
Abstract
Young children exposed to trauma often present with externalizing behaviors and attachment disruption that reflect early emerging deficits in emotion regulation and caregiver-child co-regulation abilities. Parent-Child Interaction Therapy for Toddlers (PCIT-T) is a dyadic, attachment, and behaviorally based intervention designed for children aged 12-24 months that targets these difficulties through in-vivo caregiver coaching with a focus on strengthening caregiver sensitivity, consistent limit-setting, and secure attachment within the parent-child relationship. Despite strong empirical support for PCIT with trauma-exposed populations, PCIT-T has not yet been examined in the context of complex early childhood trauma and caregiver adverse childhood experiences. This case report describes the use of PCIT-T with a 19-month-old male presenting with clinically significant tantrums, aggression, separation anxiety, and trauma reenactment behaviors following exposure to domestic violence, caregiver substance use, and caregiver instability. Treatment occurred over 27 sessions and focused on improving positive parenting skills, dyadic emotion regulation, and consistent limit-setting. The course of treatment was complicated by frequent disruptions in attendance related to caregiver occupational instability and ongoing psychosocial stressors. Despite these barriers, results indicated improvements in parenting skills, increased child compliance, improved emotional regulation, and enhanced attachment. This case supports PCIT-T as a feasible and appropriate intervention for toddlers exposed to complex trauma, with potential to disrupt intergenerational patterns of dysregulation through modification of caregiver-child interaction processes.
Keywords
Theoretical and Research Basis for Treatment
Trauma Within Families
Adverse Childhood Experiences (ACEs) are potentially traumatic events that occur before the age of 18 and can have lasting effects on an individual’s development and well-being. These experiences include various forms of abuse (emotional, physical, and sexual), neglect (emotional and physical), and household dysfunction (parental separation, domestic violence, substance misuse, mental illness, and incarceration within the home). The most common method of assessing exposure to adversity is the ACE Questionnaire, a widely used screening checklist that assesses exposure across these ten domains to better understand the risk factors associated with early adversity (Felitti et al., 1998). Higher ACE scores are associated with increased risk for chronic health conditions, mental health disorders, and substance use problems across the lifespan (Felitti et al., 1998). According to the Centers for Disease Control and Prevention, 63.9% of U.S. adults reported experiencing at least one adverse childhood experience, and 17.3% reported four or more ACEs, highlighting the widespread and cumulative nature of childhood adversity (Swedo et al., 2023). As the body of research on ACEs develops, researchers have begun to examine patterns of ACE exposure within families across generations.
Intergenerational trauma refers to the transmission of traumatic experiences and their psychological and relational effects across generations through biological, behavioral, and relational pathways (Hesse & Main, 2000). Caregivers with histories of ACEs often show disruptions in emotion regulation, reflective functioning, and caregiving sensitivity, which can impair parent-child attunement and attachment security (Dehghan Manshadi et al., 2023; Riser et al., 2025). These disruptions increase reliance on harsh or inconsistent parenting strategies and are associated with elevated child emotional and behavioral dysregulation (Bravo et al., 2023).
Impact of Intergenerational Trauma on Child Development
Parental ACEs have significant intergenerational implications, increasing a child’s risk for both direct trauma exposure and broader developmental and functional difficulties. Maternal ACEs have a strong intergenerational association with child trauma risk, with children of mothers reporting four or more ACEs demonstrating nearly fivefold increased odds of high ACE exposure compared to children of mothers with no ACEs (Schickedanz et al., 2021). ACEs in caregivers can disrupt core parenting capacities, including emotional availability, consistency, and affect regulation, which in turn shape children’s developmental trajectories (Zhu et al., 2025). These disruptions are associated with both socioemotional difficulties and alterations in neural systems involved in emotion regulation (Riser et al., 2025). Consistent with this pattern, children of mothers with histories of childhood maltreatment show elevated rates of both internalizing and externalizing symptoms across development (Bravo et al., 2023).
In early childhood, trauma-related symptoms are often expressed behaviorally. Young children are more likely to display impulsivity, emotion dysregulation, oppositionality, and aggression due to developmental limitations in language and self-regulation (Lieberman et al., 2015). Toddlers rely heavily on caregivers for co-regulation; when caregivers struggle with regulation related to their own trauma histories, this can contribute to cycles of mutual dysregulation within the dyad. Given these mechanisms, caregivers represent a critical target for intervention. Dyadic and trauma-informed parenting interventions have been shown to reduce both child internalizing and externalizing symptoms (Narayan et al., 2021). These approaches emphasize strengthening caregiver regulation and reflective capacity to improve responsiveness and interrupt intergenerational patterns of trauma, thereby promoting greater relational stability and resilience (Narayan et al., 2019).
Treatments for Toddlers
There are several evidence-based treatments for young children who are demonstrating behavioral and emotional challenges, including Child-Parent Psychotherapy, Parent-Child Care, and Parent-Child Interaction Therapy for Toddlers.
Child-Parent Psychotherapy
Child-Parent Psychotherapy (CPP) is an evidence-based, dyadic treatment designed to address trauma exposure and attachment disruption in children from birth through age five (Lieberman et al., 2015). Grounded in attachment theory, psychodynamic principles, trauma theory, and developmental psychopathology, CPP conceptualizes early childhood trauma within the context of the caregiving relationship (Lieberman et al., 2015). CPP is designed as a longer-term intervention, delivered in weekly sessions over approximately one year with families completing an average of 50 sessions. Implementation requires intensive training, with clinicians completing an 18-month training and consultation process to ensure fidelity to the model. Evidence suggests that CPP is associated with sustained improvements in children’s behavioral and emotional functioning, as well as reductions in maladaptive child representations of the caregiver-child relationship, and trauma-related symptoms (Alto et al., 2021). By directly addressing both the caregiver’s and child’s experiences of trauma within the relational context, CPP represents one approach to interrupting intergenerational patterns of trauma (Narayan et al., 2019).
Parent-Child Care
Parent-Child Care (PC-CARE) is a brief treatment intervention to address externalizing behaviors in children (ages 2–10 years) and their caregivers (Timmer et al., 2019). The model is structured as a short-term intervention (approximately seven sessions) and includes live coaching of caregivers while they interact with their child. Training in PC-CARE involves 30 hours of didactics and successful completion of six cases. Randomized controlled trial findings indicate that participation in PC-CARE is associated with significant improvements in children’s behavioral functioning and adaptive skills, as well as reductions in parenting stress and increases in positive parenting practices (Hawk et al., 2024). However, when the caregiver-child relationship is significantly disrupted, behavior dysregulation is severe, or caregiver capacity for co-regulation and skill acquisition is markedly limited, a more intensive or longer-duration evidence-based intervention may be warranted (Hawk et al., 2024).
Parent-Child Interaction Therapy for Toddlers
Parent-Child Interaction Therapy for Toddlers (PCIT-T) is an adapted version of Parent-Child Interaction Therapy (PCIT) that targets specific developmental characteristics of toddler-age children to strengthen caregiver and child attachment by increasing parental sensitivity and positive parenting strategies (Girard et al., 2018). The model emphasizes increasing caregivers’ reflective capacity, enhancing their own emotional regulation, and supporting their ability to respond to their toddler in developmentally sensitive ways. The length of treatment typically ranges from 12-18 sessions, depending on the child’s developmental needs and the caregiver acquisition of skills (Girard et al., 2018). Clinicians that can provide PCIT-T are certified in PCIT, obtain a 2-day PCIT-T training, year-long case consultation, and complete two PCIT-T cases. PCIT-T has demonstrated promising outcomes in improving both caregiver functioning and child behavior in young children. In a randomized controlled trial, caregivers receiving PCIT-T showed significant increases in positive parenting behaviors, parental sensitivity, and reduced negative language (Kohlhoff et al., 2024). In addition, caregivers reported reductions in parenting stress, and children demonstrated improvements in overall behavioral functioning. Compared to control conditions, PCIT-T produced stronger and more consistent gains across both parenting and child domains, supporting its utility as an early intervention for toddlers with emerging behavioral and relational difficulties (Kohlhoff et al., 2024). The emerging PCIT-T literature has begun to demonstrate the intervention’s applicability across diverse clinical presentations, including toddlers displaying autism spectrum disorder (ASD) traits, with case study findings demonstrating promising improvements in externalizing behavior, emotion regulation, and the parent-child relationship (Cibralic et al., 2020).
Using PCIT-T to Treat Trauma in Young Children
PCIT is a well-researched and supported treatment for trauma in children and families (Zhang et al., 2024). PCIT and its adaptations may offer a more time-efficient and comprehensive approach compared to CPP and PC-CARE. Additionally, there are widespread, international efforts to disseminate PCIT across settings (Pearl et al., 2012) and its adaptability, effectiveness, and potential has been demonstrated across settings and populations (Calderone et al., 2025). Thus, PCIT and its adaptations may be more easily accessible to families in need of early intervention services for childhood trauma. PCIT in families involved in child maltreatment yielded reductions in child behavior problems and trauma symptoms, as well as decreases in parenting stress, caregiver mental health difficulties, and harsh or negative parenting practices (Warren et al., 2022), including those with complicating caregiver factors (Druskin et al., 2023). As children under the age of three are three times more likely to experience abuse compared to older children (United States Department of Health and Human Services, 2019), there is a particular need to evaluate the use of interventions for parents and toddlers with exposure to trauma. Although PCIT has been effective in treating a variety of symptoms in families with trauma exposure, PCIT-T has not been studied specifically for children exposed to trauma or families with ACEs.
PCIT-T has several unique clinical features that may specifically target symptoms of traumatic stress in young children as well as the dyadic impairment that results from familial trauma. Notably, PCIT-T incorporates the majority of components identified by the Parent/Caregiver Trauma and Healing Coordinating Group of the National Child Traumatic Stress Network as critical for evidence-based child trauma treatment models, including engagement of a caregiver, routine assessment, a focus on parenting, dyadic co-regulation, attachment, relationship repair, caregiver/parental support, and emotional coaching (Kiser et al., 2020). Although PCIT and PCIT-T do not directly address trauma processing, this may be less relevant for toddler-aged children who, due to limited language capacities, often manifest trauma responses as externalizing behaviors. Similar to PCIT, PCIT-T has been demonstrated to improve child externalizing as well as internalizing symptoms (Kohlhoff et al., 2024). As PCIT-T is specifically aimed at facilitating a secure attachment between parents and their children, caregivers are taught to increase their sensitive and regulated responses to their child’s behaviors and emotions. Parents are taught to regulate and manage their own responses, allowing them to provide attention and reinforcement for positive child behavior. When children are able to rely on their parents for consistent and secure support, the attachment bond is able to serve as a foundation for emotional regulation.
Unlike PCIT, PCIT-T explicitly incorporates coaching to support parental understanding of child emotions. Parents are taught to scaffold their child’s emotional awareness through labeling emotions. As caregivers are coached to respond to their child’s emotions, they are also prompted to check in with their own thoughts and increase awareness of their emotions. This unique live coaching approach supports parents with their own trauma history in responding more effectively to child behavior.
Given that PCIT-T is targeted at key domains impacted by early childhood trauma, and may be more time-efficient and readily available in the community due to relatively broad dissemination, PCIT-T may be efficacious in targeting the combination of externalizing behaviors, parent-child relational difficulties, and traumatic stress that is present in families of toddlers who have experienced adverse events. As such, this paper explores the implementation of PCIT-T for a parent and child seeking treatment for a history of familial trauma and elevated child disruptive behavior.
Case Introduction
“Luca Miller” is a White, Latino 19-month-old male who was referred to an outpatient center specializing in trauma following a well-child visit with his pediatrician. Luca’s mother, “Ms. Miller,” described increased externalizing behaviors, including tantrums, separation anxiety, and trauma-reenactment behaviors. Luca has a trauma history significant for exposure to domestic violence and caregiver substance use. A comprehensive intake assessment was completed with Luca and his mother to evaluate Luca’s developmental and behavioral concerns, parent and child trauma history, and parental stress. Pseudonyms were used to protect the family’s confidentiality. Written informed consent for publication of their details was obtained from Ms. Miller.
Presenting Complaints
Ms. Miller indicated that Luca exhibited a variety of externalizing behaviors. Luca had frequent tantrums during which he yelled and threw himself onto the ground. Luca hit his mother daily, pinched her legs, and pulled his own hair when distressed. Additionally, Luca exhibited separation anxiety with his mother, including having tantrums when she left the room and clinging excessively to her. Ms. Miller expressed concern that Luca was mirroring the behaviors he saw from his father and sought treatment to obtain support in managing her responses to his behaviors and processing his trauma experiences in a developmentally appropriate way.
History
Luca was the product of a full-term, relatively uncomplicated pregnancy. During the first year and a half of his life, Luca was frequently exposed to his father’s verbal and physical aggression. In an escalation after his first birthday, Ms. Miller was repeatedly struck by Luca’s father while she was holding Luca. After she attempted to report this incident, Luca’s father, “Mr. Vargas,” attempted to strangle her while she was lying next to Luca in bed. In the aftermath of this incident, Mr. Vargas continued to harass Ms. Miller and was caught attempting to place a tracker on her vehicle. Ms. Miller was able to obtain a restraining order against Luca’s father and lived with Luca in a domestic violence shelter for several months as she received treatment for substance use. On two occasions, Luca crawled onto his mother and began to choke her, mimicking what he had witnessed between his mother and father prior to their separation. Ms. Miller’s concerns regarding Luca’s behavior began around 12 months of age.
Assessment
Assessment of Child Symptoms
Portions of the Diagnostic Infant and Preschool Assessment (DIPA; Scheeringa & Haslett, 2010) were administered as a semi-structured interview with Ms. Miller. The DIPA assesses symptoms of a variety of disorders (e.g., Posttraumatic stress disorder, Oppositional defiant disorder, Attention-deficit/hyperactivity disorder) in children aged 1 to 6 years. The DIPA uses developmentally sensitive probes and examples to differentiate normative early childhood behaviors from clinically significant symptoms, which is particularly important when assessing toddlers whose symptoms may vary widely across contexts. The interview format allows caregivers to provide detailed descriptions of symptom frequency, intensity, and impairment, supporting diagnostic decision-making consistent with DSM criteria adapted for early childhood. In Luca’s case, the DIPA provided a structured framework to assess trauma-related symptoms, including reexperiencing through behavioral reenactment, heightened arousal, and separation distress, while also screening for co-occurring concerns.
Luca’s mother completed the Ages and Stages Questionnaire, Third Edition (ASQ-3; Squires et al., 2009) for children aged 19 months to assess developmental functioning across key domains. Luca’s performance in communication, gross motor, fine motor, problem-solving, and personal-social domains fell within expected limits for his age and did not indicate a need for further evaluation at this time.
The Eyberg Child Behavior Inventory (ECBI) is a 36-item caregiver report of challenging behaviors in children from ages 2 to 16 (Eyberg & Pincus, 1999). As the ECBI is a standard measurement used weekly in PCIT, 8 items were identified to form a factor that best captures challenging behaviors in a developmentally sensitive manner to support weekly progress monitoring in PCIT-T (Phillips et al., 2023). Caregivers rate the frequency of their child’s behavior on a 7-point Likert scale and identify whether they consider each behavior to be problematic. On the ECBI toddler factor, Ms. Miller endorsed each item highly (Intensity = 53, Problem = 7). Using the normed values from the full ECBI items, Luca’s behavior fell in the clinically significant range (Intensity = 157, T = 67; Problem = 25, T = 73).
Assessment of Caregiver Symptoms and Functioning
The Life Stressor Checklist-Revised (LSC-R; Wolfe & Kimerling, 1997) is a caregiver-report measure used to assess lifetime exposure to a broad range of potentially traumatic and stressful events, including childhood adversity, interpersonal violence, and significant losses, and was administered to characterize Ms. Miller’s trauma history within the context of intergenerational risk. She was raised in a household marked by parental mental health and substance use difficulties. Notably, Ms. Miller experienced the death of her infant brother during her childhood, following a head injury, which she identified as a significant early loss. In addition to her recent experiences of domestic violence, Ms. Miller reported physical and emotional abuse throughout her upbringing. Ms. Miller identified her mother and grandmother as her primary sources of support, both of whom died within the past five years, representing significant and cumulative bereavement experiences.
The Parenting Stress Index–Short Form (PSI-SF; Abidin, 1995) is a caregiver-report measure assessing parenting-related stress across three domains: Parental Distress, Parent-Child Dysfunctional Interaction, and Difficult Child, as well as a Total Stress composite score. Ms. Miller’s scores were elevated across all subscales, indicating clinically significant levels of parenting stress. Elevations reflected high personal distress, perceptions of Luca as a highly challenging child, and increased stress related to parent-child interactions. These findings occurred in the context of substantial psychosocial adversity, including a history of homelessness, financial and food insecurity, and limited social support. Ms. Miller also endorsed feelings of inadequacy in the parenting role, expressing that she often feels she is “not a good mom,” underscoring her emotional distress and perceived parenting inefficacy.
Assessment of Dyadic Functioning
Parenting skills and parent-child interaction were assessed using the Dyadic Parent-Child Interaction Coding System, version 4 (DPICS-IV), a structured observational coding scheme that is a core assessment component of both PCIT and PCIT-T. This system is used to establish baseline interaction patterns as well as to monitor change in caregiver skill acquisition across treatment (Girard et al., 2018). In the present case, Ms. Miller and Luca were observed during a standardized pre-treatment interaction consisting of child-led play, parent-led play, and a clean-up task designed to elicit a range of caregiver demands and child compliance opportunities. At pre-treatment, Ms. Miller’s most frequent verbalizations were commands, with Luca complying to roughly 35% of these commands. During these structured play situations, Ms. Miller utilized 9 “Do” skills (total number of behavior descriptions, reflections, and labeled praises) and 98 “Don’t” skills (total number of questions, commands, and negative statements).
Case Conceptualization
Luca was a 19-month-old boy with a history of externalizing behaviors, aggression, and interpersonal trauma. Information gathered from the DIPA, caregiver-report questionnaires, and structured behavioral observations suggested that his presenting difficulties were best understood within the context of early exposure to domestic violence, disruptions in caregiver safety, and subsequent relational stress. At pre-treatment, Luca met criteria for a Trauma- and Stressor-Related Disorder and exhibited symptoms including trauma reenactment, hyperarousal, frequent tantrums, aggression, and separation anxiety. Notably, Luca’s reenactment of choking behaviors observed between his parents suggested that traumatic experiences were being expressed behaviorally rather than verbally, consistent with developmental expectations for a toddler with limited language abilities.
From a trauma-informed and attachment-based perspective, Luca’s difficulties appeared to reflect disruptions in his developing capacity for emotion regulation and his sense of safety within the caregiving environment. Exposure to violence, housing instability, prolonged separation from his father, and subsequent changes in caregivers and living circumstances likely contributed to heightened vigilance, distress during separations, and difficulty regulating strong emotions. These challenges appeared to be maintained, in part, through a transactional process in which Luca’s dysregulated behaviors increased caregiver stress, while Ms. Miller’s own trauma history, elevated parenting stress, and feelings of parenting inadequacy made it more difficult to consistently provide co-regulation and structured behavioral support during moments of distress.
PCIT-T was chosen as the intervention of choice as it is an age-appropriate treatment that has the potential for supporting parent-child dyadic functioning following familial trauma as well as offering parents tangible skills and supports to manage toddler externalizing behavior. Specifically, the intervention aims to strengthen caregiver sensitivity, increase positive parent-child interactions, improve caregiver capacity for co-regulation, and promote consistent, developmentally appropriate limit-setting. Given Luca’s age and symptom presentation, treatment focused on modifying caregiver-child interaction patterns and enhancing attachment security rather than relying on verbal trauma processing. By increasing Ms. Miller’s confidence, reflective capacity, and ability to respond predictably to Luca’s emotional and behavioral needs, PCIT-T was expected to reduce trauma-related distress, improve emotion regulation, and strengthen the parent-child relationship.
Course of Treatment and Assessment of Progress
Similar to standard PCIT, the toddler adaptation includes two sequential phases of treatment: Child-Directed Interaction-Toddler (CDI-T) and Parent-Directed Interaction-Toddler (PDI-T). The treating clinician holds a doctoral degree in clinical child psychology, has received training in PCIT-T from the treatment developers, has been involved in evaluative research and dissemination of PCIT-T, and is a certified Within-Agency Trainer in PCIT. Treatment integrity checklists from the Girard et al. (2018) PCIT-T book were used weekly to structure sessions and ensure fidelity to the model. At times, there was minor deviation from the outlined session structure to prioritize supporting parent regulation in session. Sessions were scheduled to occur weekly for 45-60 minutes; however, there were disruptions throughout the course of treatment due to Ms. Miller’s inconsistent work schedule and ongoing stressors. Ms. Miller completed a CDI-T “teach” (i.e., didactic) session and 10 CDI-T coaching sessions. In the second phase, Ms. Miller completed a two-part PDI-T “teach” session and 9 PDI-T coaching sessions. Ms. Miller frequently expressed worry and guilt over how her work schedule taxed her physically and emotionally and reduced opportunities for daily special time and skills practice. On average, she completed 3.5 days of special time practice each week, which offered her a clear and fairly consistent routine to enhance her connection to her son.
During CDI-T coaching sessions, Ms. Miller was supported in increasing her use of positive parenting skills, reducing negative verbalizations, and implementing active ignoring strategies when appropriate. CDI-T includes techniques to promote toddler regulation through “C.A.R.E.S.” skills (Girard et al., 2018). This framework emphasizes increasing physical proximity (“Coming in”) to signal safety and availability during moments of distress. Caregivers are supported in gently scaffolding their toddler’s coping by assisting with problem-solving around emotionally triggering situations (“Assisting”). They are also encouraged to provide clear verbal reassurance that the child is not alone in their emotional experience (“Reassuring”), while actively labeling and validating the child’s feelings to strengthen emotional understanding (“Emotionally validating”). Finally, caregivers offer verbal and physical comfort (“Soothing”) to help the child return to a regulated state (Girard et al., 2018). Collectively, these strategies enhance co-regulation and foster the gradual development of independent emotion regulation skills. Coaching sessions were characterized by longer check-ins at the start of session due to ongoing stressors and instability. Following the extended check-ins, Luca often had difficulty with the clinician leaving the room, resulting in heightened distress and requiring an immediate shift into coaching using C.A.R.E.S. skills to support regulation within the dyad. The clinician prompted Ms. Miller to sit next to Luca (Come in), rub his back (Soothe), and state that “Mommy is here with Luca” (Reassure). These in-the-moment coaching strategies, combined with increased use of P.R.I.D.E. (Praise, Reflection, Imitation, Description, Enjoy) skills, directly target trauma-related symptoms by reinforcing safety, predictability, and positive caregiver attention, which are critical for reducing Luca’s hyperarousal, aggression, and separation distress. By strengthening co-regulation and reshaping the caregiver-child interaction, these approaches help interrupt trauma reenactment patterns and support the development of adaptive emotional and behavioral responses.
Unique to PCIT-T, coaching of the adult C.A.R.E.S. skills provided a trauma-informed approach to parental skills building. C.A.R.E.S. coaching strengthened Ms. Miller’s awareness of her emotional responses to Luca’s hitting, particularly in the context of her domestic violence history (“He may be worried that you will leave the room. We have a plan for when he tries to hit you. Check in with how your body anticipates this behavior and how this may change your response to him”). As shown in prior research on how in-vivo coaching supports parents and children with trauma histories (Skowron & Funderburk, 2022), live coaching allowed Ms. Miller to notice the way that Luca’s behavior triggered her own responses and provided feedback to respond to him in a safe, adaptive manner.
The goal criteria for CDI-T were achieved during the 10th session where Ms. Miller was able to demonstrate 10 behavior descriptions, 10 reflections, and 15 labeled praises, exceeding the standard PCIT-T criterion of 10 labeled praises. At this point in CDI-T, Luca was consistently calm during the clinician’s transitions in and out of the room as well as during the end of session transition. He was frequently seeking comfort and support in his mother, indicating improvements in his attachment security. Ms. Miller was in tune with Luca’s and her own emotions, regularly labeling these feelings out loud. Luca’s ECBI had decreased to a toddler factor Intensity score of 40 and Problem score of 5 (Full ECBI: Intensity = 144, T = 63; Problem = 17, T = 63).
To begin the second phase of treatment (Parent-Directed Interaction-Toddler; PDI-T), Ms. Miller attended a PDI-T teach session to provide information about the Tell-Show-Try Again-Guide procedure used to increase caregiver consistency, effective command delivery, and follow-through with a structured process for supporting Luca’s listening. The Tell phase involves delivering a clear, developmentally appropriate command to support Luca’s understanding of expectations (e.g., “hand mommy the block”). If Luca did not comply, Ms. Miller was coached to move into the Show phase, in which she modeled the behavior and repeated the command. If Luca did not comply, she was guided to use “Try again” and restate the instruction in a neutral, regulated tone. When needed, the Guide phase involved gentle physical assistance to support compliance while maintaining emotional safety and reducing escalation. Over time, Ms. Miller demonstrated increased confidence in delivering commands without escalating emotionally or over-explaining. As treatment progressed, Luca showed increasing ability to comply with simple one-step commands following structured Tell-Show sequences, particularly when Ms. Miller maintained a calm and predictable tone.
Trauma-informed coaching remained central throughout PDI-T, particularly in supporting Ms. Miller’s interpretation of Luca’s dysregulated behaviors. The clinician supported Ms. Miller in noticing her own stress reactions when Luca threw toys or tried to hit her and coached her to maintain regulated responses during these episodes by reinforcing the predictable structure of clear instructions, calm follow-through, and reconnection and co-regulation following compliance. For example, the clinician frequently supported Ms. Miller with the phrase, “He is OK. He is learning that when he falls apart, you will keep it together.” This approach appeared to reduce her emotional reactivity over time and increased her sense of efficacy in managing Luca’s behavior safely. Ms. Miller met PDI-T goal criteria in the 9th coaching session. She noted that Luca was beginning to “listen more” and recover more quickly from tantrums when she remained calm and consistent. Clinically, Luca demonstrated improved transition tolerance and increased compliance with caregiver-directed tasks, particularly when commands were delivered with clear structure and paired with positive attention for compliance.
Luca’s interactions with his mother drastically changed, both qualitatively and quantitatively, by the end of treatment. During in-session special time, Ms. Miller consistently used high levels of “Do” skills (i.e., reflections, behavior descriptions, labeled praises). Ms. Miller was able to confidently and effectively deliver commands to Luca and appropriately support his behavior with guided compliance protocols as needed. Although fewer meltdowns occurred in session, Ms. Miller was able to quickly label Luca’s emotion and independently transition to C.A.R.E.S. skills to support his regulation. Changes in Ms. Miller’s parenting skills (as measured via the DPICS) are depicted in Figure 1. At the end of treatment, Ms. Miller’s ratings on the ECBI continued to improve. On the ECBI toddler factor, Ms. Miller’s responses resulted in an Intensity score of 25 and Problem score of 3. Using the normed values from the full ECBI items, Luca’s behavior fell in the normative range (Intensity = 116, T = 56; Problem = 10, T = 54). On the Parenting Stress Index–Short Form, all scores across domains fell in the normal range with the exception of the Parental Distress, which fell into the borderline elevation range. Although reduced, Ms. Miller continued to struggle with accessing social support and juggling responsibilities related to childcare, employment, and Luca’s needs. Parenting skills across time as measured by the DPICS. CDI = Child-directed Interaction-Toddler; CLP = Child-led play; DPICS = Dyadic Parent-Child Interaction Coding System; Don’t skills = Questions, commands, negative talks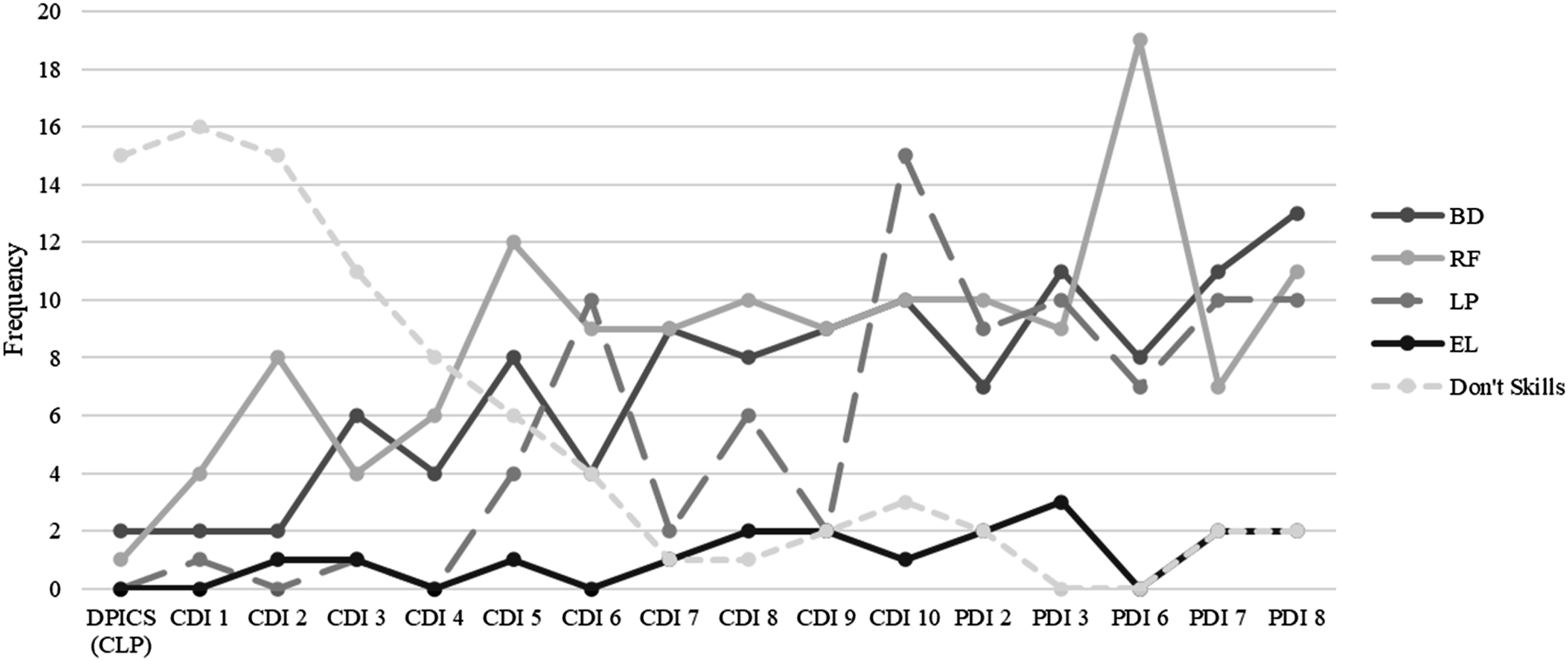
Complicating Factors
Given Ms. Miller’s trauma history and Luca’s exposure to domestic violence, particular emphasis was placed on how caregiver affect, tone, and physiological regulation influenced Luca’s threat response system during limit-setting. Ms. Miller was coached to monitor her own emotional activation when Luca displayed oppositionality or aggression, as these moments frequently evoked fear- and guilt-based responses linked to her history of interpersonal violence. The clinician explicitly supported her in differentiating past traumatic contexts from present-day parenting interactions, reinforcing that calm, structured limit-setting could function as a form of safety rather than threat within the dyad. Early PDI-T sessions were marked by Luca’s heightened distress during transitions into structured demands, particularly when limits were introduced following play-based interaction. In these moments, Luca often escalated to tantrums, including crying, dropping to the floor, and reaching for physical proximity to his mother. Ms. Miller initially responded with hesitation and occasional withdrawal from commands, reflecting both emotional discomfort and fear of escalating Luca’s distress. In one session, Luca threw himself on the floor during a tantrum, hitting his head on the table as he fell. Although Ms. Miller had become quite skilled in maintaining her composure and “under-reacting” while implementing the Tell-Show-Try Again-Guide sequence, she became visibly dysregulated and asked to stop the session. The clinician paused the coaching and joined Ms. Miller and Luca in the room, first supporting her physiological reaction through slowed breathing. Once she was more regulated, the clinician helped Ms. Miller to see the link between her emotional reaction to her past experience of the early loss of her infant brother due to a head injury, noting how Luca’s fall may have felt particularly alarming given this context.
Access and Barriers to Care
Several contextual and systemic factors complicated the course of treatment and presented barriers to consistent engagement. Ms. Miller experienced significant instability in employment throughout treatment, obtaining and subsequently losing two positions before transitioning through a third job change. Although these transitions were a positive long-term outcome, the shifting work schedules and competing demands contributed to a longer treatment duration and increased overall stress.
Ms. Miller also experienced ongoing financial strain, including periods of food insecurity and limited access to reliable transportation. These challenges were compounded by a motor vehicle accident in which she fell asleep at the wheel following consecutive work shifts, further disrupting daily functioning and increasing stress within the household. In addition, Luca required three hospital visits over the course of treatment, adding to caregiver burden and interfering with treatment continuity. Ms. Miller’s history of domestic violence and limited social support contributed to heightened stress, emotional reactivity, and challenges with regulation during parent-child interactions. Despite these barriers, Ms. Miller demonstrated sustained motivation for treatment and increased insight into the impact of her own experiences on her parenting. Importantly, she initiated individual therapy during the course of treatment and attended sessions approximately twice per month to address her own mental health needs, which appeared to support her capacity for reflection and engagement in PCIT-T.
Follow-up planning focused on maintaining gains in parenting skills, supporting continued caregiver mental health treatment, and reinforcing the use of PCIT-T strategies within the home environment. Ongoing stability in employment and engagement in individual therapy were identified as key protective factors to support long-term maintenance of treatment gains.
Follow-Up One Month After Treatment
At follow-up, treatment gains were maintained across behavioral, emotional, and relational domains. Ms. Miller reported continued use of PCIT-T skills, including emotion validation, positive reinforcement, and co-regulation strategies, and noted that Luca continued to demonstrate improved emotion regulation, fewer behavioral concerns, and reduced separation distress. Recently, Ms. Miller had shared some of the handouts and PCIT-T principles with Luca’s new daycare provider to support the consistency of skills used for managing Luca’s behavior. Although the family continued to experience ongoing financial and environmental stressors, Ms. Miller described feeling better equipped to manage setbacks as they arose and reported greater confidence in her ability to respond to Luca’s needs in a consistent and supportive manner. She also demonstrated a stronger understanding of developmentally appropriate expectations for Luca’s behavior, which appeared to reduce parenting frustration and support more effective responses to challenging situations. The parent-child relationship remained warm and positive, and ongoing stressors did not appear to interfere with the family’s continued use of treatment skills or maintenance of therapeutic gains.
Treatment Implications of the Case
Findings from the present case highlight several important clinical implications for practitioners working with toddlers exposed to trauma and their caregivers. First, this case illustrates that PCIT-T may be a particularly good fit for families in which trauma is expressed primarily through externalizing behaviors and relational dysregulation. Luca’s trauma history was most evident through aggression, reenactment, and separation distress rather than verbalized fear or narrative recall, which is consistent with developmental expectations for toddlers. PCIT-T’s emphasis on in-the-moment coaching, co-regulation, and behaviorally anchored parenting strategies allowed these symptoms to be addressed directly within the caregiver-child interaction, rather than requiring verbal trauma processing that would be developmentally inappropriate.
Second, PCIT-T offers a time-efficient, skills-based alternative to longer-term dyadic trauma treatments. Compared to models such as Child-Parent Psychotherapy, which often require year-long engagement, PCIT-T provides a structured and relatively brief intervention that can still target key domains affected by trauma, including attachment security, caregiver responsiveness, and child emotion regulation. This may be especially beneficial for families experiencing instability, such as inconsistent employment, financial stress, or transportation barriers, where sustained long-term participation may be more difficult. An additional advantage of PCIT-T as an intervention with strong implementation potential is the relative ease of monitoring treatment fidelity. Because PCIT-T is structured around discrete, observable caregiver behaviors and in-the-moment coaching strategies, treatment adherence can be evaluated continuously within sessions through direct observation of coaching behaviors and caregiver skill acquisition. This allows for ongoing fidelity monitoring that is relatively straightforward and low-burden, compared to interventions such as CPP, in which fidelity is not feasible to assess at the session level. In CPP, fidelity is conceptualized across broader intervention phases and “strands,” with structured forms that are more intensive and completed less frequently across the course of treatment. This may enhance both implementation scalability and the likelihood of sustained model adherence across service settings. In the current case, despite frequent disruptions and missed sessions, the structured and skills-focused nature of PCIT-T supported continued progress. Further, because PCIT-T reduces challenging child behavior relatively quickly, decreases in child externalizing behavior may be accompanied by a corresponding and timely reduction in caregiver stress.
Third, the live coaching format appears particularly valuable for caregivers with their own trauma histories. In-session coaching allowed the clinician to help Ms. Miller recognize and regulate her emotional responses to Luca’s behaviors as they occurred, facilitating more adaptive parenting responses in real time. This approach may be especially important for interrupting intergenerational patterns of trauma, as it targets both caregiver regulation and child behavior simultaneously. Clinicians would benefit from not only attending to parental skill acquisition but also to how caregivers’ trauma histories shape their interpretations of and reactions to child behavior. Integrating brief reflective prompts during coaching can enhance this process without shifting away from the behavioral framework of PCIT-T. However, it is important to note that Ms. Miller’s own individual therapy likely enhanced her capacity for reflection, emotional regulation, and consistency in implementing parenting strategies. For caregivers with significant trauma histories or ongoing psychosocial stressors, referral to concurrent individual treatment may strengthen overall outcomes and should be considered a key component of care planning.
Recommendations to Clinicians and Students
From a dissemination perspective, PCIT-T holds practical advantages. Because it is an adaptation of standard PCIT, clinicians already trained in PCIT can acquire competency in PCIT-T through relatively brief additional training and consultation. This may lower the barriers to implementation and support broader access to developmentally appropriate, trauma-informed interventions for young children. Expanding training opportunities in PCIT-T may therefore be a feasible strategy for increasing the availability of evidence-based care for toddlers and their families across community settings.
Finally, clinicians should anticipate and proactively address barriers to engagement when working with high-risk families. Flexible scheduling, consistent check-ins regarding basic needs, and an emphasis on achievable home practice may support retention and skill generalization. Even in the context of significant adversity, this case demonstrates that caregivers can make meaningful gains when provided with a structured, supportive, and accessible intervention.
Overall, PCIT-T represents a promising approach for addressing the intersection of early childhood trauma, externalizing behavior, and caregiver-child relational disruption. Its combination of developmental sensitivity, behavioral specificity, and scalability makes it a valuable option for clinicians working with young children and families impacted by adversity.
Footnotes
Ethics Considerations
This study was determined not to constitute human subjects research by the authors’ institution and therefore did not require Institutional Review Board approval. Written informed consent for publication of clinical details was obtained from the child’s caregiver.
Funding
This work was conducted as part of routine clinical services and did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to this case study, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the first/corresponding author upon reasonable request.