
Abstract
A 72-year-old male was referred to our hospital for a plantar ulceration that had occurred many years earlier. The lesion, with exuberant granulation and large areas of necrosis and fibrin, had long been treated by plastic surgeons with no positive evolution. At admission in our hospital no ischemia was detected, and foot radiograph was negative for bone involvement. The patient underwent a foot magnetic resonance imaging, which showed high vascularization in the plantar region and early capture of the contrast medium. We then performed multiple biopsies of the ulceration that revealed a moderately differentiated squamous cell carcinoma. The total body computed tomography exam raised a systemic involvement. A lymph node biopsy and immunohistochemistry assay on the pleural cytological sample proved the presence of a primary squamous cell carcinoma of the foot with systemic dissemination. Although rare, squamous cell carcinoma could be associated with chronic nonhealing ulcers; therefore, when a lesion does not heal, despite adequate standard treatment, its etiopathogenesis should be challenged.
A 72-year-old male was referred to our hospital for a large plantar ulceration not typically neuropathic with exuberant granulation, large areas of necrosis, and fibrin (Figure 1). The patient had a 4-year history of type 2 diabetes mellitus, which was managed with glibenclamide and metformin. The lesion occurred when he was 13 year old due to a burn during an epileptic crisis. The lesion was treated with local medications, antibiotic therapy, and 2 autologous skin grafts, but it never completely healed.
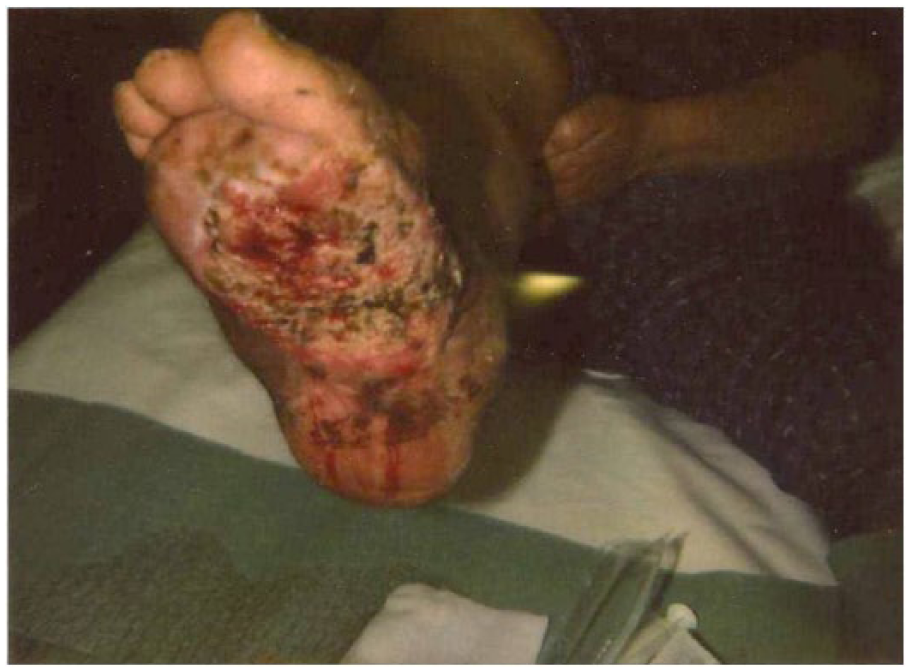
The lesion as presented at first visit.
The patient, treated by plastic surgeons for many years in another region of Italy, was referred to our center by his general practitioner for a second opinion. At admission in our hospital no ischemia was detected at general examination, which showed only cough and wheezes all over the chest. Blood tests were normal. A culture of the wound bed yielded colonies of Pseudomonas aeruginosa. Foot radiograph was negative for bone involvement. Chest radiograph showed an enlargement of the right hilus and an obliteration of the right costal-phrenic sinus.
Because of the long durance and clinical history of the ulceration, we decided to perform magnetic resonance imaging of the foot, which showed a plantar region with high vascularization and early capture of the contrast medium, suspected to be neoplastic and flogistic (Figure 2). Therefore, we drew multiple biopsies of the ulceration, and the histological assay revealed a moderately differentiated squamous cell carcinoma. A total body computed tomography exam raised a systemic involvement with a heteroplastic lesion in the right pulmonary hilus, right pleural effusion, and lymphadenopathy from the neck to the inguinal region (Figure 3). Tumor markers were normal excepted for a high Ca 125 (43.2 UI/mL).
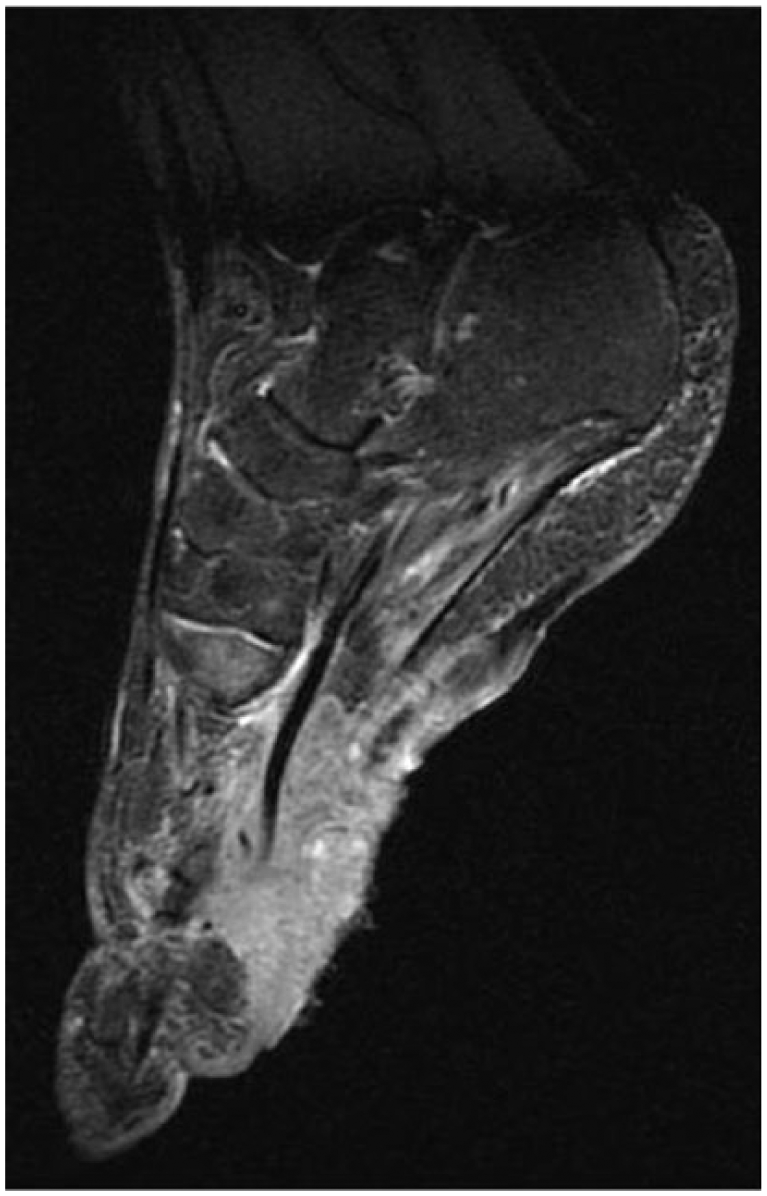
Magnetic resonance image of the foot.
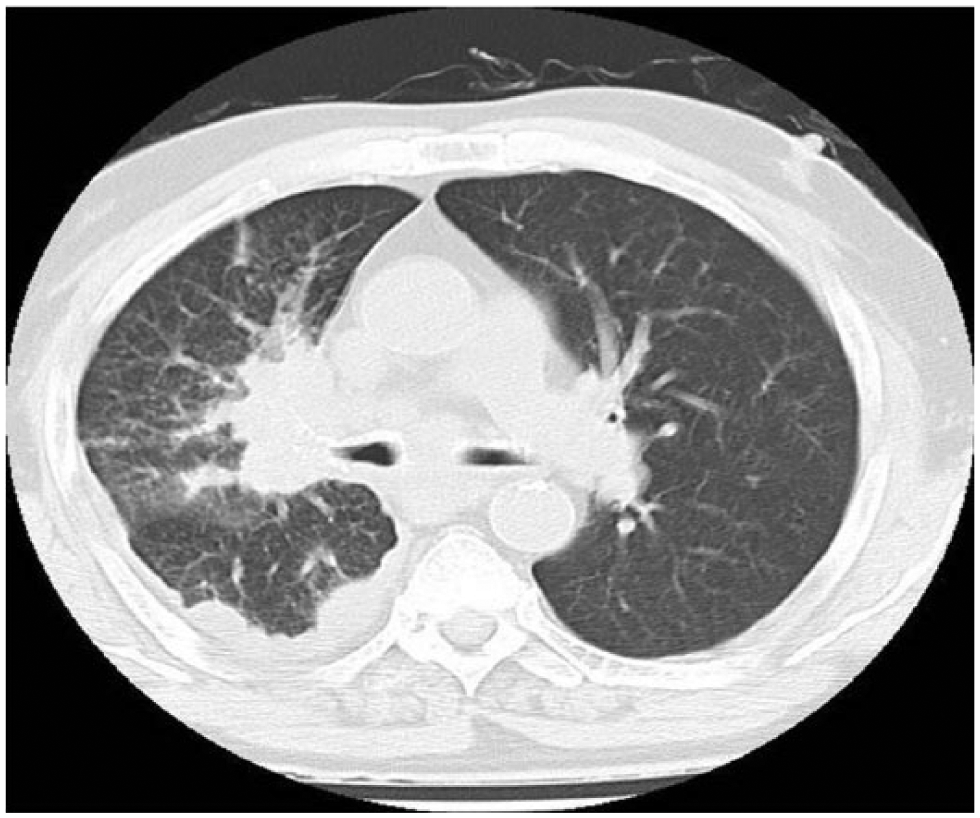
Image of chest computed tomography exam.
A lymph node and pleural biopsy proved the presence of squamous cell carcinoma (Figure 4A and B). Immunohistochemistry assay was done on the pleural cytological sample, testing the positivity of TTF-1 (thyroid transcription factor-1), which is normally expressed in most pulmonary tumors but not expressed in any other epithelial neoplasia. The test was negative, suggesting that this was a primary tumor of the foot with systemic dissemination. The patient received only supportive care. One month after the hospital discharge the patient died.
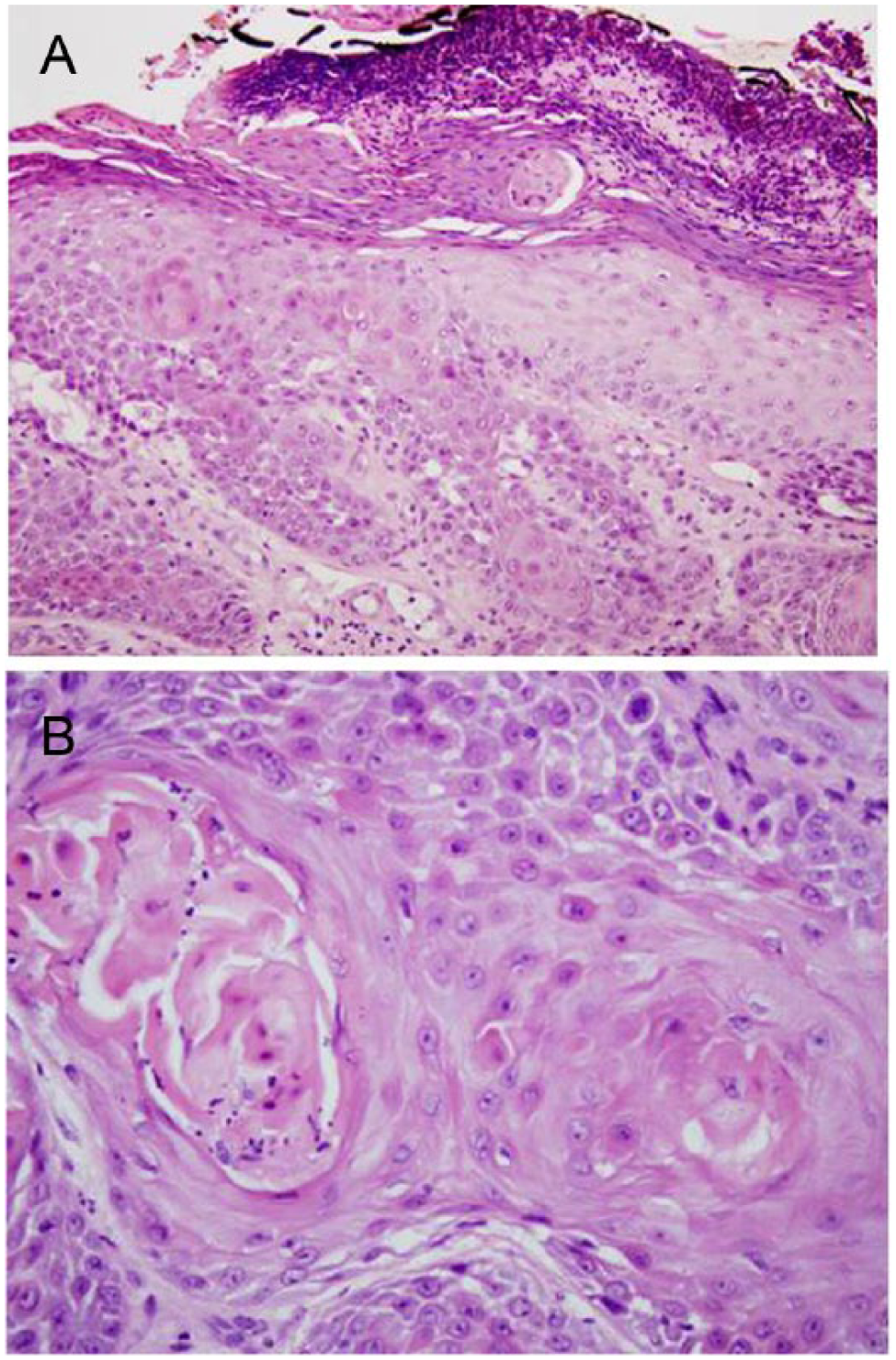
(A, B) Histological examination of the biopsy.
Although rare, squamous cell carcinoma could be associated with chronic nonhealing ulcers, 1 with long-lasting skin grafts, 2 and with burn scars. 3
Chronic ulcerations that evolve in neoplasm are defined as Marjolin ulcerations. A retrospective review from 1930 to 2004 on 412 lesions showed that 71% were squamous cell carcinoma, 12% basal cell carcinoma, 6% melanomas, 5% sarcomas, and 6% other neoplasms. 3 The latency period from the beginning of the ulceration till the development of the cancer was 30 years, and the median time for the diagnosis was 20 months. The local recurrence was about 16%; the lymph node dissemination was about 22% and the metastatic dissemination was about 14%. 3
When a chronic lesion does not heal with adequate standard treatment or it occurs in an atypical site, etiopathogenesis should be challenged and biopsies should be performed to determine the histology of the lesion.
An early diagnosis could avoid systemic dissemination, limb loss, and death of the patient.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.