
Abstract
This cross-sectional study investigated the prevalence and correlates of lower-extremity amputation (LEA) in a Saudi population with diabetic foot ulcer. The study population consisted of 91 participants, with a median age of 55.0 years. Biomarkers were measured following standard protocols. Local symptoms of foot ulcer, including peripheral neuropathy (PN), peripheral artery disease (PAD), and foot infection were diagnosed by standard objective diagnostic tools or diagnosed clinically by a specialized surgeon. The severity of foot ulcer was classified according to the Wagner wound classification system. The prevalence of LEA was 29.7% in this population. The odds ratio for LEA comparing extreme tertiles was 2.42 (95% confidence interval [CI] = 0.70-8.45; P for trend = .03) for ulcer size and 0.22 (95% CI = 0.06-0.87; P for trend = .03) for high-density lipoprotein cholesterol. C-reactive protein and homocysteine levels were each positively associated with odds of LEA, but the associations became nonsignificant in multivariable models. Participants with foot infection showed a significantly higher adjusted prevalence of LEA (40.7%, 95% CI = 27.1%-54.3%) compared with those without foot infections (19.3%, 95% CI = 6.0%-32.4%, P = .03). Participants with Wagner grade ≥3 presented a significantly higher prevalence (40.5%, 95% CI = 27.8%-53.2%) than those with Wagner grade of 1 or 2 (16.4%, 95% CI = 2.4%-30.5%, P = .02). Participants with PN and PAD showed nonsignificantly higher prevalence of LEA. We found a relatively high prevalence of LEA as well as several clinical markers and local symptoms associated with LEA in this Saudi population with diabetic foot ulcer.
Foot ulcer is a common and refractory complication among diabetic patients. The lifetime risk of developing foot ulcer is as high as 25% among diabetics in Western populations. 1 One major and feared outcome of diabetic foot ulcer is lower-extremity amputation (LEA). It demands long and intensive care, impairs the life quality of patients, 2 and causes catastrophic health care expenditure.3,4 For example, in 2012, the average cost of the care of LEA caused by diabetic foot ulcer was $50 351 per patient in the US Veterans Affairs Healthcare System. 3 Although epidemiological and clinical data were critical for creating guidelines on prevention and standard care of diabetic foot, 5 existing data, especially those on amputation, are still limited. 6 Some efforts have been made to identify risk factors with potential predictive power for diabetic foot outcomes, including amputation and mortality, in certain risk classification systems.7-10 However, clinical application of these risk factors in different populations with heterogeneous environmental and genetic backgrounds remains controversial.8,9
Because of dramatic changes in lifestyle and diet, the prevalence of diabetes has been soaring in Saudi Arabia (SA) in the past decades. By 2013, SA was ranked as having the seventh highest adult diabetes prevalence (23.9%) in the world. 11 Accompanying this diabetes epidemic, foot complications of diabetes have imposed a heavy burden on the health care system in SA. 12 However, the latest report on amputation among diabetics in SA was in 1996 and found a relatively lower prevalence of amputation compared with the Western population. 13 In this study, we investigated (1) the prevalence of LEA and (2) the associations of clinical markers and local symptoms with LEA among patients with diabetic foot ulcer in Jeddah, SA.
Patients and Methods
Potential participants from Jeddah Governance, SA, were recruited between June 2009 and May 2010. Participants 30 years or older, who had diabetes for at least 2 years and currently had diabetic foot ulcer, were eligible for this study. The diagnosis of diabetes mellitus was first self-reported by patients and then confirmed by physicians using medical records. The final study population comprised 91 participants. The study was approved by the King Abdulaziz University Hospital bioethics and research committee (No. 297-09). Study methods, benefits, and adverse reactions and objectives of this study were explained to all participants. Written consent was obtained from all participants. Information on age, smoking status, and duration of diabetes and foot ulcer were collected by specialized physicians.
Foot Ulcer Characterization
Foot ulcer was defined as a break in continuity of full thickness of foot skin, including surgical wounds for abscess drainage, and diagnosed by a specialized surgeon. 14 Duration of foot ulcer was categorized into <1, 1 to 2.9, and ≥3 months. Ulcer size was calculated by multiplying the largest by the second-largest diameter perpendicular to the first.
Clinical Markers
Duration of diabetes was categorized into 2 to 4.9, 5 to 9.9, 10 to 19.9, and ≥20 years. We measured the participant’s body weight to the nearest of 0.1 kg by using an electronic weighing scale (Seca, Birmingham, UK). We also measured their height to the nearest 0.5 cm using a stadiometer (Seca, Birmingham, UK). Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared (kg/m2). Waist circumference was measured as the smallest circumference between the rib margin and iliac crest. Obesity was defined as BMI ≥30 kg/m2. Abdominal obesity was defined as waist circumference ≥102 cm for men and ≥88 cm for women. We measured the participants’ blood pressures twice in their right arm in a seated position after 5 minutes of rest by using an electronic vital signs monitor (SuresignsVs3, Philips medical system, Andover, MA). The mean of the 2 consecutive readings of blood pressure was used for analysis. Hypertension was defined as systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg 15 and/or use of blood pressure–lowering drugs. Participants were instructed to fast and abstain from vigorous exercise for 12 hours prior to medical examination and blood draw. Fasting venous blood samples (10 mL) were taken from the antecubital vein by the laboratory staff at the time of enrollment and sent to the King Abdulaziz University hospital’s accredited central laboratory for daily assay. Fasting blood glucose, glycated hemoglobin (HbA1c), lipid profile (high-density lipoprotein [HDL], low-density lipoprotein [LDL], triglyceride), homocysteine, creatinine, and high-sensitivity C-reactive protein (CRP) levels were measured using standard methods.
Local Symptoms of Diabetic Foot
In this analysis, local symptoms of diabetic foot included peripheral artery disease (PAD), peripheral neuropathy (PN), and foot infection. Using a bidirectional hand-held Doppler ultrasound instrument (Huntleigh Diagnostics, Cardiff, UK), one trained nurse, under the supervision of a vascular specialist, measured the participant’s 2 ankle blood pressures at the posterior tibial and dorsalis pedis arteries in both legs while the participant was in the supine position. The ankle-brachial index (ABI) was computed by taking the higher pressure of the 2 arteries at the ankle divided by the average of brachial systolic blood pressure measurements or the higher of the 2 brachial values if the difference between the 2 brachial readings ≥10 mm Hg. 16 Diagnosis of PAD followed the American College of Cardiology and American Heart Association Practice Guidelines for the Management of Patients with PAD. 17 PAD was diagnosed as ABI <0.9 in either leg. In participants with ABI >1.4, the toe brachial index (TBI) was calculated by dividing the systolic pressure of the great toe by that of the brachial artery. In this case, PAD was diagnosed as TBI <0.7 in either leg. 18 PN was defined as reduced vibration perception and/or reduced light touch perception in either foot of a patient with at least 1 of the following symptoms: loss of sensations, tingling, and deformed foot. Vibration perception was assessed over bony prominences on the dorsal aspect of the first and fifth metatarsal heads using the Horwell Neurothesiometer (Scientific Laboratory Supplies, Nottingham, UK). Reduced vibration perception was defined by a vibration perception threshold ≥25 V in either foot. 19 Light touch perception was evaluated using a 10-g Semmes-Weinstein monofilament (Huntleigh Diagnostics, Cardiff, UK) at the plantar aspect of the first and fifth metatarsal heads. 20 Loss of sensations at these areas in either foot was defined as reduced light touch perception. Infection was diagnosed based on the presence of 2 or more of the following signs: frank purulence, local warmth, periwound redness, lymphangitis, periwound edema, pain or tenderness on palpation, or fever. 7 To characterize the severity of foot ulcer, we classified participants according to the Wagner wound classification system. The grades of the Wagner system are defined as follows: grade 0, skin lesions absent, hyperkeratosis below or above bony prominences; grade 1, skin and immediate subcutaneous tissue are ulcerated; grade 2, lesions are deeper and may penetrate to tendon, bone, or joint capsule; grade 3, deep tissues are always involved, and osteomyelitis may be present; grade 4, gangrene of some portion of the toes or forefoot; and grade 5, the entire foot is gangrenous. 21 All the assessments were conducted by an assessor first and then confirmed by a second assessor independently.
Ascertainment of Outcome
LEA was defined as complete loss in the transverse anatomical plane of any part of the lower limb 22 and diagnosed at the enrollment of this study by the same specialized surgeon. In this study, LEA included amputations through or proximal to the tarsometatarsal joint as well as those from distal to the tarsometatarsal joint.
Statistical Analysis
All the continuous variables are presented as medians and interquartile ranges. Comparison of continuous variables between participants who had and who had not undergone LEA was conducted using the 2-sample Wilcoxon rank-sum test. All the categorical variables are presented as numbers and percentages. The χ2 test was used to compare the distribution of categorical variables between participants with and without LEA. We further investigated the associations of the clinical markers that significantly related to LEA in univariate analysis and local symptoms with LEA using multivariable models. We used the logistic regression model to estimate the odds ratio (OR) and its 95% confidence interval (CI) for each tertile of clinical markers to investigate their associations with LEA. The first logistic model (model 1) was adjusted for sex and age (continuous); the second logistic model (model 2) was further adjusted for presence of foot infection (yes, no) and duration of foot ulcer (<1 month, 1 month, and ≥3 months). For the associations between local symptoms and LEA, we calculated the adjusted prevalence of LEA for participants with or without certain local symptoms. We used a generalized linear model for this calculation, with multivariate adjustment for sex and age. All statistical analyses were conducted using SAS 9.4 software (SAS Institute, Cary, NC). All P values were 2 tailed (α = .10).
Results
Table 1 shows the characteristics of the study population and results from univariate analyses. The prevalence of LEA was 29.7% in this population, with a median age of 55.0 years. Among 27 participants who had undergone LEA, only one was a major amputation (amputation above the ankle). More than half of the participants (52.7%) had had diabetic foot ulcers for 3 months or longer. About 60% of the participants had Wagner grade of 3 or 4. Among our study population, 68 patients presented with only PN (74.7%), 14 patients presented with both PN and PAD (15.4%), and no patients presented with only PAD. Participants who had undergone LEA had longer durations of foot ulcers (P = .02) and were more likely to have foot infection (P = .02). We found higher prevalence of PN (P = .004) and dyslipidemia (P = .006) among LEA cases. Participants who had undergone LEA also showed higher levels of homocysteine (P = .02) and CRP (P =0.06) but lower levels of HDL (P = .05), fasting blood glucose (P <0.001), and HbA1c (P = .003). The level of ABI was slightly lower among participants who had undergone LEA compared with those who had not, but the difference was not significant (P = .42).
Characteristics of the Study Population.
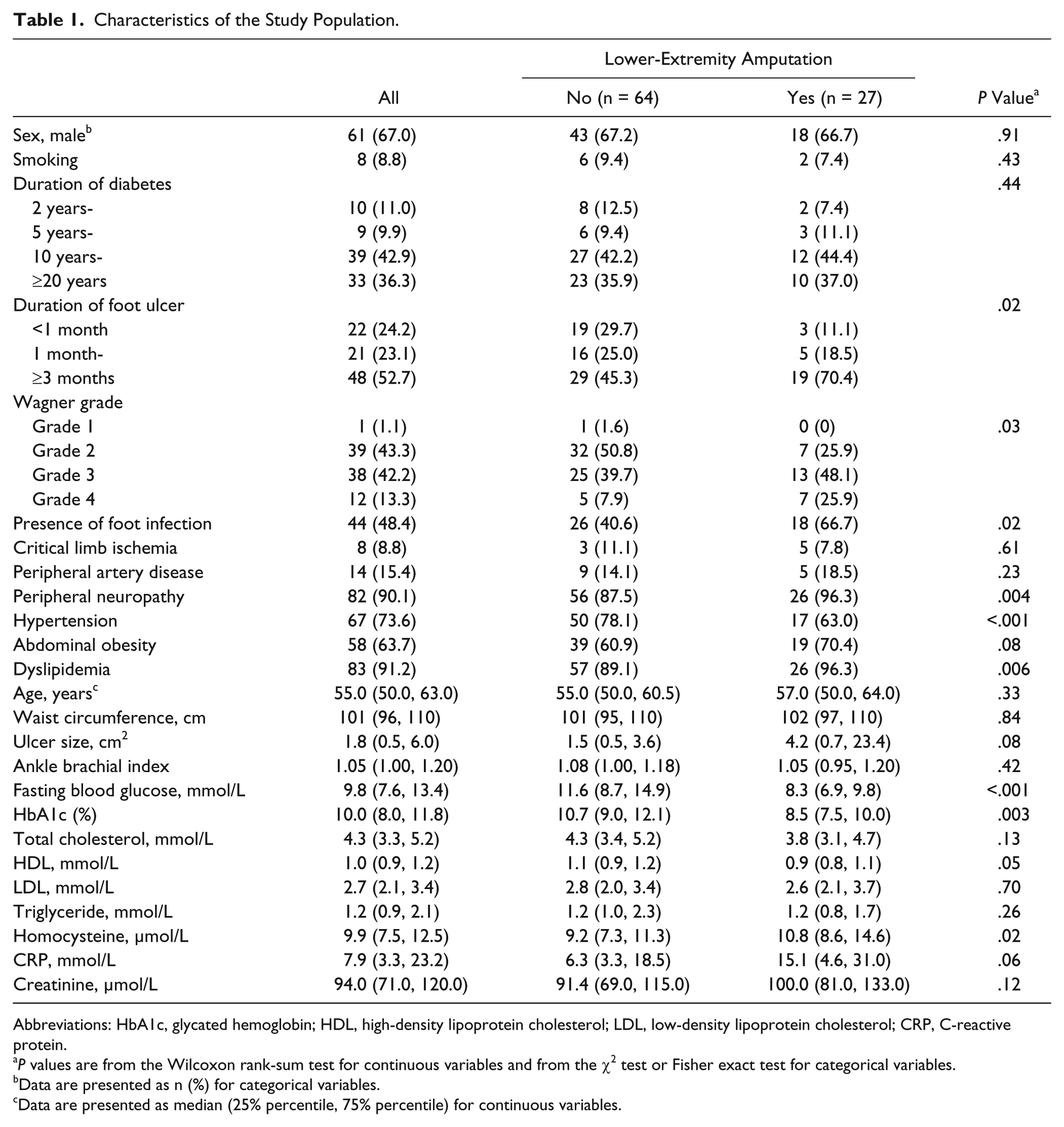
Abbreviations: HbA1c, glycated hemoglobin; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol; CRP, C-reactive protein.
P values are from the Wilcoxon rank-sum test for continuous variables and from the χ2 test or Fisher exact test for categorical variables.
Data are presented as n (%) for categorical variables.
Data are presented as median (25% percentile, 75% percentile) for continuous variables.
Table 2 presents the associations between clinical markers and LEA. Ulcer size was positively associated with odds of LEA, independent of duration of ulcer and foot infection (P for trend = .03); OR for LEA comparing the top to the lowest tertile of ulcer size was 2.42 (95% CI = 0.70-8.45). We found an inverse association between HDL level and LEA (P for trend = .03). Participants in the highest tertile of HDL had a 78% (OR = 0.22; 95% CI = 0.06-0.87) lower odds of LEA compared with those in the lowest tertile. CRP and homocysteine levels were each positively associated with odds of LEA. However, the associations became nonsignificant after further adjustment for presence of foot infection and duration of foot ulcer (P for trend = .17 for CRP and .30 for homocysteine).
Odds Ratio (95% Confidence Interval) of Lower-Extremity Amputation According to Tertiles of Correlates.
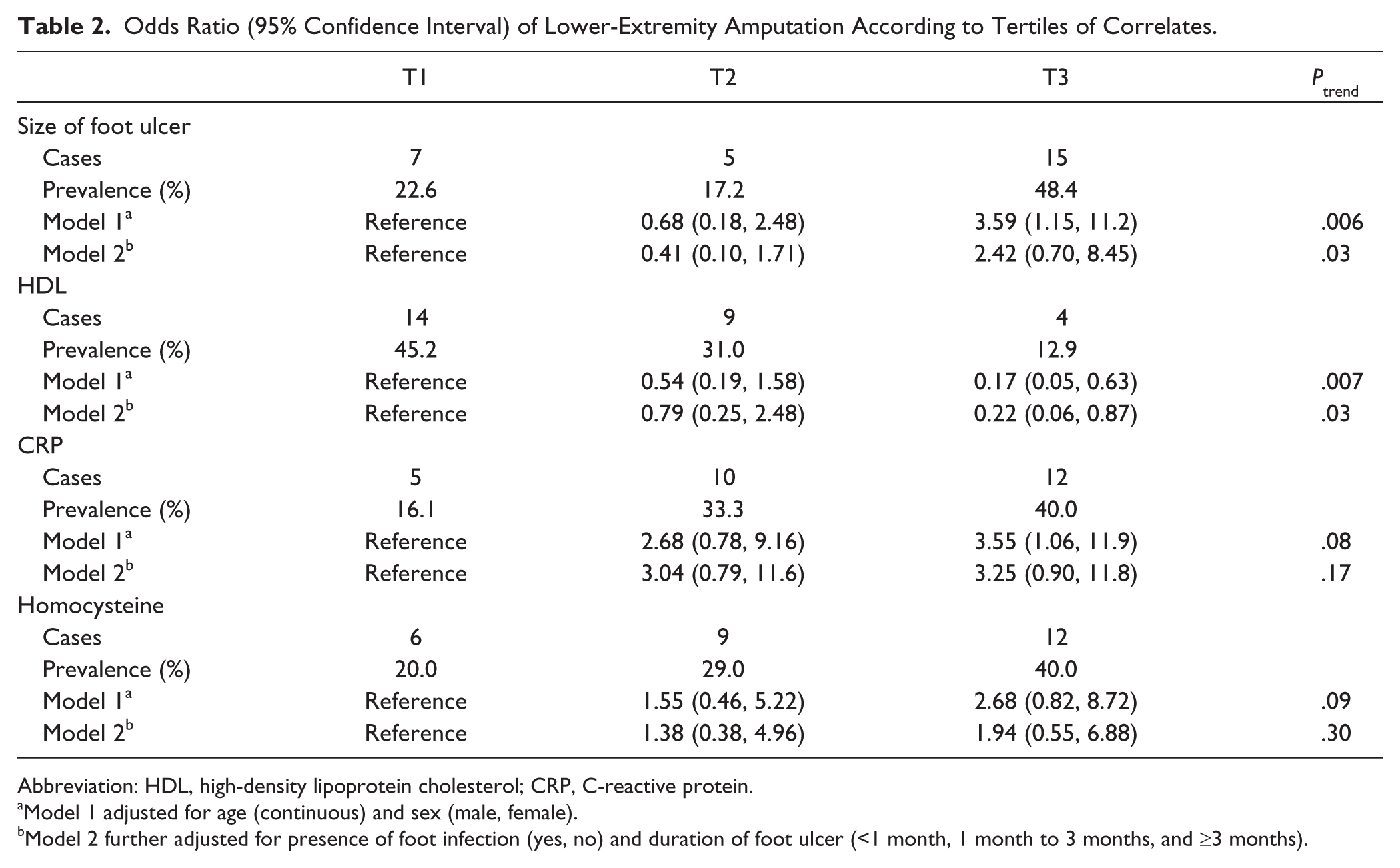
Abbreviation: HDL, high-density lipoprotein cholesterol; CRP, C-reactive protein.
Model 1 adjusted for age (continuous) and sex (male, female).
Model 2 further adjusted for presence of foot infection (yes, no) and duration of foot ulcer (<1 month, 1 month to 3 months, and ≥3 months).
Participants with local symptoms of diabetic foot generally presented with higher adjusted prevalence of LEA (Figure 1). Participants with foot infection showed a significantly higher adjusted prevalence of LEA (40.7%, 95% CI = 27.1%-54.3%) compared with those without foot infections (19.3%, 95% CI = 6.0%-32.4%, P = .03). Although higher adjusted prevalence of LEA was found among participants with PN and PAD, the differences in the prevalence of LEA were not statistically significant between participants with and without these 2 local symptoms. Participants with Wagner grade ≥3 had a significantly higher prevalence (40.5%, 95% CI = 27.8%-53.2%) than those with a Wagner grade of 1 or 2 (16.4%, 95% CI = 2.4%-30.5%, P = .02).
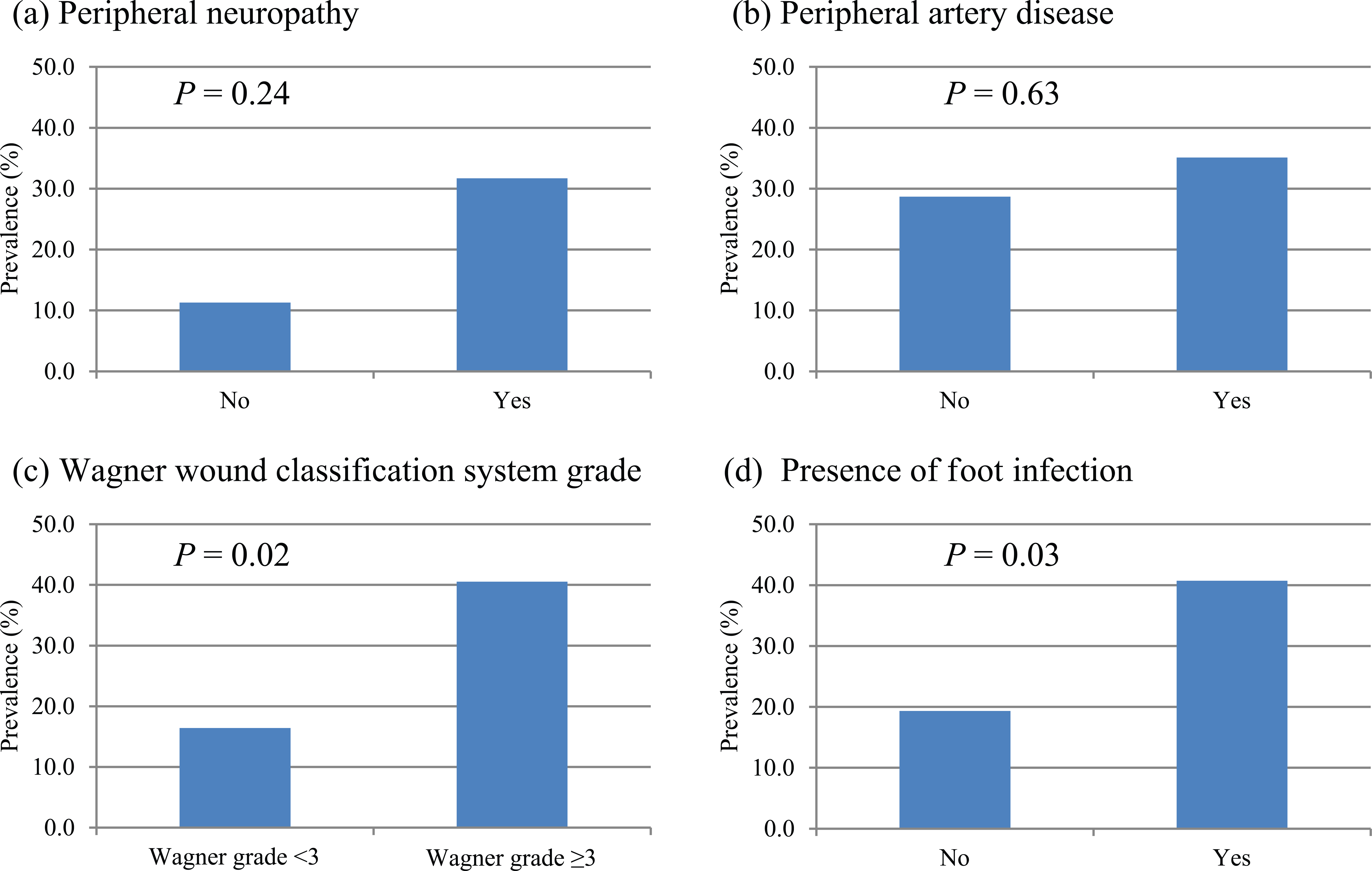
Adjusted prevalence of amputation according to presence of clinical manifestations; model adjusted for sex (male, female) and age (continuous).
Discussion
This cross-sectional study documented the most recent prevalence of LEA in a Saudi Arabian population with diabetic foot ulcer. Several clinical markers, including ulcer size, HDL, CRP, and homocysteine levels, were linked to LEA. We also observed a relatively higher prevalence of LEA among patients with local symptoms of diabetic foot, including PN and foot infection.
Considering that about half of our study population only had foot ulcers for less than 3 months, the observed prevalence of LEA of 29.7% was higher than the estimates in Western populations. For example, the incidence of LEA within 12 months was 8.0% in a UK cohort. 23 In another prospective cohort in both UK and US populations, the incidence of LEA among participants with diabetic foot ulcers over a 1-year follow-up was 15.0%. 8 Our finding was different from the report in 1996, in which the authors concluded that the Saudi population had a lower prevalence of LEA among diabetics than the Western population. 13 Our finding also suggested that this Saudi population may have greater susceptibility to LEA even at the same level of ulcer severity. For instance, the prevalence of Wagner grade ≥3 was 58.5% in our study population, which is comparable to that in a Chinese population (58%). 24 However, the prevalence of LEA in this Chinese population was 19.0%. These comparisons suggested a rising trend in diabetes epidemic and its comorbidities in this population in the past decades but potential insufficient resources of multidisciplinary diabetic foot care in SA.
We found a positive association between ulcer size and LEA, which was in line with previous findings from the EURODIALE consortium, a multicenter cohort study in a European population. 6 In another cohort study in the United Kingdom, ulcer size was identified as one of the dominant risk factors for predicting LEA resulting from diabetic foot ulcer. 25 Interestingly, the association between ulcer size and LEA was independent of foot infection and duration of foot ulcer in our data, whereas previous reports inclined to attribute the positive association between ulcer size and LEA to the greater severity of infection and longer duration of ulcer associated with a larger foot ulcer.25,26 Our finding supports the proposal to place greater emphasis on ulcer size in the foot ulcer classification system. 26
Consistent with existing evidence,6,27 PN was associated with a higher prevalence of LEA in our population. The potential mechanism for this association was 2-fold. First, PN leads to sensory loss, undermining patients’ perception of pain from repetitive stress and sense of pain and, therefore, delaying sufficient treatment of minor foot lesions. Second, PN could also directly affect wound healing. Sympathetic autonomic neuropathy causes reduced sweating, resulting in dry skin that is prone to crack or fissure, delayed wound healing, and amputation. 27 Denervation could also play a direct role in wound healing. 28 Although the prevalence of LEA was slightly higher among participants with PAD than those without PAD, the difference was not statistically significant, which was different from findings in Western populations.6,9 Possible explanations include that foot ulcers in non-Western populations are more likely to be neuropathic in origin rather than from pathological changes in peripheral arteries, which has been suggested by Boulton et al. 1 In addition, all the patients with PAD in our study also had PN. It is possible that the effect of PAD on LEA is distorted by the concomitant presence of PN. Also, we cannot exclude the possibility that the association could have been confounded by unmeasured factors, including medication use and lifestyle risk factors. Considering that only 14 participants had PAD, it is also possible that a lack of statistical power to detect this association is responsible for this result. Therefore, this finding warrants confirmation in large prospective cohort studies. We observed significant associations of foot infection and CRP, an inflammatory marker, with LEA. Current risk classification systems all included foot infection as an important metric for predicting foot ulcer prognosis.5,7,8 It is worth noting that, although a manageable symptom, foot infection still presented in almost half of our study population, suggesting a lack of screening and sufficient treatment of foot infection in this population. Our analysis confirmed previous findings8,24,29 that the severity of foot ulcer, measured by the Wagner wound classification system, was positively associated with likelihood of LEA, adding further evidence for the use of multiple physical symptoms in LEA prediction.
HDL was inversely associated with LEA in this current analysis. Previously, Ikura et al 30 also reported an inverse association between HDL and LEA resulting from diabetic foot ulcer, with a 1 mmol/L increment in HDL associated with a 67% lower risk of minor amputation and 88% lower risk of major amputation. The underlying mechanism for this finding is still not clear; potential explanations include HDL’s effects related to immunomodulation and acute infection suppression.31,32 This finding indicated the possibility of including HDL into a risk prediction system for diabetic foot outcome. However, prospective studies are still warranted to confirm our finding.We observed a positive association between homocysteine, an indicator of oxidative stress, and LEA, but this association became nonsignificant after further adjusting for duration of diabetic foot and foot infection. An increasing body of evidence from mechanistic studies has suggested the important role of oxidative stress in the pathogenesis of diabetic comorbidities. 33 In addition, our previous studies have linked higher homocysteine levels to higher prevalence of PAD and PN, also providing supporting evidence for the relationship between oxidative stress and LEA.34,35
Previous data on the outcome of diabetic foot ulcer in the Saudi population are sparse. Our data provided the latest evidence in this population. The strengths of this study include objective and detailed assessment of several local symptoms and comprehensive measures of clinical and biochemical markers. Several limitations of this study warrant attention. First, the cross-sectional nature of this study design limits the inference of causal relationship between risk factors and PAD. Therefore, our findings need to be confirmed in prospective studies. Second, because we used a study population from a clinical setting, findings from this study may not be extrapolatable to the broader populations with diabetic foot ulcer in the community setting. Finally, the statistical power was small because of a small sample size.
In conclusion, our study documented a very high prevalence and several correlates of LEA in this Saudi population with diabetic foot ulcer. The high prevalence of LEA, as well as foot infection and neuropathy, underscore the necessity of a multidisciplinary and cooperative system, including screening, early treatment, and wound healing, for diabetic foot care in SA. Our findings also highlight the potential to identify individuals at high risk of LEA based on a combination of clinical markers and local symptoms, although prospective studies in the Saudi population are warranted to confirm our findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mohammad Hussein Al-Amoudi Chair for Diabetic Foot Research, Saudi Arabia.