
Abstract
Sarcoidosis is a multisystemic disease of unknown etiology. Up to 30% of patients develop cutaneous manifestations, either specific or nonspecific. Ulcerating sarcoidosis leading to leg ulcers is a rare observation that may lead to confusions with other, more common types of chronic leg ulcers. We report the case of a 45-year-old female patient with chronic multisystemic sarcoidosis presenting with pretibial leg ulcers. Other etiology could be excluded. Histology revealed nonspecific findings. Therefore, the diagnosis of nonspecific leg ulcers in sarcoidosis was confirmed. Treatment consisted of oral prednisolone and good ulcer care. Complete healing was achieved within 6 months. Sarcoidosis is a rare cause of leg ulcers and usually sarcoid granulomas can be found. Our patient illustrates that even in the absence of sarcoid granulomas, leg ulcers can be due to sarcoidosis.
Sarcoidosis is a multisystemic disease of unknown etiology characterized by epitheloid cell granulomas (sarcoidal type), with some intermingled giant multinucleated Langhans cells and surrounded by a small rim of lymphocytes. The formation of granulomas is a complex and dynamic process. 1
In Europe, incidence varies between 20 and 60 cases per 100 000 inhabitants and year. About 30% of patients develop cutaneous lesions, either specific or nonspecific. The most common lesions are papules, plaques, and nodules. Alopecia may develop, and the nail apparatus and mucous membranes may be affected. Ulcers are uncommon.1,2
Case Report
We report the case of a 45-year-old woman with erythematous lesions that persisted since 3 months. After minor trauma on the left leg, a chronic ulcer developed within the erythematous lesion. Some weeks later the lesion on the right leg became ulcerated as well. Her family history was negative for leg ulcers.
Her medical history was positive for thyroidectomy with postsurgical hypothyreosis in 2014 and first cervical lymph node enlargement in 2013. A cervical lymph node biopsy in February 2014 confirmed sarcoidosis.
On examination we found a slim and agile woman with good general health. No palpable lymph nodes were noted, probably because she had got an oral short-time prednisolone treatment (30 mg/day) before she came to the hospital. She presented with highly inflammatory pretibial ulcers of about 3 cm (right leg) and 3.5 cm (left leg) in diameter (Figure 1). She had no clinical signs of chronic venous insufficiency or peripheral arterial disease.

Pretibial leg ulcer with elevated borders.
Skin biopsies were taken from both ulcers but remained nonspecific. No sarcoid granulomas could be identified. A lymph node biopsy from the right groin disclosed nodal sarcoidosis with typical “naked granulomas” (Figure 2). A bone marrow biopsy ruled out any sarcoidosis there; the bone marrow was normocellular.
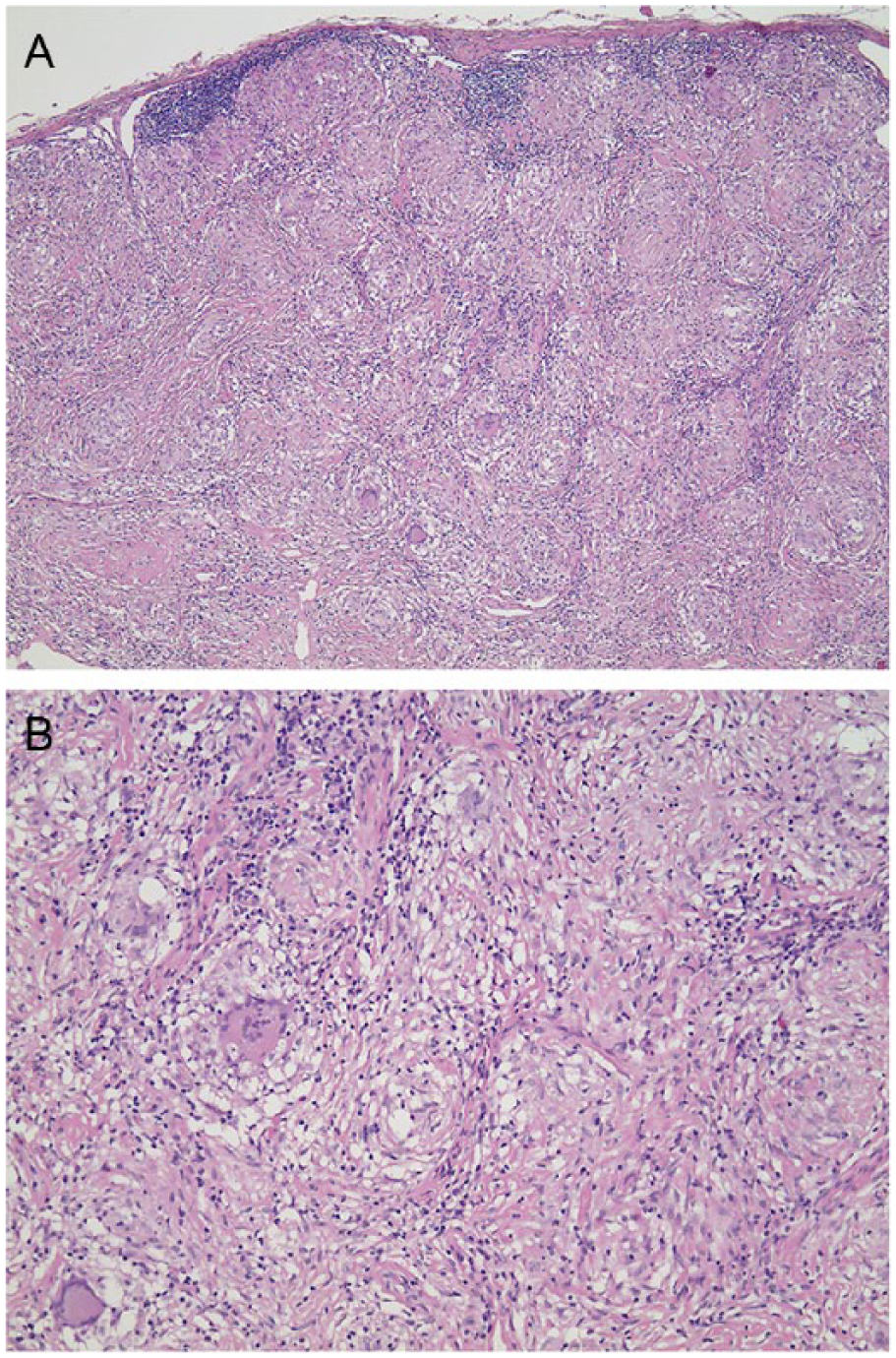
Histology of an affected lymph node. (A) Overview with multiple nonnecrotizing “naked” granulomas and intermingled giant multinuclear Langhans cells (hematoxylin-eosin, 4×). (B) Detail (hematoxylin-eosin, 10×).
Laboratory investigation demonstrated the following pathologic findings: leukocytes ↓ 3.09 Gpt/L (normal range = 3.8-11.0 Gpt/L), lymphocytes ↓ 0.6 Gpt/L (1.2-3.5 Gpt/L), C-reactive protein ↑ 12.7 mg/L (<5 mg/L), angiotensin-converting enzyme ↑ 141.9 U/L (8-62 U/L), β-2-microglobulin ↑ 4.26 mg/L (0.8-2.4 mg/L), and soluble interleukin-2-receptor ↑ 1901 U/mL (300-900 U/mL).
Microbiology (Swabs From Leg Ulcers)
There was no bacterial growth on the right leg but abundant Staphylococcus epidermidis on the left leg.
Imaging
Thoracic X-ray demonstrated bilateral hilar lymphadenopathy. Diagnostic ultrasound of the neck disclosed multiple enlarged lymph nodes on both sides. Diagnostic ultrasound for the ankles was unremarkable. Computed tomography of the trunk demonstrated generalized lymphadenopathy, diffuse infiltration of the spleen, and pulmonary involvement.
Electrocardiography and cardiac echography remained normal. Ventilation or diffusion disturbances could be excluded by body plethysmography.
Ophthalmological investigation revealed no specific involvement.
The diagnosis of systemic sarcoidosis with nonspecific cutaneous manifestation—pretibial leg ulcers—was confirmed.
Treatment and Course
We treated the patient with 50 mg prednisolone orally per day and 40 mg pantoprazole per day. Topical ulcer treatment was started with fluocinolone-neomycin ointment to reduce the inflammation followed by hydrogel to force the autodebridement and petrolatum gauze. Resistant necrotic areas were removed surgically and after that the wounds were covered by polyacrylate wound dressings.
The corticosteroids could be tapered down. The ulcers healed within 6 months leaving flat scars.
The patient is further monitored by her pulmonologist.
Discussion
We report a female patient with chronic systemic sarcoidosis and pretibial leg ulcers with a high granuloma burden. This is also illustrated by elevated levels of angiotensin-converting enzyme and soluble interleukin-2-receptor. 3 Although she had a spleen involvement, fortunately no thrombocytopenia occurred. Furthermore, pulmonary involvement did not result in functional impairment. Skin manifestation is seen in up to 30% of patients with systemic sarcoidosis. However, ulcerating sarcoidosis is uncommon. Only 1% of Caucasians affected by sarcoidosis develop skin ulcers. 4
Our patient developed secondary cutaneous signs, that is, pretibial ulcers. Leg ulcers are a rare cutaneous manifestation of sarcoidosis and can be either due to secondary ulceration of specific cutaneous infiltrates with sarcoid granulomas,5-12 granulomatous vasculitis, 13 or are nonspecific (Table 1). The largest series has been published by Albertini et al, 4 with a review of 29 cases presenting with leg ulcers, all with proven sarcoid granulomas.
Leg Ulcers in Sarcoidosis (Without Granulomatous Vasculitis).
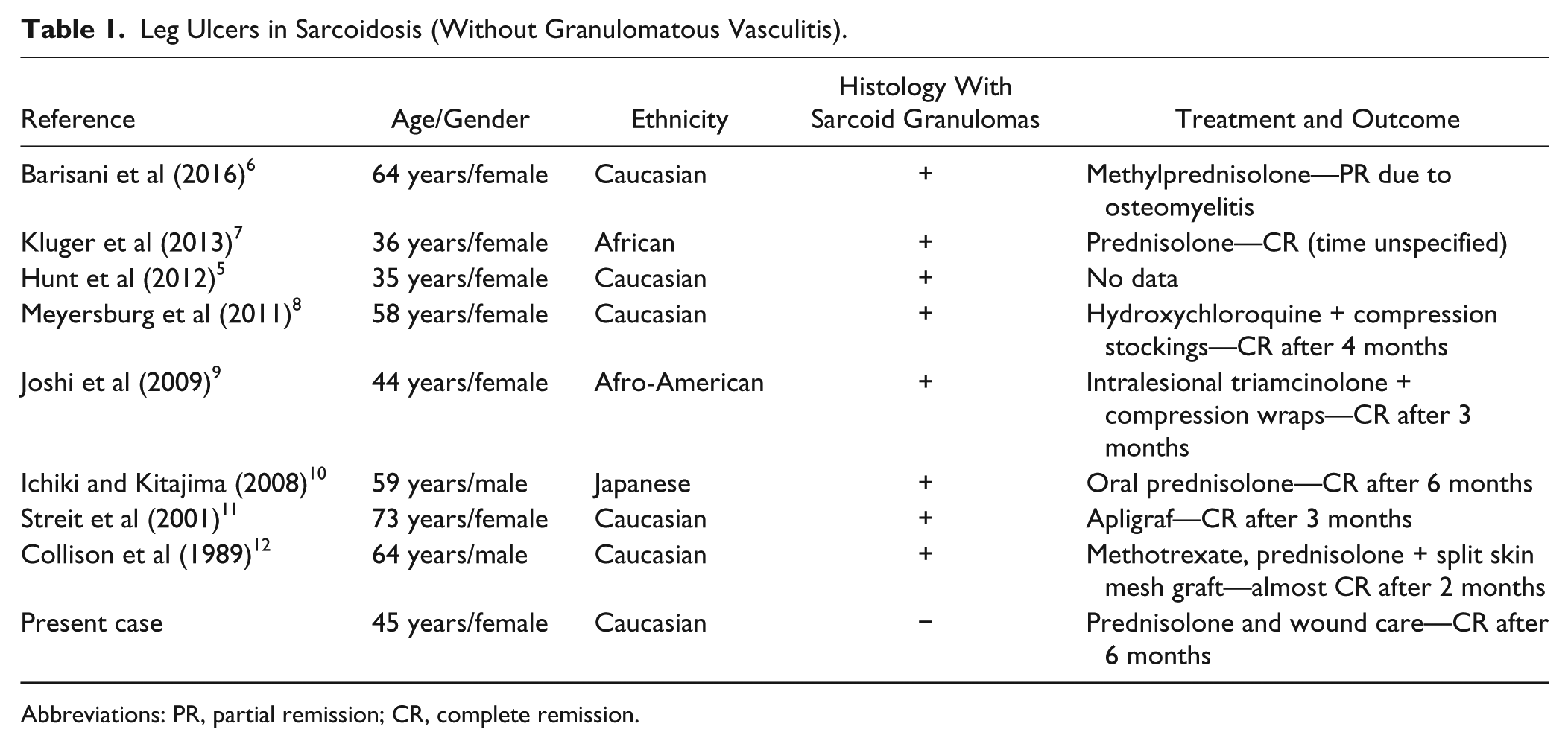
Abbreviations: PR, partial remission; CR, complete remission.
Since skin biopsy disclosed only nonspecific skin ulcers, we classify the pretibial ulcers as nonspecific cutaneous manifestation of sarcoidosis. 1 Other causes of leg ulcers had been excluded. Ulcerative sarcoidosis is mainly found in young adults with a clear predominance of women. Afro-American and Japanese patients are more frequently affected than Caucasians.2,10 This might be due to a different genetic background.
The diagnosis is often delayed. Treatment of choice is corticosteroids and methotrexate as second-line treatment.4,6 Surgical intervention has only occasionally been reported.11,12
In conclusion, our patient suffered from chronic systemic sarcoidosis with pulmonary, nodal, and spleen involvement. This patient is exceptional because of leg ulcers without granulomas in case of sarcoidosis. Other relevant pathologies of leg ulcers had been excluded.
Footnotes
Acknowledgements
We highly appreciate the support by Dr J. Schönlebe, Department of Pathology.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.