
Abstract
The aim of this study was to evaluate the impact of end-stage renal disease (ESRD) on health-related quality of life (QOL) in patients with diabetic foot disease. We compared a group of 30 diabetic patients with ESRD requiring dialysis to a group of 60 diabetic patients without ESRD. Both groups consisted of patients with active diabetic foot disease (ulcer, Charcot, infection) and were matched with regard to age and gender. Self-reported QOL was assessed using the Short Form-36 (SF-36) physical and mental component summary (PCS and MCS) scores and the region-specific Foot and Ankle Ability Measure (FAAM). Diabetic foot patients with ESRD requiring dialysis were found to have significantly higher creatinine levels, lower hemoglobin levels, lower albumin levels, higher rates of peripheral arterial disease, and lower rates of Charcot neuroarthropathy than patients without ESRD. The median PCS was significantly lower in the ESRD group; however, no significant difference was found when comparing the median MCS and FAAM. Patients who ultimately died had a tendency to report lower PCS scores at baseline compared with those patients who did not die (P = .07). Patients who ultimately required major amputation also reported lower PCS scores at baseline. ESRD negatively affects physical QOL to a greater degree than mental QOL in patients with diabetic foot disease. The SF-36 may not be sensitive enough to capture impaired mental QOL because both groups had relatively high MCS scores. Low physical QOL may be associated with mortality and the eventual need for major amputation.
Diabetic foot complications occur secondary to microvascular disease (neuropathy) and macrovascular disease (peripheral artery disease), leading to diabetic foot ulceration (DFU), neuropathic fractures, Charcot neuroarthropathy (CN), infections, and amputations. It has been well established that patients with diabetic foot–related complications experience reduced self-reported health-related quality of life (HRQOL).1-10 Somewhat surprisingly, physical HRQOL is negatively affected to a much greater degree than mental HRQOL.2,3,6,7 Because of microvascular disease, patients with diabetic foot disease often have concurrent nephropathy and retinopathy. Diabetic nephropathy has become one of the most frequent causes of end-stage renal disease (ESRD), and providers who treat diabetic foot disease are encountering patients with ESRD with increasing frequency. 11 Patients with diabetic foot disease fear major amputation more than death, and nearly 10% of patients rank ESRD as their greatest fear. 12
Studies that examine HRQOL in patients with ESRD largely demonstrate significantly reduced physical QOL in comparison to mental QOL.13-17 Although these studies included patients with diabetes, HRQOL was not discriminated based on diabetes status. Studies that have directly compared HRQOL in dialysis patients have reported lower physical QOL in diabetic patients compared with nondiabetic patients.18-20 Based on these studies, mental QOL does not appear to be significantly affected in patients with ESRD. To the best of our knowledge, only 1 study has evaluated HRQOL in patients with ESRD and diabetic foot ulcers. 11
The primary aim of this study was to assess the impact of ESRD on HRQOL in a cohort of patients with diabetic foot–related complications. We sought to compare this study group with a control group of patients with diabetic foot disease who did not have ESRD. Our hypothesis was that patients with ESRD and diabetic foot disease would have lower HRQOL than patients with diabetic foot disease alone. A secondary aim was to determine if there was association between low HRQOL and adverse outcomes such as mortality and major lower-extremity amputation (LEA).
Methods
After institutional review board approval (IRB No. PRO12020607), we retrospectively identified patients with ESRD and diabetic foot disease. For the purposes of this study, ESRD was defined as requiring hemodialysis or peritoneal dialysis. Diabetic foot disease included patients with DFU, diabetic foot infections, CN, or neuropathic fractures. Major LEA was defined as an amputation at the level of the ankle or more proximal (ie, transtibial or transfemoral).
Self-reported HRQOL was evaluated using the Medical Outcome Study Short Form-36 (SF-36) and the Foot and Ankle Ability Measure (FAAM). The SF-36 is a generic measure of QOL and has been used to report on a diverse group of medical conditions, including diabetes mellitus (DM). The SF-36 comprises 8 subscales (physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health), and the score for each subscale ranges from 0 to 100. An overall physical component summary (PCS) score is calculated from the 4 subscales of physical functioning, role physical, bodily pain, and general health, whereas the overall mental component summary (MCS) score is calculated from the subscales of vitality, social functioning, role emotional, and mental health. The median PCS and MCS scores for the general population have been established at 50, and higher scores represent better self-reported QOL than lower scores. SF-36 scores have been reported for a variety of diabetic foot disorders such as diabetic foot ulcers, CN, and diabetic foot infections.1-10 The FAAM is a region-specific tool and assesses lower-extremity function by surveying activities of daily living and sports-related activities and recently was found to be valid and responsive in assessing diabetic foot disease.7-9 A total of 21 activities comprise the activities of daily living subscale, and 8 activities comprise the sports subscale. Scores range from 0% to 100%. Higher FAAM scores indicate a higher level of lower-extremity function than lower scores.
After retrospective review of inpatient and outpatient records, we identified 30 patients with ESRD and diabetic foot–related complications who had completed a baseline SF-36 and FAAM during the time period of April 1, 2009, through January 31, 2016. All patients were treated by the senior author in an academic foot and ankle center. Our study group comprised patients with ESRD and diabetic foot–related complications, and our control group comprised patients with diabetic foot–related complications who did not have ESRD.
We used a 2:1 control-to-study match to select 60 control patients with diabetic foot–related complications but no ESRD. The 2:1 match was utilized as a means of increasing the power of this study while minimizing the loss with the small number of case control sets available from our database. The control group was matched for age and gender. Although the selection of patients for matching was performed in a blinded manner without knowledge of the outcome scores, this was not done in a random manner.
Peripheral neuropathy was clinically diagnosed using the Michigan Neuropathy Screening Index (score ≥ 2.5), and peripheral artery disease (PAD) was diagnosed as an ankle brachial index <0.91 or toe brachial index <0.7.21-23
Statistical Methods
Patient demographic factors were reported using descriptive statistics. Median values along with 25th to 75th interquartile ranges (IQRs) were used to describe continuous factors, such as age and body mass index (BMI), and frequency (%) was used to describe categorical variables such as gender and type of diabetes. Laboratory values and survey scores (SF-36 and FAAM) were also reported this way (Table 1). After testing for normality using the Shapiro-Wilk test, patient demographic factors and patient-reported outcome measures were compared between those who had ESRD and those who did not have ESRD using the Mann-Whitney U test, Student t test, or χ2 test of homogeneity. Finally, patient outcomes of mortality, amputation, and surgery were correlated with SF-36 scores. All statistical analyses were performed with a significance level of .05.
Patient Demographics and Comorbidities by Presence of ESRD.
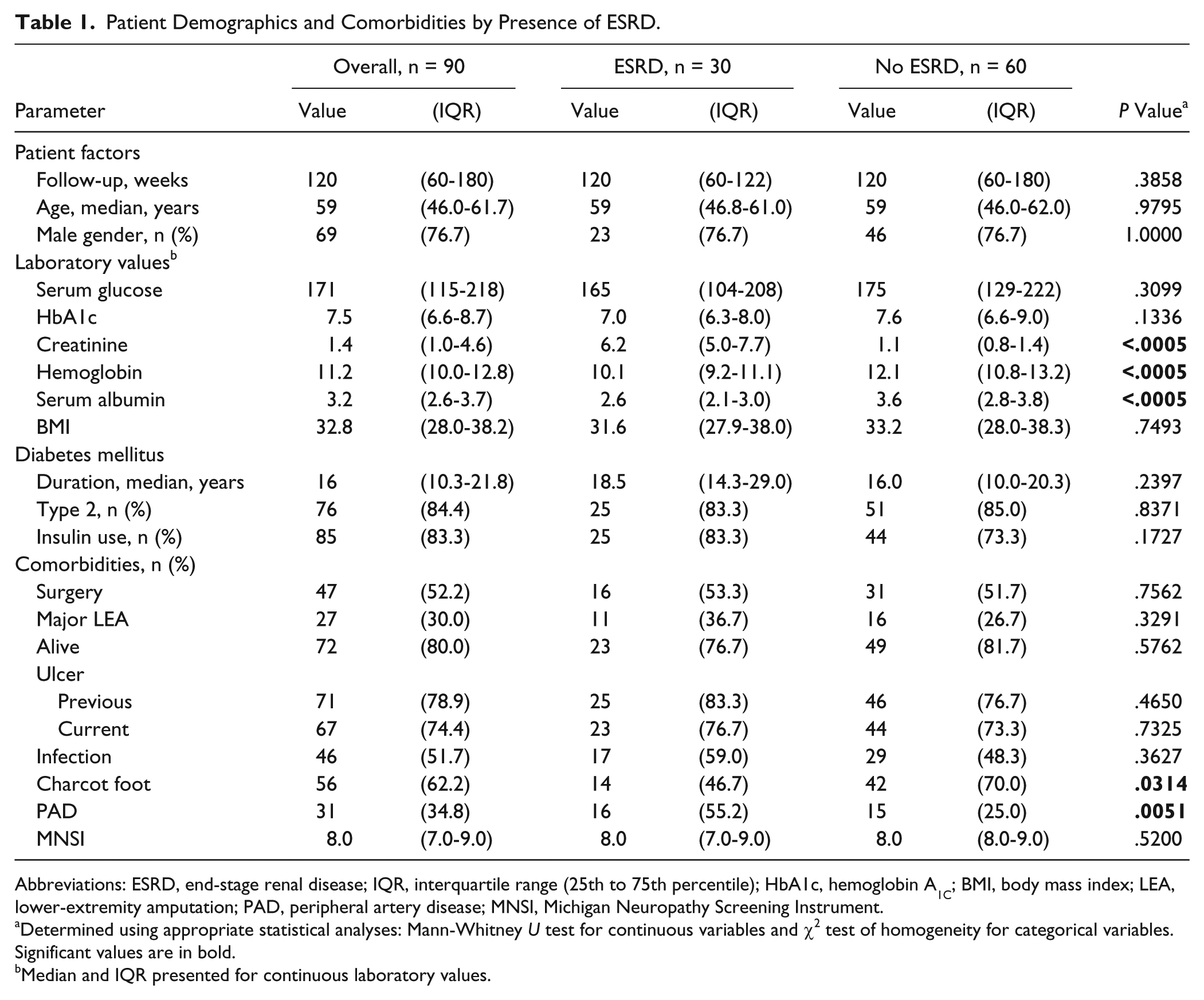
Abbreviations: ESRD, end-stage renal disease; IQR, interquartile range (25th to 75th percentile); HbA1c, hemoglobin A1C; BMI, body mass index; LEA, lower-extremity amputation; PAD, peripheral artery disease; MNSI, Michigan Neuropathy Screening Instrument.
Determined using appropriate statistical analyses: Mann-Whitney U test for continuous variables and χ2 test of homogeneity for categorical variables. Significant values are in bold.
Median and IQR presented for continuous laboratory values.
Results
ESRD and Patient Factors
A total of 90 patients were included in this study, and all the patients had diabetic foot complications. The study group consisted of 30 patients with ESRD, and the control group consisted of 60 patients who did not have ESRD. There was no significant difference between the 2 groups regarding age, gender, serum glucose, glycated hemoglobin, BMI, duration of DM, type of DM (type 1 vs 2), insulin use, prevalence of DFU, or prevalence of diabetic foot infection (Table 1). Patients in the study group (ie, ESRD) had higher serum creatinine (P < .0005), lower hemoglobin (P < .0005), lower serum albumin levels (P < .0005), higher prevalence of PAD (P = .005), and lower prevalence of CN (P = .03); see Table 1.
ESRD and Patient-Reported Outcome Measures: SF-36 and FAAM
Patients in the study group had significantly lower median SF-36 PCS scores, SF-36 physical function subscale scores, and SF-36 social function subscale scores than the control group (Table 2). However, there were no significant differences between the 2 groups with regard to median SF-36 MCS scores, the remaining 6 subscale scores of the SF-36, or the median FAAM scores (Table 2).
Patient-Reported Outcomes by Presence of ESRD.
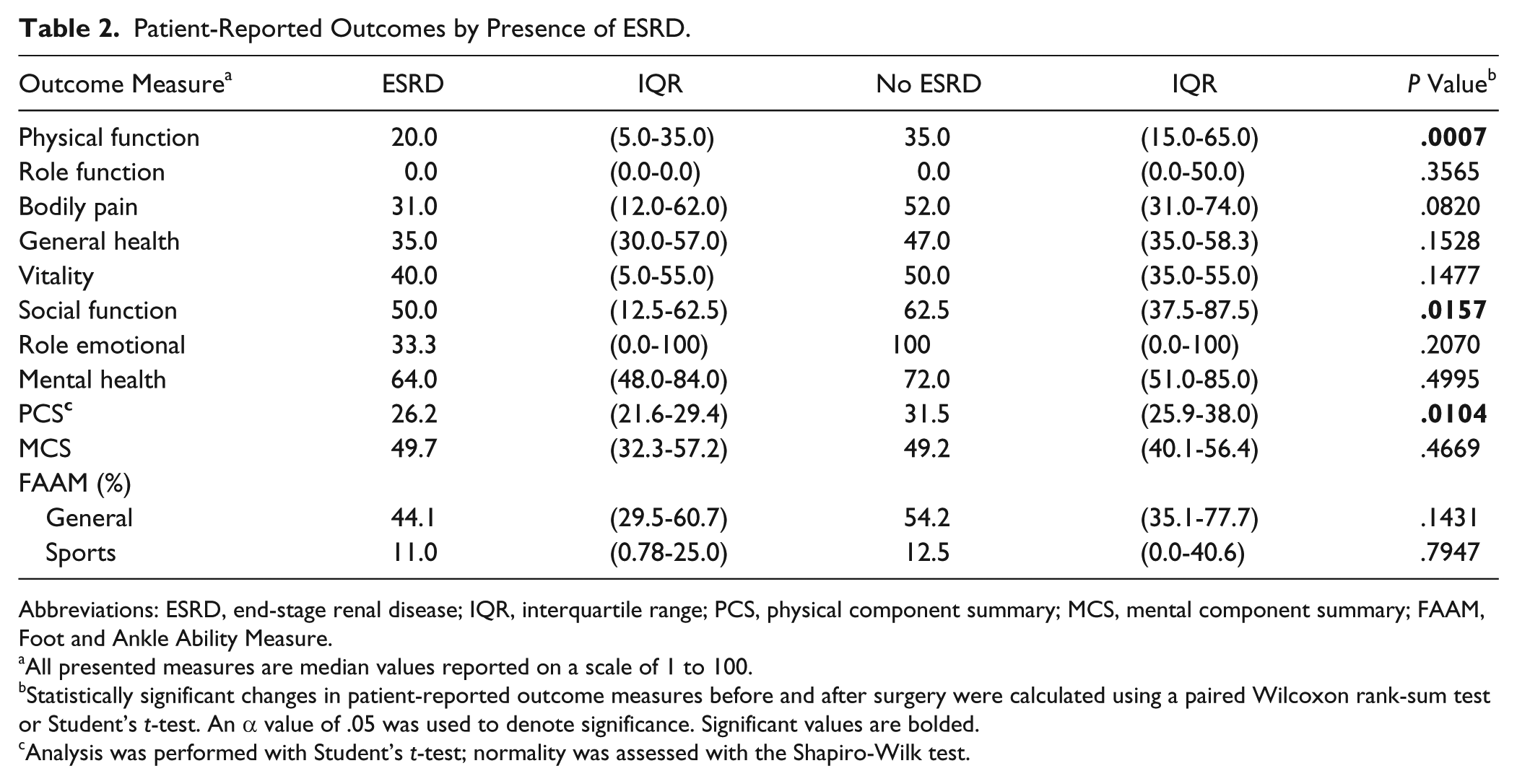
Abbreviations: ESRD, end-stage renal disease; IQR, interquartile range; PCS, physical component summary; MCS, mental component summary; FAAM, Foot and Ankle Ability Measure.
All presented measures are median values reported on a scale of 1 to 100.
Statistically significant changes in patient-reported outcome measures before and after surgery were calculated using a paired Wilcoxon rank-sum test or Student’s t-test. An α value of .05 was used to denote significance. Significant values are bolded.
Analysis was performed with Student’s t-test; normality was assessed with the Shapiro-Wilk test.
Patient-Reported Outcome Measures and Clinical Outcomes
The median length of follow-up in our cohort of 90 patients was 120 weeks (25th -75th IQR = 60-180), and there was no significant difference in the length of follow-up between the 2 groups (Table 1). During the course of our study, 27 of the 90 patients (30%) underwent major LEA (all transtibial), and 18 of 90 patients (20%) died. Although there were no significant differences between the 2 groups with regard to mortality, ultimate need for major LEA, or the need for surgical intervention, several interesting observations were noteworthy (Table 3). Patients who ultimately died tended to report a lower SF-36 PCS score (P = .07) and lower SF-36 vitality score (P = .07) than patients who were alive at final follow-up (Table 3). However, no significant effects were seen in any of the SF-36 scores when dichotomized by mortality. In contrast, patients who required subsequent major LEA reported significantly lower median SF-36 PCS scores (P = .013) and SF-36 physical function subscale scores (P = .0014). In addition, SF subscale scores for role physical, social function, and role emotional scores tended to be lower in patients who required major LEA. Among patients who required further surgery (reconstructive surgery or treatment of infection), the median SF-36 physical function subscale scores were significantly lower. Interestingly, although SF-36 scores related to physical function were lower among patients who experienced adverse clinical outcomes, SF-36 MCS scores were not significantly affected by mortality, amputation, or surgery (Table 3).
PROM Score Associations With Mortality, Amputations, and Surgical Intervention.

Abbreviations: PROM, Patient-Reported Outcome Measure; IQR, interquartile range; PCS, physical component summary; MCS, mental component summary.
All presented measures are median values reported on a scale of 1 to 100.
Changes in PROM scores before and after surgery were analyzed using the paired Wilcoxon rank sum test. PCS scores were compared between groups using Student’s t-test. Normality was assessed using the Shapiro-Wilk test. An α value of .05 was used to denote significance. Significant values are bolded.
Death at final follow-up denoted with “+.”
All amputations were performed after patient surveys were completed.
All surgeries were performed after patient surveys were completed.
Patient-Reported Physical and Mental Scores: Predictive Factors
Patient demographics, laboratory values, and comorbidities were evaluated for strength in predicting PCS and MCS scores using multivariate linear regression. Patient ESRD status was the only factor that was significantly correlated with PCS scores (P = .025), but it was not correlated with MCS scores (P > .05). However, the presence of current and previous foot ulcers were found to be significantly co-linear (p<0.0001) because 100% of patients who had a current ulcer had a previous ulcer (67 patients), and 82.6% of patients who did not have a current ulcer also did not have previous ulcers (19 patients out of 23). Using multivariate ANOVA, previous (p=0.034) and current ulcers (p=0.027) were predictive of MCS scores. Furthermore, history of previous ulcers (p=0.007) and presence of current ulcers (p=0.014) were also significantly associated with PCS scores. The median PCS and MCS scores for patients without current ulcers or a history of previous ulcers were 35.0 and 55.3, while the median PCS and MCS scores for patients with either current ulcers or previous ulcers were 28.2 and 47.8 respectively.
Discussion
Many previous studies of diabetic patients have demonstrated that foot complications such as CN and DFU have a profoundly negative impact on physical QOL; however, mental QOL is not affected to the same degree (Table 4).1-4,6-9,24 This study demonstrates that ESRD further negatively affects physical QOL in patients with diabetic foot–related complications. Somewhat unexpectedly, mental QOL was not significantly affected by ESRD. Although we found this surprising, several other studies of patients with ESRD have reported similar findings.13-17 We do not have a clear explanation as to why dialysis does not result in reduced mental QOL in view of the fact that ESRD is associated with premature mortality and other complications. It is possible that the SF-36 does not adequately capture emotional distress and reduced mental QOL in patients with ESRD. A similar observation has been noted in patients with DFU and CN. 24 A potential explanation for this is the absence of pain in patients with diabetic foot disorders.9,25 The neuropathy and foot ulcer–specific QOL instrument (NeuroQOL) may be more reliable than the SF-36 in capturing psychosocial function in patients with diabetic foot disorders. 26
Quality of Life in Patients With Diabetes. a
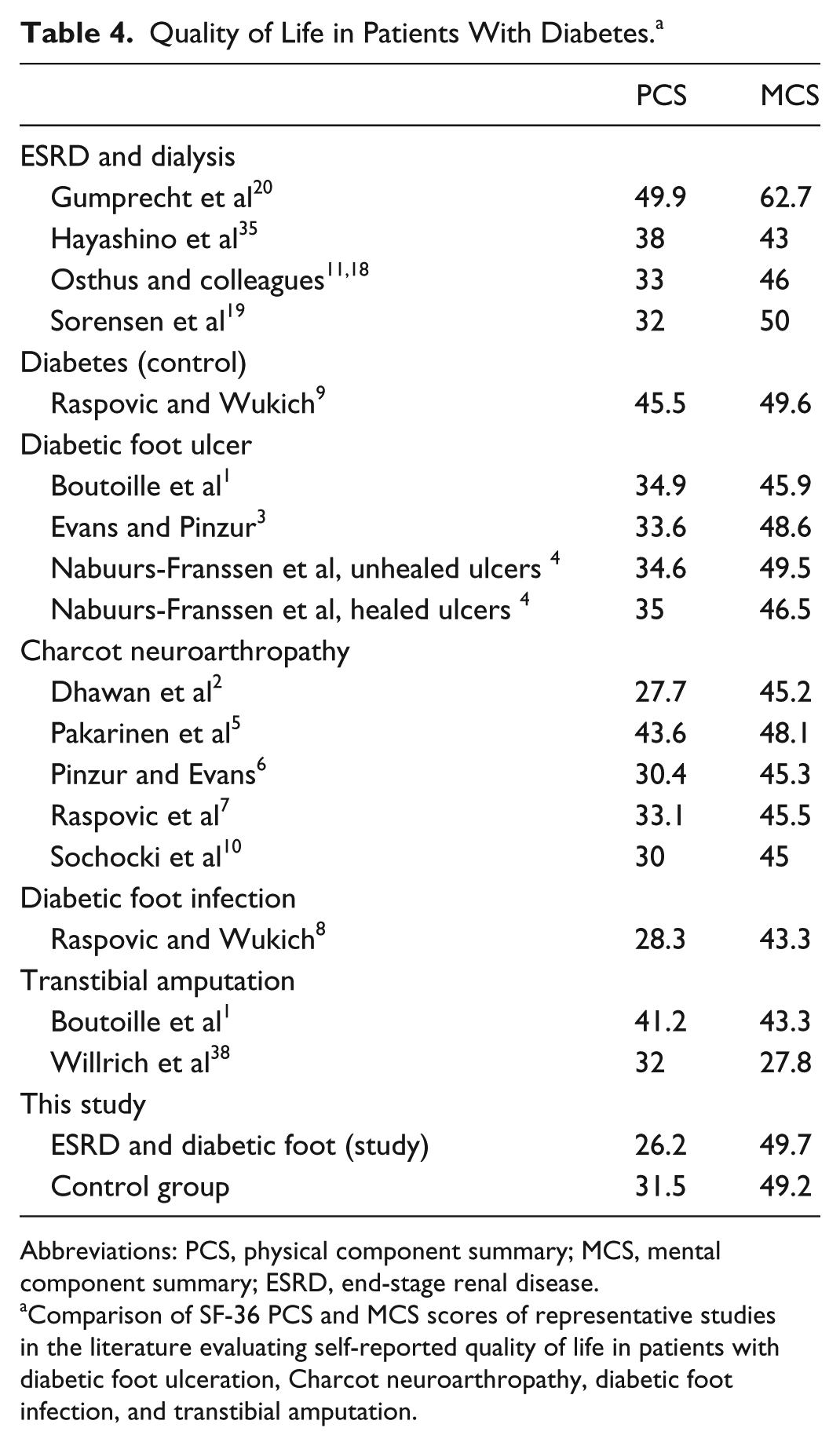
Abbreviations: PCS, physical component summary; MCS, mental component summary; ESRD, end-stage renal disease.
Comparison of SF-36 PCS and MCS scores of representative studies in the literature evaluating self-reported quality of life in patients with diabetic foot ulceration, Charcot neuroarthropathy, diabetic foot infection, and transtibial amputation.
Diabetic patients with ESRD are at high risk for DFU and LEA.27-30 Examining Medicare data, Eggers et al 27 reported that diabetic patients on dialysis had a 10 times higher rate of amputation than diabetic patients at large. Dialysis treatment in patients with diabetes is also an independent risk factor for developing a foot ulcer. 29 Patients with diabetes and ESRD also have disproportionally high rates of foot-related hospitalizations and higher rates of mortality after major LEA.31-33 Osthus et al 11 reported that SF-36 subscale scores for vitality and general health were significantly lower in patients with ESRD and DFU compared with patients with DFU but not ESRD. Although that study only looked at 7 of 8 subscale domains and did not report on PCS or MCS scores, our results are consistent with their findings.
Another important aim of our study was to evaluate if a significant association was present between low self-reported HRQOL and adverse outcomes (major LEA and mortality). Because our ESRD cohort was relatively small (n = 30), we chose to include all 90 patients who comprised our study and control groups. We found that patients with diabetic foot disease who ultimately died tended to have lower SF-36 PCS scores and lower vitality subscale scores than patients who were alive at final follow-up. Patients who ultimately required major LEA had significantly lower SF-36 PCS scores than patients who did not require major LEA. Although the lower SF-36 subscale scores of vitality, social function, and role emotion did not reach statistical significance in association with future major LEA, we feel that this finding is clinically meaningful. Many authors have reported higher rates of mortality in patients with diabetic foot disease. This study demonstrates that in patients with diabetic foot disease, low HRQOL is potentially associated with adverse outcomes such as mortality and major LEA. We are certainly not the first to associate low HRQOL scores with adverse outcomes in patients with diabetes. Low self-reported HRQOL has been associated with mortality in patients with diabetes. Using a Cox proportional hazard model, Kleefstra et al 34 found that the SF-36 PCS score was inversely related to mortality in patients with type 2 diabetes, whereas the SF-36 MCS score was not. Similar to diabetes patients in general, low self-reported HRQOL in dialysis patients is associated with mortality. 11 Osthus et al 11 reported that SF-36 MCS scores were independent predictors of mortality in diabetic patients with ESRD in a multivariate model that adjusted for age, heart disease, and PCS score. In contrast, Hayashino et al 35 found that low SF-36 PCS scores were independent predictors of mortality in diabetic patients with ESRD. The increased mortality in diabetic patients with ESRD is largely a result of cardiovascular disease and sepsis.11,18,36 The Eurodiale Study, involving 14 centers in 10 European countries, assessed HRQOL in patients with DFU. They utilized the EQ-5D rather than the SF-36 to measure QOL. This instrument is also a validated and standard method of assessing self-reported HRQOL in Europe. The authors reported that low HRQOL in patients with DFU, especially in the physical domains, was predictive of major amputation and death. 37 Independent of ESRD, major amputation in patients with diabetes has been associated with low HRQOL. 38
All retrospective studies are subject to potential bias. The data obtained from retrospective review relies on the accuracy and completeness of the medical record, and the quality of data for analysis is only as good as the documentation in the medical record. The selection of a control group can introduce bias, and we attempted to minimize bias by matching the 2 groups based on age and gender. We recognize that our control group was not selected randomly, and this could potentially introduce bias. Our 2 groups were similar in most categories, with a few exceptions. As expected, patients with ESRD had higher serum creatinine, lower hemoglobin, and lower serum albumin levels than the control group. The ESRD group had a significantly lower prevalence of CN but a higher prevalence of PAD than the control group. Medial arterial calcinosis is common in patients with DM, neuropathy, and ESRD, leading to decreased elasticity, increased arterial wall stiffness, and decreased perfusion.39-42 The pathogenesis of CN relies on the ability of the patient to mount an acute inflammatory response, and this hyperemic response requires adequate arterial perfusion. 43 This may explain why our results show that the ESRD group had a significantly lower prevalence of CN but a higher prevalence of PAD than the control group. Consequently, the reader should interpret the findings of this study recognizing these differences between the 2 groups. Nonetheless, both groups appear to be representative of a high-risk academic diabetic foot and ankle practice based on the high prevalence of CN, neuropathy, PAD, and DFU. We attempted to minimize selection bias by including all patients with ESRD who completed the SF-36 and FAAM; however, the small size of our ESRD cohort (n = 30) is a weakness that makes this study potentially underpowered to definitively state that there are no real differences between our 2 groups. As a result of our small sample size, a type II error is possible, which would lead us to wrongly conclude that no significant differences exist between our 2 groups with regard to MCS scores, FAAM scores, or various SF-36 subscales. Normally, sample size calculations are a priori based on 80% power and an α of .05. Calculations of adequate sample size are based on previous studies, and to the best of our knowledge, only 1 study reported on DFU in patients with ESRD. However, that study did not report PCS or MCS scores, so consequently, we could not do a power analysis a priori. 11 Another potential limitation of our study is that we utilized several different diagnoses to define diabetic foot disease.
In conclusion, our findings show that ESRD negatively affects physical QOL to a greater degree than mental QOL in patients with established diabetic foot disease. The SF-36 may not be sensitive enough to capture impaired mental QOL because both groups had relatively high MCS scores. This study also demonstrates that in patients with diabetic foot disease, low HRQOL is potentially associated with adverse outcomes such as mortality and major LEA. Although patients with ESRD and diabetic foot disease have lower baseline QOL scores than patients without ESRD, this study does not suggest that patients with ESRD would not benefit from the same treatment options offered to patients without ESRD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.