
Abstract
This case report evaluated the effects of behavior analytic intervention on post-feeding rumination in a 10-year-old child with Phelan-McDermid Syndrome (PMS), a genetic disorder associated with intellectual and neurodevelopmental disabilities and co-occurring medical abnormalities. A preintervention functional analysis screening conducted with the child suggested that rumination was maintained by automatic reinforcement. Non-contingent reinforcement (NCR) consisting of fixed-time (FT) presentation of preferred foods was associated with decreased rumination within a concurrent multiple baseline design across lunch meals and snacks combined with a snack-only reversal design analysis. Low rumination rates continued during an intervention withdrawal phase (lunch) and a phase of systematic schedule fading (snack). Social validity measures reported by the child’s mother and therapists revealed positive acceptance and approval of the intervention plan.
Theoretical and Research Basis for Treatment
Phelan-McDermid syndrome (PMS) is a genetic disorder resulting from SHANK3 haploinsufficiency, caused either by a chromosomal deletion at the 22q13.3 region encompassing the SHANK3 gene or by a pathogenic sequence variant within SHANK3 itself (Phelan et al., 2005). These changes are linked to severe cognitive and language impairments, motor delays, and behavior consistent with autism spectrum disorder (ASD). Other co-occurring symptoms include kidney abnormalities, seizures, hypotonia, sleep problems, ataxic gait, loss of previously learned skills, and decreased pain perception (Kolevzon et al., 2014; Srivastava et al., 2023). Further, individuals diagnosed with PMS have a higher likelihood of presenting gastrointestinal issues such as gastroesophageal reflux (GER), diarrhea or constipation, and feeding problems like pica and rumination.
Specifically, rumination disorder is characterized by four main diagnostic criteria (American Psychiatric Association, 2022). Repeated regurgitation of food must occur for at least 1 month with the individual possibly re-swallowing or expelling the consumed contents. Next, gastrointestinal causes for the rumination are ruled out. Third, rumination does not occur solely during episodes of anorexia nervosa, bulimia nervosa, binge-eating disorder, or avoidant/restrictive food intake disorder (ARFID). Finally, if rumination is comorbid with other mental disorders such as intellectual disability or ASD, they must be severe enough to require independent clinical attention.
Among many untoward outcomes, rumination can lead to negative physical and social effects, often malnutrition, weight loss, pulmonary aspiration, dental erosion, halitosis, and avoidance by peers and care providers (Kelly et al., 2014; Starin & Fuqua, 1987). Thus, rumination is classified among challenging behavior due to potential self-injury, association with feeding problems, and frequent incidence in individuals with intellectual and developmental disabilities (Van Dijk et al., 2021). Behavior analytic interventions, in particular, have been effective reducing and sometimes eliminating rumination in this population (Luiselli, 2015; Wilder & Lipschultz, 2016). Many of these interventions consist of multicomponent treatment packages comprised of complimentary procedures occasionally integrated with medication and nutritional strategies (Lang et al., 2011; Sanders-Dewey & Larson, 2006). The most widely researched procedures are food satiation diets (Jackson et al., 1975), differential reinforcement (Thibadeau et al., 1999), access to continuous competing stimulation (Rhine & Tarbox, 2009), and contingent application of unpleasant liquids like lemon juice and mouthwash (Foxx et al., 1979; Sajwaj et al., 1974). Procedural effectiveness in these and other studies depends on isolating the variables responsible for rumination, managing contingencies in the treatment environment, and training care providers to implement intervention competently.
An additional intervention approach to rumination is non-contingent reinforcement (NCR) presented on a fixed-time (FT) or variable-time (VT) schedule (Kliebert & Tiger, 2011; Lyons et al., 2007; Wilder et al., 2009; Woods et al., 2013). The behavior reductive effects of NCR result from frequent presentation of reinforcers functioning as a motivating (abolishing) operation that eliminates the positive value of certain stimuli, i.e., the automatic reinforcement contacted through ruminating (Cooper et al., 2020). As well, NCR is an antecedent control procedure that focuses on the prevention of challenging behavior without reliance on negative (punishment) consequences. Many care providers tasked with treating rumination may be more accepting of non-aversive intervention, which can promote procedural fidelity and lasting maintenance outcomes (Kennedy, 2002).
Schroeder et al. (2022) proposed that individuals with PMS would benefit from behavior analytic intervention, however “No studies or reviews are available to guide behavior analysts on how to effectively work with individuals in the PMS community” (p. 988). Accordingly, we present herein a case report of NCR implemented with a child who was diagnosed with PMS and engaged in chronic rumination after ingesting food. The study evaluated intervention within a single-case research design (Kazdin, 2020), assessed social validity among care providers (Wolf, 1978), and programmed NCR exclusively without the addition of behavior-contingent consequences (Baker et al., 2010).
Case Introduction
João (a fictitious name) was a 10-year-old boy diagnosed with PMS who resided at home with his biological family. He did not speak and used low-tech communication boards combined with gestures as his primary means of communication. João received intensive behavioral intervention for 40 hr per week and specialized speech-language therapy also on a weekly basis. Each weekday, he attended a clinic serving children and adults with intellectual disability, neurodevelopmental disorders, and rare genetic syndromes. Clinical services included individual and group therapies administered by multidisciplinary professionals. Throughout the study, João received omeprazole (20 mg), topiramate (50 mg), quetiapine (100 mg), and guanfacine extended release (1 mg) daily as prescribed by his medical team. The study described in this case report was conducted at the clinic, João’s mother (legal guardian) provided informed consent, and an institutional ethics committee approved all procedures (CAAE: 95078126.9.0000.5544).
Presenting Complaints
João had engaged in rumination for many years, consisting of regurgitating previously ingested food, typically re-swallowing the masticated contents, at times with ejection from the mouth. His mother reported during a preintervention interview that rumination in the home was common during the day especially after meals. She indicated that ruminating appeared to be volitional (“He induces the food’s return.”) and was difficult to manage. Hospital evaluations had ruled out medical causes and there were no biopsychosocial factors within the family to account for his rumination. João also displayed rumination daily after consuming food at the clinic.
History
On the Vineland Adaptive Behavior Scales-3 (Sparrow et al., 2016) administered when he was 9.7 years old, João achieved an overall score below 2 years of age. The Vineland score was more than 3 standard deviations below the normative mean across all assessed domains. As referenced earlier, he had a multi-year history of frequent ruminating that was unresponsive to pharmacologic treatment. His skill development was significantly delayed, he relied on alternative and augmentative communication (AAC), and challenging behavior (e.g., self-injury, dangerous climbing) occurred on occasion.
Assessment
Rumination was defined as João regurgitating partially consumed food into the oral cavity, re-chewing or maintaining the food bolus in his mouth, and either re-swallowing or expelling the contents passed his lips. A rumination response was detected from visible movement of the trachea. A trained observer recorded responses on a paper-and-pencil form during functional analysis screening, baseline, and intervention sessions (described below). The data were converted to a rate-per-minute measure by summing the number of recorded rumination responses in a session and dividing by session duration.
Social validity assessment consisted of the five therapists who conducted intervention with João completing a seven-item questionnaire when the study concluded. Questionnaire items were statements pertaining to concerns about safety, dignity, implementation time, efficiency, and generalization of intervention effects (e.g., “The procedure was effective in reducing rumination”). The therapists rated each statement according to a five-point Likert-type scale (1 = strongly disagree, 2 = partially disagree, 3 = neutral, 4 = partially agree, 5 = strongly agree). One additional item on the questionnaire inquired of the therapists: “How would you rate the difficulty level for implementing the procedure?” (1 = very difficult, 2 = difficult, 3 = moderate, 4 = easy, 5 = very easy).
João’s mother also completed a post-study questionnaire with eight statements that inquired about her acceptance and approval of the intervention plan procedures and results. Her responses to the questionnaire were based on observing João at the clinic and his behavior at home. The same five-point Likert-type scale on the therapist questionnaire applied to each statement (1 = strongly disagree, 2 = partially disagree, 3 = neutral, 4 = partially agree, 5 = strongly agree).
Case Conceptualization
As described by Querim et al. (2013), we conducted functional analysis screening based on the premise derived from parent interview that the rumination João exhibited was automatically reinforced by response-produced sensory stimulation. He was exposed to five consecutive 5-min sessions during a “no-interaction” condition implemented in a therapy room immediately after lunch. A single therapist (clinical supervisor) remained silent and stationary in one corner of the room while João engaged freely with several preferred and safe objects. Thus, the functional analysis screening was intended to document how often João ruminated absent social interactions and instructional demands.
The results of the functional analysis screening, represented in the lunch baseline phase of Figure 1, were a variable trend in rumination ranging from 0.8 to 1.4 responses-per-minute (M = 1.0). We hypothesized that these results suggested rumination was maintained by automatic reinforcement notwithstanding that the controlling effects of social positive and social negative reinforcement were not tested (Vollmer, 1994). The case conceptualization was that NCR with food might compete with and attenuate rumination-produced reinforcement and promote response reduction. Rumination responses per minute during baseline, intervention, and follow up sessions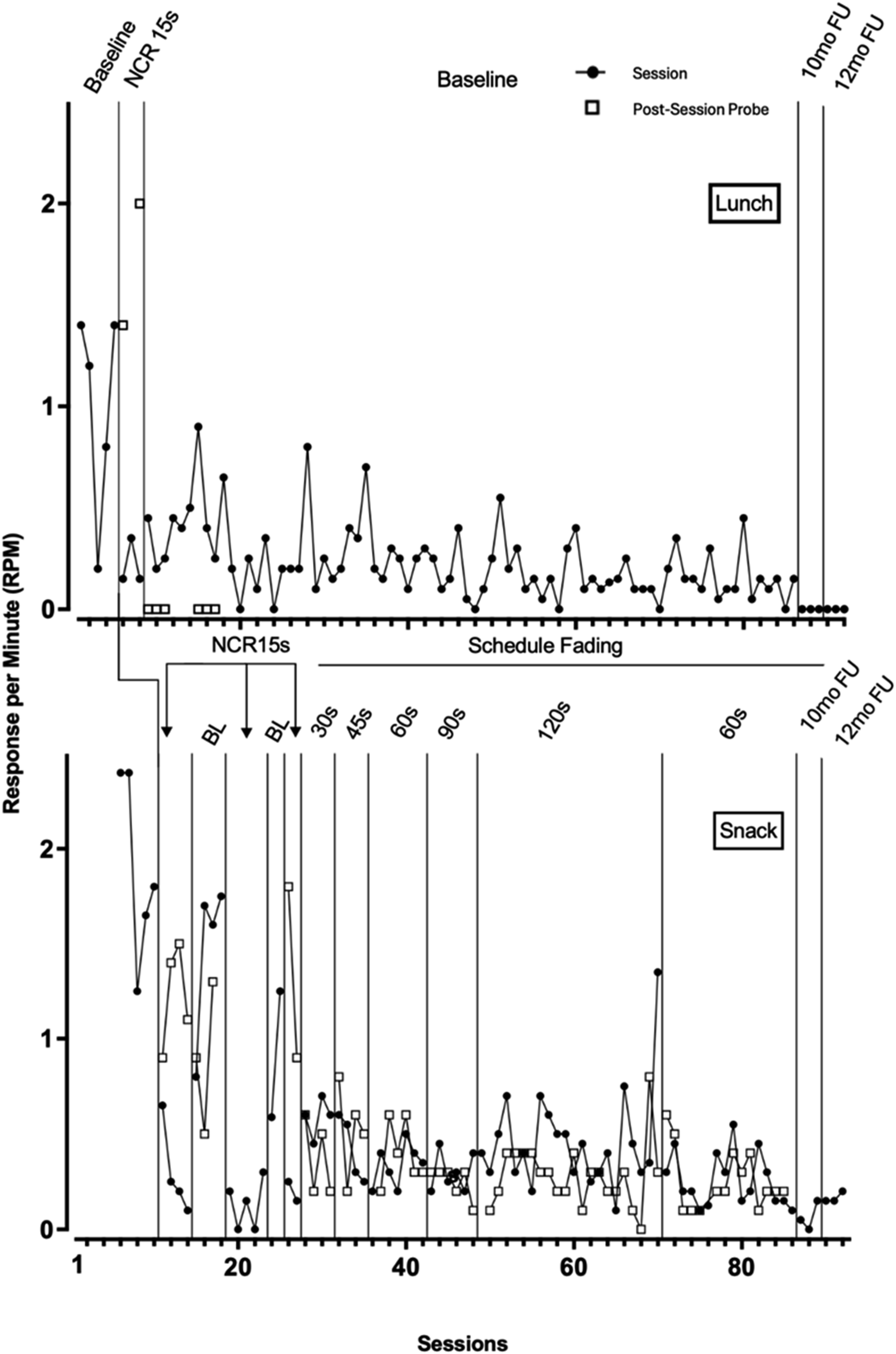
Course of Treatment and Assessment of Progress
Two of the authors, who were psychologists specializing in applied behavior analysis (ABA), trained and supervised four psychology interns and another psychologist with more than 5 years of clinical experience as therapists responsible for intervention in the study. The therapists learned to follow the intervention plan through instructions from the trainer and simulation until they demonstrated 100% accuracy during two consecutive training opportunities. Once the study began, the supervisors convened daily meetings with the therapists to monitor session data and progress. One of the supervisors also completed two to three observations of intervention sessions each week.
Baseline
Data recorded during the functional analysis screening represented the baseline phase for lunch meals. In addition, baseline measurement was introduced following a daily snack. The foods João ate were sent from home each day and remained relatively constant at lunch and snack throughout the study. For lunch, he typically consumed chicken, rice, beans, farofa (toasted cassava flour), and vegetables. His snack foods were banana, tangerine, mango, kiwi, frozen grapes, and pear, along with a type of porridge containing oats, honey, and whey protein. During post-lunch and post-snack sessions that lasted 20 min at baseline, a single therapist was present with João, did not interact with him, and withheld rumination-contingent consequences.
Intervention
Before lunch and snack, João participated in a multiple stimulus without replacement preference assessment (MSWO: DeLeon & Iwata, 1996) with his favorite foods (e.g., banana candy, peanuts, raisins) cut into 0.5 cm cube-shaped portions. The food item he selected most frequently was incorporated as a reinforcer during that day’s intervention session which immediately followed lunch and snack, lasting 20 min, and conducted in the therapy room. At post-lunch sessions, a single therapist presented him with a food item every 15 s (FT-15s) when signaled by the observer from intervals set on an iPhone timer. The food was delivered immediately and without delay when the interval passed, even if João was ruminating, which he always accepted and consumed. Subsequent to three intervention sessions, baseline conditions were reinstated for the remainder of the study. At post-snack sessions following a baseline phase, a single therapist implemented the FT-15s schedule for four sessions, whereafter baseline and FT-15s conditions were repeated within a four-phase reversal analysis. Subsequently, the FT schedule programmed during post-snack sessions increased by 15 s to a maximum of 120 s when the rate of rumination within the preceding phase decreased by at least 80% relative to baseline levels (i.e., schedule fading). The therapists continued to withhold rumination-contingent consequences during intervention sessions.
Post-Session Probes
We scheduled probe assessments periodically within baseline and intervention phases to evaluate within-session carryover effects. Immediately following a baseline and intervention session, João was observed and rumination recorded for an additional 10 min while a single therapist maintained the baseline conditions.
Figure 1 shows the rate of rumination responses per minute during baseline and intervention phases. As reported previously, the lunch baseline phase displays results of the functional analysis screening ranging from 0.2 to 1.4 responses per minute. Rumination decreased between 0 and 0.35 responses per minute with NCR in effect over three sessions. The rate of rumination in the two probe assessments was 1.4 and 2.0 responses per minute. Upon withdrawing NCR within the reversal phase, rumination remained low at a range of 0–0.9 responses per minute throughout baseline sessions and probe assessments.
Rumination recorded in the snack baseline phase ranged from 1.2 to 2.4 responses per minute. The NCR intervention was associated with decreased rumination between 0.3 and 0.7 responses per minute. Within the four-phase reversal analysis, rumination increased within the two baseline phases (range = 0.8–1.7 responses per minute) and decreased within the two intervention phases (range = 0.2–0.4 responses per minute.) A range of 0.1–0.8 rumination responses per minute occurred in probe assessments. Across schedule fading, the range of rumination responses was 0.3–1.3 in intervention sessions and 0.1–0.3 in probe assessments.
Social Validity Questionnaire Ratings of Therapists and Mother
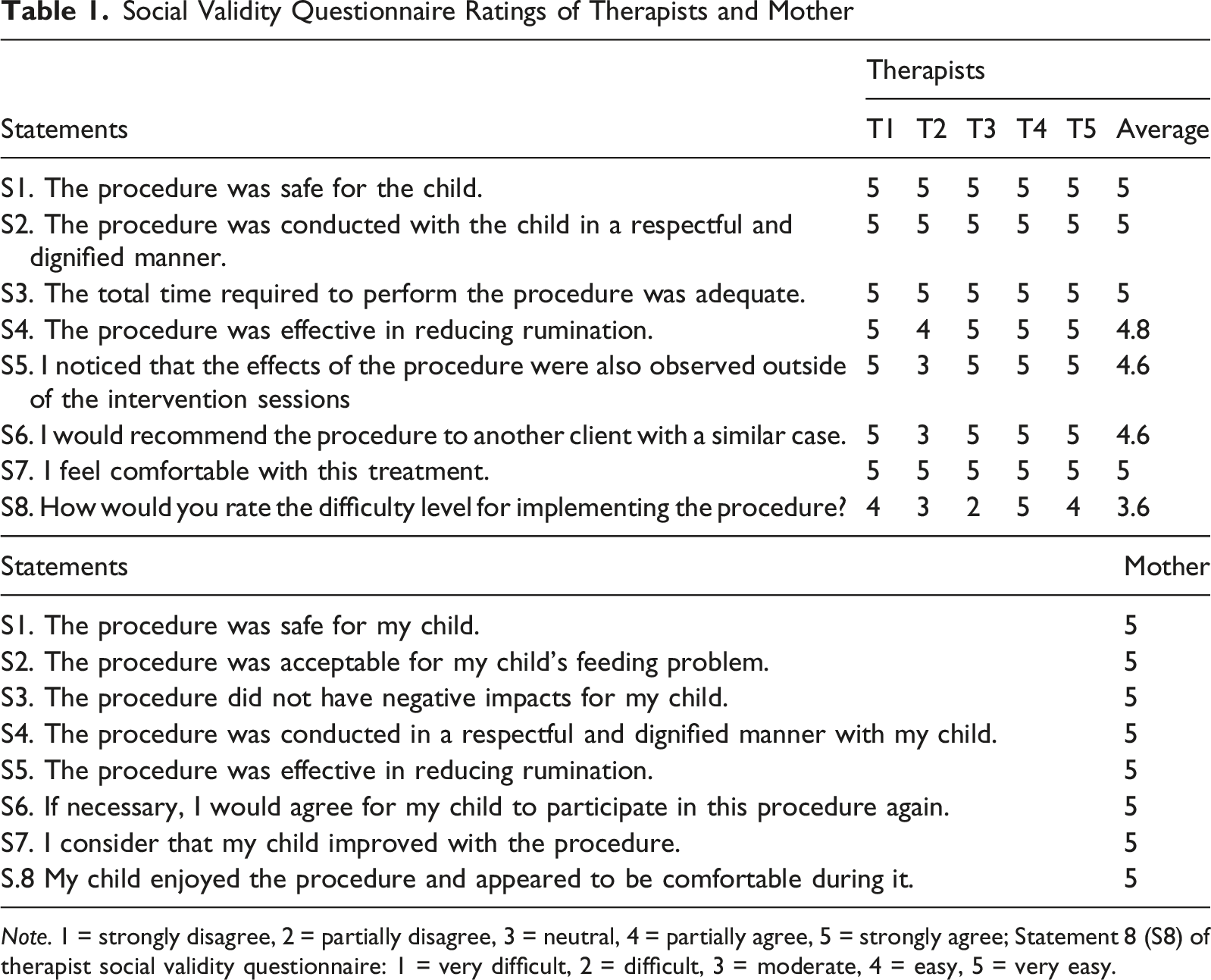
Note. 1 = strongly disagree, 2 = partially disagree, 3 = neutral, 4 = partially agree, 5 = strongly agree; Statement 8 (S8) of therapist social validity questionnaire: 1 = very difficult, 2 = difficult, 3 = moderate, 4 = easy, 5 = very easy.
Complicating Factors
Performing assessment and intervention with João required rearranging the therapy room to have limited furniture and removing objects that were not acceptable for play and exploration. Otherwise, there were no complicating factors affecting conduct of the study.
Access and Barriers to Care
João participated in the study at the clinic where he received daily therapy services. His familiarity with the setting eliminated difficulties that might have arisen if he were required to attend a novel location such as a hospital. A treatment team at the clinic made it possible to coordinate his care and closely monitor the rumination-reduction plan.
Follow up
Results at 10-month and 12-month follow up assessments while João continued to attend the clinic (Figure 1) were rates of rumination between 0 and 0.1 responses-per-minute within three sessions per phase. Baseline conditions continued in the follow up sessions after lunch and NCR at a FT-60s schedule was maintained in the follow up sessions after snack. Anecdotal report from João’s mother confirmed low-rate rumination at home during the same follow up phases.
Treatment Implications of the Case
This case study is the first to evaluate the effects of behavior analytic intervention in a child diagnosed with PMS (Schroeder et al., 2022). In summary, João had engaged in post-feeding rumination for many years preceding the study despite recommendations from a gastroenterologist and a prescribed pharmacologic regimen. We found that his rumination after eating lunch decreased when NCR was implemented on a FT-15s schedule. Unexpectedly, the rate-per-minute continued at relatively low levels when ongoing intervention was withdrawn. Conversely, evaluation of rumination after snack revealed that reduced rates were dependent on implementation of NCR. Gradual fading of the FT schedule also was consistently effective at durations ranging from FT-30s to FT-90s. Low occurrence of rumination was evident at follow-up.
The combined multiple baseline and reversal designs confirmed the controlling effects of the FT-15s schedule on rates of rumination following lunch and snack. The probe assessments at this schedule also showed that without intervention, rumination approximated or exceeded baseline rates. However, after three intervention sessions rumination did not increase post-lunch in the return-to-baseline phase including six probe assessments. Similarly, low-occurrence of rumination was documented in the snack intervention sessions and probe assessments following termination of FT-15s during schedule fading. We note that the rate-per-minute of rumination João displayed in the initial lunch baseline phase was variable with a decreasing trend before recovering to higher rates within the final two sessions. It is possible that this pattern may have continued naturally without intervention and explains the absence of a reversal effect at return-to-baseline.
Control over rumination at the FT-15s schedule was more definitive in the after-snack reversal analysis and results of subsequent fading suggest further sensitivity to gradually increasing FT schedules. Though not explored in the study, it is possible that the different textures and bulk of lunch and snack foods also could have influenced the respective outcomes within and across phases (Johnston et al., 1990). At lunch, for example, João ate foods with different textures (e.g., rice, beans, vegetables, mashed potatoes), suggesting that future studies should not mix texture-types and instead, compare the effects of solid foods versus soft-creamy foods on rumination. The same strategy could be used to evaluate whether varied food composition at lunch and snacks, as well as breakfast and dinner meals, and possibly the types of NCR edibles, affects the occurrence of rumination differentially.
The post-session probe data warrant attention. During lunch, although rumination rates remained low within three intervention sessions, the suspension of NCR during probes conducted 10 min after the session was associated with a transient reemergence of rumination. This pattern initially suggests that NCR may have merely delayed occurrence of rumination. However, João did not ruminate across six additional probes within the return-to-baseline phase. A similar pattern of increased rumination during snack probes was observed when the FT-15s schedule was implemented. One possible interpretation of these lunch and snack probe results is that motivating operations may have influenced the differential outcomes. Specifically, the larger volume of food João consumed at lunch combined with the additional portions delivered through NCR may have had an abolishing effect (satiation) on rumination during the post-intervention probes. In contrast, the snack food portions were considerably smaller and the same level of satiation may not have been achieved.
The therapists and João’s mother were consistently positive about the goals, quality, and effects of the rumination-reduction plan. Two therapists expressed “difficulty” implementing the procedures, possibly related to preparation tasks (e.g., cutting foods into small pieces) and having to deliver reinforcers on a dense schedule. Mother was uniformly satisfied with all facets of intervention and her child’s improvement. Notably, social validity assessment informs decisions about the selection and design of behavior-change procedures recommended to human services stakeholders (Luiselli, 2021). Such assessment is especially valuable when confronted with a problem as serious and often treatment-resistant as rumination.
Being limited to one participant, it is difficult to generalize our findings to other children with PMS and replication studies certainly are warranted. Additionally, this case was restricted to a day-clinic, the parents did not receive in-clinic training, and it was not possible to evaluate the effects of clinic-based intervention during dinner meals and on weekends at home. Further, the rumination data we acquired were recorded from direct observation but without periodic assessment of inter-observer agreement (IOA). Another limitation is that we did not record the duration of rumination episodes, an outcome measure that might provide additional insight into the clinical acceptability of NCR, particularly when rumination rates remained above zero. Notwithstanding these limitations, results of the study appear to support prior research on NCR as an effective treatment for post-feeding rumination encountered in children with intellectual and neurodevelopmental disabilities (Luiselli, 2015; Wilder & Lipschultz, 2016).
Recommendations for Clinicians and Students
Clinicians and students are advised to complete functional behavior assessment and/or functional analysis before intervening in cases of rumination. Assessment of behavior-function allows practitioners to formulate intervention plans based on hypothesized antecedent and consequence variables that evoke and maintain ruminating. The functional analysis screening method illustrated in this study is a practical and time-efficient approach when automatic reinforcement is suspected as the source of control over challenging behavior (Querim et al., 2013). A functional analysis with alone, attention, and demand conditions would be indicated if social contingencies appear to reinforce rumination (Iwata et al., 1994).
Also, during our functional analysis screening, we conducted a minute-by-minute visual inspection of the data and observed that responding was distributed quite uniformly within sessions. A more detailed within-session analysis may be especially valuable during NCR intervention to determine whether temporal patterns related to the most recent meal influence responding at the beginning of treatment sessions. Such findings could inform implementation of a variable NCR schedule with shorter intervals at the start of the session that are increased progressively as the session continues.
Implementing NCR on a dense FT schedule can be demanding and as much as possible, should be “thinned” to a schedule that is less frequent but effective (Demchuk et al., 2024). This study demonstrated successful schedule fading through FT-90s, then stable reduction of rumination upon a return to FT-60s. One strategy that was not evaluated in the study would be to repeat and further increase a sequence of schedule fading if an initial course was only moderately effective. Another approach to bolster intervention effectiveness might be instituting schedule fading with smaller increases in interval duration over a longer period of time.
Finally, the therapists responsible for intervention with João received comprehensive training and supervision before and during the study but there were no formal assessments of intervention integrity (Fryling et al., 2012). Integrity assessment targets the fidelity of procedural implementation according to prescribed protocols and written plans. Monitoring integrity ensures that ineffective intervention, if encountered, is not attributed to the procedures themselves but rather, stems from misapplication errors that must be corrected.
Footnotes
ORCID iDs
Ethical Considerations
The study was approved by an institutional ethics committee and conformed to the Helsinki Declaration and its amendments or comparable ethical standards.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data from the study are included in the published article.