
Abstract
Loss of soft tissue coverage distally around the foot poses threats of amputation of the exposed boney structures. An amputation of a portion of the foot leads to loss of the biomechanical structural integrity of the foot. This promulgates an imbalance with its inherent risks of developing new ulcers. This in turn potentiates the limb loss cycle. The reverse abductor hallucis muscle flap is ideally suited for small to moderate-sized defects in the vicinity of the first metatarsophalangeal joint based on its arc of rotation. In this article, we present cases of 5 patients who failed local wound care and healing by secondary intention for at least 6 months duration. The patients were treated successfully using reverse abductor hallucis muscle flap.
Loss of soft tissue coverage distally around the foot poses threats of amputation of the exposed boney structures. An amputation of a portion of the foot leads to loss of the biomechanical structural integrity of the foot. This promulgates an imbalance with its inherent risks of developing new ulcers. This in turn potentiates the limb loss cycle.
Exposure of critical structures such as joints, bone, ligaments, and tendons necessitates expeditious closure. The longer these structures remain open to the environment, the higher the risk is for that patient developing osteomyelitis and an amputation. Soft tissue reconstruction of the lower extremity often requires coverage by local or distant flaps. Utilizing vascularized flaps to attain rapid wound closure diminishes the risk in our patients with already compromised health. This not only allows for immediate closure but also has the ability to perfuse the area with parenteral antibiotics.
Muscle flaps remain often first choice when dealing with bone infections associated with osteomyelitis, soft tissue infections, and large cavities. 1 Because common local distally based muscle transpositional flaps have difficulty reaching the forefoot plantar region, these defects are normally treated by free tissue transfer. 2 However, free flap procedures are relatively complex, time consuming, requires microsurgical expertise, and has donor-site morbidity, which may not be suitable to candidates who are high risk for long operating times and extensive anesthesia risk.3,4
Major advantages of muscle flaps are reliable soft tissue coverage of bone and tendons and preservation of arteries of the lower extremity.5,6 There have been reports of satisfactory results of distally based abductor hallucis muscle flap for medial forefoot defects. 7
The reverse abductor hallucis muscle flap is ideally suited for small to moderate-sized defects in the vicinity of the first metatarsophalangeal joint based on its arc of rotation. It allows for robust vascularized soft tissue coverage. It is simple to rise and is transposed easily within the wound. 5
In this article, we present our experience with 5 patients who failed local wound care and healing by secondary intention for at least 6 months duration. The patients were treated successfully using reverse abductor hallucis muscle flap.
Patients and Methods
From September 2015 to May 2017, 5 distally based abductor hallucis muscle flaps were used for reconstruction of soft tissue and bone defects of the first metatarsal head region. Of these patients, 2 were females and 3 were males with an age range of 39 to 56 years (average 48 years). The patients were followed-up from 1.1 years to 1.7 years. All patients’ wound was due diabetes mellitus peripheral neuropathy. The size of the defects ranged from 1.7 cm × 3.2 cm to 3.2 cm × 3.3 cm (average = 9.17 cm2; Figure 1A and B). Patients’ wound was staged8,9 with an initial surgical intervention of incision drainage and excisional debridement of all nonviable tissues and bone. The patients then underwent a second staged procedure of reverse abductor hallucis muscle flap.

All patients’ wound was due diabetes mellitus peripheral neuropathy. The size of the defects ranged from 1.7 cm × 3.2 cm to 3.2 cm × 3.3 cm (average = 9.17 cm2).
Surgical Technique
A skin incision was made from the proximal most aspect of the ulcer with extension along the glaberous junction of the medial aspect of the foot under tourniquet.
The abductor hallucis tendon was identified distally and a vessel loupe was inserted around it for manipulation (Figure 2). The abductor hallucis muscle was dissected out proximally under 3.5× loupe magnification and a hand-held Doppler. Two minor perforator arteries were identified in between the abductor hallucis and the flexor hallucis brevis muscle belly. The minor pedicles appeared to be approximately 1 mm in diameter. Vessel loops were utilized to tag the minor pedicles. The muscle was then dissected proximally. It was skeletonized from the abductor hallucis tendon utilizing blunt dissection.
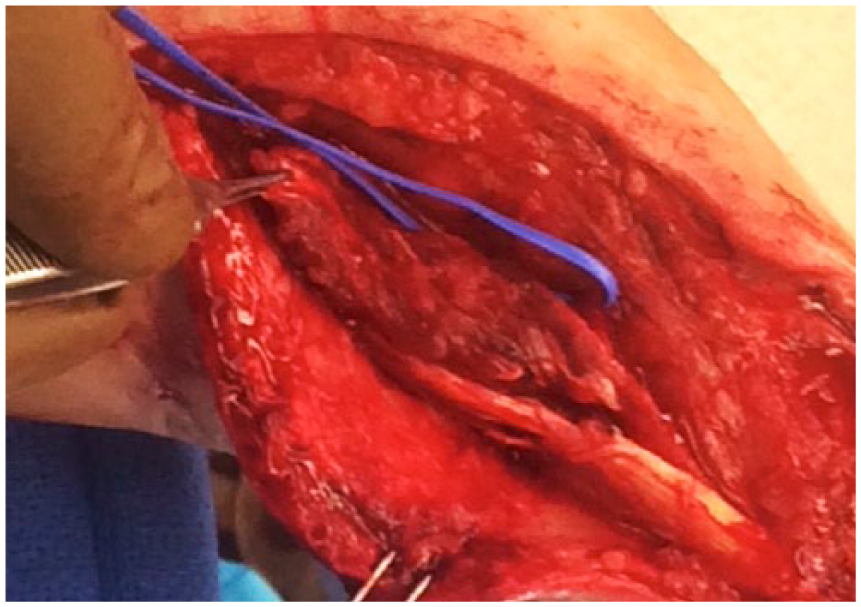
The abductor hallucis tendon was identified distally and a vessel loupe was inserted around it for manipulation.
The tourniquet was deflated. Utilizing a hand-held intraoperative Doppler, a brisk signal was obtained from the minor pedicles. An approximate measurement was made from the distal most pedicle flap to distal most aspect of the ulcer. The measurement was then transposed proximally from the pedicle. The pedicle was to be utilized as the pivot point. One centimeter was added to the length of the muscle proximally. The muscle was then cut with a tenotomy scissors (Figure 3). A vascular clamp was then applied to the proximal pedicle. The muscle cut was evaluated for bleeding based on the distal pedicle. This intraoperatively confirmed adequate vascularity to the muscle flap. The proximal minor pedicle was ligated with a hemoclip.
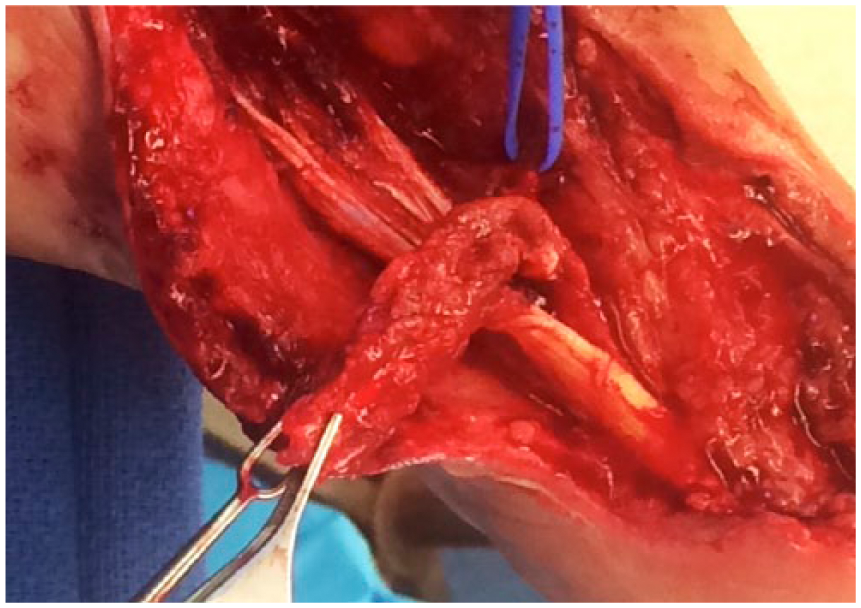
After exposure of the abductor hallucis muscle, the muscle was then cut with a tenotomy scissors proximally.
The muscle was then turned down distally to cover the exposed bone and joint of the medial first metatarsophalangeal joint (Figure 4). It was provisionally tagged distally with 4-0 Vicryl. The artery pedicle was then checked via hand-held Doppler and confirmed a brisk signal. The remainder of the muscle was then secured in place with 4-0 Vircyl. The area was irrigated with normal saline. The muscle continues to bleed. A 2 × 2 bilayer allograft matrix was then utilized to close the remainder of the soft tissue deficit (Figure 5). It was secured in place utilizing skin staples.

The muscle was transposed distally to cover the exposed bone and joint of the medial first metatarsophalangeal joint.

A 2 × 2 bilayer allograft matrix was utilized to close the remainder of the soft tissue deficit and was secured in place utilizing skin staples.
Results
All flaps survived with no further operations needed to achieve defect coverage. All cases underwent a third-stage wound closure 3 weeks postoperatively that involved harvest and application of split thickness skin graft from the ipsilateral lower extremity (Figure 6). They attained complete wound closure 6 weeks from the initial incision and debridement. The donor sites in all patients healed uneventfully (Table 1). At the last follow-up all flaps provided stable defect coverage and good contour (Figure 7). No patients needed further flaps for defect reconstruction. In our series, all patients were satisfied with the surgical outcome. No disturbance of foot mobility and strength was noticed. The absence of abductor hallucis muscle did not affect the foot function and secondary hallux valgus deformity.

All flaps survived with no further operations needed to achieve defect coverage and underwent a third-stage wound closure 3 weeks postoperatively that involved harvest and application of split thickness skin graft from the ipsilateral lower extremity.
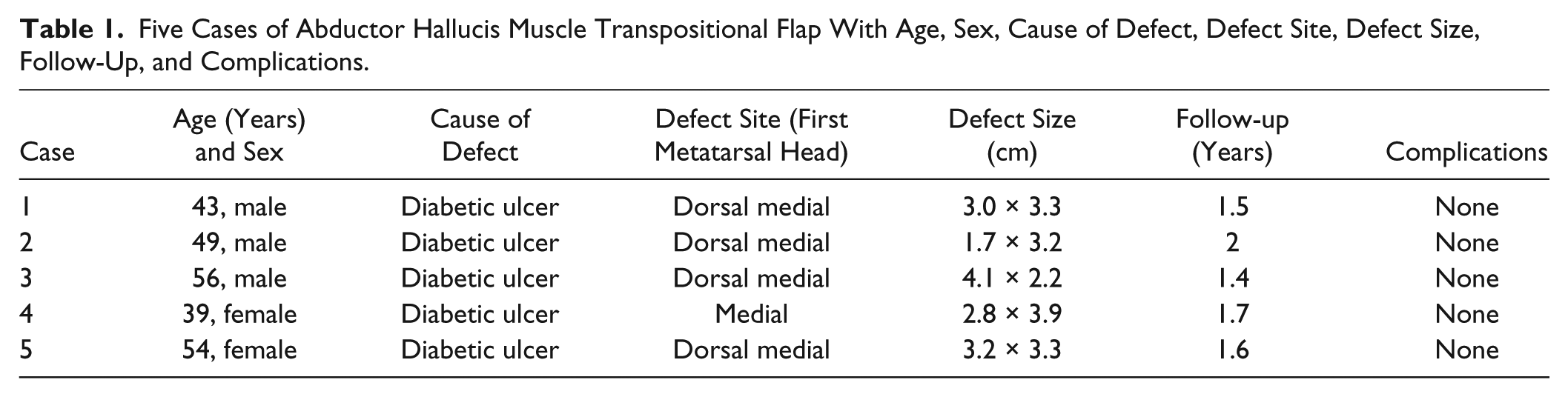
Five Cases of Abductor Hallucis Muscle Transpositional Flap With Age, Sex, Cause of Defect, Defect Site, Defect Size, Follow-Up, and Complications.

At the last follow-up all flaps provided stable defect coverage and good contour.
Discussion
Vascularized muscle flaps offer coverage of wounds in the lower extremity when local wound care fails. They provide increase blood supplies with improve oxygen transports, which allows direct delivery of host defense mechanisms. 4
The abductor hallucis muscle is 1 of 6 intrinsic muscles reported useful for foot and ankle defects. It is a Type II muscle classified by Mathes and Nahai and defined as being supplied by one major proximal pedicle and minor distal pedicles. 10
The distally based abductor hallucis flap has well-vascularized tissue in providing reliable coverage. It receives its blood supply from minor and major pedicles in a retrograde fashion from both the dorsal arterial network and the deep plantar system through communicating branches with the medial plantar artery. Because the proposed flap has a double source of vascularity, the presence of a single, patent dorsalis pedis or tibial artery alone would suffice for utilization of the flap with safety. Since the lateral plantar artery is not sacrificed during flap dissection, the vascularity of the sole and the entire foot is preserved. 11
The abductor hallucis muscle flap is advantageous for lower extremity wounds since donor site morbidity is minimal and harvest does not harm the weight-bearing surface. In addition, the majority of the donor site can be closed primarily while the muscle is covered with bilayer allograft matrix.
A disadvantage of the abductor hallucis muscle may be the small muscle bulk, which may not be adequate for coverage of wounds. A study by Attinger et al reported that local muscle flaps are ideal for closure of defects less than or equal to 3 × 6 cm2 at the foot or ankle with exposed bone, joint, or tendon. 12
This article demonstrated that distally based abductor hallucis muscle flap is an excellent option for reconstruction of the soft tissue defects of the forefoot. Delayed split thickness skin graft for the muscle flap as utilized in order to enhance the survival rate as the exudate of the flap would be decreased and uptake of the skin could be more favorable. Therefore, bilayer wound matrix allograft was used initially to augment the muscle transfer. 13
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.