
Abstract
Pretibial myxedema (PM) is a rare autoimmune manifestation of Graves’ disease, which commonly presents as diffuse, nonpitting edema of shins and less often as plaques, nodules, or elephantiasis lesions mimicking lymphedema. We present a 57-year-old woman with 12-month history of PM, which occurred a year after treatment of Graves’ disease and improved with topical corticosteroids, support stockings, and intralesional steroid injections until recurrence with local erythema and woody edema. A literature review was undertaken of the evidence-based treatment modalities for symptomatic PM: although commonly asymptomatic and self-limited, severe cases of PM may be treated with topical corticosteroid, compressive therapy, and intralesional corticosteroid injections.
Pretibial myxedema (PM) is a rare autoimmune manifestation of Graves’ disease. 1 PM often presents 12 to 24 months after the diagnosis of Graves’ disease and is commonly associated with severe Graves’ opthalmopathy (GO). 1 Clinically, more than 50% of patients develop diffuse, nonpitting edema of shins, and less often with plaques, nodules, or elephantiasis lesions mimicking lymphedema. 2
Case Presentation
A 57-year-old woman presented with a 12-month history of lower leg pain and pruritus aggravated by sitting or standing. She had bilateral, nonpitting edema of the anterior shins, and slight periorbital edema without exophthalmos (Figure 1). Since treatment of Graves’s disease with radioactive iodine a year previously, the patient had remained euthyroid with thyroid-stimulating hormone (TSH) levels in the normal range on levothyroxine prescribed for postradioiodine hypothyroidism. Family history was significant in that 1 of her 2 sisters died of lupus in her 30s.

Pretibial myxedema. Bilateral, nonpitting edema of the anterior shins.
A punch biopsy of the dorsal foot was consistent with PM. In March 2011, the patient was treated with topical steroids under occlusion (clobetasol propionate 0.05% daily) and 20 to 30 mm Hg knee-high support stockings. On follow-up 1 month later, the lesions treated with corticosteroids were less erythematous; however, the induration of the lesions and the edema persisted. Thyroid indices were under control (TSH 1.53, free T4 12.6, and free T3 4.0) with
After only minimal improvement eight months later, intralesional steroid injections were infiltrated into the dermal tissue. The symptoms improved within 6 weeks and the treatment regimen was continued. However, in June 2013, the PM recurred with local erythema and woody edema. Thyroid indices remained stable (serum TSH 0.36, free T4 18, and free T3 3.7); however, TSH level was on the lower end of normal, prompting a decrease in
Discussion
Pretibial myxedema is an autoimmune extrathyroidal manifestation of Graves’ disease and less often Hashimoto’s thyroiditis with an incidence of 1 case per 100 000 per year.1-3 Up to 4.3% of patients with Graves’ disease develop PM, which often presents 1 to 2 years after the diagnosis of Graves’ disease and almost always after the onset of relatively severe GO. 2 PM is almost always present with GO and 4 times more likely to occur in females.1,2
The pathophysiology of the disease is not fully understood; however, TSH receptors in the connective tissue as seen in GO may be the nonspecific antigen. The release of cytokines from T lymphocytes stimulates fibroblast for the increased production of glycosaminoglycans (GAGs) and hyaluronic acid in reticular dermis. T-lymphocyte associated antigen-4 (CTL-4) has an inhibitory effect on T-cell functions and polymorphism in this gene may be responsible for low incidence of PM in patients with Grave’s disease. 3
Histological findings characteristic to PM include extensive deposition of mucin—namely GAGs—in the reticular dermis, lack thereof in the superficial papillary dermis, stellate fibroblasts that are not increased in number, and collagen fibers that are frayed, fragmented, and preserved in the superficial papillary dermis (Figure 2).2,4,5 Findings that distinguish PM from GO are mucin deposition and dermal edema, as well as relatively small amount of lymphocyte infiltration. 2 Findings that distinguish PM from other causes of mucinosis in the pretibial area include mucin deposition in the reticular dermis, spared collagen in the superficial papillary dermis, lack of angioplasia, and absence of hemosiderin. 2
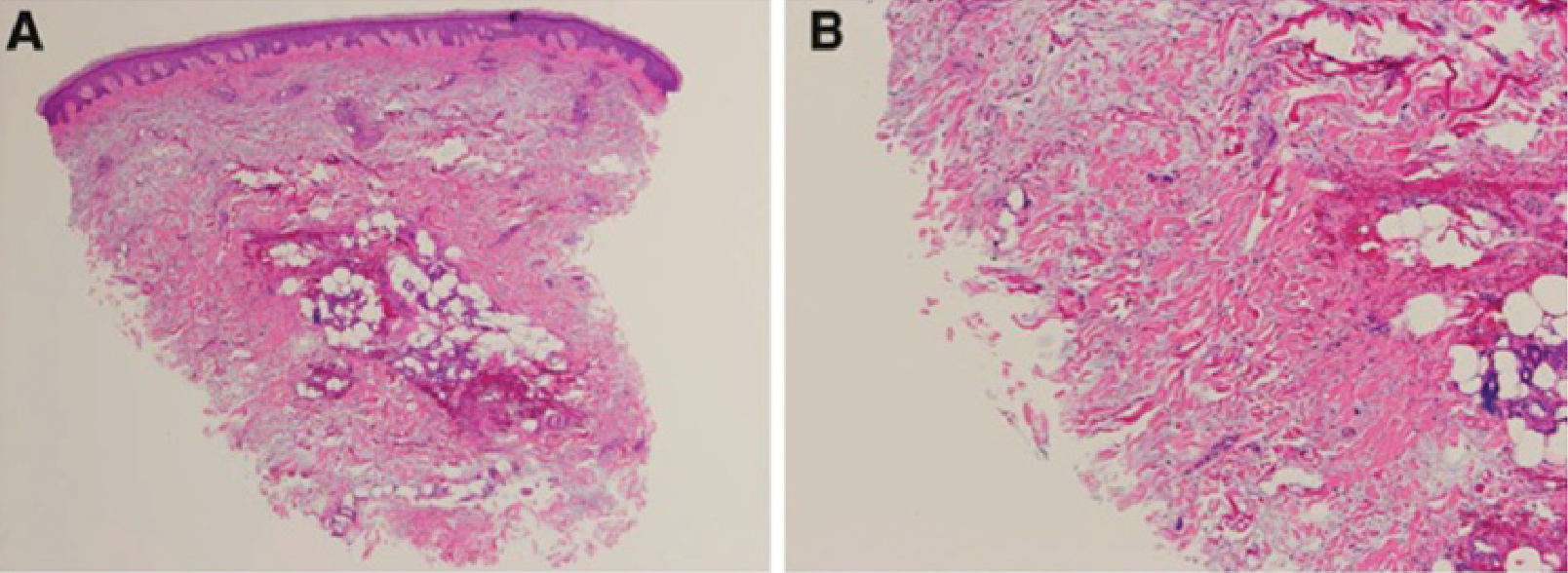
Direct immunofluorescence microscopy showing mucin deposition, stellate fibroblasts, and mast cells in the reticular dermis, consistent with pretibial myxedema. Reproduced from Lohiya et al. 1 with permission.
Clinically, more than 50% of patients develop diffuse, nonpitting edema with erythematous or flesh-colored skin lesions that resemble orange peels in appearance and texture; 21% develop plaques; 20% develop nodules; and less than 1% develop elephantiasic lesions associated with advanced dermopathy.1,2,6,7 Commonly localized in the pretibial area and occasionally in the feet and toes, lesions characteristic to PM are rarely symptomatic, neither painful nor pruritic. 2
The diagnosis of PM can be made based on the characteristic pretibial lesions, history of Graves’ disease, and presence of GO. 2 Biopsy of localized lesions, serological findings of thyroid autoimmunity (ie, presence of TSH receptor antibodies), and imaging studies may confirm diagnosis.2,8 Except in rare cases, such as when GO is absent or occurs subsequent to PM, physical examination along with history of thyrotoxicosis is sufficient to make the diagnosis. 2 The differential diagnoses include scleromyxedema (generalized lichen myxedematosus), scleredema, venous insufficiency, lipodermatosclerosis, lymphedema, obesity, and trauma (Table 1).2,4,9,10 History of thyroid disease, physical examination, and histologic characteristics help differentiate PM from other conditions that lead to similar pretibial deposition of mucin without thyroid disease. 2
Differential Diagnosis of Pretibial Myxedema, Lymphedema, and Lipodermatosclerosis.
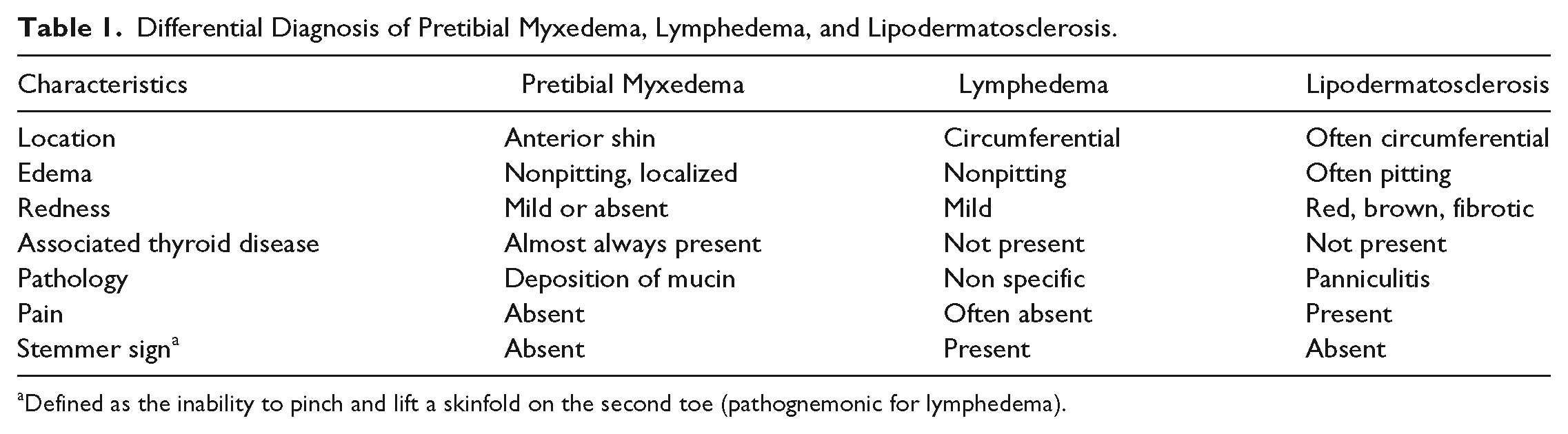
Defined as the inability to pinch and lift a skinfold on the second toe (pathognemonic for lymphedema).
Pretibial myxedema is commonly asymptomatic and has the potential of self resolution with time, so therapy is rarely needed.1,2,4,11 In more severe cases, however, cosmetic issues, impaired function, or localized discomfort may arise, in which case therapy may be appropriate.2,11 The first therapy to consider is topical corticosteroid.2,12,13 Either a mid-potency corticosteroid such as fluocinolone acetonide cream (0.2%) or high-potency corticosteroid such as clobetasol propionate may be used.2,12 The efficacy of the treatment increases as the extent and severity of lesions decrease. 13 The corticosteroid is directly applied to the lesion with occlusive dressing (hydrocolloid or plastic wrap) each night; the frequency of therapy may be incrementally reduced to 2 to 4 times per month after improvement is seen in 4 to 6 months. 14 Finally, adverse effects such as atrophy, ecchymosis, or telangiectasias should be monitored for. 15 If edema or elephantiasis is present, local compressive therapy is beneficial; use of support stockings or compressive bandages may limit the extent of disfigurement, enhance function, and avoid tissue breakdown and compressive complications.2,15 Additionally, complete decompressive physiotherapy is reported to produce sustained improvement in a patient with elephantiasic PM. 11 Another treatment option is intralesional corticosteroid injection, which has been effective in several published reports.2,15 In one case series, intermittent injections for 3 months resulted in complete remission of PM in 3 patients that was sustained for 4 months. 16 Multipoint injection of triamcinolone acetonide, administered every 25 to 28 days, for 6 months also produced complete resolution in a patient with severe PM. 17 Despite these results, further investigation is needed to better understand the long-term effects of this therapy before routine use can be recommended. 15 Other treatment modalities include surgical excision of lesions, systemic immunomodulation, and octreotide therapy, none of which have enough conclusive evidence to be recommended to patients. 15
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.