
Abstract
Impaired wound-healing activity in diabetes could result from several factors, including severely damaged angiogenic responses, which can affect wound healing process to cause delayed wound repair. Mesenchymal stem cells (MSCs) have been shown to enhance wound healing via multiple effects, including promoting angiogenesis both in vitro and in vivo; however, the mechanisms involved in enhancing diabetic wound healing are barely understood. This article reviews the recent literatures on MSCs treatment for promoting angiogenesis or vascularization in diabetic wounds and the potential mechanisms involved, with an emphasis on the role of paracrine soluble factors. Meanwhile, the potential benefits and related risks associated with the therapeutic use of MSCs have been presented and may lead to better understanding of the influence of MSCs without increasing potential risks. Further investigation will be required to determine the molecular basis of paracrine mechanisms and regulated angiogenesis of MSCs for its rational manipulation for impaired angiogenesis repair and diabetic wound healing.
Mesenchymal stem cells (MSCs) are multipotent cells were first recognized more than 40 years ago by Friedenstein. 1 MSCs are among the most promising candidates for regenerative therapies because they can differentiate into a number of cell types in vitro. Although there is evidence for MSCs differentiation in the wound, most of the therapeutic effects are likely because of MSCs releasing soluble factors that regulate local cellular responses to cutaneous injury. In recent years, numerous literature have demonstrated that soluble factors secreted by MSCs have multiple considerable effects, including angiogenesis, stimulation of endogenous progenitor cells (EPCs), modulation of inflammatory and immune reactions, and antiapoptosis effects and so on. When the angiogenic response was impaired, MSCs could secrete stromal cell-derived factor-1 (SDF-1), vascular endothelial growth factor (VEGF), insulin-like growth factor-1 (IGF-1), epidermal growth factor (EGF), keratinocyte growth factor (KGF), angiopoietin (Ang)-1, macrophage inflammatory protein (MIP)-1α and β and erythropoietin (EPO), 2 and matrix metalloproteinase-9 (MMP-9), 3 or other cytokines to stimulate recruitment, proliferation, and differentiation of EPCs, hence promoting angiogenesis and tissue regeneration. Pro-inflammatory environment may stimulate MSCs to secrete tumor necrosis factor (TNF)-α stimulated gene/protein-6 (TSG-6) and prostaglandin E2 (PGE2) or stanniocalcin-1 (STC-1) and SDF-1 or interleukin (IL)-6 and IL-8, which suppress excessive immune responses and protect the injured tissues from inflammation. In addition, direct T cell inhibition by indoleamine-2,3-dioxygenase (IDO) or PGE2, as well as immune tolerance induced by transforming growth factor-β (TGF-β) and PGE2, may also contribute to MSCs-mediated immunosuppressive effects.4,5
Diabetes mellitus (DM) is a chronic metabolic disease. Because of the long-term hyperglycemia, many complications may occur in diabetics. 6 These complications are implicated with a large number of cellular and subcellular changes on vessels, atherosclerosis, and tissue ischemia and hypoxia may be observed, which direct result in impaired wound healing. Impaired angiogenesis and diminished formation of granulation tissue are the major factors contribute to unhealing wound 7 and impairment of angiogenesis thought to play a critical role since this process is required for successful wound repair. The sufficient blood flow can deliver immune cells and metabolic substrates, which is important to wound healing. 8 Several investigations demonstrated that critical cytokines and growth factors secreted by MSCs could affect neovascularization such as extracellular matrix (ECM) molecules, VEGF, IGF-1, phosphatidylinositol-glycan biosynthesis protein class F (PIG-F), monocyte chemoattractant protein-1 (MCP-1), basic fibroblast growth factor (bFGF), and IL-6; they also stimulate mitosis of tissue-intrinsic progenitor or stem cells by secretion of stem cell factor (SCF), macrophage colony–stimulating factor (M-CSF), SDF-1, leukemia inhibitory factor (LIF), and Ang-1. 9 Based on considerable experimental and clinical data, it is evident that these factors are necessary for repairing the impaired angiogenic responses in diabetic wounds.
Paracrine Effects of MSCs on EPCs and Other cells
Endogenous progenitor cells are progenitor cells that are released by bone marrow and non–bone marrow origin tissues or organs, such as spleen, adventitia, fat tissues, vessel wall, liver, and intestine. 10 The ability of EPCs to mobilize and home to injured areas and promote vessel formation is their important characteristic. 11 Progenitor cells differentiation into endothelial cells (ECs), mobilization of EPCs, and EPCs homing can be regulated by some critical growth factors and cytokines, and most of them can be secreted by MSCs administration. These important growth factors and cytokines, including VEGF, MMP-9, SDF-1, and granulocyte macrophage colony–stimulating factor (GM-CSF), can also mediate mobilization of EPCs. 12 Figure 1 summarized the proposed critical factors and cytokines released by MSCs involved in stem cell–mediated angiogenesis under ischemia or hypoxia conditions.
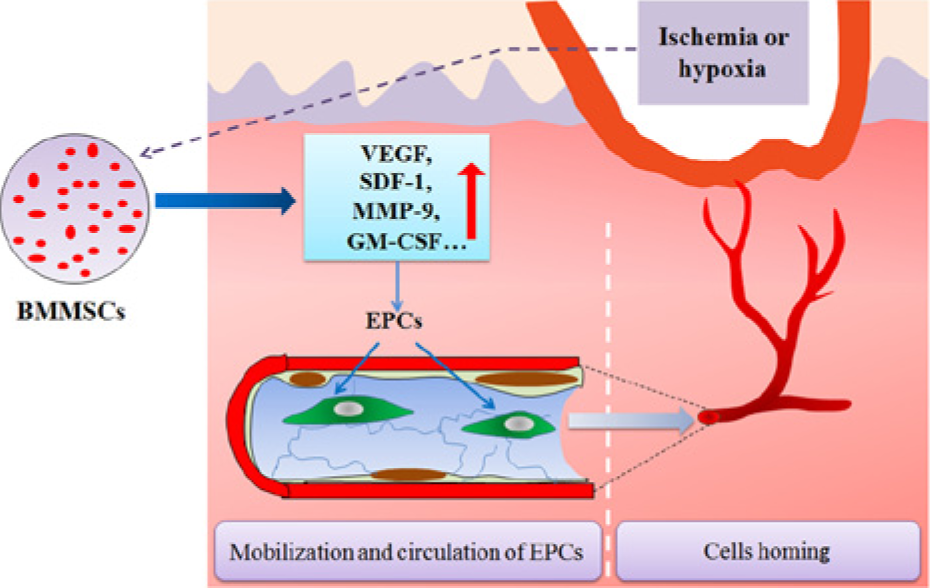
The proposed critical factors and cytokines released by mesenchymal stem cells (MSCs) involved in stem cell–mediated angiogenesis under ischemia or hypoxia conditions. Growth factors such as vascular endothelial growth factor (VEGF), stromal-derived factor-1 (SDF-1), fibroblast growth factor (FGF), matrix metalloproteinase-9 (MMP-9), platelet-derived growth factor (PDGF), and transforming growth factor (TGF) released from MSCs regulate the functions of endogenous progenitor cells (EPCs) within the wound during vasculogenesis.
Vascular Endothelial Growth Factor
Vascular endothelial growth factor plays a vital role in mobilizing EPCs effectively and inducing neovascularization. In the process of wound healing, when neovascularization is urgently required, VEGF mediates mobilization, migration, homing, proliferation, and chemotaxis of ECs. 13 VEGF has also been demonstrated to regulate the expression of endothelial cell surface proteins known as integrins, which comprise a family of transmembrane heterodimeric proteins, play a major role in regulating EPCs mobilization, homing, invasion, and differentiation when tissue injury or ischemia hasoccured. 14 Furthermore, implantation of bone marrow MSCs (BM-MSCs) were found adjacent to the ECs but not in the vascular walls, suggesting a paracrine effect of BM-MSCs with releasing great amounts of VEGF-α, IGF-1and EGF, to enhance wound healing in normal and diabetic mice associated with increased angiogenesis. 15 Accordingly, VEGF secreted by MSCs may be a critical factor responsible for an angiogenic potential of MSCs. Apart from VEGF, other molecules expressed by MSCs, including TGF-β1 and MMPs (eg, MMP-2 and MMP-14), also could contribute to MSCs–ECs interactions. 16
Matrix Metalloproteinase-9
Studies have shown that MMP-9 possess the ability to recruit EPCs from the BM. The activated MMP-9 through the conversion of Kit-ligand (KitL, stem cell factor) from a membrane-bound molecule to a survival factor soluble Kitl (sKitL) regulate cell mobility and promotes recruitment of EPCs, thereby enhancing rapid differentiation. Recruitment of EPCs to the tissue of injury and promotes neovascularization need a rapid elevation of the circulating VEGF level and is MMP-9 dependent.17,18 MMP-9 plays a vital role in augmenting EPCs mobilization and migration in a hindlimb ischemia model have been authenticated by using MMP-9 knockout mice. 19 Paradoxically, high levels of MMP-9 have been implicated in poor wound healing in diabetics, 20 but MMP-9 is upregulated during scarless wound healing in athymic nude mice, 21 and mice that lack MMP-9 also exhibit impaired wound healing with inability to properly assemble collagen fibers, and defect in keratinocyte migration. 22
Stromal-Derived Factor-1
The chemokine SDF-1 also plays a crucial role in EPCs trafficking through the circulation, 23 and the level of SDF-1 could be rapidly upregulated by a range of stimuli such as inflammatory mediators, and hypoxia. 24 SDF-1 binds exclusively to the chemokine receptor CXCR4, which could be widely expressed by EPCs, CD34+ cells and so on, SDF-1/CXCR4 interaction play a vital role in vasculogenesis, and VEGF release from EPCs has been observed enhanced when EPCs treated with SDF-1 in vitro. 25 Lack of SDF-1 has been highly implicated in age-impaired wound healing because of defective vasculogenesis. 26
Granulocyte Macrophage Colony–Stimulating Factor
Granulocyte macrophage colony–stimulating factor is a potent cytokine that can not only increase the mobilization of hematopoietic progenitor cells but also stimulate the mobilization of EPCs and enhance EPCs recruitment in hindlimb ischemia models. 27 Another report also indicated that GM-CSF could accelerate the proliferation of EPCs in vitro. MTT confirmed the effect of GM-CSF on accelerating the proliferation of EPCs. 28 GM-CSF is known to be important for ischemia wound healing, so the potential beneficial of GM-CSF released from MSCs in the application of treating diabetic patients is promising.
Angiogenic Effect of BM-MSCs-Conditioned Medium
Mesenchymal stem cells possess considerable paracrine effects that are beneficial to ECs functions. MSCs-conditioned medium significantly increased survival of ECs, which is shown by increased cell numbers through exerting cytokine effects compared with serum-free control. 29 A recent study demonstrated that MSCs-conditioned medium promote in vitro proliferation and migration of both ECs and smooth muscle cells in a dose-dependent manner. 30 In addition, VEGF is one of the most important factors contained in MSCs-conditioned medium that could potentially mediate the complex interaction of MSCs and ECs. High levels of VEGF in cell culture supernatant of MSCs could be measured when MSCs cultured in hypoxia conditions, increased sprouting of ECs could be observed when transfer the supernatant to human umbilical vein endothelial cells (HUVEC). 31
In addition, an investigation of BM-MSCs-conditioned medium prepared under hypoxic conditions suggested that the high levels of proangiogenic cytokines such as VEGF-α, IGF-1, platelet-derived growth factor (PDGF)-BB, and Ang-1 may enhance proliferation of ECs and neovascularization in the wound. 2 Angiogenic factors were significantly increased in MSCs-conditioned medium compared with conditioned medium from control constructs without cells. MMP-2, TGF-β1, and bFGF were upregulated in conditioned medium of stimulated MSCs, but levels of VEGF and hypoxia-inducible factor (HIF)-1α were unchanged in response to mechanical stimulation of MSCs. 16
Cell Survival Factors in MSCs-Conditioned Medium
Cell survival factors such as Akt (also known as protein kinase B or PKB) and endothelial nitric oxide synthase (eNOS) were strongly upregulation in MSCs-conditioned medium following brief hypoxia in vitro, and H9c2 cells treated with MSCs-conditioned medium displayed a reduction in caspase-3 activity compared with controls.32,33 Apoptosis was prevented as a result of activation of Akt survival pathway and Akt upregulation under ischemia. Similarly, chronic hypoxia increases eNOS expression and several studies clearly indicate that NO plays an important protection role after ischemic injury.
Angiogenic Effect of Adipose-Derived MSCs
Although MSCs derived from adipose tissues have similar characteristics of BM-MSCs, 34 such as proangiogenic effect in ischemia model, paracrine effects and differentiate into ECs and smooth muscle–like cells, their effects on mediating neovascularization in response to vascular ischemia are different. An investigation asserted that conditioned media from human adipose–derived MSCs (hADSCs) have better effects in vitro on tube formation and higher expression of MMP-3 and MMP-9 than conditioned media from hBMSCs, and hADSCs showed better biologic effects of increased blood flow in vivo. 35 The data revealed that hADSCs might be superior to hBMSCs in proangiogenic action in response to vascular ischemia, and seemed to be a promising candidate in the future.
Angiogenic Effect of Placenta-Derived MSCs
In recent years, placenta-derived MSCs are a very attractive source of MSCs because of the high efficiency of achievement with no intrusive procedures and few ethical conflicts. Besides the use of MSCs derived from the amniotic membrane (AM), other components of the placenta such as Wharton’s jelly (WJ) of umbilical cord as well as umbilical cord blood and vein, have been proved to possess angiogenic potential, they may also open new possibilities for promoting angiogenesis through cell-based therapeutic strategies.36 -39 Like MSCs derived from other sources, the beneficial effects conferred by placenta-derived MSCs may act mainly through paracrine secretion mechanism. In some cases, angiogenic properties of placenta-derived MSCs were higher than BM-MSCs.40,41 Therefore, although they may offer a highly promising and easily applicable option, further investigation will be required to test whether these cells are capable of enhancing diabetic wound healing.
Challenges for Translation
Mesenchymal stem cells have the potential ability to paracrine numerous growth factors, cytokines and chemokines, hence promoting angiogenesis and tissue regeneration. MSCs-based therapies with a profound and multifaceted effect on neovascularization and diabetic chronic wound healing had been demonstrated by numerous in vitro and in vivo experiments. 42 Although the mechanisms involved are not entirely clear and most of these therapies remain unproven in controlled clinical trials, several recombinant cytokines have been shown to have a considerable effect on nonhealing wounds 43 .
Numerous studies have demonstrated that angiogenesis was critical to promoting wound healing, while they are also inseparable from tumor formation and maintenance. 44 These growth factors can be secreted by MSCs, and they exert angiogenesis effects in a dose-dependent manner, the effects will be weakened or even disappeared when lower dose was used. 30 Nevertheless, these angiogenic factors such as VEGF, FGFs, TGF-β, MMP-2 could be involved in tumor angiogenesis, which is essential for tumor proliferation and metastasis in a hostile environment. 45 Hence, the potential risk of tumor growth should be considered when the therapeutic benefit of MSCs-based therapies was applied, in spite of rare probabilities. On the other hand, the paracrine effects of MSCs-based therapy represents a reasonable strategy because the beneficial multiple factors might be functioning synergistically. However, direct application of growth factors therapy remains limited because of the necessity to maintain therapeutic concentration to induce the desired effect for the necessary length of time. Different protein actions may require different concentrations and timing. Protein stability and pharmacokinetics represent other possible hurdles.
Recently, MSCs-based cellular therapies have received significant attention; meanwhile, the questions about aging of MSCs have also been raised. A decline of proliferative capacity was observed in aged MSCs compared with young donors. 46 Angiogenic factors such as TGF-β secreted by MSCs were found to be decreased with aging, 47 which indicated that agiogenic effects of aged MSCs was downregulated. Angiogenic gene expression can be partially be improved by hypoxic preconditioning; however, the effect is also age dependent. 48 Above all, several evidences showed that distinct changes in quantity, regeneration capacity, mobilization capacity were observed within aged MSCs. 49 These results imply that MSCs-based therapeutic approaches for the elderly should focus on augmentation of secretion or allogenic transplantation research, rather than simply stimulating cell proliferation.
Discussion
Chronic wounds especially in elderly patients with diabetes are common diseases in the clinical setting; because of nonhealing properties, many patients will face the risk of amputation.50,51 One possible reason is that aging could induce cellular senescence, leading to inflammatory cytokine generation and impaired adipogenesis. A variety of physiologic factors involved in impaired wound healing or in the diabetic foot ulcer and decreased expression of growth factors contribute to the occurrence of the pathological process of impaired angiogenesis. 52 Numerous literature demonstrate that BM-MSCs secrete a broad spectrum of cytokines, which stimulate EPCs, ECs, and smooth muscle cells to proliferate and migrate. These effects are dose dependent and appear to be mediated by several cytokines. In addition, these angiogenic factors and chemokines secreted by MSCs also contribute to other important effects such as increased survival of ECs and promoting tube formation and antiapoptosis. Based on these and the previously described observations, one could speculate that implantation of MSCs promoted wound healing, at least in part, result from their angiogenic action.
On the other hand, analyses of BM-MSCs-conditioned medium by antibody-based protein array and ELISA indicated that BM-MSCs secreted greater amounts of distinctively different cytokines and chemokines, compared with normal dermal fibroblasts. These molecules are known to be important in normal wound healing and diabetic wound healing. BM-MSCs-conditioned medium might also significantly enhanced migration and proliferation of macrophages, keratinocytes, and ECs compared with fibroblast-conditioned medium. Furthermore, local injection of MSCs-conditioned media alone in a diabetic mouse model could accelerate wound healing.
Recent and ongoing studies demonstrated angiogenic effect of MSCs secreted factors is a promising therapeutic target for enhancing diabetic wound healing. Hypoxic conditioning of MSCs can increase angiogenic properties via secreted more factors, and might therefore be considered useful in MSCs-based therapies for angiogenesis. A further understanding of the molecular basis of paracrine mechanisms and regulated angiogenesis might allow for rational manipulation of MSCs without increasing the potential risks. In the future, another possibility is that cell-free treatments based on the use of rich angiogenic factors–conditioned medium will represent a novel therapeutic strategy.
Footnotes
Authors’ Note
Chengwei Gu, MM, Sha Huang, PhD, and Dongyun Gao, MM, contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the National Nature Science Foundation of China (81121004, 81230041, 81372066) and the National Basic Science and Development Program (973 Program, 2012CB518105).