
Abstract
“Mycetoma” means a fungal tumor. Mycetoma is a chronic, granulomatous, subcutaneous tissue infection caused by both bacteria (actinomycetoma) and fungi (eumycetoma). This chronic infection was termed Madura foot and eventually mycetoma, owing to its etiology. Inoculation commonly follows minor trauma, predominantly to the foot and hence is seen more among the barefoot-walking populations, common among adult males aged 20 to 50 years. The hallmark triad of the disease includes tumefaction, fistulization of the abscess, and extrusion of colored grains. The color of these extruded grains in the active phase of the disease offers a clue to diagnosis. Radiology, ultrasonology, cytology, histology, immunodiagnosis, and culture are tools used in diagnosis. Recently, DNA sequencing has also been used successfully. Though both infections manifest with similar clinical findings, Actinomycetoma has a rapid course and can lead to amputation or death secondary to systemic spread. However, actinomycetomas are more responsive to antibiotics, whereas eumycetomas require surgical excision in addition to antifungals. Complications include secondary bacterial infections that can progress to full-blown bacteremia or septicemia, resulting in death. With extremely disfiguring sequelae, following the breakdown of the nodules and formation of discharging sinuses, it poses a therapeutic challenge.
History
The oldest description of this disease appears to date back to the ancient Indian Sanskrit text Atharva Veda, in which reference is made to pada valmikam, translated to mean “anthill foot.”
1
The history of mycetoma dates as far back as the Byzantine period (
It was also referred to by other names at various times 5 : morbus Tuberculosis pedis, fungus disease of India, Godfrey and Eyre’s disease, endemic degeneration of the bones of the foot, fungus foot, morbus pedis entophyticus-affection singuliere, and perforating ulcer of the foot.
Epidemiology
Native of the tropical, subtropical, and equatorial areas, the condition is seen in the belt between latitudes 30°N and 15°S commonly called “the mycetoma belt.” 6 The belt includes Sudan, Somalia, Senegal, India, Yemen, Mexico, Venezuela, Columbia, Argentina, and other countries. 7 In Sudan, the mycetoma homeland in the subtropics, 300 to 400 patients are diagnosed with mycetoma every year. 5 Central and South America and the middle or Far East between the latitudes 15°S and 30°N also harbor mycetoma. Increased worldwide travel has increased the incidence in temperate zones as well. 8
Mycoses are not notifiable in the United Kingdom; hence the incidence is unknown. Diagnosis of mycetoma in such uncommon locations requires a high degree of suspicion. 9 Mycetoma can also be uncommon in tropical areas such as Tunisia. 10 In India, maduromycotic mycetoma is commonest in western Rajasthan, but the ratio of prevalence of maduromycotic mycetoma to actinomycotic mycetoma has reduced from 4:1 to 1.9:1. 11 Red grain mycetoma caused by Actinomadura pelletieri is rare in Asia. 12 El Muttardi et al 9 and Malone et al 13 also noted sporadic cases in the Western world, especially the United States. In 1981, Actinomadura madurae infection was reported in the United States. 14
Environmental factors such as rainfall play an important role in the distribution of this condition. According to Mathur et al, 11 annual rainfall, nature of the soil, and presence of abundant sharp thorny vegetable matter influence the prevalence of the causative agents. Eumycetoma is more common in north India, with average rainfall less than 350 mm; whereas actinomycetoma is common in south India, with more than 600 mm of rainfall.11,15 Arid hot areas, with prolonged hot sunshine and scanty annual rainfall of 250 to 350 mm, are home to maduramycotic mycetomas. 6 Fungal grains grow in drier areas and actinomyces in the wet areas. 16
Causative Organisms
Thirty or more species of bacteria and fungi responsible for mycetoma have been identified. Etiologic agents include actinomycetes, eumycetes, eubacteria, and dermatophytes. 17
The etiological agents vary between regions. In northwest India M mycetomatis accounts for the maximum number of cases, followed by M grisea and Aspergillus nidulans. Mixed infection by both M mycetomatis and M grisea has been observed. 6 In Sudan. M mycetomatis accounts for 70% of the infections. 18 Eumycetomas were secondary to M mycetomatis, Leptosphaeria senegalensis, Pseudallescheria boydii, and Rhinoclediella atrovirensi. 16 P boydii (Scedosporium apiospermum) is the most common cause of mycetoma in the United States. 13 In south India, eumycetomas were secondary to M mycetomatis, Neoscytalidium dimidiatum, and Aspergillus flavus.
In Mexico City, the common etiologic agents were Nocardia brasiliensis, Nocardia asteroides, and M mycetomatis. 10 However, in Senegal from 1983 to 2000, Actinomadura pelletieri was the commonest, in addition to Actinomadura madurae and Streptomyces somaliensis. Neoscytalidium dimidiatum and A flavus were unusual pathogens. 19 See Table 1.
Commonly Implicated Organisms in the Etiology of Mycetoma and Their Grain Color
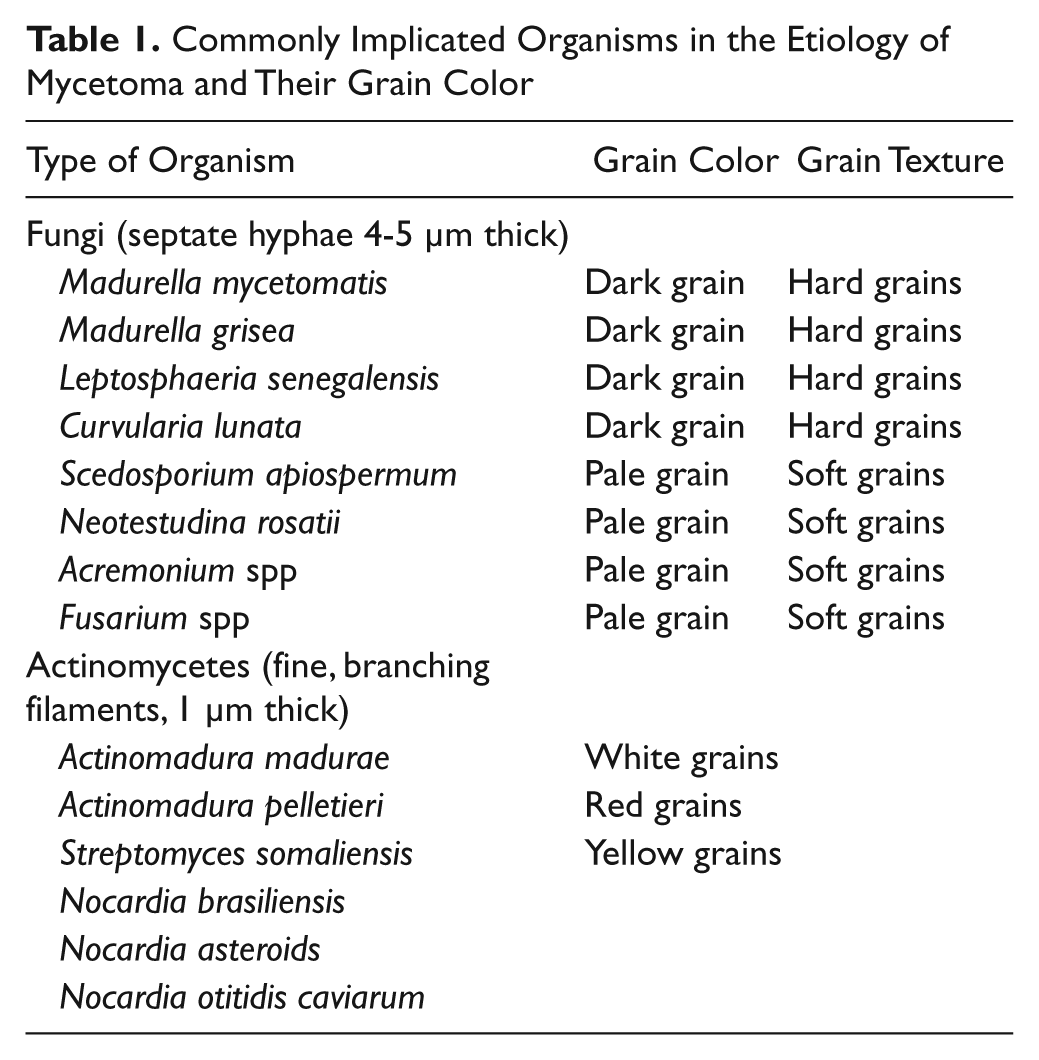
Other organisms implicated were Cylindrocarpon destructans 20 and Fusarium solani.21-23 An unusual Nocardia species, N veterana, was the first human pathogen in a clinical setting.24,25
Pathogenesis
Following inoculation of organisms, through thorn pricks or preexisting abrasions or trauma, these nonpathogens grow and survive through the production of grains. The matrix material is host derived along with some pathogens. Cells of the innate immune system attempt to engulf and inactivate the microorganisms. Abscesses containing grains are seen in association with granulomatous inflammation and fibrosis. This host response does not appear to be able to control infection. 1
No immune compromise has been documented prior to the onset of the disease. Genetic studies have identified polymorphisms linked with neutrophil function. It has been suggested that the greater frequency of disease in men is not completely explained by increased frequency of exposure to soil and plant material. 26
Progesterone has been shown in vitro to inhibit the growth of M mycetomatis, P romeroi, and N brasiliensis. In the study of N brasiliensis, estradiol limited disease produced in animals.1,27
Eumycetoma lesions are well vascularized. Hypoxia inducible factor 1 (HIF-1) regulates the transcription of vascular endothelial growth factor and adrenomedullin, 2 proangiogenic factors. Expression of HIF-1α protein was found to be upregulated in the fungal-infested tissue. These findings denote an important role of HIF-1 in the vascularization of eumycetoma lesion caused by M mycetomatis, which is upregulated by an oxygen-independent mechanism in the lesion. 28 A flowchart for diagnosis and management is shown in Figure 1.
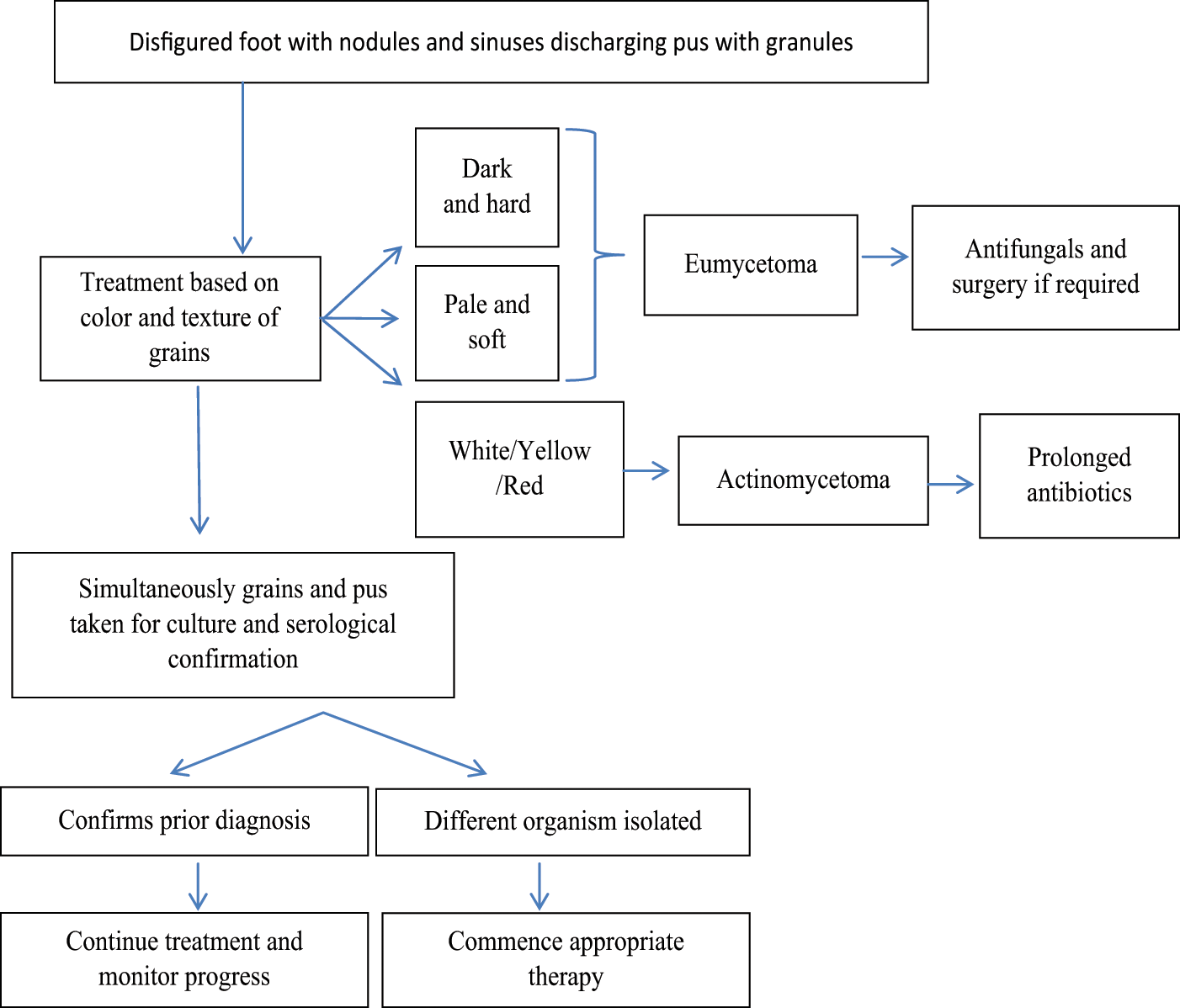
Flowchart for diagnosis and management
Clinical Features
Mycetoma is a chronic infection of exogenous origin, usually presenting as multiple nodules, with oozing and colored granules in the pus.6,10 The varying colors are black, yellow, and white.29,30
The incubation period varies from several weeks to months. 31 The incubation period is long and asymptomatic. Complaints of minimal pain are not uncommon. The infection spreads under the skin and forms subcutaneous abscesses. 32 Sinuses develop after 6 to 12 months and extend to involve the underlying fascia, muscle, and bone. See Figure 2.
The diagnostic triad
Tumefaction refers to the tumor-like mass that develops following the long and asymptomatic incubation period. Disease begins as a single, small, painless subcutaneous nodule. This nodule slowly increases in size, becomes fixed to the underlying tissue, and ultimately develops sinus tracts beneath the lesion. These tracts open to the surface and drain purulent material with grains. Grains are several millimeters in diameter and may be seen by close inspection of a gauze bandage covering the sinus tract. Progression to draining sinus tracts can take weeks, months, and even years, occurring more rapidly in actinomycetoma.33-35
Common risk factors for acquiring the fungal infection are the following:
A minor trauma due to a thorn prick or abrasion inoculates the organism into the skin6,10,11
People walking barefoot 10
Individuals in the age-group of 21 to 30 years are at high risk, because of the need to go out and work in the open environment
Men are more commonly affected (sex ratio 1.61:1) 6
Agricultural work and farming are high-risk occupations 6
Environmental factors: rainfall, temperature, soil, thorny sharp vegetable material
Social factors: walking barefoot and/or carrying goods on the back6,16
Homelessness 13
AIDS patients 13
Immunocompromised individuals, for example, post–renal transplant patients 36 and diabetic patients 13 may develop invasive infection
Actinomycotic mycetomas expand fast, are invasive, and have more sinuses than eumycotic variants. 31 Atypical presentations without grains in the discharge or sinuses have been reported due to M mycetomatis.36,37
Following a minor trauma, painless swellings develop after a prolonged and asymptomatic incubation period, with intermittent discharge of pus. A study conducted in Senegal of 130 patients revealed that they consulted for restricted movement or pain secondary to the expanding tumor on an average 4.8 to 5.6 years after inoculation. 16 Persisting pain due to bone invasion or secondary bacterial infection (SBI) is common. 38 Tumoral or pseudocystic presentations have been reported due to A pelletieri. 39
Fahal and Hasan 40 and Diallo et al 39 noted that the commonest site of occurrence is the foot in 70% and 80% of the cases, respectively. (Fahal, 2004) Hand is the next most common site. 31 Bedi et al 12 in 1978 reported the first case of red grain mycetoma on the scalp, in India. Axillary and thoracocervical lesions have occurred. 12 Nonvenereal, perineal lesions, 41 slow-growing facial swellings, subcutaneous frontal skull swelling, proptosis, nasal blockage, epistaxis, discharging leg sinuses, flank mass, convulsion, and pain have also been presenting complaints. 42 Mycetoma is uncommon in children. 10 Lymphatic spread occurs rarely.
Diagnosis
Diagnosis of mycetoma requires a detailed clinical history and physical examination (see Appendix). Particular attention should be given to the duration of the disease, the presence of sinuses, discharge of grains, and color of the grains, the presence or absence of pain, and involvement of the regional lymph nodes. X-ray and laboratory tests help confirm the diagnosis. Cultures are the gold standard in the diagnosis and management of mycetoma. Rarely, when cultures are falsely negative, actinomycetoma can be diagnosed on clinical and histopathological grounds.10,36,43,44
Investigations
Ultrasonic Imaging of Mycetoma
Characteristic features include numerous, isolated sharp hypereflective echoes corresponding to the grains in the lesion in eumycetoma. In actinomycetoma, the grains are less distinct because of their smaller size and consistency. The technique is safe, simple, accurate, and useful in planning surgical treatment.
Fine Needle Aspiration Cytology of Mycetoma
Cytology shows polymorphous inflammatory cells consisting of a mixture of neutrophils, lymphocytes, plasma cells, histiocytes, macrophages, and foreign-body giant cells and grains. In sections, the grain is closely surrounded by neutrophils, causing fragmentation. Surrounding this, monocytic cells and giant cells are seen. This is surrounded by granulation tissue rich in fibroblasts and blood vessels. The technique is simple and sensitive and can be tolerated by patients. 45
Microbiology
The grains are the source of the culture, and they should be alive and free of contaminants. They are obtained by deep surgical biopsy, inserting sterile cotton swabs into the sinus tracts or percutaneous aspiration of closed or inactive fistulae. Grains should be sent immediately in sterile containers to the laboratory for culture. Culture media include Sabouraud, blood agar, malt extract agar, MacConkey agar, and mannitol salt agar plates, and the culture is incubated aerobically at 37°C for 24 hours. 46 Actinomycetes take 48 to 72 hours to grow on culture plates. Therefore, it is essential to mention on the request form the need for the culture and the organism suspected. 47
Histopathology
Multiple sections of deep biopsies, including the subcutaneous tissue, should be taken from areas with purulent discharge. A diagnostic finding would be the presence of 5 to 7 grains per cavity, walled by fibrous tissue.
Eumycetoma: Sections from indurated skin show extensive granulation tissue containing abscesses, leading to sinuses. A neutrophil zone surrounds the grains, forming granulomas. 48 These granulomas are surrounded by palisading histiocytes beyond which a mixed inflammatory infiltrate comprising lymphocytes, plasma cells, eosinophils, macrophages, and fibroblasts is seen. The occasional multinucleated giant cell was also seen. 8 Later, fibroblasts predominate.
Actinomycetoma: Chronic abscess with polymorphs surrounding granulation tissue and fibrosis is seen. Organisms form matted colonies (granules or grains).These sulfur granules maybe 20 µm to 4 mm in diameter. They are gram-positive. The peripheral filaments often terminate in a club. A Splendore–Hoeppli reaction may be found around the grain. (Homogeneous, eosinophilic material coats the grains.)
In 1908 Splendore and in 1932 Hoeppli individually described eosinophilic coating of microorganisms visible on histological study. Subsequent descriptions refer to the Splendore–Hoeppli phenomenon, which may appear as radiating eosinophilic spokes or as thick eosinophilic rings. The Splendore–Hoeppli phenomenon has been reported in association with a variety of fungal and parasitic infections (especially by helminths and schistosoma eggs) and is particularly striking in actinomycosis, mycetoma, and botryomycosis.
They represent antigen–antibody precipitates with immunoglobulin; the third component of complement; cellular debris from plasma cells, macrophages, lymphocytes, and eosinophils; and eosinophil granule major basic protein, which constitutes the core of the granule and is toxic to the microorganisms. The immunoglobulin component of the eosinophilic matrix presumably represents a localized attempt at containment on the part of the host. Whether this degree of immunological responsiveness is ultimately helpful or harmful to the host remains to be elucidated
The grain morphology of some commonly isolated organisms is as follows (see Figures 3-5):
Madurella mycetomatis: Large granules (5 mm or more) with interlacing hyphae embedded in interstitial brownish matrix; hyphae peripherally arranged radially with numerous chlamydospores
Petriellidium boydii: Eosinophilic, lighter in the center; numerous vesicles/swollen hyphae; peripheral eosinophilic fringe; other pale eumycetomas have a minimal fringe and contain a dense mass of intermeshing hyphae
Actinomadura madurae: Large (1-5 mm and large) and multilobulate; peripheral basophilia and central eosinophilia or pale staining; filaments grow from the peripheral zone
Streptomyces somaliensis: Large (0.5-2 mm or more) with dense thin filaments; often stains homogeneously; transverse fracture lines
Nocardia brasiliensis: Small grains (approximately 1 mm); central purple zone; loose clumps of filaments; gram-positive delicate branching filaments breaking up into bacillary and coccal forms; gram-negative amorphous matrix 8
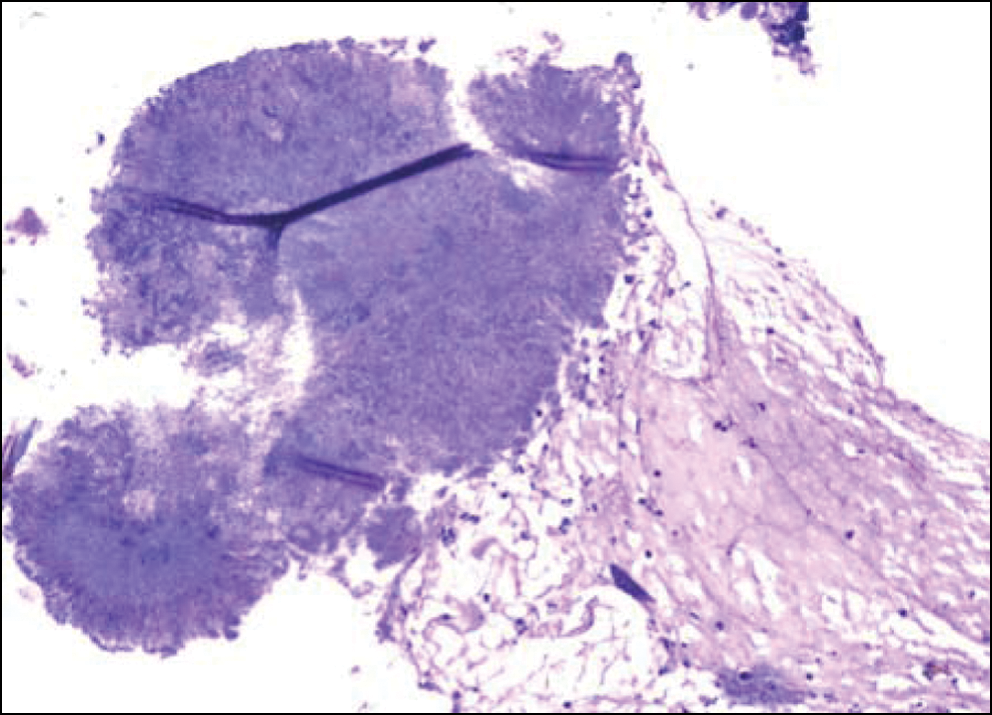
Actinomycetoma: Section showing filamentous aggregates of actinomycetes surrounded by scattered inflammatory cells (hematoxylin and eosin, ×200)
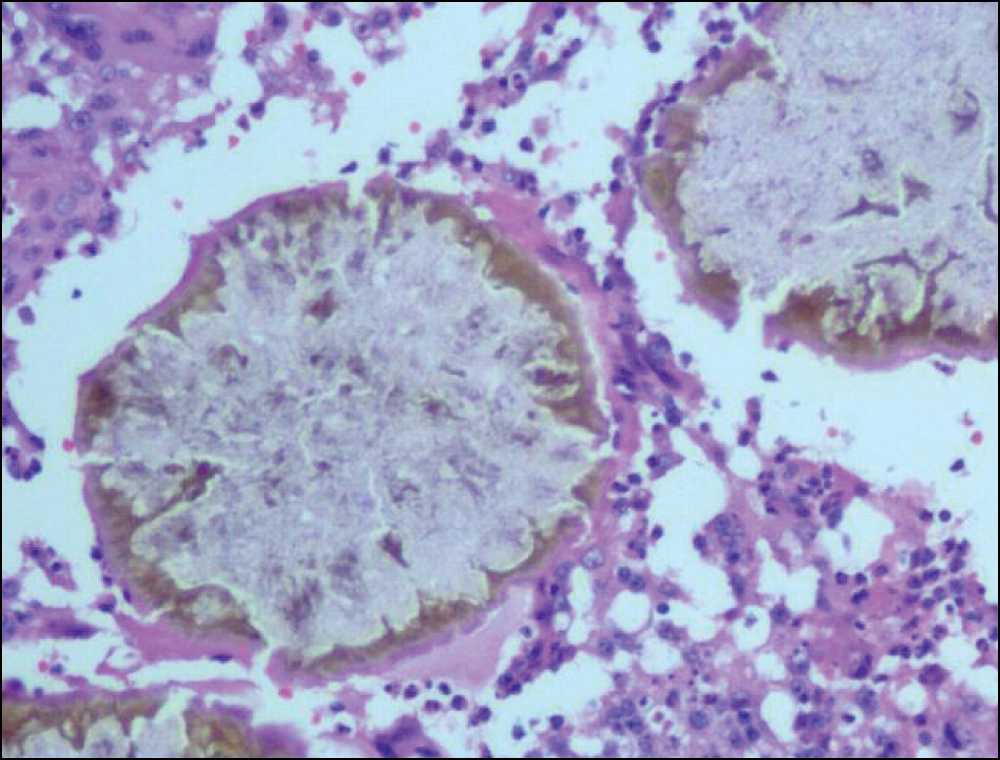
Eumycetoma: Pigmented fungus with Splendore–Hoeppli reaction (hematoxylin and eosin, ×200)
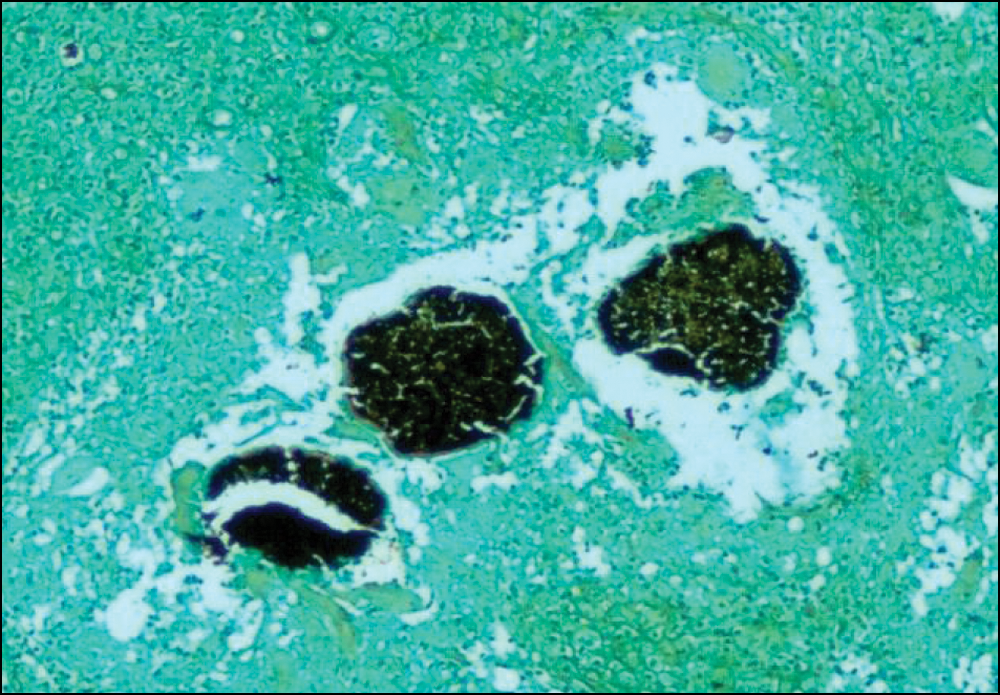
Eumycetoma: Gomori methanamine silver stain showing positive staining for the fungus (×100)
Gram staining is useful in differentiation.8,22,35 Dark (black) grains are found only among the eumycotic mycetoma, because of the pigment melanoprotein. 49 The gram stain is more useful in actinomycetoma, and Gomori methenamine silver and periodic acid-Schiff stains are better in eumycetoma. 23 Staining with lactophenol blue allows differentiation between the thin and thick filaments. 35
Stained sections usually show three types of tissue reaction to the organisms:
Type I: The grain is surrounded and invaded by neutrophil infiltrate
Type II: A vascular layer containing foamy macrophages, lymphocytes, plasma cells, and giant cells containing fragments of the grain
Type III: Formation of pure epithelioid granuloma
Biopsies are usually fixed in 10% formal saline. 50
Serodiagnosis in Mycetoma
Serodiagnosis is of great help in identification and classification of the various organisms.
Counterimmunoelectrophoresis: A laboratory technique used to evaluate antigen antibody binding. It is similar to immunodiffusion but with the addition of an applied electrical field across the diffusion medium, usually an agar or polyacrylamide gel. The effect is rapid migration of the antibody and antigen out of their respective wells toward one another to form a line of precipitation, or a precipitin line, indicating binding.
Immunodiffusion: A technique involving diffusion of antigen or antibody through a semisolid medium, usually agar or agarose gel, resulting in a precipitin reaction. Precipitin lines or bands form where the concentration of an antigen and antibody are serologically equivalent.
Enzyme-linked immunosorbent assay (ELISA): A simple and highly sensitive assay based on the specific recognition of the target compound (analyte/antigen) by antibodies that bind to the compound. The antigen–antibody complex is detected with the aid of an enzyme-labeled antibody or antigen. On addition of a noncolored reagent the enzyme produces a color reaction where the color intensity is directly or inversely proportional to the concentration of the analyte in the sample.
These tests are not very sensitive, and if antigens are not pure, it can be negative in early cases. ELISA is highly sensitive for detecting antibodies, but cross-reactivity is unavoidable.51,52
Bone Scan, Computed Tomography Scan, and Magnetic Resonance Imaging
Radiological studies are gaining importance in diagnosis and planning of management. They help in accurately identifying the location of the lesion, planning of surgical management, and also monitoring of its response to treatment in the form of lesion shrinkage. They are widely available but expensive. 50 In a resource limited setting, this investigation can be used for cases not identifiable by other modalities.
DNA Sequencing
DNA sequencing identified a case of Fusarium solani infection by analysis of fungal internal transcribed spacers 1 and 2 and 5.8S ribosomal DNA regions. 21 16S ribosomal RNA gene sequencing identified an unusual Nocardia species, N veterana, by biochemical characterization for the first time. 24
Radiology
Davies reported a variety of radiological changes in Madura foot.
The early change: Soft tissue granuloma, appears as a single or multiple soft tissue shadows with calcification and obliteration of the fascial planes. The cortex loses definition due to external compression by the granuloma leading to bone scalloping.
The disease development: When the bone is involved, there may be a periosteal reaction. This will lead to the formation of sun ray appearance and Codman triangle, an appearance that may be indistinguishable from that of osteogenic sarcoma.
The late stage: Formation of cavities that may be multiply punched out throughout an otherwise bone of normal density. These cavities are large in size, few in number, with well-defined margins in eumycetoma. The cavities in actinomycetoma are usually smaller in size, are numerous, and have no definite margins.
The terminal stage: Gives a melting snow appearance. 53 Osteogenic sarcoma and tuberculosis are differential diagnoses on radiological examination. 40
X-Ray
Madurella mycetoma appears as localized, large, well-defined, black fungus balls. 54 Plain radiographic classification is useful in monitoring treatment response. Stage 0 shows soft tissue swelling without bone involvement. Stage 1 shows the pressure effects of the expanding granuloma on normal bones. Stage 2 is when there is periosteal reaction of the bone without bone invasion. In Stage 3 there is cortical erosion and medullary invasion. Stage 4 is when infection spreads longitudinally along a single ray. Horizontal spread along a single row represents Stage 5. In Stage 6 there is multidirectional and uncontrolled spread. 32
A study conducted in Saudi Arabia also revealed similar changes on X-rays and computed tomography (CT) scans (Somotom DR-2 machines). Magnetic resonance imaging (MRI) is useful for studying the soft tissue invasion. The method of choice for the pretherapy assessment of bone involvement is CT scan. 5 The dot in circle sign is highly specific for mycetoma. The fungal grains appear as hypointense foci within high-intensity spherical lesions representing the surrounding granulomata on T2-weighted, short inversion time inversion-recovery, and T1-weighted fat-saturated gadolinium-enhanced images. 55
Eumycotic lesions form few large cavities ≥1 cm in diameter, whereas actinomycetes form many small cavities giving a moth-eaten appearance. 56
Osteoporosis at and distal to the affected part is sometimes observed because of disuse atrophy or external compression of the bone and its blood supply by the granuloma.
Complications
Due to Disease
Secondary bacterial infections
In Sudan, Staphylococcus aureus, Streptococcus pyogenes, and Proteus mirabilis were common secondary invaders. 46 Eumycetomas are susceptible to SBIs, contrary to popular belief that the antibiotics produced by the fungi keep it sterile.40,57 The lower incidence of SBI in actinomycetomas is because these patients receive streptomycin as part of antimicrobial therapy. 46
Dorsolumbar actinomycetoma with spastic paraplegia
Three out of 130 patients in Senegal who had back injury later developed dorsolumbar actinomycetoma and neurological complications such as spastic paraplegia. 16 Contiguous spread and visceral involvement occur. 43
Delayed presentation
Asymptomatic and chronic course leads to the disease presenting at an advanced stage for the first time. 8
Due to Therapy
Toxicity may occur due to prolonged antimicrobial or antifungal therapy, anemia, or leucopenia.
57 Drug resistance may be seen since treatment is of prolonged duration, 58 especially in bone and visceral involvement and Dapsone syndrome.
During Diagnosis
Multiple surgical biopsies are sometimes required for culture and staining to arrive at the etiological diagnosis.
This increases the morbidity and delays diagnosis and treatment. 56
Treatment
The primary step is the distinction between eumycetoma and actinomycetoma. 16 A tentative diagnosis based on the grain color is sufficient to commence therapy. Melanoid grains are always caused by fungi and ochroid or pale grains by actinomycetes.
Treatment of Actinomycetoma
Actinomycetoma is amenable to medical treatment with antibiotics and other chemotherapeutic agents. Chemotherapy causes radiological improvement consisting of remolding, absorption of the sclerotic bone, and reappearance of the normal trabecular pattern. Combined drug therapy is always preferred to a single drug in order to avoid drug resistance and eradicate residual infection.
Therapeutic end point is clinical, serological, and radiological cure. The time taken for this rarely exceeds a year. Preoperative and postoperative chemotherapy improves the prognosis. 2 Dieng et al 16 reported complete cure with antibiotics in 66 patients with actinomycetoma in Senegal.
Trimethoprim–sulfamethoxazole (TMP-SMX) and diaminodiphenylsulfone (DDS; 1.5mg/kg twice daily) were an effective combination.
Failures were successfully treated with amoxicillin/clavulanate. 10 Gentamycin and cefotaxime, 37 amikacin, streptomycin, kanamycin, or phosphomycin may be added. 59
Nocardia brasiliensis infection in a 10-year-old responded to TMP-SMX with DDS and rifampicin. 60
We add a word of caution: The patient who requires dapsone should be tested for glucose-6-phosphate dehydrogenase deficiency before commencing therapy.
The Welsh regimen, which proposed the use of amikacin with TMP-SMX in the treatment of actinomycetoma, was first published by Welsh et al 61 in 1987. In 2011, Palit et al 43 reported a dramatic response of mycetoma to the modified 2-step regimen. An intensive phase follows, with intravenous gentamicin 80 mg 12th hourly and cotrimoxazole 320/1600 mg twice daily orally for 4weeks. A maintenance phase is next, with oral cotrimoxazole and doxycycline 100 mg twice daily
Addition of rifampicin to the Welsh regimen showed no recurrences for up to 18 months. 62 If resistant, streptomycin can be used. 63
Streptomyces species were responsive to novobiocin, gentamycin, and doxycycline.
Fusidic acid, bacitracin, streptomycin, cephaloridine, clindamycin, ampicillin, rifampicin, and tetracycline were less effective. Resistance to amphotericin B, penicillin, and sulphamethoxazole was noted. 64
In advanced bone or visceral involvement, with streptomycin sulphate (14mg/kg/d), dapsone, TMP-SMX, sulfadoxine-pyrimethamine, rifampicin, and imipenem, were effective. 59
In infections secondary to N brasiliensis, amoxicillin–clavulanic acid (500 mg–125 mg) is beneficial in preventing relapses.58,65
The unusual N veterana responded to the combination of intravenous imipenem/cilastatin and amikacin along with oral clarithromycin and minocycline. 24
The prolonged duration of treatment, a major drawback, was shortened by a 2-step regimen initiated by Ramam et al to hasten improvement and promote compliance.
Intensive phase: Penicillin + gentamycin + co-trimoxazole (5-7 weeks), followed by amoxicillin + cotrimoxazole (2-5 months)
Treatment of Eumycetoma
Eumycetoma can be treated with the following
Ketoconazole: 400-800 mg daily
Itraconazole: 400 mg itraconazole daily. P. boydii (S. apiospermum) responded
Good response has been noted with Terbinafine
Eumycetoma treatment usually extends into many years. They are well circumscribed8,17 and combined medical and surgical treatment is the gold standard for management. 66
Madurella mycetomatis
Madurella mycetomatis has responded to
Surgery after therapy with griseofulvin and penicillin. 57
Oral itraconazole 400 mg daily for 3 months; followed by 200 mg daily for 9 months (the dose reduction slowed down the healing), leading to lesion encapsulation, thus making surgical removal easy. Recurrences have been noted.10,48
Ketoconazole
Amphotericin B
Tea tree oil but not Artemesinin derivatives; has been found to penetrate the skin and help treat this fungal infection. 67
Echinocandins: caspofungin, anidulafungin, and micafungin were unsuccessful in treating it. 68
Kaliswaran et al 64 in 2003 treated 25 patients with mycetoma foot. The actinomycetomas received 4 different regimens.
Regimen 1: Welsh regimen (TMP-SMX with Amikacin)
Regimen 2: TMP-SMX with Inj. Streptomycin
Regimen 3: TMP-SMX with Rifampicin
Regimen 4: TMP-SMX monotherapy
The eumycetomas received ketoconazole (regimen-A) and itraconazole (regimen-B).
Therapeutic outcome in actinomycotic mycetoma was good with the Welsh regimen. In eumycetoma, complete surgical excision following antifungal therapy at an early stage gave the best results. 64 Carbapenems, oxazolidinones, and triazoles have emerged as promising therapeutic options. 69
Surgery aims at complete removal or size reduction as an adjunct to medical treatment. Local anaesthesia is contraindicated because of the disease extent. Eumycetomas are well encapsulated, and if ruptured, they lead to recurrence by invasion. Actinomycetomas are ill defined, and hence healthy tissue should always be excised with the lesion. Simple bone curettage is recommended for localized bony lesions. Flooding the wound with tincture of iodine can destroy missed grains. Wound closure may require skin grafting. If the wound is left open, postoperative wounds should be dressed with 2% iodine in glycerin to destroy any fungal elements.
Repeated excisions of the diseased tissue, including bone, may be carried out several times to avoid the social consequences of amputation. When surgery is inadequate, amputation becomes inevitable.
Follow-up
Mycetomas require prolonged systemic treatment. These have a propensity for liver damage. Patient review every 8 weeks to assess liver function also helps assess prognosis. Regular follow-up also aids early detection of recurrence.
The disease can leave behind severe scarring and in extreme cases disability. Psychological support and occupational rehabilitation are vital in the multidisciplinary management of mycetoma.
Criteria for Cure
Disappearance of the subcutaneous mass and healing of sinuses are the main criteria. Three consecutive negative counterimmunoelectrophoresis tests 1 month apart are required. Normal bone on radiology has to be attained. There has to be absence of hyperreflective echoes and cavities on ultrasonology. No grains should be found on fine needle aspiration cytology.
Differential Diagnosis
Chronic bacterial osteomyelitis, chronic osteitis, tuberculosis, Buruli ulcer, other deep fungal infections such as blastomycosis or coccidiomycosis, leishmaniasis, yaws, and syphilis may be considered
Prognosis
Subcutaneous bacterial actinomycetoma is completely amenable to antibiotic therapy, whereas fungal infections have a high rate of recurrence. The eumycetomas require surgical debriding in addition to antifungals. High incidence of SBI can cause increased pain, disability, and septicaemia. This may become fatal if untreated.12,46
Prevention
No prophylaxis or vaccine is available against this disease. Health education of susceptible population about protective footwear and other risk factors can go a long way in curbing the incidence of mycetomas. Improvement in hygienic practices and living conditions can reduce this disfiguring infection. Immunocompromised populations are susceptible, and great care has to be taken to avoid nosocomial spread.
Quality of Life
The life quality index of mycetoma patients were studied in the Mycetoma research centre in Khartoum, Sudan, in 2008 using a Glasgow Health Status Inventory. The disease negatively affects the patients’ daily routine, profession, and social life.
Conclusion
Mycetoma is the clinical manifestation of a chronic, exogenous bacterial or fungal infection and is often at an advanced stage when diagnosed. Its asymptomatic nature leads to the patient ignoring the progression.38,70 This foot pathology has increased in prevalence in the United States and Europe because of international travel and migration. 13 Morphological similarities and unusual locations and presentations pose diagnostic difficulties. 39 Culture is the gold standard for diagnosis. Radiological diagnosis is not accurate, 53 and hence, species identification and susceptibility testing guide therapy. ELISA is useful in community surveys.
SBIs are common in eumycetomas, causing pain and increasing the morbidity. 46 Treatment regimens are currently based on expert opinion because no randomized controlled trials have been performed. Most patients receive 3 to 24 months of therapy to obtain an adequate response. 8 Treatment response is better for actinomycetomas with chemotherapy than for eumycetomas with antifungals and surgery. 10 Surgical management is recommended for excising small localized lesions and debulking of massive lesions for better response to medical treatment and of lesions that become encapsulated by medical treatment. Amputation, if done, is for very advanced lesions and is recommended as a lifesaving procedure.
Footnotes
Appendix
Acknowledgements
We would like to acknowledge Dr Sandhya Sridhar, Professor, Department of Pathology, Sri Ramachandra University and Prof Sandhya Sundaram, MD, Department of Pathology, Sri Ramachandra University, for providing us with the histopathology slides.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.