
Abstract
The manner in which high-energy transfer limb injuries are dressed can alter the wound environment through manipulation of the bacterial burden, thus minimizing tissue degradation and influencing healing potential. Infection is the principal complication of such wounds, and antiseptic soaked gauze is accepted in early coverage of extremity wounds despite a lack of evidence to support this practice. There has been resurgence in the use of silver in acute wounds, through dressings manipulated to deliver sustained elemental silver to the wound interface. In vitro and in vivo experimentation of silver dressings are characterized however by methodological compromise, primarily through lack of similarity of models to the physiology of the healing wound. Results from in vitro studies caution against the use of silver because of evidence of cytotoxicity, but this is not reproduced in in vivo or clinical experimentation, leading to ambiguity. Review of silver dressing application in burns and chronic wound studies fails to support its use over other dressing systems. Similarly, evidence for the use of silver in acute limb wounds is lacking. This article provides a comprehensive overview of the use of silver dressings in acute wound care and highlights in particular the paucity of evidence regarding its routine use in extremity injury.
Wound care and infection are inextricably linked to the overall morbidity and ultimate outcome of significant limb injury,1-5 and the material chosen to cover a wound has an impact on the bacterial burden contained within. Combined with the increasing resistance of wound pathogens to antibiotics 6 and the impact of infection on outcome from injury, the need for continued investigation of alternative antimicrobial agents is transparent.
Sterile cotton gauze either dry, soaked in saline or antiseptic, and applied to the wound surface is in widespread use, 7 although scientific rationale for this practice is lacking.4,8 Although silver dressings are widely used in nonhealing wounds, proof of superior efficacy either in this role or in the setting of acute extremity injury is scarce,9,10 and paradoxically, evidence is available for potential cytotoxicity of silver wound preparations. Despite a lack of proven efficacy and concerns over cytotoxicity, proprietary recommendations for, and anecdotal use of, silver-lined fabric dressings in acute traumatic and surgical wounds exist. 11
A range of proprietary silver dressings are available for use in wound care, the majority incorporating the metal into an alginate or hydrocolloid base for the management of nonhealing wounds. 12 Widely used, such preparations are nevertheless contraindicated in large open wounds partly because of the inability to sustain silver release. 13 Fabric-based silver-impregnated dressing systems subsequently have been introduced as a more practical alternative to traditional silver wound therapies in extremity wounding and burns care. To review the experimental evidence for the use of silver dressings applicable to acute musculoskeletal wounds such as those resulting from combat or high-energy civilian trauma, we carried out an electronic search of the MEDLINE database using the PubMed search engine limited to manuscripts published in English until August 2011. Medical Subject Headings of wounds and injuries, bandages, silver; and wound infection were entered, and Boolean operators were used to construct a search strategy. Although the nature of the studies reviewed preclude systematic review or meta-analysis, the fate of retrieved abstracts is presented (Figure 1). Articles initially missed in this search were obtained from manual searching of the bibliography of retrieved studies. Experimental articles were excluded from further analysis if silver fabric dressings were not included as an intervention.
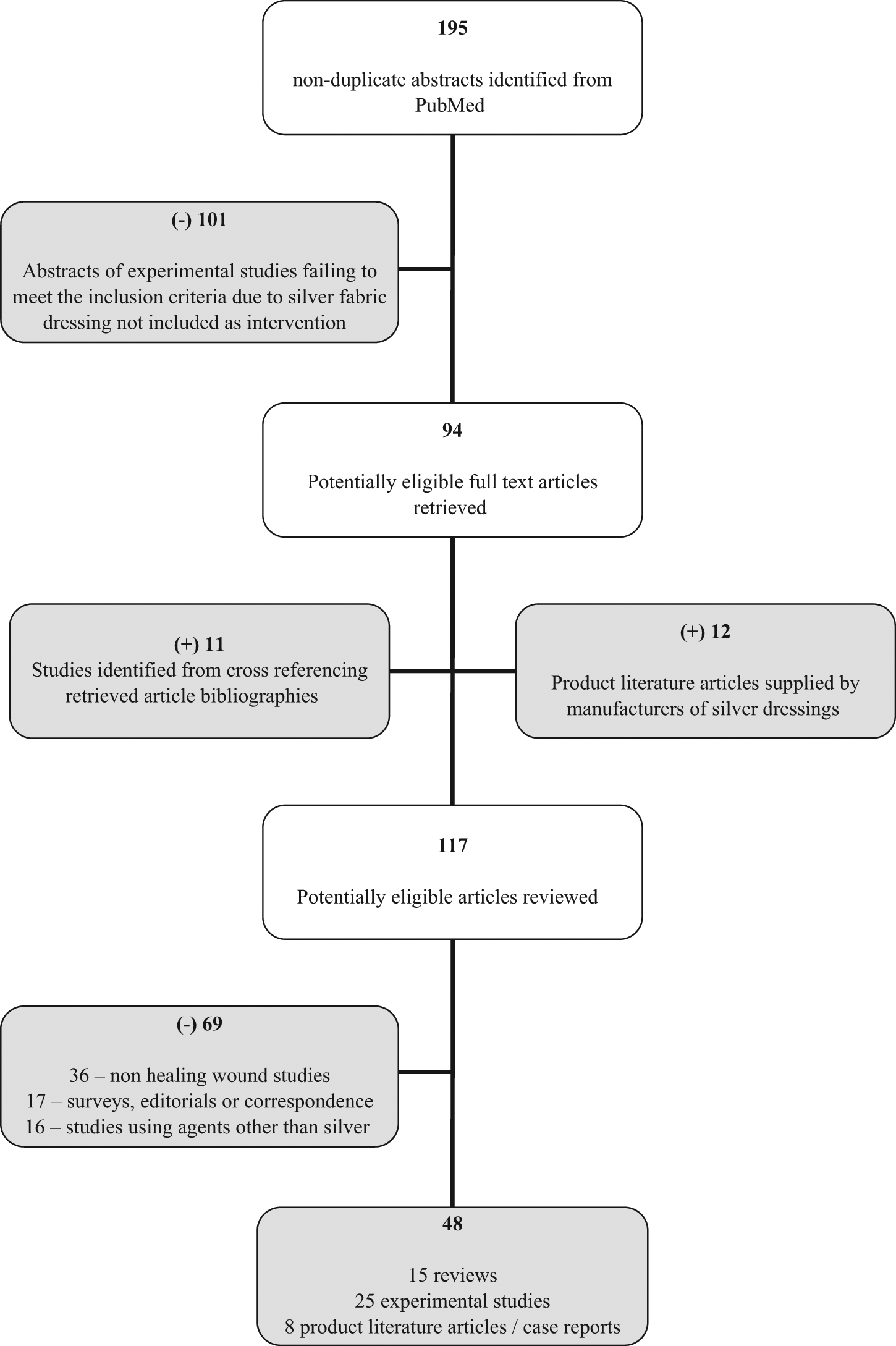
Flowchart of article identification
The Use of Silver in Wound Care
Alongside lead and mercury, silver was the mainstay of therapy against infective diseases in the preantibiotic era. 14 Recognized first as treatment of ophthalmia neonatorum,15,16 silver salts were used during the World War II by combination with sulfonamide antibacterials17,18 in burns wound care.
Temporarily eclipsed by the introduction of penicillin antibiotics and a shift toward parenteral administration, subsequent complications with infection of burn wounds despite systemic antibiotics heralded a renaissance of topical therapy and a return to silver and sulfonamide dressings. Fox 19 combined silver nitrate with sodium sulfadiazine to produce silver sulfadiazine (SSD) after Moyer 20 detailed the use of silver nitrate–soaked gauze dressings. SSD was eventually marketed as Flamazine (Smith and Nephew, Hull, UK), the most widely used topical antibacterial in burns treatment. 21
Mechanism of Action of Silver-Based Wound Dressings
Largely independent of its causation, the events subsequent to a penetrating injury to the skin may be described in a phased manner comprising hemostasis, inflammatory response, and cellular proliferation, ultimately ending with wound remodeling. Traditionally characterized as occurring only in a defined, early part of tissue trauma, inflammation persists throughout all wound healing phases, stimulating and coordinating the reparative process. 22
With regard to inflammation, whereas the use of silver agents is accepted in wound care, it is only recently that the complex relationship between collagenase enzyme activity, inflammation, and silver therapy in the healing of tissue injury has been established. In particular, the altered balance between tissue destruction and synthesis because of excess matrix metalloproteinase (MMP) activity and diminished levels of tissue inhibitors of metalloproteinase have now been identified as a key aspect of prolongation of wound healing. 23
In addition, it has been suggested that it is an imbalance of enzymes within the wound fluid and not the healing tissue itself that results in delay in healing and persistence of an inflammatory response. In particular, it has been demonstrated that a MMP subcomponent (MMP-9) is present at higher levels in wound fluid than in the corresponding wound, suggesting that much of the destructive effects observed in chronic wounds may be compounded by components of the wound exudates, resulting in a continuum of tissue damage. 24 It can be seen, therefore, that agents that have proof of efficacy against MMP while demonstrating antibacterial potency could play a dual role in optimizing tissue healing.
Much of the discussion of the impact of silver therapy on protracted inflammation and the wound milieu on an in vivo basis arose from the porcine study of Wright et al 25 of the effect of nanocrystalline (NC) silver on MMPs and cell apoptosis. Frequently cited as the rationale for the use of silver dressings in early modulation of inflammatory mediators in wounding,23,26 there are a number of limitations to this study as detailed in the later exploration of in vivo modeling in this article.
In addition to the inflammatory response, the wound bioburden also significantly affects the nature of healing following tissue injury. Transitory presence of contaminating organisms, although unavoidable, does not by definition, however, result in exacerbation of host tissue damage, and even when organisms remain present, colonizing and replicating within a wound, satisfactory healing may occur with minimal intervention. It is the presence of wound infection that has a negative impact on ultimate outcome through disruption and prolongation of the normal phases of healing. 22
Defining what constitutes an infected wound is not straightforward. Described as a wound in which healing is interrupted by microbial growth, multiplication, and tissue invasion with resulting cellular injury and overt host immunological response, 27 debate exists as to whether such wounds should be defined quantitatively or qualitatively. 28 Dogma holds that infection will result if the density of microorganisms within the wound exceeds 105 CFU (colony-forming units)/g of tissue 29 based on surgical wound closure and skin graft studies in the presence of contaminating organisms. 28
In addition to arbitrary quantitative cutoffs, it is appreciated that equilibrium exists between bacteria and host factors, and when this balance is tipped in favor of the contaminating microorganism, the potential for infection occurs. The point at which the balance alters (~1 million organisms per gram of tissue) may be of use, but of equal import is the recognition that like many biological phenomena, this distribution forms a bell-shaped curve and both host and organism factors interact to determine when infection will truly occur. 28
Having established the potential of silver therapy to target wound bioburden and inflammatory response, 2 key concepts underlying its delivery and action at the wound interface that contrast to other agents must also be appreciated. First is the oligodynamic (inhibiting or killing of microorganisms by the use of very small amounts of a substance) effect demonstrated by silver inducing the sensitive bacteria to absorb and concentrate Ag+ from dilute solutions, often below 1 part per million.23,30 Second, silver has an ability to be applied to dressings, catheters, and prostheses without affecting its antimicrobial properties, thus enhancing its mode of delivery. 31
Central to the oligodynamic action of silver is the level of flux between its relatively inert elemental form (Ag0) and the more reactive cationic or positively charged ionized form (Ag+). Regardless of the delivery agent, associated compounds, or material state of the preparation, the antimicrobial efficacy is reliant on the release and availability of Ag+, even if per the concept of oligodynamic effect above, the resultant concentration is very low. Hence the reservoir of any dressing or cream is the inert elemental form (Ag0), with cationic Ag+ being the active element. A number of mechanisms by which the latter exerts an antimicrobial effect have been described, including disruption of the electron transport chain affecting metabolic function, interaction with thiol groups in the cell wall leading to its structural compromise, and finally, direct binding to DNA and RNA resulting in flaws in bacterial replication.14,32,33
Delivery of silver to the wound surface will vary both according to the nature of the preparation applied and the wound bed itself. Silver nitrate solution (SNS) and SSD applied to the skin release Ag+ at concentrations of up to 3200ppm, 32 albeit at different rates, with the latter occurring over a longer duration than that seen with the nitrate salt.
These high concentrations, however, are short lived as a result of the fact that inactivation of silver occurs through contact with the wound environment because complexes are formed both with organic matter and available anions, such as that most commonly seen with precipitation as chloride salts. With increasing availability of organic matter and circulating anions, such as the situation found in wounds, rapid reduction in active silver is seen. 32 In a phosphate buffer solution, the oligodynamic property of silver is most evident, with biological activity of the metal maintained at concentrations as low as 0.05 ppm. In contrast, as the complexity, organic nature, and ion content of the fluid increases, effective concentrations of up to 70 ppm are required to maintain a level of biological activity. 32
This drop in the bioavailability of cationic silver in wounds has practical implications in the use of topical silver preparations. Moyer 20 recommended that dressings be applied daily so that they remain saturated with SNS—a regime with obvious impact on resources and patient discomfort. Similarly, for the SSD cream, the recommendation is for daily dressing change or for more frequent change should the ointment rub off onto bed linen.19,34 Contemporary silver dressings in contrast enable less frequent nursing interventions with greater control over elemental silver flux at the wound bed. In such dressings, nanocrystals are applied by vacuum vapor deposition onto a mesh, creating a NC layer with markedly greater surface area than that of elemental silver. This nanocrystallization alters the reactivity and solubility of the silver layer; whereas silver in the bulk elemental state will not dissolve, NC silver does so rapidly to provide a concentration of around 70 ppm at the wound surface. In contrast to the nitrate salt solutions, this rapid early dissolution is followed by a steady state of silver ion release dependent on the equilibrium of ions in the solution in which the dressing is placed. 32
Silver-Plated Fibers, Nanotechnology, and Modern Silver Fabric Dressings
In contrast to the number of products enabling delivery of silver to chronic wounds through foams, hydrofibers, or alginates, the choice of simple silver fabric dressings, applicable to use in traumatic extremity wounding is limited.
Silverlon (Argentum Medical, Chicago, IL) and SilverSeal (Noble Biomaterials, Scranton, PA) are both wound contact dressings featuring knitted nylon fabric coated with silver. Evidence for the use of either agent is limited. The manufacturers of Silverlon provide unpublished case studies of the use of their dressing system in acute wounding, including conflict wounds. In vitro, unpublished data reveal antimicrobial efficacy that is similar to that of other proprietary silver fabric dressings when assessed by Kirby-Bauer or disk-sensitivity assay. 35 Experimental assessments of SilverSeal are lacking, with neither proprietary nor independent in vitro, in vivo, or clinical studies available for analysis.
Another wound contact dressing recently released and indicated for use in acute traumatic as well as nonhealing wounds is the 3M Tegaderm Ag Mesh Dressing (3M, Bracknell, UK) consisting of silver sulfate particles coated onto cotton fibers. No independent scientific data are provided to support the use of this dressing system. Data presented within the product literature regarding the antimicrobial efficacy of Tegaderm Ag is exclusively “on file” at 3M. 36 Neither SilverSeal, Silverlon, nor Tegaderm Ag is in widespread use in the United Kingdom.
The preparation on which there is the greatest quantity of experimental evidence is Acticoat (Smith & Nephew, Hull, UK), a 3-layer dressing consisting of an absorbent rayon-polyester core sandwiched between 2 layers of silver-coated high-density polyethylene mesh held together with ultrasonic welds.
As highlighted, central to the ability of Acticoat to continuously release silver into the wound and where it differs from the other fabric dressings is the use of nanotechnology in its design. NC metals are those with a range of grain sizes smaller than 100 nm, 37 and nanotechnology relates to a scientific discipline in which matter of size less than 100 nm is manipulated. 38 In Acticoat dressings, silver is applied by vapor deposition in an argon vacuum, creating a NC layer with markedly greater surface area than elemental silver. With nanocrystallization, the reactivity and solubility of the silver layer is altered. In contrast to the nitrate salt solutions, rapid early dissolution is followed by a steady state of silver ion release dependent on the equilibrium of ions in the solution in which the dressing is placed. As available silver cations are depleted, more are released from the dressing to restore the equilibrium concentration at therapeutic levels. 32
The potential benefits of such products are the ability to deliver elemental silver—without the associated side effects of its nitrate or sulfadiazine salts—rapidly and in a sustainable manner, negating the need for continued application.
With an absence of published data for the only other related fabric products, review of silver dressings applicable to use in acute extremity wounds is focused by necessity on analysis of studies using Acticoat and more traditional (SSD and SNS) perpetrations. Such studies may be categorized as preclinical in vitro, preclinical in vivo, and clinical studies, the latter divided between silver as therapeutic intervention for either burn injury or chronic wounds.
In Vitro Investigation of Silver Dressings in Wound Care
Despite both zone-of-inhibition assays and cytotoxicity testing being distinctly different to the physiological setting of the wound bed and of questionable validity as a measurement tool for antimicrobial efficacy, 39 much emphasis has been placed on the results of such experimentation and the implied effect this may have on wound care. 40
Wright et al 41 report early in vitro experimental work in which 3 modes of silver delivery by dressing are assessed: SNS, SSD, and a silver-coated dressing (Acticoat). Following inoculation with bacteria of proven antibiotic resistance, the results suggest that both the nitrate- and sulfadiazine-impregnated dressings were ineffective against a number of the bacterial strains, whereas Acticoat demonstrated efficacy against all the challenge organisms. The method involves bacterial recovery suspensions with conditions entirely disparate to that in injured tissue, questioning the validity of such in vitro testing.
Extending the scope of organisms but with the same basic methodology, Wright et al 42 carried out a subsequent evaluation of topical silver against 5 fungal burn wound pathogens, revealing an apparent enhanced effectiveness of Acticoat against fungal isolates, particularly evident in terms of rapidity of action and broadness of range. Acticoat undergoes further evaluation by Yin et al 43 at the same institution, albeit with a different study design. In this series of experiments, 5 organisms are used as a challenge panel and the interventions (Acticoat, SNS, SSD and mefenide acetate) analyzed in terms of minimum inhibitory and bactericidal concentrations, zones of inhibition, and killing curves.
The results reveal that all the silver products performed similarly, with no difference in outcome between them other than rapidity of action, with the Acticoat dressing demonstrating a faster bactericidal rate. The clinical relevance of this in light of similar overall efficacy, however, is unclear.
Although not immediately apparent as a conflict of interest, all these studies41-43 were carried out at the laboratories of Westaim Biomedical Corporation, developers of Acticoat. They also form the basis of a number of unpublished, industry-sponsored studies intended to demonstrate proposed rapidity, broad spectrum, and longevity of action against antibiotic-resistant organisms. 44 Apart from the industry bias, their validity in terms of clinical relevance is also questionable. The methodology involves assessment, for the most part, of inoculated dressings in entirely nonphysiological circumstances. The in vitro condition of these studies is very different from that seen at the wound surface, where exudate, organic matter, and contamination are present.
Thomas and McCubbin45,46 subsequently performed a comparison of the antimicrobial effects of silver-containing dressings using zone of inhibition and bacterial transmission testing. Again, the results suggest increased inhibitory in vitro activity of Acticoat against the challenge organisms, although as with the other in vitro assessments, these experimental conditions do not accurately replicate the conditions of the wound interface, and extrapolation to the clinical domain is questionable. In addition, in similarity to all the previous studies, this work is supported by the manufacturers of the dressing itself (Acticoat, and Smith & Nephew, Hull, UK).
One of the first, non-industry-sponsored, in vitro studies of Acticoat is that performed by Holder et al 47 in an evaluation of its use on excised burns. Using organisms isolated from burn patients, the authors carried out barrier, zone of inhibition, and timed antimicrobial action testing, with results suggesting that Acticoat was an effective barrier to microbial transmission but possessing only partial direct inhibitory action against Gram-negative organisms. Paradoxically, bactericidal activity was seen in the timed antimicrobial testing, which is in essence a suspension test. This led to the authors speculating that there may be a time-dependent effect on some organisms.
This would, however, contrast with all previous studies in which the rapidity of action of Acticoat gains particular attention. Although this discrepancy is noteworthy, it does not detract from the main result of the study in demonstrating that Acticoat functions as an effective barrier to microbial transmission and may have a role in protection of wounds and skin grafts against environmental organisms.
Identifying sepsis as a leading cause of mortality with major burns, the Royal Children’s Hospital Burns Research Group 48 undertook in vitro evaluations of silver-based dressings. Against a challenge panel of 8 organisms in a suspension test, the combination of 1% SSD and 0.2% chlorhexidine digluconate (Silvazine, Sigma Pharmaceuticals, Melbourne, Australia) resulted in the most effective killing of all bacteria, in comparison to 1% SSD alone or Acticoat. Interestingly, in contrast to previous studies, Acticoat is demonstrated to have only bacteriostatic action against Enterococcus faecalis and MRSA (methicillin-resistant Staphylococcus aureus). Viable methicillin-sensitive S aureus was also still present after 24 hours in the Acticoat dressing. The impressive antimicrobial efficacy of Silvazine thus demonstrated is tempered by subsequent cytotoxicity testing, however, using a strain of immortalized human keratinocytes. 49 The results show that although all silver preparations are associated with some cytotoxicity, the level of cell destruction associated with Silvazine is considerable. Although Silvazine is not used outside of Australasia, this study serves as an indicator of the potential cytotoxic effect of silver on host skin cells with implications for wound healing.
Also, investigating potential cytotoxicity, Poon and Burd 50 used cultured keratinocytes and fibroblasts and found that silver released either from Acticoat or SNS is lethal for both cell types in vitro. Although, as with other in vitro assessments, the authors advise caution in extrapolation of their results to the clinical scenario, Poon and Burd do suggest that silver-based products should be avoided where proliferating keratinocytes are exposed. This finding is further supported by similar in vitro assessments of Acticoat cytotoxicity by Burd et al 51 and Lam et al, 52 which conclude that Acticoat is cytotoxic to cultured skin cell lines and should not be applied as a topical dressing on cultured skin grafts.
Cytotoxicity is not confined to keratinocyte studies, however, being reported across a range of in vitro studies. Adverse effects have been demonstrated on osteoblasts and osteoclasts, 53 macrophages,54,55 murine blastocysts and fibroblasts,56,57 and fish. 58 This in vitro cytotoxic potential of silver nanoparticles, identified as being cell-type and size dependent, 59 is put into perspective by the fact that studies exist investigating its use in cancer therapies. 60
Although not addressing cytotoxicity but from the same institution as Poon and Burd, 50 Ip et al 61 performed an assessment of 5 commercially available silver preparations in a suspension test and found a wide range in rate and completeness of antimicrobial action between the dressings. Acticoat was very effective and had a rapid and wide spectrum of bactericidal activities, particularly for S aureus. This notable efficacy of Acticoat in terms of bactericidal action on Gram-positive organisms was a similar finding in further in vitro analysis carried out by Aramwit et al 62 in a study of 6 dressings and 5 challenge organisms using corrected zone-of-inhibition testing. Once again, however, the method used is questionable in terms of appropriateness 39 and clinical relevance. The study periods were less than 24 hours, and suspension testing was carried out in nonphysiological media. No impact of exudate or of the complex physiology of the wound bed was considered.
The disparity in antimicrobial effects of silver dressings, their relation to the amount and rate of silver released, and the wide range of products available are highlighted by Castellano et al 63 in their comparative evaluation of silver-containing antimicrobial dressings and drugs. In the most inclusive evaluation available, Castellano et al performed zone-of-inhibition determination (disc diffusion test) and suspension-based quantitative analysis of antimicrobial activity of 12 commercially available silver-impregnated dressings, foams, creams, and gels. In agreement with the findings of Ip et al, 61 the results suggest that all silver preparations exhibit antimicrobial efficacy although silver- or antibiotic-containing creams or gels demonstrate increased antimicrobial efficacy compared with the silver fabric–impregnated dressings. This leads the authors to make the observation that although the latter may provide a barrier to organisms, their antimicrobial properties are inferior to commonly used topical, nonfabric systems.
Although it shares the limitations of all in vitro antimicrobial efficacy testing, it is the sole, non-industry-sponsored evaluation of silver dressings and the results contrast greatly with those published in the early evaluations of Acticoat against similar agents.
There are thus concerns over the heterogeneity of methods used in in vitro studies, the results they yield, and also in their marked dissimilarity to the clinical conditions of either acute or chronic wounds. As a result of this and to further inform the evidence base regarding the use of silver dressings in wound care, a number of animal studies have been performed.
In Vivo Investigation of Silver Dressings in Wound Care
Burrell et al, 64 developers of Acticoat, reported a murine study of burns wounds contaminated with Psuedomonas aeruginosa in a survival analysis comparing untreated, control burned, and contaminated rats with those receiving silver fabric dressings or SNS therapy. The results suggest that Acticoat improved survival of the burned animals and also resulted in a lesser body weight loss, as a marker of systemic involvement, in those that survived. Appropriate statistical analysis reveals that burned, contaminated animals treated with NC silver dressings had a greater chance of survival than other treatment groups and that survivors showed no significant difference in body weight when compared with noncontaminated burn control animals, all of whom survived. This early study benefits from a simple methodology, with transparent outcome measures in assessing a pathogen relevant to burns care. No quantitative assessment of reduction in organism count is presented, however, which would have been valuable to enable correlation between bacterial load and mortality.
Wright et al, 25 again from Westaim Biomedical Corporation, investigated early healing events in a porcine model, looking in particular at the effects of NC silver on MMPs and inflammatory cell apoptosis. The authors investigate their hypothesis that NC silver influences the prolonged inflammatory response seen in nonhealing wounds by creating full-thickness skin wounds contaminated with a polymicrobial solution. The authors estimate the challenge dose at 8 × 104 CFU/cm2, although the actual dose or the presence of other host organisms was not recorded.
Following inoculation, the wounds were dressed with either silver-containing (SNS or Acticoat) or a control, nonsilver dressing. Only skin grafts placed over the wounds at day 4 that were dressed with Acticoat survived to full take. Tissue evaluation suggests greater fibroblast numbers and granulation tissue formation and lower polymorphonuclear leukocyte density, bacterial counts, and MMPs in the Acticoat group. There are a number of limitations to this study, as with the earlier experiments,41-43 in terms of potential industry bias. With regard to method, the interventions are not randomized, and the challenge dose is uncontrolled. No systemic data as to the effects on the animals are presented. In addition, these results, in particular regarding the impact of silver on successful graft take, directly contradict the in vitro work of Poon and Burd, 50 who found that silver released from such dressings was lethal to fibroblasts.
Identifying the negative aspects of repeated dressing changes, Heggers et al 65 conducted a murine study of silver dressings in Sprague-Dawley rats receiving a standard contact burn. Following injury and inoculation with P aeruginosa or S aureus, the rats were treated with either a control or 1 of 3 silver dressings. The details of the methodology are limited, and there is no evidence of randomization. The results imply that following 10 days of dressing application, the levels of challenge organism are decreased significantly in all dressings other than in controls, although no difference is seen statistically between dressing types. Although the raw data do show discrepancies, with such limited methodological description, it is presumed that the numbers of animals were too small to show a difference between dressings. The authors use the bulk of their discussion to describe the effect of silver in wound care—information that is not supported by their study. Their conclusions that it is efficacious to leave silver-containing dressings on for 10 days seems to be based entirely on the level of organisms found in the wound at this point. No histological analysis is provided to demonstrate the level of healing and/or cytotoxic effects seen in leaving a dressing with proven in vitro cytotoxicity on a wound for this duration. The significant limitations in the methodology threaten the validity of the findings of this work and cannot support the hypothesis that extended duration of application of the dressings is either efficacious in healing or in decreasing organism load.
These methodological limitations are not present in a subsequent series of murine burn wound management studies by Ulkur et al. 66 Here, 24 hours after inoculating MRSA onto standardized burn wounds, these were dressed at random with Acticoat, chlorhexidine acetate 0.5% (Bactigras, Smith & Nephew, Hull, UK), or fusidic acid 2%. 66 Then, 7 days postburn, the animals were euthanized and the eschar, muscle, and lung tissue and arterial blood were quantitatively assessed for microorganisms. The results demonstrate that the fusidic acid treatment resulted in no organisms being recovered from any of the sample sites. The control group had microorganisms present both locally and also in lung and blood samples. The Acticoat group prevented deep and systemic spread, although organisms were still present in the eschar.
The same model is used by the authors to compare the efficacy of Acticoat, Bactigras, and SSD in P aeruginosa–contaminated wounds. 67 All test therapies prevented both systemic and deep tissue spread of the challenge organism and showed significant differences in antimicrobial efficacy compared with controls. Although there was no difference between the NC silver and chlorhexidine in decreasing bacterial activity, significant improvement in antimicrobial action was seen with the use of SSD cream.
Both these studies demonstrate the efficacy of Acticoat in reducing deep and systemic spread of microorganisms in burn wounds. They do, however, show that this efficacy, although demonstrable against controls, is inferior to more established, cream-based antimicrobial preparations in similarity to the later in vitro findings of Castellano et al. 63 The work of Ulkur et al66,67 was extended within the same research group more recently by Acar et al 68 and Uygur et al 69 using the same model to investigate the management of Candida albicans and Acinetobacter baumannii contamination, respectively. Using a challenge of C albicans and comparing Acticoat, Bactigras, and nystatin, Acar et al found that in contrast to the previous bacterial studies using the same model, none of the dressings prevented contamination of the underlying deep musculature when contaminated with a fungus challenge. Bactigras was found to be associated with systemic spread, whereas both Acticoat and nystatin showed similar overall efficacy and prevented systemic involvement. 68
With a challenge of A baumannii and comparing Acticoat, Bactigras, and SSD, Uygur et al 69 demonstrate the comparative virulence of this pathogen in the standardized burn wound. In contrast to previous studies, all preparations other than Acticoat demonstrated systemic spread as well as involvement of the eschar and deep tissues, whereas in contrast, only 2 of 8 animals had the organism recovered from the eschar at the end of the study in the NC dressing group, and none had deep or systemic involvement. Of note with the challenge organism A baumannii, in contrast to P aeruginosa, Acticoat demonstrates superior antimicrobial efficacy than the cream-based silver preparations seen in the group’s earlier study. 67
Although no conflicts of interest are declared by the authors, they recommend the use of Acticoat in the management of burn injuries, primarily because of the proposed requirement for fewer dressing changes. Although this may concur with contemporary literature demonstrating a trend for recommending NC dressings for this reason, this is not completely supported by the murine models described. In all cases, the cream preparation is applied once daily, whereas the NC silver dressing is changed every other day. The cost implications and effect on patient discomfort associated with alternate daily dressings with Acticoat has not been considered in this recommendation. What would have been of considerable value for all these experiments would have been to have a group of animals in which the NC dressing is left on for the full study period. The findings of such experimentation would provide much more compelling evidence for infrequent NC silver dressing change in wound care if similar efficacy was demonstrated when the dressing was left undisturbed for several days.
These contrasting results of in vivo and in vitro studies, particularly in terms of host cell damage, are highlighted in a murine model by Supp et al 70 evaluating cytotoxicity of Acticoat in the management of contamination in cultured skin substitutes (CSSs). In a combined in vitro and animal study, the authors demonstrated that in vitro, Acticoat when applied to the CSS, was rapidly cytotoxic. In vivo, however, 7-day exposure of the NC dressing to full-thickness wounds to which the cultured cells had been applied did not injure CSS or inhibit wound healing. With regard to contamination, although efficacious in reducing Pseudomonas challenge organism count in the wound bed, the application of Acticoat did demonstrate complete efficacy in the barrier role by preventing transmission of the organism to those wounds having clean wound beds.
This well-constructed study reinforces the role of Acticoat as a proficient barrier dressing confirming the in vitro barrier transmission work of Thomas and McCubbin. 45 Using a combined experimentation approach, the authors demonstrate the apparent cytotoxicity of Acticoat on cultured cells in vitro with compelling evidence for lack of toxicity of the same cells with the same dressing in vivo. This study therefore corroborates the apparently conflicting findings of Poon and Burd 50 and Wright et al 25 detailed earlier.
Clinical Investigation of Silver Dressings in Wound Care
Although there are no published reports on the use of silver fabric dressings in acute extremity wounding, evidence is available for burn and nonhealing wound care. Aziz et al 71 performed a review of silver fabric dressings and creams in the management of burns wounds. In a robust assessment of 14 randomized controlled trials (RCTs), significant methodological heterogeneity prevented meaningful analysis of the effectiveness of either preparation in preventing or promoting healing of burn wounds. A weak association is seen between SSD and increased healing time when compared with nonsilver dressings, although this is not a new finding. A Cochrane analysis of 26 RCTs of all burn wound dressings for superficial and partial thickness burns comments on the paucity of high-quality RCTs on dressings for burn injury. Of the included studies, most were methodologically poor, and although this is acknowledged, the authors similarly recommend that the use of SSD on burn wounds needs to be reconsidered. 72
Khundkar et al 73 further reinforced the lack of quality published evidence to support the use of silver fabric dressings, identifying only one level-1 study comparing Acticoat to standard (SSD) therapy. 74 The majority of other studies involving the NC silver dressing were confined to preclinical experimentation or case reports. Lack of evidence limits the recommendations of the authors, which are confined to a suggestion that Acticoat may be associated with increased antimicrobial action in comparison with SSD as well as fewer adverse effects and decreased healing times.
For nonburns wounds, Bergin et al 9 found that despite the widespread use of silver in diabetic foot ulcers, no randomized or even controlled clinical trials exist to demonstrate their effectiveness.
Storm-Versloot et al 75 interrogated RCTs comparing silver dressings and topical agents with non-silver-containing comparators on uninfected wounds to evaluate their efficacy in preventing wound infection. Identifying 26 RCTs, the authors found again that significant heterogeneity of method prevented meaningful meta-analysis. Twenty of the evaluated trials were on burn wounds and thus overlap the work of Khundkar et al 73 and Wasiak et al, 72 whereas the other 6 represented a mixture of wound types. The retrieved studies satisfying the inclusion criteria were small and of poor quality, and the authors conclude that there is not enough evidence to support the use of silver-based wound therapy in the prevention of wound infection. 75
This significant heterogeneity of methodologies was not in contrast encountered by Lo et al 76 in a well-constructed meta-analysis of the efficacy of silver-releasing dressings in the management of a different population—nonhealing chronic wounds. Analyzing pooled data from 1399 patients in 8 RCTs, using outcome measures of improved wound healing times, decreased odor, decreased wound exudates, and increased patient comfort, the authors found that silver-releasing dressings showed significant improvements over alternative methods of wound care. The authors do quantify these findings, however, as being representative of chronic wounds in a predominantly elderly study population with several advanced associated chronic diseases and caution against direct extrapolation to other populations, identifying the need for further work in these areas.
Although meta-analysis of similar studies by Carter et al 10 found that evidence may be interpreted for improvements in wound healing with silver dressings, these are based mainly on decreasing wound size, not on complete wound healing or eradication of infection. The authors suggest that although silver dressings may decrease wound size, there is no evidence that they promote complete wound healing superior to other wound care options.
Evidence of the efficacy of silver dressings is therefore limited because of a paucity of high-quality experimental work. This is particularly apparent in clinical studies where no evidence exists for the use of silver in acute traumatic wounds and evidence pertaining to the broad range of nonacute wounds is unable to withstand robust analysis, generating at best equivocal recommendations for its use. Summarizing, Chaby et al 77 conclude in a recent review that there is only weak evidence of any difference in efficacy of modern dressings compared with more traditional saline or paraffin gauze alternatives. In particular, the authors found no scientific evidence for the use of specific dressings in the prevention and treatment of infection.
An insight into the evidence on which the use of Acticoat specifically is based can be gained from product literature released by the license holders (Smith & Nephew, Hull, UK). There are 9 studies presented, of which initial inspection reveals that 3 are peer-reviewed publications and the remainder are unpublished work. Of interest and questioning the integrity of their literature review, is the fact that one of the articles that afforded level-2 evidence is a newsletter with no experimental content. Attention to the only comparative clinical study demonstrates it to be a semiretrospective, uncontrolled, nonblinded, nonrandomized cohort assessment of wound complications following vascular surgical procedures. 78 The other publication is a case report of necrotizing fasciitis 79 in which the role of dressings as a whole and Acticoat in particular are not actually mentioned at all.
The third peer-reviewed work provided as evidence for the efficacy of Acticoat in acute wounds is the in vitro study by Edwards-Jones 80 of the barrier properties of silver-containing and silver-donating dressings against MRSA. Although it demonstrates the barrier properties of the dressing and some antimicrobial effect, there is no comparison presented with nonsilver dressing alternatives, and the methodology, as identified in other similar studies, limits the extrapolation of the findings to the clinical domain. The data used to support the use of Acticoat in acute wounds by the manufacturers may be limited and of questionable quality, and the same is also seen with their assessment of evidence for its use in burns and chronic wounds. In particular, the multiple systematic reviews regarding silver preparations in wound care that demonstrate insufficient evidence for their recommended use are notably absent from the appraised literature.9,72,75,77
Summary
Infection of limb wounds significantly influences the outcome from extremity trauma, and as an antimicrobial modality, silver pre-dates the use of antiseptics and antibiotics.
Although a promising concept, the evidence for the use of silver dressings in traumatic extremity wounds is lacking. There are limited clinical trials of relevance to acute limb injury, and those proposed to demonstrate efficacy in acute wounds have significant methodological limitations. The preclinical studies on which the dogma surrounding silver use in wound care is based are characterized by heterogeneity of method and the use of models that are nonrepresentative of the environment of the acute wound. Although less evident in vivo, cytotoxicity is also demonstrated with the use of silver in preclinical dressing assessments.
Selective extrapolation of imperfect in vitro and in vivo experimentation to the clinical setting has occurred without meaningful data to support such theorizing. Although silver-impregnated dressings are efficacious in both barrier and antimicrobial roles in chronic wounds, there is insufficient evidence to recommend their routine use over standard dressings.
This review is limited to appraising the use of silver dressings in the context of the acute, traumatic wound. Aspects of wound care outwith the early management of the acute wound and the role that silver dressings have in other areas of health care were by requirement of brevity, omitted. The interpretation of this review must be held in the context of acute extremity injury and the potential use of silver dressings in such challenging wounds. Although it is often interpreted thus, the absence of quality experimental evidence does not de facto equate to a proven lack of efficacy. It is apparent for the investigation of acute extremity wounds that robust, randomized trials are required, and because of the complexities of experimentation in the significantly injured, in the first instance, this requires the construction of in vivo models both representative of extremity trauma and capable of allowing therapeutic manipulation with dressing systems.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.