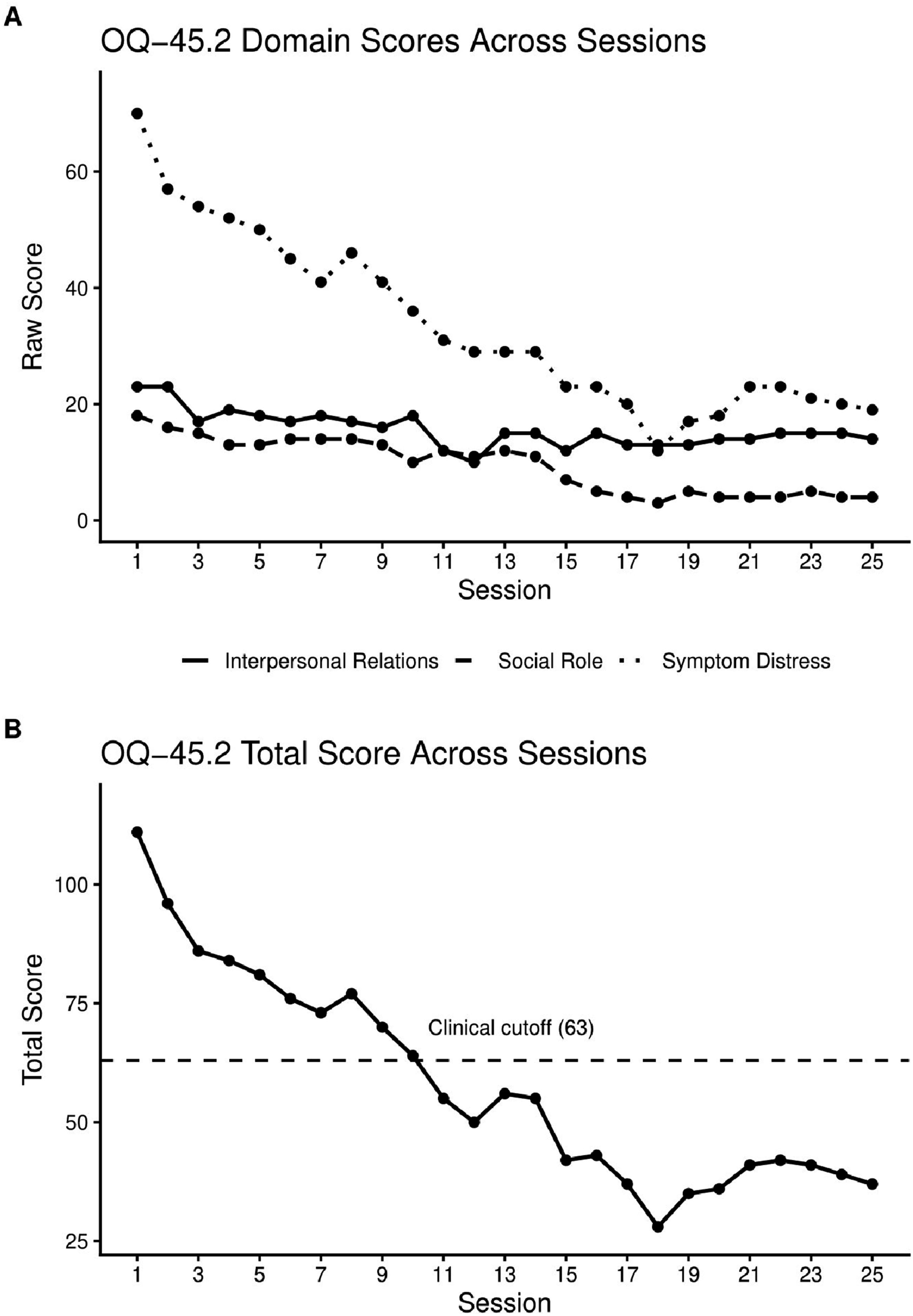
Treatment Implications of the Case
This care illustrates the feasibility and clinical integration of Performance Optimization Focused Family Behavior Therapy (POFFBT) within a coordinated specialty case (CSC) program for an individual with early bipolar I disorder with psychotic features and comorbid social anxiety and cannabis use disorder. Over the six-month course of treatment, improvements were observed across multiple domains, including depressive, manic, and psychotic symptom severity, interpersonal functioning, and engagement in artistic performance. These changes occurred alongside consistent participation in POFFBT, psychiatry, and peer support services.
Notably, the client demonstrated high treatment engagement, sustained attendance, and active participation in goal-directed exercises in vivo. The optimization-focused treatment framework highlights the increased willingness to engage in treatment by shifting focus from negative pathology to growth and performance enhancement. This strengths-oriented positioning may be particularly valuable for individuals with stigmatized mental health conditions such as bipolar disorder.
Recommendations to Clinicians and Students
This report offers several practical considerations for clinicians and trainees working within coordinated specialty care (CSC) programs for early bipolar disorder and related serious mental illnesses.
First, incorporating strengths-based, optimization-focused language into psychotherapy may enhance engagement and reduce stigma associated with treatment. Many individuals with bipolar disorder experience shame, self-criticism, and fear of failure, particularly in domains central to identity and performance. Framing intervention around growth, skill development, and performance enhancement rather than symptom reduction alone may increase motivation and promote sustained participation in care. Second, this case highlights the potential value of integrating a consistent therapeutic framework across interdisciplinary team members. The use of shared optimization language in psychiatry, psychotherapy, peer support, and family services may strengthen treatment coherence and reinforce adaptive cognitive and behavioral patterns across settings. Further, a strength of the optimization framework is that it is well-suited for use beyond acute symptom phases (Galante et al., 2019). Teaching cognitive and behavioral skills during periods of relative stability may help individuals build resilience, anticipate stressors, and maintain functioning across mood fluctuations. Clinicians may therefore consider incorporating optimization-oriented goals work not only during symptomatic periods but also during remission to support long-term recovery. Finally, future research should evaluate optimization-focused approaches using controlled and longitudinal designs to determine whether they confer incremental benefit beyond standard CSC components and pharmacological management. Randomized trials, single case evaluation designs, and long-term follow-up investigations across diagnostic groups would clarify mechanisms of action and identify which patients may benefit most from this approach.
Taken together, this case supports continued exploration of optimization-based interventions such as POFFBT as a non-stigmatizing, engagement-enhancing strategy within early serious mental illness services.
Footnotes
Acknowledgements
We would like to acknowledge the many individuals that were part of Coordinated Specialty Care Early Treatment Program (CSC ETP). This was a project founded in helping the community and could not have been done without those on the administrative side, UNLV PRACTICE, and the individuals whose passion is to help others.
Ethical Considerations
The current report was exempt based on policies of the local university’s Institutional Review Board (IRB) for the protection of human services because it is based on deidentified archival clinical data.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided to Daniel Allen by the Substance Abuse Mental Health Services Administration Block Grant (1B09SM085370-01) and the Shear Family Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.