
Abstract
Lipedema is a disorder of adipose tissue that primarily affects females and is often misdiagnosed as obesity or lymphedema. Relatively few studies have defined the precise pathogenesis, epidemiology, and management strategies for this disorder, yet the need to successfully identify this disorder as a unique entity has important implications for proper treatment. In this review, we sought to review and identify information in the existing literature with respect to the epidemiology, pathogenesis, clinical presentation, differential diagnosis, and management strategies for lipedema. The current literature suggests that lipedema appears to be a clinical entity thought to be related to both genetic factors and fat distribution. While distinct from lymphedema and obesity, there are some existing treatments such as complex decongestive physiotherapy, liposuction, and laser-assisted lipolysis. Management of lipedema is complex and distinct from lymphedema. The role of newer randomized controlled studies to further explore the management of this clinical entity remains promising.
Keywords
Introduction
Lipedema is a disorder of adipose tissue that is characterized by abnormal subcutaneous fat deposition presenting by swelling and enlargement of the lower limbs (Figure 1). 1 Although lipedema is commonly misdiagnosed as lymphedema or simple obesity, it appears to be a distinct entity with possible inheritance of X-linked dominant or autosomal dominant pattern with sex limitation. 1 It commonly affects females at a young age and significantly affects activities of daily living. The diagnosis of lipedema is frequently missed due to unfamiliarity of clinicians with this condition. Health care professionals need to be familiar with this disease to be able to provide a proper approach. Advanced cases of lipedema led to venous disease (venolipedema), lymphatic abnormalities (lympholipedema), and subsequently ulceration and recurrent infection. In this review, we discuss the epidemiology, pathogenesis, clinical presentations, differential diagnosis, and management options of this often misdiagnosed disease.

Lipedema: disproportionate swelling of waist and lower extremities while feet are spared. This creates “cuff sign.”
Epidemiology
Lipedema was originally described by Allen and colleagues as “large legs due to the subcutaneous deposition of fat in the buttocks and lower extremities and the accumulation of fluid in the legs.” 2 The condition is found almost exclusively in females, although there have been some reports of lipedema in males.2-4 The majority of patients with lipedema have high body mass index (BMI), are either overweight or obese, although most patients have a normal appearance above their waist, accounting for a disfigurement between their lower and upper extremities.1,4
The onset of lipedema is usually between the teenage years or third decade of life. 4 There are some reports of the disease onset after pregnancy or even menopause. 1 Although the evidence on the epidemiology of lipedema in the current literature is limited, Child et al estimated the minimum prevalence to be 1 in 72 000 though this may be an underestimate due to misdiagnosis or lack of referrals. 1 Other studies have cited lipedema to affect up to 11% of women or postpubertal girls to some extent. 5 Furthermore, in 2 different studies the prevalence of lipedema in patients referred to lymphedema clinic was reported as 10% to 15%.6,7 Although lipedema is not currently recognized as a hereditary disease, studies suggest that positive family history in patients with lipedema ranges between 16% and 64%. 8
Pathogenesis
The pathophysiology of lipedema appears to be multifactorial but initial studies have suggested that microangiopathy in affected adipose tissue leads to increased permeability of proteins and increased capillary fragility. 4 It is well known that hypoxia is an induction factor for the development of angiogenesis, which in many cases can lead to pathological effects, for instance, the development of diabetic retinopathy. 9 As fragility of capillary vessels is a common feature in both angiogenesis and lipedema, investigators have delved into this idea to find a link between the two. Siems et al 10 in fact discovered that in patients undergoing shock-wave therapy for lipedema or cellulite, the average value of VEGF, or vascular endothelial growth factor, was 530 pg/mL, compared to normal values of plasma VEGF, which are reported to be 100 to 130 pg/mL. 10 These findings suggest that pathological angiogenesis may play a role in the development of lipedema.
Another theory regarding the pathophysiology of lipedema is based on a study by Suga et al. 11 Here, the authors carried out immunohistochemical analyses of lipedema tissue, which were characterized by crown-like structures (necrotizing adipocytes surrounded by infiltrating CD68+ macrophages), which is a feature commonly seen in obese adipose tissue. Furthermore, there was a proliferation of adipose-derived stem cells, progenitor cells, and stromal cells (Ki67+ CD34+ cells). Such findings suggest that one possible mechanism leading to the development of lipedema may involve one of increased adipogenesis, leading to hypoxia, and further adipocyte necrosis and macrophage recruitment.11-13
A previous study by Bilancini et al 14 used dynamic lymphoscintigraphy, a measure of lymphatic function, in 12 women affected by lipedema, with comparison to 5 normal subjects and 5 patients suffering from idiopathic lymphedema. Patients with lipedema demonstrated an abnormal lymphoscintigraphic pattern with slowing of lymphatic flow, in a similar manner to patients with lymphedema. Fat deposition can lead to micro-lymphatic disturbances and lipolymphedema after the long-term presence of lipedema.15,16 Although the effects of obesity on lymphatic function have been poorly understood, in an animal study, Blum et al demonstrated that adipose tissue expansion leads to a functional impairment of the collecting lymphatic vessels. 17
A similar study by Harwood et al 18 also investigated photoplethysmography, which measures venous function, and quantitative lymphoscintigraphy in 10 patients with lipedema compared to healthy volunteers. Results demonstrated that there were only minor abnormalities of venous function in 2 patients, moderately impaired lymphatic function in both legs of 1 patient, and marginal impairment in one or both legs of 7 patients. 18 Thus, unlike lymphedema, lipedema may not be entirely due to a primary venous or lymphatic disturbance but rather, as mentioned previously, a form of lipodystrophy or diffuse lipomatosis. The female predominance and onset after puberty suggest a hormonal influence on disease phenotype. 1
Clinical Presentations
The diagnosis of lipedema is a clinical diagnosis and sometimes challenging. Wold et al proposed a series of criteria to diagnose lipedema, which include the following: (a) occurrence almost exclusively in women; (b) bilateral and symmetrical nature with minimal involvement of the feet (reverse shouldering) 1 ; (c) minimal pitting edema; (d) pain, tenderness, and easy bruising; and (e) persistent swelling of lower extremities despite elevation or weight loss.1,2 Unlike obesity or lymphedema, lipedema typically affects those between the ages of 10 and 30 years, and most commonly affects the bilateral legs, thighs, and buttocks (Figure 2). 4

Lipedema: symmetrical bilateral increase of adipose tissue that typically affects the hips, buttocks, thigh, and calves.
In a typical presentation of lipedema, the enlargement of the lower extremities is disproportionately greater than that of the trunk and upper extremities. 8 Initially, the first sign indicating the development of lipedema may be filling of the retro-malleolar sulcus on both lower extremities; in most cases, the feet are unaffected and the fat begins to accumulate above both malleoli, which creates for a visible distinction between the normal and abnormal tissue near the ankle, known as the “cuff sign” (Figure 1). 8 In addition, fat pads are usually found anterior to the lateral malleolus with additional tissue present between the Achilles tendon and medial malleolus. 4 The skin is usually normal in appearance, and there is no apparent dermal thickening or induration, which is a common feature found in lymphedema (Figure 3). In some cases, there may also be extensive fatty deposition in the upper extremities that spares the wrist, in the same manner as the feet are spared in the lower extremities. 8

Lymphedema: involvement of skin with inflammation and fibrosis is common in lymphedema and feet are involved.
Other clinical features of lipedema may include a mild pitting edema that can improve with elevation and a sensation of heaviness or discomfort in the legs that is worsened with pressure; this feature has previously been described in the literature as “painful fat syndrome.” 4 The presence of tenderness has been reported in 70% of these patients. 1 A report by Meier-Vollrath and Schmeller has also described a staging system to categorize the severity of lipedema: stage I being described as “flat skin with enlarged subcutis,” stage II as “walnut to apple-like indurations akin to a mattress,” and stage III as “larger indurations and deforming fat deposits.”4,19
In addition, literature has also subcategorized the clinical manifestations of lipedema into 2 main clinical phenotypes: columnar and lobar. The columnar phenotype is typically defined as enlargements of the lower extremities appearing as a series of conic sections, whereas the lobar type is defined as large bulges or lobes of fat overlaying the lower extremities, hips, and/or upper arms. 5
Differential Diagnosis
Lipedema is often misdiagnosed clinical entity. 13 Distinguishing lipedema from obesity is not always easy. Patient history and physical examination provides clues to the diagnosis. 5 Lipedema has an association and clinical resemblance to generalized obesity and is frequently misdiagnosed as such. BMI is helpful in some cases although other cases of lipedema in a later stage of life develop obesity. In a study by Child et al, on 38 patients with lipedema, the BMI of the majority of patients with lipedema was consistent with either overweight (BMI = 25-29.99, 11%) or obese class I (BMI = 30-34.99, 80%). Patients with lipedema have no response to restricted diet intake especially in the waist and lower extremities. 1
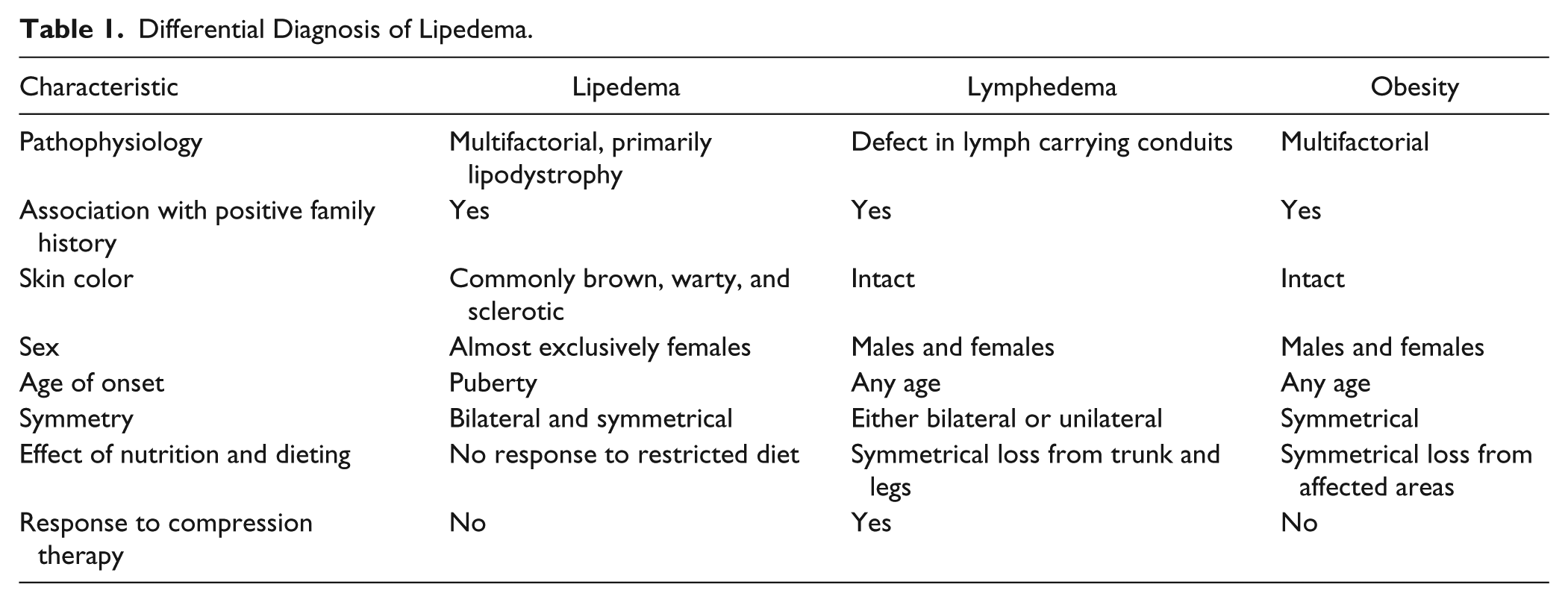
Lymphedema is the accumulation of protein-rich fluid in the interstitial tissue due to lymph drainage failure. Lymphedema commonly responds to compression therapy, while lipedema responds poorly to compression therapy. The primary cause of lymphedema is due to an inherent defect within the lymph carrying conduits and is either familial or sporadic. Lipedema is symmetrical while lymphedema is usually asymmetrical. The skin in patients with lymphedema is brown, warty, and sclerotic, while the skin in lipedema is commonly intact (Figure 3). Stemmer sign, or the inability to pinch the base of the second toe, is also a unique characteristic symptom for lymphedema. 20 A more complete list of differences between lipedema and lymphedema can be found in Table 1.
Differential Diagnosis of Lipedema.
Different types of lipodystrophy are in differential diagnosis, but many of these patients have distinct presentations and abnormal glucose metabolism. 1
Management
The management of lipedema includes conservative treatment of secondary edema and the surgical intervention for debulking of fat tissues (Table 2). 13 Szolnoky et al investigated the role of complex decongestive physiotherapy as a treatment option for patients suffering from lipedema. 21 The authors measured capillary fragility (CF) before and after complex decongestive physiotherapy (CDP) to determine whether CDP may reduce CF. A total of 38 women were included in the study; 21 were patients treated with CDP and 17 with moisturizers as a control. CDP consisted of daily manual lymph drainage, intermittent pneumatic compression, and multi-layered short-stretch bandaging throughout a 5-day course. Results demonstrated that CDP significantly reduced the number of petechiae in the treatment group, in addition to significantly reducing CF in such patients. Thus, CDP was demonstrated as a management option for reducing hematoma formation in patients with lipedema. 21
Treatment Options for Lipedema.
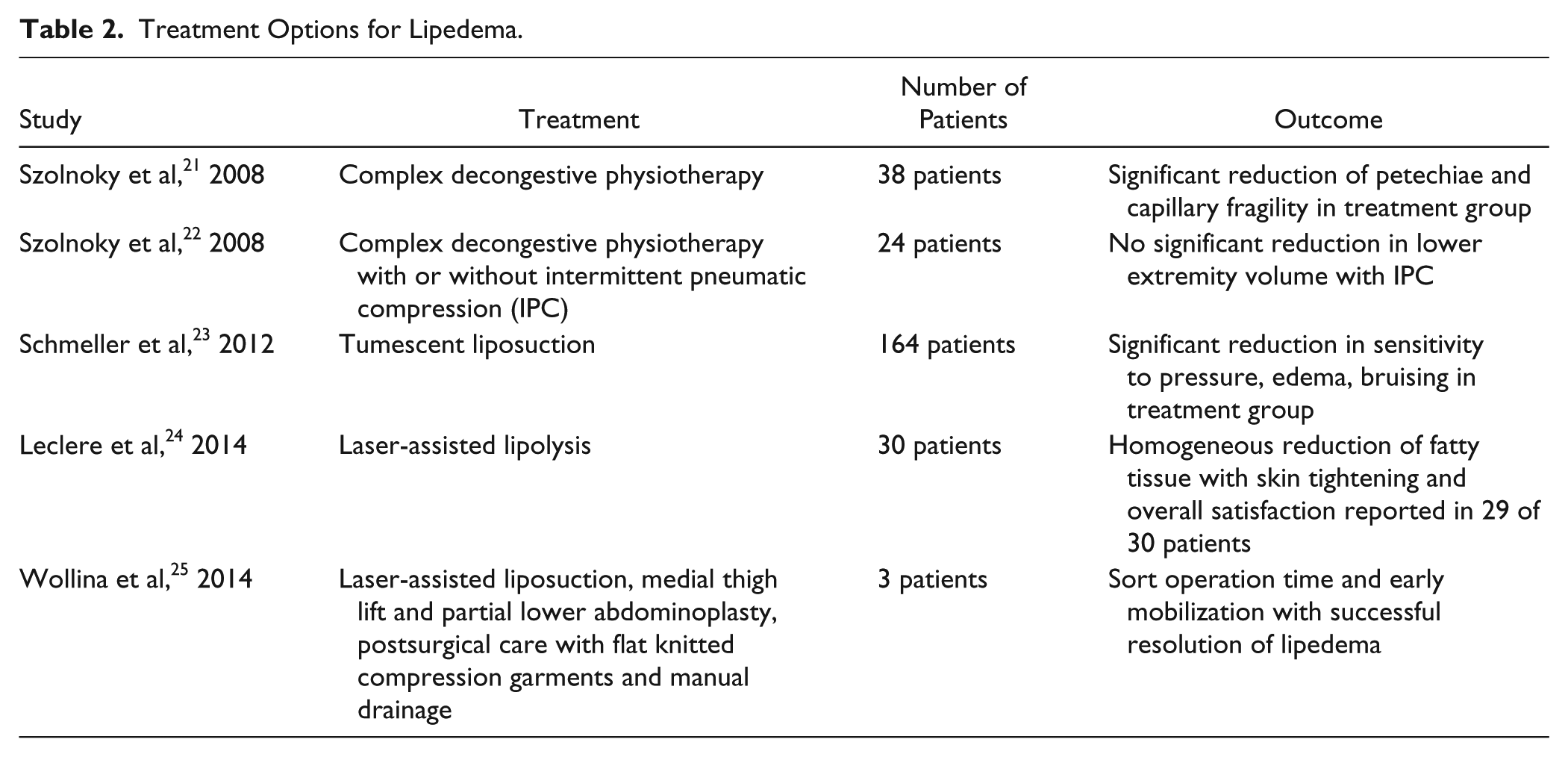
In a subsequent study, Szolnoky et al studied whether CDP alone or combined with intermittent pneumatic compression (IPC) could improve treatment outcomes in women with lipedema. 22 In both groups, there was a significant reduction in mean lower extremity volume (P < .05), demonstrating that although IPC is safe in such patients, it does not add significant value to CDP without IPC in reducing leg volume. 22
Recent investigations have also sought to determine the efficacy of liposuction as a treatment option for lipedema.23,24 A total of 164 patients included in the study underwent liposuction under tumescent local anesthesia with vibrating microcannulas. In all, there was an average reduction of 9846 mL of subcutaneous fatty tissue per person. In addition, patients undergoing the procedure reported less sensitivity to pressure, less edema, less bruising, and fewer restrictions of movement and cosmetic impairment (P < .001). Additionally, no serious complications occurred following surgery, with the wound infection rate at 1.4% and bleeding rate at 0.3%. Tumescent liposuction was demonstrated to be highly effective for lipedema patients both cosmetically and functionally. 23 Cankles refer to the area where the calf and ankle meet; cankle remodeling is an indication for laser-assisted lipolysis in these patients. Recent studies have also demonstrated successful use of this form of treatment for patients with lipedema. 24
In a recent case series, Wollina et al reported a combined approach to improving advanced lipedema in elderly females with multiple comorbidities. 25 Three women aged 55 to 77 years with advanced lipedema of the legs underwent microcannulas laser-assisted liposuction of the upper legs and knees, medial thigh lift, and partial lower abdominoplasty with minimal undermining to correct skin laxity and prevent intertrigo. This was followed by postsurgical care with nonelastic flat knitted compression garments and manual drainage. Albeit a small case series, the authors demonstrated a short operation time and early mobilization. Furthermore, there were minor adverse effects (including temporary methemoglobinemia due to anesthesia and postsurgical pain) and no severe adverse effects. In patients with multiple comorbidities, this step-by-step approach for managing lipedema seems safe and efficacious for potential further exploration.15,25
Conclusion
Lipedema is an underdiagnosed entity and commonly misdiagnosed with lymphedema. Management of the 2 conditions is different. Awareness of the lipedema presentations enables clinicians to diagnose and manage these patients appropriately.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.