
Abstract
Revision surgery (RS) is frequently needed to control diabetic foot infections. It is the aim of this retrospective observational study to analyze the variables associated with undergoing RS and the variables associated with undergoing a major amputation when RS was required. We conducted a retrospective study of patients with diabetes treated in our department during 10 years (January 1, 2000 to January 1, 2010) who had foot infections identifying those who required RS. In all, 167 out of 417 patients (40%) with diabetes who underwent surgery for foot infections underwent RS for persistent infection. The predictive variables related to undergoing revision surgery were erythrocyte sedimentation rate >70 mm/h (odds ratio [OR] = 1.6, 95% confidence interval [CI] = 1.1-2.6), leukocytosis (OR = 1.6, 95% CI = 1.1-2.5), peripheral arterial disease (OR = 1.5, 95% CI = 1.0-2.4), and isolation of gram-negative rods from tissue biopsy (OR = 2.2, 95% CI = 1.5-3.4). Seventy-nine out of 167 patients (47.3) who underwent RS required a higher level of surgery achieving a limb salvage rate of 70.7%. Predictive variables related to undergoing a major amputation after RS were persistent infection located in the bone (OR = 0.08, 95% CI = 0.03-0.22), ischemic heart disease (OR = 3.4, 95% CI = 1.4-8.5), 2 or more reoperations (OR = 3.0, 95% CI = 1.2-7.1), isolation of gram-negative rods from tissue biopsy (OR = 3.3, 95% CI = 1.3-8.4), and peripheral arterial disease (OR = 6.5, 95% CI = 1.9-22.8). Despite the fact that 40% of patients underwent reoperations for diabetic foot infections and 47.3% of them required a higher level of surgery, a high rate of limb salvage could be achieved.
Foot infection is a dramatic complication in the feet of patients with diabetes. Stabilization of severe patients, antibiotics, metabolic control, and surgery, including revascularization, are necessary in many cases and it should be carried out in a stepwise fashion by a multidisciplinary team.1,2 Surgeons who confront such challenging patients should have an appropriate knowledge of the anatomy of the foot, the ways in which the infections spread through the foot, and should be able to quickly detect when the patient will require reoperation to control the infection.3,4 Revision surgery (RS) is frequently needed when residual infection remains in the wound after the first procedure or infection complicates the wound because of desiccation and/or tissue necrosis. 5
Revision surgery for diabetic foot infections (DFIs) has not sufficiently been addressed in the medical literature. It is the aim of this retrospective observational study to analyze the variables associated with undergoing RS in cases of DFI, the indications of undergoing RS, and the variables associated with undergoing a major amputation when RS is required.
Patients and Methods
We conducted a retrospective study of patients with diabetes treated in our department during 10 years (January 1, 2000 to January 1, 2010) who had foot infections. We extracted all clinical and microbiological data from our database, which we have used since 1999 to identify patients with infections and those who required RS. Foot infection was diagnosed according to the presence of draining pus and/or a combination of classic signs, including erythema, a foul smell, edema, warmth, lymphangitis, regional lymphadenitis, crepitus, skin blistering, and pain. From 2000 to 2005, infections were classified as limb- and life-threatening infections. From 2005, infections were also classified as moderate (equivalent to limb-threatening infections) and severe (equivalent to life-threatening infections). 6 We diagnosed soft-tissue infections either preoperatively (if there were superficial signs or symptoms of inflammation, necrosis, or purulence) or during surgical procedures (if there was deep-tissue purulence or necrosis), according to previously published criteria.7-9 The diagnosis of osteomyelitis in each case was based on a sequential combination of the probe-to-bone test and plain X-rays, as published elsewhere. 10 The diagnosis of osteomyelitis was always confirmed by histopathology. We diagnosed peripheral arterial disease if the patient lacked both pedal pulses or had an ankle brachial index less than 0.9. We defined anemia according to World Health Organization criteria as a hemoglobin concentration <12 g/dL in women and <13 g/dL in men, and leukocytosis as a white blood cell count of >11 × 109/L. We considered patients whose glycated hemoglobin was <7% to have good metabolic control and those with a higher value to be poorly controlled. Erythrocyte sedimentation rate (ESR) rate was categorized into 2 groups: greater and smaller than median (70 mm/h).
Every patient underwent surgery during which we extracted soft tissue and bone samples aseptically and sent them to both the pathology and microbiology laboratories. Our microbiology laboratory performed aerobic (but not anaerobic) cultures on submitted specimens using the usual methods. We categorized cases in which any gram-negative rods (GNRs) were isolated, either alone or together with any gram-positive cocci, as the GN group. Cases in which no GNRs were isolated from tissue biopsy were designated the non-GN group. Cases in which no bacteria were isolated were included in the non-GN group.
All surgical procedures and reoperations were performed by the first author (JA-S). Surgical treatment was defined as (a) conservative surgery if the infected tissue, whatever its size and depth, was removed without amputating any part of the foot; (b) minor amputations if they involved a partial amputation of the foot that did not involve the ankle joint; and (c) major amputations if located above the ankle joint; the latter was further divided into below-the-knee and above-the-knee amputations. We defined debridement and minor amputation as limb salvage procedures. The decision of performing amputation was based on a combination of clinical findings during initial evaluation and intraoperative assessment of the tissues involved and it was always taken in an individualized way.
Patients who underwent RS for persistent infection after the index procedure were included in the study group. The criterion for RS was persistent infection that did not respond to culture-guided antibiotic therapy and minor debridement (ie, not performed in the operating theatre). Surgical reports were reviewed to define in which tissue the infection that was the cause of the reoperation was located. The location was divided into 3 groups for descriptive purposes: bone, soft tissue, and both. The 3 groups were dichotomized into 2 groups for statistical purposes: infections in which exclusively soft tissues were involved and those in which the bone was involved. The variable “higher level of surgery” was defined as follows: patients who initially underwent conservative surgery and finally underwent any type of amputation after undergoing any number of reoperations, and patients who initially underwent a minor amputation and finally required a major amputation. We considered that the cure of the infection was definitive when healing was achieved. Healing was defined as the complete epithelialization of the ulcer and/or the surgical wound that was created while treating the infection.
This retrospective study did not require approval by an ethics committee since all the procedures were part of our standard practice; we did not alter or exceed our usual scope of medical care. The authors declare that they have conformed to the Declaration of Helsinki in the code of ethics. All patients gave written informed consent for surgery, for photographs taken of their wounds, to be included in our computer database, and for their anonymized case data to be included in a publication.
Statistical Methods
For descriptive purposes we used median and quartiles 1 and 3 (Q1 and Q3) for nonnormally distributed continuous variables and percentage for discrete variables. The series was divided into 2 groups: patients who did and did not undergo RS. By univariate analysis we compared discrete variables using the χ2 test; for continuous variables we used the nonparametric Mann–Whitney U test. Then, to model the effects of predictors of undergoing reoperation while controlling for potential confounding variables, we conducted a stepwise logistic regression analysis for all variables with P value <.1. The group of patients who underwent reoperation was subsequently divided into 2 groups: limb salvage and major amputation. The same sequence of univariate and stepwise logistic regression analysis was undertaken to detect the variables associated with undergoing a major amputation after reoperation procedures. To calculate the time to healing of both groups, patients who underwent a major amputation were excluded and timing was calculated from the first surgical procedure to healing. A P value <.05 was fixed as the threshold of statistical significance. We performed statistical analysis with SPSS version 15.0 for Windows (SPSS Inc., Chicago, IL).
Results
A total of 417 patients with diabetes underwent surgery for foot infections, 285 (68.3%) with osteomyelitis. There were 280 men (67.1%) and 137 (32.9%) women. The median age was 66 years (Q1 56, Q3 73) with a median duration of diabetes mellitus of 17.5 years (Q1 10, Q3 23). In all, 212 patients (50.8%) were treated with insulin. Patients did not have a good metabolic control; the median glycated hemoglobin was 8% (Q1 7, Q3 10) and 307 patients (73.6%) had a glycated hemoglobin >7%. Comorbidities were frequent; 278 patients (66.7%) had hypertension, 263 (63.1%) retinopathy, 131 (31.4%) ischemic heart disease, 131 (31.4%) had previously undergone amputation, 57 (13.7%) nephropathy, and 44 (10.6%) had had a previous stroke.
A total of 167 patients (40%) underwent RS for persistent infection. Patients underwent RS after a median time of 8 days (Q1 5, Q3 18). Overall, 104 patients (62.2%) underwent 1 reoperation, 28 (16.8%) 2 reoperations, 18 (10.8%) 3 reoperations, 9 (5.4%) 4 reoperations, and 8 (4.8%) more than 4 reoperations. The persistent infection that required reoperation was located in soft tissues in 78 cases (46.7%), in the bone in 52 (31.1%), and in both in 37 (22.2%). Persistent infection in the bone was present in 13 patients (21.7%) without osteomyelitis and 77 (71.3%) who underwent index surgery for osteomyelitis (P < .01). Tendons were involved in 30 cases, which meant 26% of cases in which soft tissues were involved. Tendon involvement was present in 16 patients (26.7%) without osteomyelitis and 14 (13%) with osteomyelitis (P = .02). Univariate analysis between the patients who did and did not require RS is shown in Table 1. After applying logistic regression model, the predictive variables related to undergoing reoperations were ESR >70 mm/h (odds ratio [OR] = 1.6, 95% confidence interval [CI] = 1.1-2.6), leukocytosis (OR = 1.6, 95% CI = 1.1-2.5), peripheral arterial disease (OR = 1.5, 95% CI = 1.0-2.4), and isolation of GNRs from tissue biopsy (OR = 2.2, 95% CI = 1.5-3.4). Final outcomes of surgery can be seen in Table 2. Seventy-nine out of 167 patients who underwent RS (47.3%) required a higher level of surgery, achieving a limb salvage rate of 70.7%. Univariate analysis between patients who underwent RS and finally required a major amputation is shown in Table 3. Predictive variables related to undergoing a major amputation after RS were persistent infection located in the bone (OR = 0.08, 95% CI = 0.03-0.22), ischemic heart disease (OR = 3.4, 95% = CI 1.4-8.5), 2 or more reoperations (OR = 3.0, 95% CI = 1.2-7.1), isolation of GNRs from tissue biopsy (OR = 3.3, 95% CI = 1.3-8.4), and peripheral arterial disease (OR = 6.5, 95% CI = 1.9-22.8). Patients who required RS were admitted for a median of 30 days (Q1 15, Q3 54.5) and those who did not require RS were admitted for a median of 13.5 days (Q1 7, Q3 27; P < .01). Healing was achieved in a median of 114 days (Q1 81, Q3 166) in the group of patients who required reoperation and in 69 days (Q1 46, Q3 112) in the group of patients who did not (P < .01).
Univariate Analysis Between Patients Who Did and Did Not Undergo Revision Surgery.
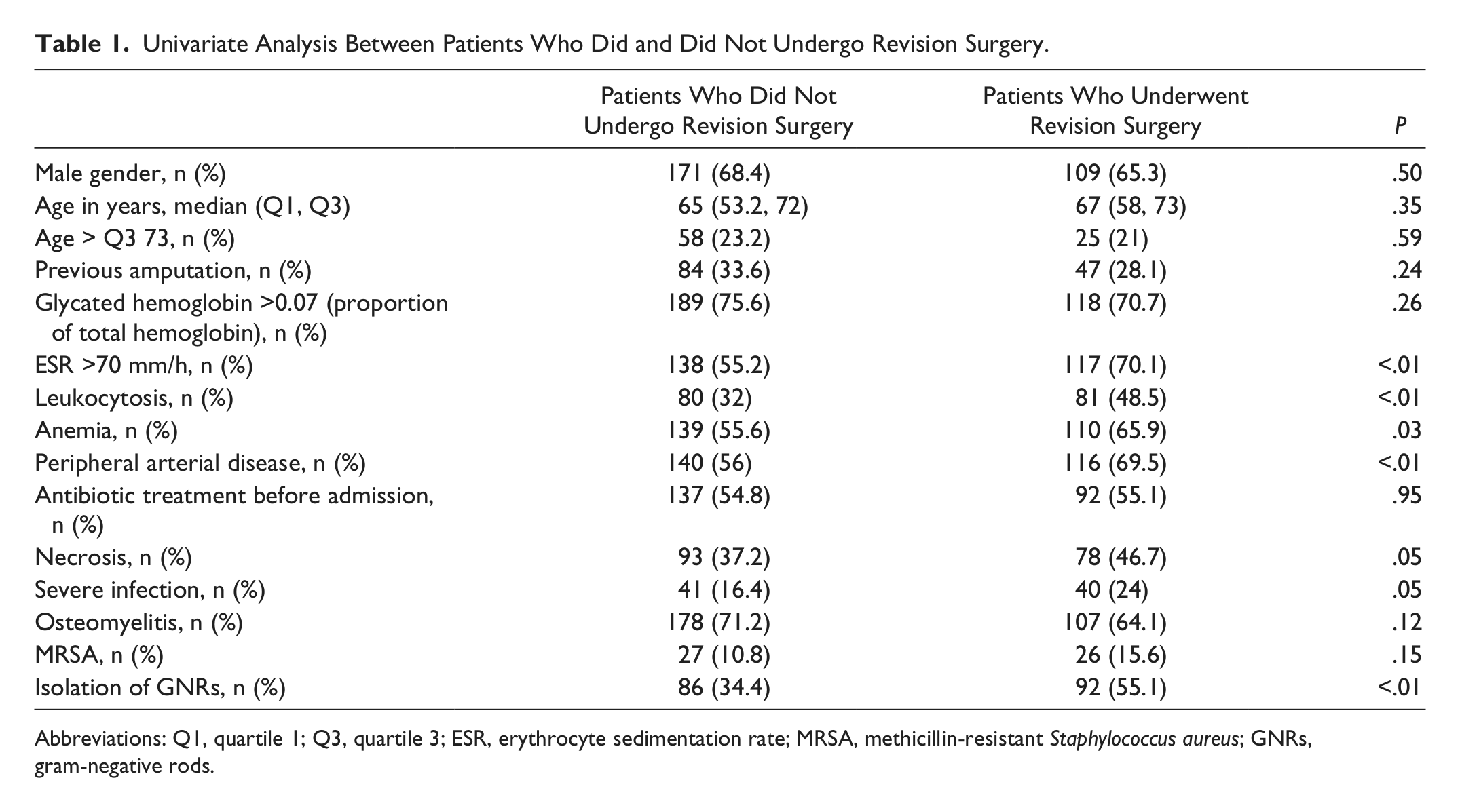
Abbreviations: Q1, quartile 1; Q3, quartile 3; ESR, erythrocyte sedimentation rate; MRSA, methicillin-resistant Staphylococcus aureus; GNRs, gram-negative rods.
Final Outcomes of Surgery.

Univariate Analysis Between Patients Who Did and Did Not Undergo Major Amputation.
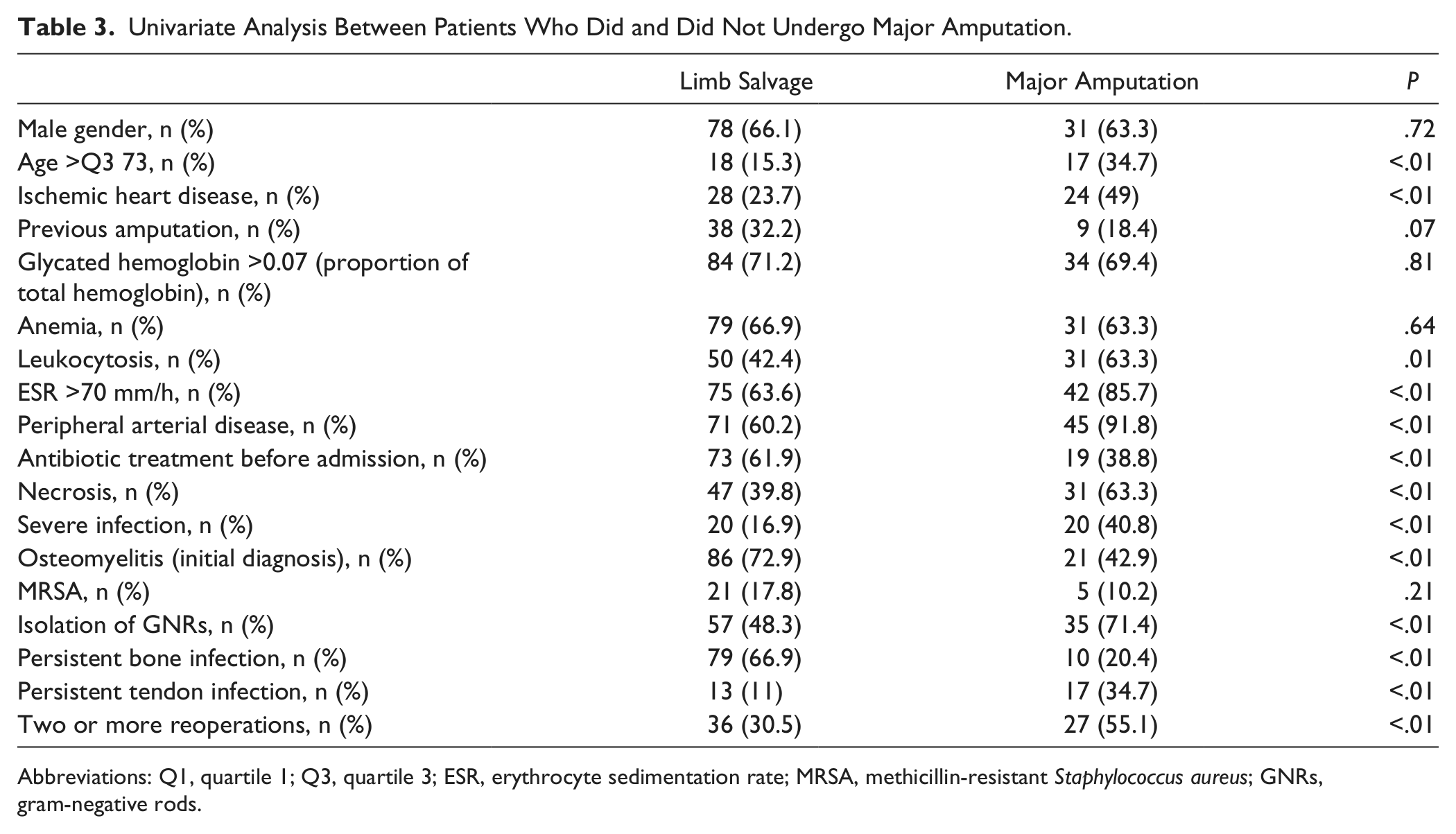
Abbreviations: Q1, quartile 1; Q3, quartile 3; ESR, erythrocyte sedimentation rate; MRSA, methicillin-resistant Staphylococcus aureus; GNRs, gram-negative rods.
Discussion
Surgery is one of the tenets in the management of DFIs. Need for reoperation and a higher level of amputation after initial surgery is frequently quoted in the literature dealing with DFIs11-17 and specifically with osteomyelitis.5,18-22 However, the factors associated with the need for RS has not been adequately identified in the medical literature. We have found a rate of RS of 40% and that the predictive variables related to undergoing RS were baseline ESR >70 mm/h, baseline leukocytosis, presence of peripheral arterial disease, and isolation of GNRs from tissue biopsies. One study reported a similar figure: 17 out of 38 patients (44.7%) with foot infections required RS, which was considered as a criterion of poor clinical response. 13 In this study, persistent leukocytosis after initial treatment was a marker for predicting a poor clinical response. Even though white blood cell count is always checked after index surgery in our practice, these data were not included in the study database and this variable could not be studied.
Another study dealing with partial foot amputations in patients with diabetes reported that 32 out of 102 patients underwent revision surgery; of these only 4 (12%) had been carried out by a consultant, whereas 28 (88%/) had been undertaken by a surgeon-in-training. 17 The outcomes of RS were also worse in patients in which no distal pulses were palpable. 17 Peripheral arterial disease was also a predictive factor for RS in our study and this has been reported by other authors. 15 Our group recently reported the predictive variables associated with the need for reoperation in a prospective cohort consisting of 81 patients with osteomyelitis. 21 Twenty patients (24.7%) required reoperation because of persistent infection. Predictive variables were the presence of necrosis, having undergone conservative surgery, ischemia, and previous ulceration. However, this series did not include patients with types of infection other than osteomyelitis. 21 Furthermore, osteomyelitis in the present study was not associated with undergoing RS.
Gram-negative rods have been reported in many series dealing with this issue whether in developing or developed countries. 23 However, the impact of isolating gram-negative bacteria from tissue samples has not been evaluated previously. The finding that isolating GNRs was associated with the need for RS is novel but it should be carefully balanced because of 2 reasons: first, the retrospective nature of this study, and second, the fact that anaerobic bacteria were not grown. The synergist effect of anaerobes over the other type of bacteria could not be evaluated.
In the present series, 79 out of 167 patients who underwent RS (47.3%) required higher level of surgery. Limb salvage was achieved in 70.7% of the cases. A group of authors reported a series including 146 patients in which 92 underwent foot-sparing surgery; 52% of them required RS to a more proximal level; 28% of the patients who had previously undergone primary toe amputations and 24% of those who had undergone forefoot amputations. 15 In all, 29.3% of our patients who underwent RS finally required a major amputation. One study reported that 21 out of 79 (26.5%) patients required a major amputation, 8 (38%) during the initial hospitalization, and 13 (62%) on a subsequent admission. 12
Predictive variables related to undergoing a major amputation after RS in the present study were persistent infection located in the bone, ischemic heart disease, undergoing 2 or more reoperations, isolation of GNRs from tissue biopsy, and peripheral arterial disease. The persistence of the infection located in the bone presented a “protective” effect against a major amputation (OR = 0.08, 95% CI = 0.03-0.22). This finding reinforces the idea of our working group that patients with osteomyelitis can be treated by means of conservative surgery and repeat RS, thus achieving limb salvage.24,25 The association of peripheral arterial disease and major amputation is well known in the medical literature and so also the impact of revascularization on achieving limb salvage in patients with diabetes and foot infections.26,27 However, the impact of revascularization in our series cannot be evaluated because until 2008, patients with critical ischemia had to be evaluated and treated in the vascular departments of teaching hospitals. Many patients included in the current series were referred to our department as “non-revascularizable patients” and it is possible that criteria in our specialized departments are quite different.27,28 We believe that if revascularization had been broadly used according to our criteria, the outcomes might have been different and fewer major amputations would have been performed. It could have been interesting to know whether level of local skin microcirculation investigated by transcutaneous oxygen pressure (TcPO2) had any impact on undergoing RS. However, TcPO2 device is available in our unit from the beginning of 2004 and it is not routinely used in every case. The present study had several limitations. First, the retrospective nature of the study might have produced bias in the results. Second, the fact that anaerobes were not grown limits the impact of GNRs on the results. Third, the criteria for revascularization were established by an external vascular department and these results could be different in departments specialized in diabetic foot problems in which revascularization is more broadly used. Finally, 10 years is a long period of study and our experience in the management of DFIs has improved throughout this period. Strengths are the fact that a large number of patients have been included in this study, data were prospectively filed in the clinical database, and all the surgical procedures were performed by the same surgeon, thus limiting the possibility of bias.
In conclusion, RS was necessary in 40% of patients with diabetes and foot infections requiring surgery. Osteomyelitis was not a predictive factor of undergoing RS. Despite the fact that 79 out of 167 patients who underwent RS (47.3%) required a higher level of surgery, limb salvage was achieved in 70.7% of patients. Predictive variables related to undergoing a major amputation after RS in the present study were ischemic heart disease, undergoing 2 or more reoperations, isolation of GNRs from tissue biopsy, and peripheral arterial disease. The persistence of the infection located in the bone presented a “protective” effect against undergoing a major amputation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.