
Abstract
The aim of this study was to identify overall recurrence rates after reconstructive surgery in patients with pressure ulcers and to identify risk factors that associated with recurrence after reconstructive surgery. This study was done in Faculty of Medicine Chiang Mai University, including recurrence at the same site as well as on new sites, between January 1998 and December 2015. 165 patients with 272 pressure ulcers were retrospectively collected and analyzed. The overall pressure ulcer recurrence rate was 16.54% (45 from 272 ulcers) from an overall patient recurrence of 19.39% (32 from 165 patients). From multivariable analysis, we found 9 prognostic factors that were statistically significant for recurrence after surgery, divided into 2 groups: uncontrollable and controllable factors. Uncontrollable factors consisted of being female (hazard ratio [HR]=1.90;95%CI=1.54-2.34), being older than 45 years (HR=1.67;95%CI=1.40-2.0), and location of pressure ulcers on ischium (HR=1.65; 95% CI=1.51-1.80) and sacrum (HR=1.17;95%CI=1.10-1.23). Controllable factors included spasticity (HR=1.11;95%CI=1.04-1.20), incomplete healing before discharge (HR=5.42;95% CI=3.95-7.44), serum albumin level ≤3 g/dL (HR=1.27;95%CI=1.13-1.43), pressure ulcer stage 4 (HR=1.90;95%CI=1.41-2.54), non -muscle-based procedure (HR=3.82;95%CI=2.54-5.76), and length of hospitalization >21 days (HR=2.94;95%CI=1.60-5.40). Patients with these factors were strongly advised to address and improve all these factors for decreasing the recurrence rate after reconstructive surgery.
Pressure ulcers, pressure sores, or bedsores are defined as ischemic changes resulting in soft-tissue injuries from unrelieved pressure over an extended period of time. Pressure ulcers usually occur on skin over bony prominences or on bare seated weight areas such as the trochanter or sacrum.1,2 Pressure ulcers are one of the most common complications in patients who suffer from acute critical illness, who are unconscious, or have spinal cord injury or a chronic complicated disease that compromises the mobility and sensitivity of the patients.
In the United States, approximately $11 billion was utilized in the treatment of 2.5 million pressure ulcers. 2 However, pressure ulcers not only result in excessive medical expenses and make high demands on labor in the health care system, but also prolong recovery time and hospital stay for the patients. Final outcomes can lead to chronic disability, and there is an increase in overall morbidity and mortality.
In Thailand, the incidence of pressure ulcer is between 6.4% and 55% of all patients in hospitals. 3 At Maharaj Nakorn Chiang Mai hospital, the incidence of all stages of pressure ulcers per year is estimated to be in the region of 0.5%. Numerically, this is almost 200 out of the 40 000 patients admitted per annum, which is less than the rate in the previous report, which covered the whole of Thailand.
As described above, there is a high level of occurrence and far-reaching consequences of pressure ulcers, but there have also been many improvements in treatment protocol and preventive guidelines. The most problematic issue is the recurrence after surgical closure, which ranged from 5% to 90% in 1998. 4 In 2013, it was reported to be between 3% and 82%, of which 49% of recurrence is in patients with spinal cord injuries. 2 This statistical record is very interesting, if rather worrying, because over a 15-year period, the recurrence rate is still high with no decrease in trend. From an extensive review of the literature, there is a lack of evidence to support why recurrence after surgical management is still high, especially in Thailand where demographics and socioeconomics of patients are very different from that in the west.
Study Objectives
The primary objective was to study overall recurrence rates after reconstructive surgery of pressure ulcers in Maharaj Nakorn Chiang Mai hospital, including whether recurrence is on the same site or at a new site. The secondary objective was to identify risks and prognostic factors that promote recurrence after reconstructive surgery.
Materials and Methods
This study was initiated after ethical approval from the ethics committee of Faculty of Medicine, Chiang Mai University (072/2016:EC4). A retrospective observational cohort study was carried out using data from the medical records of all high-grade pressure ulcer patients (stages III and IV), who underwent reconstructive surgery by the Department of Plastic and Reconstructive Surgery at Maharaj Nakorn Chiang Mai hospital between January 1998 and December 2015. Individuals with pressure ulcers at stages I and II who were treated with nonoperative methods are not included in this study. To ensure accuracy and to limit missing results, data collected regarding all patients who matched the inclusion criteria were cross-checked using the surgical admission form at the outpatient department and the recording system in the operating room.
Data were gathered for 3 categories: patients, pressure ulcers, and operative treatments. First, the patient demographics were evaluated according to the following: gender; age; cause and onset of injury; status of patient (paraplegia, quadriplegia, hemiplegia); presence or absence of spasticity and joint contracture; preoperative albumin level; the Braden scale (the most frequently used assessment scale to identify risk of developing pressure ulcers, composed of 6 subscales: sensory perception, skin moisture, activity, mobility, friction/shear, and nutrition; Braden allows the classification of patients into 5 groups: no risk, at risk, and moderate, high, and very high risk 1 ); comorbidity that diminishes blood circulation (diabetes, smoking, heart failure, vasculitis, and peripheral vascular disease), and caregiver of patient (family, foundation, or unaccompanied). In the second category, the ulcer characteristics were evaluated as primary (patients who had a first-time diagnosis of a pressure ulcer) or secondary/recurrence (those who had previously been diagnosed with pressure ulcers and underwent reconstructive surgery; these were subclassified into recurrence at the same site and development at a new site). Also, in this second category, the following were included: location, stage, number of pressure sores, onset, size (area of skin defect in centimeter squared), and pocket (volume of affected space in centimeter cubed). Third, the operative treatments were evaluated according to surgical procedure, length of hospital stay, postoperative complications, and condition at discharge (complete or partial healing).
Data analysis was performed using STATA version 11.0. Categorical data were reported as frequencies and percentages. Continuous data were presented as means ± SDs or medians (interquartile range). The risk stratification between the recurrence and nonrecurrence group was calculated using Fisher’s exact test (categorical variables), and Student’s t-test and Wilcoxon rank sum test (normal and nonnormal distribution of continuous variables, respectively). The prognostic factors of recurrence were evaluated using the Cox proportional hazard model, reported as hazard ratio (HR), 95% CI, and P value. The difference was taken to be statistically significant when P <.05.
Results
A total of 165 patients with 272 pressure ulcers were admitted to the Department of Plastic and Reconstructive Surgery at Maharaj Nakorn Chiang Mai hospital between January 1998 and December 2015 for surgical reconstruction.
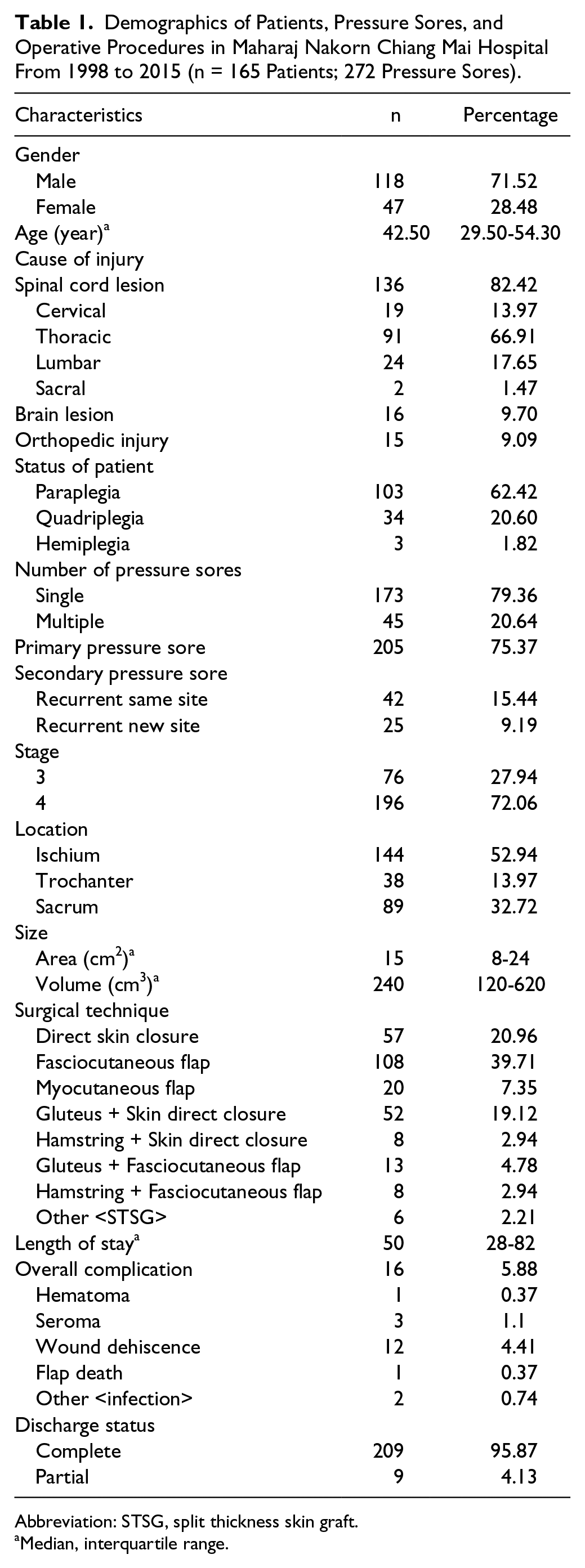
The patient demographics are shown in Table 1. The majority of patients were male (71.5%). The median age was 42.5 years at the time of surgery (interquartile range = 29.5-54.3 years). Pressure ulcers most commonly occur in spinal cord injury patients (82%), most of whom are affected at the thoracic level (67%), followed by brain injury (10%) and orthopedic injury (9%) patients. The highest category of patient status was paraplegia (62%).
Demographics of Patients, Pressure Sores, and Operative Procedures in Maharaj Nakorn Chiang Mai Hospital From 1998 to 2015 (n = 165 Patients; 272 Pressure Sores).
Abbreviation: STSG, split thickness skin graft.
Median, interquartile range.
The ulcer characteristics are also illustrated in Table 1. Of 272 pressure ulcers, 75% are first-diagnosis pressure ulcers (primary). The remaining 67 pressure ulcers are recurrent/secondary; of these, 15% had recurred on the same site, and 9% had developed on new sites. Multiple pressure ulcers (≥2 pressure ulcers) were found in 21% of cases. A majority (72%) of pressure ulcers were stage IV, with nearly half occurring on the ischium (53%), followed by sacrum (33%) and trochanter (14%). The median skin defect area was 15 cm2 (range 8-24 cm2), and the median pocket volume was 240 cm3 (range 120-620 cm3).
The operative treatments are also presented in Table 1. The 3 most frequent techniques used in pressure ulcer closure are fasciocutaneous flap (40%), direct skin closure (21%), and gluteus muscle with skin direct closure (19%). The median total length of stay was 50 days (range = 28-82 days). The overall postoperative complication rate was 6%, of which the most common was wound dehiscence (4%), and all cases were resolved by conservative treatment. Flap death occurred in 1 patient who underwent the gluteus muscle with direct skin closure procedure. He required reoperation for debridement and split thickness skin graft coverage, and complete healing was finally achieved. Pressure ulcers had healed completely in 96% of cases before discharge.
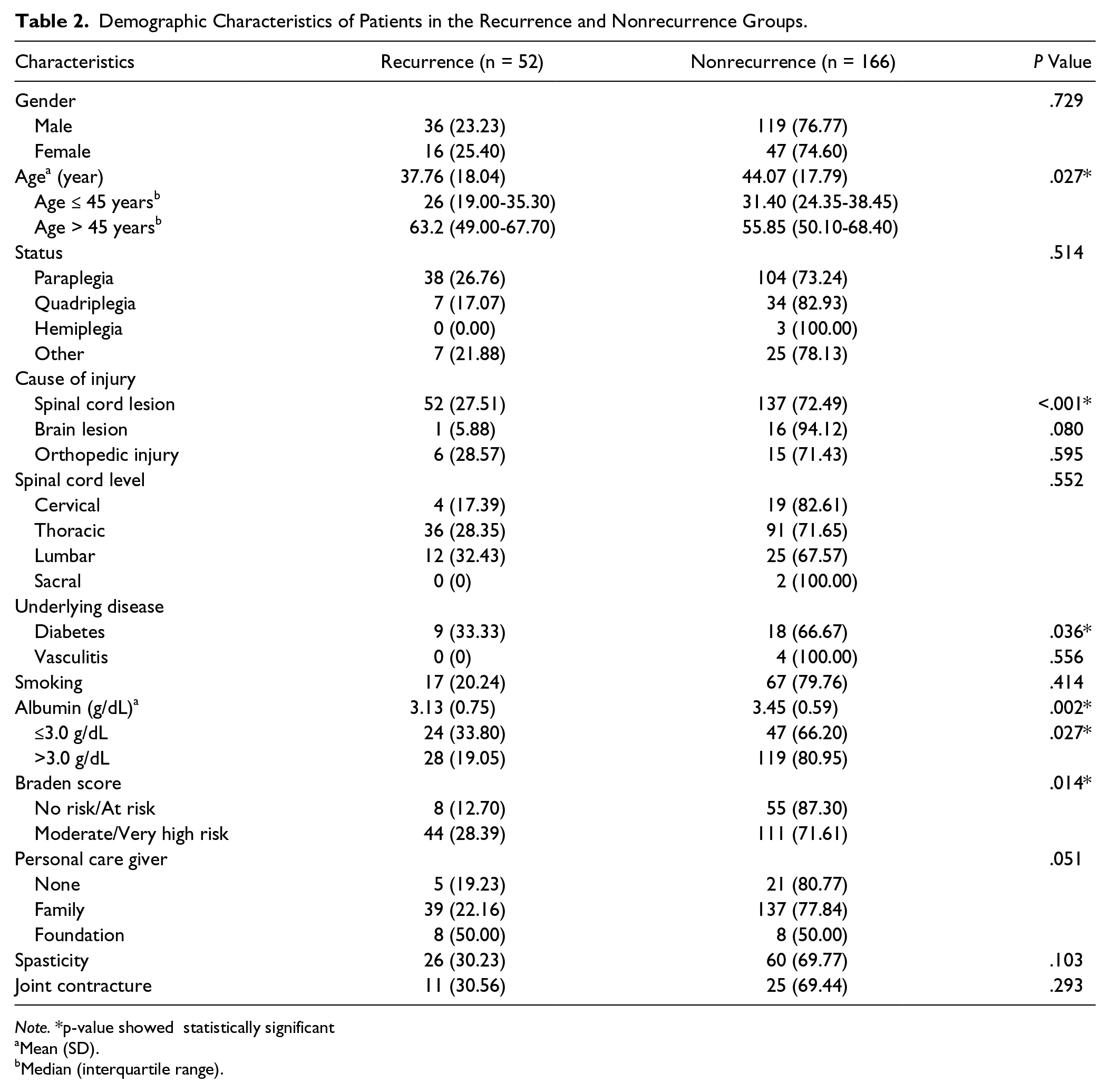
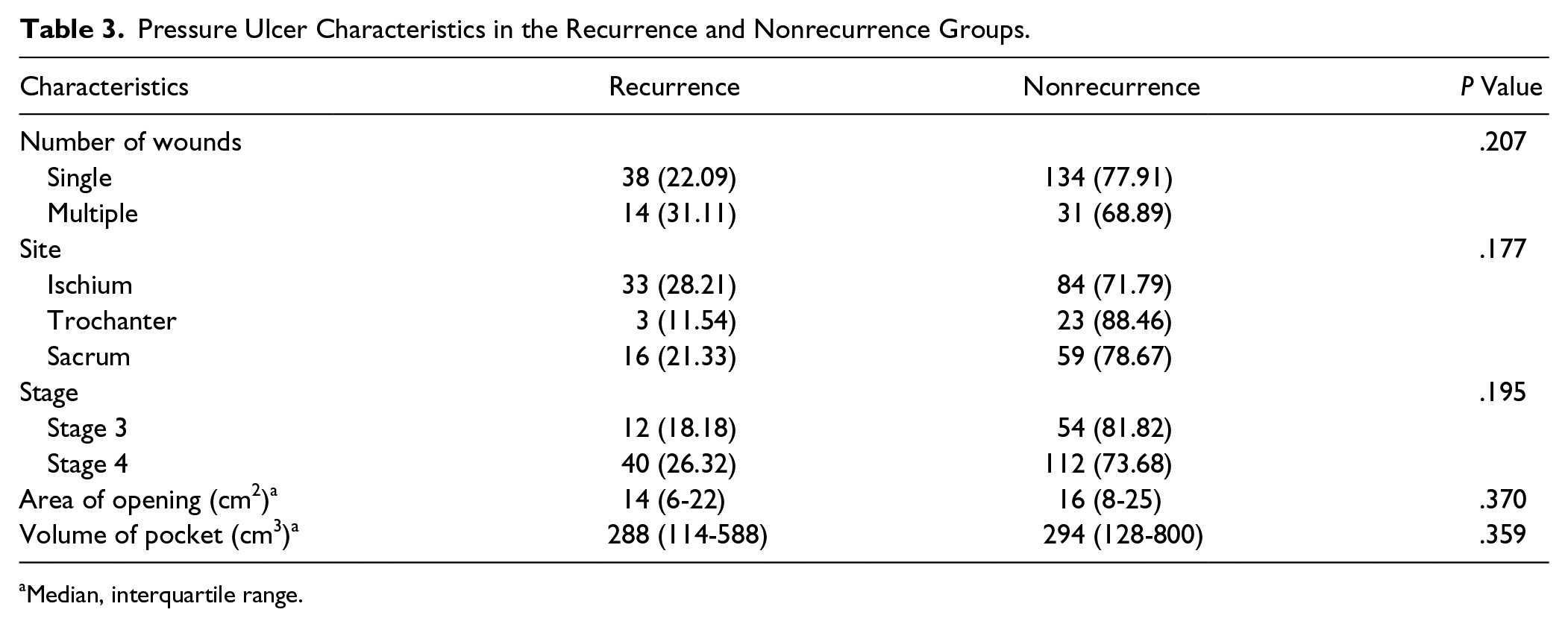
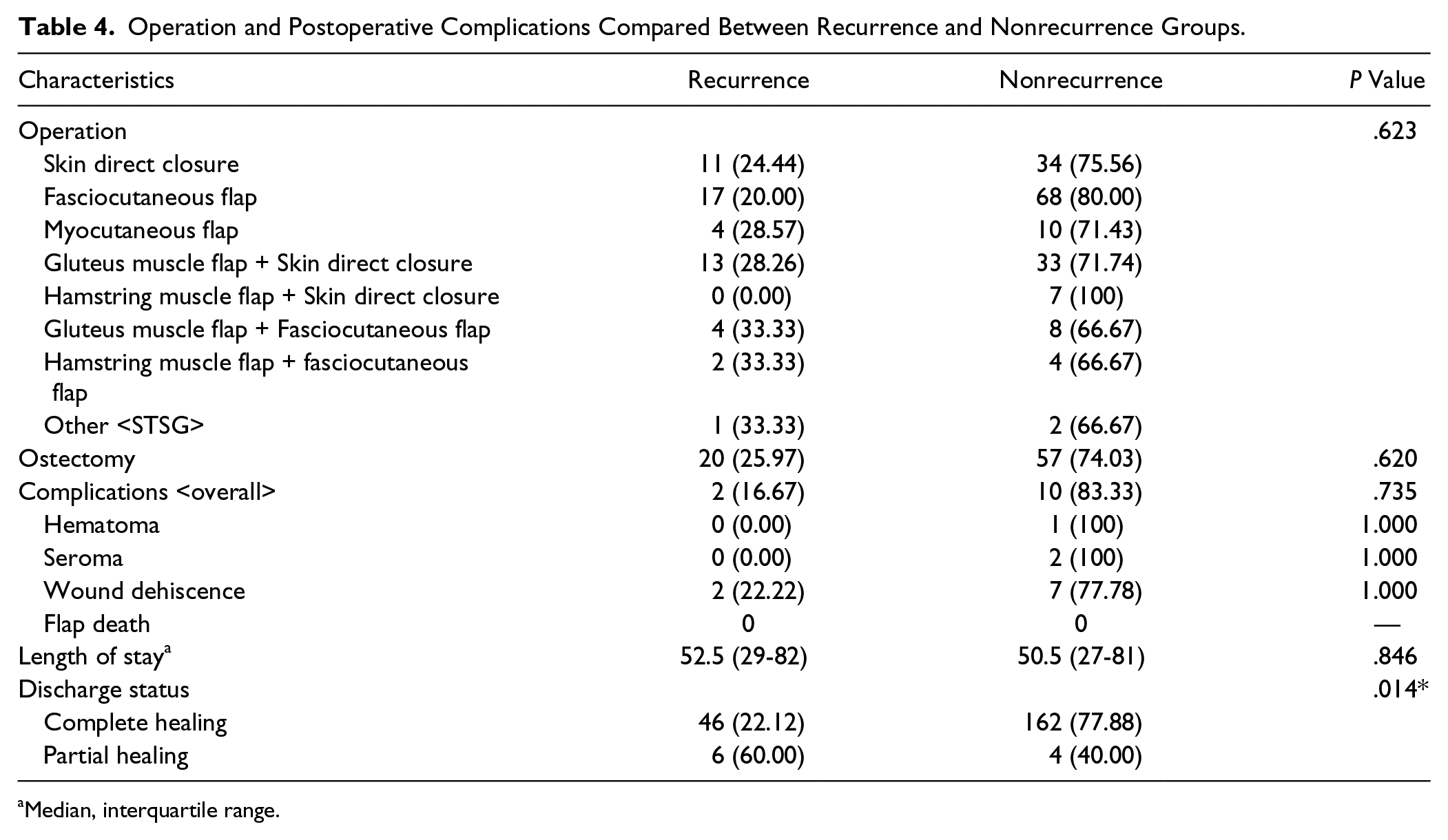
Of the 272 pressure ulcers requiring reconstructive surgery in 165 patients, the recurrence rate was 45 ulcers (16.54%) from an overall patient recurrence of 19.39% (32 from 165 patients). The patient factors that showed statistically significant differences between the recurrence and nonrecurrence groups (Table 2) were age (P = .027) and underlying diseases such as diabetes (P = .036) and spinal cord lesions (P < .001). Albumin level before the operation was also significant (P = .002). In the recurrence group, the mean albumin level was 3.13 ± 0.75 g/dL, whereas that in the nonrecurrence group was 3.45 ± 0.59 g/dL. The cutoff point level at 3.0 g/dL still showed a significant difference between the 2 groups (P = .027). When the Braden Scale was categorized into 2 main groups—no risk to at risk (score 15-23) and moderate to very high risk (score 6-14)—there was a significant difference between recurrence and nonrecurrence groups, with P =.014. Surprisingly, there was no significant difference between the recurrence and nonrecurrence groups when it came to the personal care aspect (familial support vs foundation vs live alone). There was also no statistically significant variation in the pressure ulcer stage, location, number, or even area and volume between recurrence and nonrecurrence groups (Table 3). But timing to the development of pressure ulcers after the cause were different; for the recurrence group, it was 9.71 months (3.26-30.43) and for the nonrecurrence group, 7.09 months (1.34-18.03; P = .040). For operative and postoperative factors, the patient status before discharge between complete and partial healing was found to be the only significantly different factor (P = .014; Table 4).
Demographic Characteristics of Patients in the Recurrence and Nonrecurrence Groups.
Note. *p-value showed statistically significant
Mean (SD).
Median (interquartile range).
Pressure Ulcer Characteristics in the Recurrence and Nonrecurrence Groups.
Median, interquartile range.
Operation and Postoperative Complications Compared Between Recurrence and Nonrecurrence Groups.
Median, interquartile range.
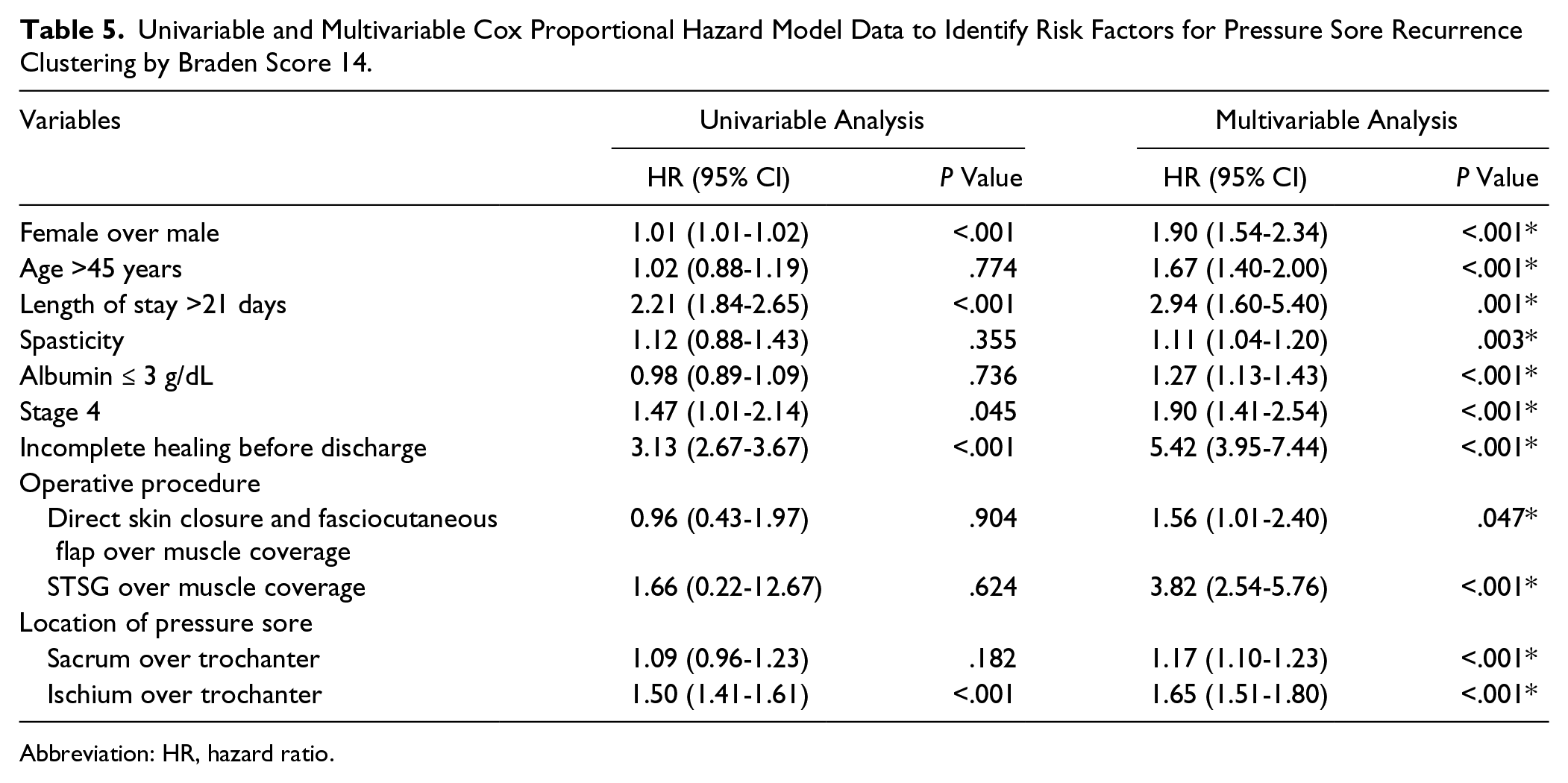
To identify prognostic factors using the univariable and multivariable Cox proportional hazard model, clustering by Braden Score 14 showed 9 factors that affected the recurrence of pressure ulcers (Table 5). First, the incomplete healing of pressure ulcers before discharge was the strongest factor predicting the recurrence of pressure ulcers, with HR = 5.42 (95% CI = 3.95-7.44; P = .001). Surgical closure technique, the second most important factor, was also an important part that definitely affected recurrence. Operations that obliterated the cavity of the pressure ulcer with muscle-based coverage—in this study, the myocutaneous flap, gluteus or hamstring muscle flap with skin direct closure, and gluteus or hamstring muscle flap with fasciocutaneous flap closure—were found to be the best techniques for prevention of recurrence. A split thickness skin graft was the worst technique, when compared with muscle coverage, with promoted recurrence HR =3.82 (95% CI = 2.54-5.76; P < .001), followed by direct skin closure and fasciocutaneous flap coverage alone, with HR = 1.56 (95% CI = 1.01-2.40; P = .047).The third strongest prognostic factor was a total length of stay of more than 21 days, having an increased recurrence, with HR =2.94 (95% CI = 1.60-5.40; P = .001). Being female and age >45 years also put the patients at risk, with HR = 1.90 (95% CI = 1.54-2.34; P < .001) and 1.67 (95% CI = 1.40-2.00; P < .001), respectively. As regards status before the operation, patients with spasticity and poor nutrition, with an albumin level ≤3.0 g/dL, tended to have a higher incidence of recurrence, with HR =1.11 (95% CI = 1.04-1.20; P = .003) and 1.27 (95% CI = 1.13-1.43; P < .001), respectively. Stage 4 pressure ulcers were more recurrent when compared with stage 3, with HR =1.90 (95% CI = 1.41-2.54; P < .001). The 3 most common locations of pressure ulcers in this study were ischium, sacrum, and trochanter, respectively; when compared, the trochanteric site is rarely the site of recurrence, with the risk increasing for the sacrum (HR = 1.17; 95% CI = 1.10-1.23; P < .001) and ischium (HR = 1.65; 95% CI = 1.51-1.80; P < .001).
Univariable and Multivariable Cox Proportional Hazard Model Data to Identify Risk Factors for Pressure Sore Recurrence Clustering by Braden Score 14.
Abbreviation: HR, hazard ratio.
Discussion
Pressure ulcers are one of the most important complications in patients who are admitted all over the world, including those in Thailand and Maharaj Nakorn Chiang Mai Hospital. Despite treatment protocols and preventive strategies being implemented over several years to reduce the incidence of pressure ulcers, the recurrence rate after surgical treatment, either at the same or a new site, is still high and there is no decrease in trend. Cushing and Phillips 2 reported a recurrence rate of between 3% and 82%. In this study, we found that pressure ulcers recurred after surgical treatment in 45 out of 272 pressure ulcers in 165 patients from 218 admissions between January 1998 and December 2015. The overall pressure ulcer recurrence rate was 16.5%, very close to the 19% reported by Kierney et al. 5 Getting an overall understanding and studying the factors that promote the recurrence is key to solving this problem.
The patient demographics of the 165 patients, 72% of whom were men, were discussed previously.5,6 The most common cause of induced pressure ulcers was spinal cord injury (82.4%), with the most frequent injury level being the thoracic spine (66.9%) and the most frequent status being paraplegic (62.4%), again, similar to many reports.4-6
The univariable analysis, indicated no significant difference in spinal cord lesion between the recurrence and nonrecurrence groups (P < .001). Also, the multivariable risk analysis showed no statistical significance in either the spinal cord lesion, including level of injury, or paraplegic status. So both cause of injury and status of the patient did not play significant roles in the recurrence of pressure ulcers.
The median age of all patients with pressure ulcers was 42.5 years (ranging from 29.5 to 54.3 years); this paralleled a previous report, with 42 ± 13.65 years. 6 We found cause of injury to be age related: the commonest cause in the younger age group was trauma associated but in the older age population, it was usually related to severe illness and chronic disease. Cited rehabilitation research that focused on spinal cord injured patients reported that the mean age was 39.27 ± 11.4 years. 7 The older the age, the higher the risk of developing pressure ulcers. This is supported by Catherine et al 8 whose study mentioned that being older than 70 years is one of the risk factors for recurrence after surgery. The American Heart Association also reported that age >45 years increases the lifetime risk of cardiovascular disease both in men and women. 9 There is also a recommendation by the American Diabetes Association that screening for diabetes should start at 45 years of age. 10 Both cardiovascular disease and diabetes not only compromise vascularization and impaired wound healing, but also lead to immobility in cases of complications such as cerebrovascular accident. Keys et al 11 found that poorly controlled diabetes with hemoglobin A1c >6% is a significant predictor of recurrence of pressure ulcers. Diabetes, from the results of the univariable analysis in our study, led to a significant difference between recurrence and nonrecurrence groups (P = .036). But in the multivariable analysis, neither cardiovascular disease nor diabetes affected the recurrence of pressure ulcers. But age >45 years significantly increased the risk of pressure ulcer recurrence (HR = 1.67; 95% CI = 1.40-2.00; P < .001). This is in contrast to the study carried out by Keys et al, 11 which reported that age <45 years was associated with an increased risk of recurrence. The Keys et al 11 study, a multiyear retrospective data review about predictors of flap coverage failure in early and late recurrence, included data from 137 service veteran patients, and overall flap failure with recurrence was 38.8%. The difference between our study and that of Keys et al 11 is that the patients were predominantly male and they were all veterans, whom we suggest are stronger and have no serious underlying disease. This study did not mention the causes of the pressure ulcers, which we assume were from war-associated severe trauma. So all these veterans tended to suffer from pressure ulcer conditions from a young age and had lived with them; these severe causes may be uncorrectable for a lifetime. So they were faced with more chance of recurrence than in our study, which was carried out on a normal Thai population, including all age groups with many underlying diseases.
Being female is another factor that increased the risk of recurrence, with HR =1.90 (95% CI = 1.54-2.34; P < .001). Supported by Opara et al, 12 a cross-sectional study about an aging society in Thailand, in 2011, found that the majority of the elderly are female (70.4%). Older age, severe underlying diseases, and longer periods in welfare centers significantly increase risk of illness, including skin problems (P = .002). After an acute phase, all patients turn to rehabilitation programs, as reported by Pattanakuhar et al, 7 who found athletic characteristics in men more than women (P < .001). In paraplegic patients, the major part of the pressure ulcer population, arm strength is needed to participate in a rehabilitation program. The higher performance is by men in this area, hence time of pressure sustained is less. Another result from the same study 7 shows that women have less coping skills to face and accept the consequences of illness than men (P = .001), with delay in participating in rehabilitation programs and decreased intention of taking care of themselves, which leads to spiritual and functional problems later. All these reasons explain why being female is a significant risk factor for pressure ulcer recurrence.
Preoperative status also plays an important role in pressure ulcer treatment. Bauer Bauer and Phillips 13 showed that adequate wound healing required more than 2.0 g/dL of serum albumin. Catherine et al 8 indicated that the promoting factors for recurrence of pressure ulcer after surgery is poor nutritional status, and prevention of pressure ulcer development needs a serum albumin level of at least 3.5 g/dL. In our study, we found that a serum albumin level of ≤3 g/dL increased the risk for recurrence, with HR =1.27 (95% CI = 1.13-1.43; P < .001). This is concordant with a wide acceptance of preoperative nutritional principles. A meta-analysis showed that these patients need an oral nutritional supplement of 250 to 500 kcal for at least 2 to 26 weeks 14 and a protein intake of 1.5 to 3.0 g/kg/d 13 to decrease this risk.
Spasticity also shows a correlation with the risk of pressure ulcer recurrence, with HR =1.11 (95% CI = 1.04-1.20; P = .003). Evidently, spasticity is a common neurological sequela and is frequently found after spinal cord injuries. This is diagnosed by greater muscle tone, hyperreflexia, and clonus, all of which will increase the stress, castrate the pressure distribution, and finally lead to pressure sore occurrence. Bauer and Phillips 13 pointed out that the key to successful recovery of a pressure ulcer coverage is to treat spasticity and joint contracture promptly before surgery.
When considering pressure ulcer characteristics, primary pressure ulcers constituted nearly three-quarters of the cohort, as found previously. 5 Of the remainder, our study found that anatomical location is significantly associated with recurrence. Ischium is the most common site for recurrence, a fact also cited in many reviews,4-6,11 when compared with trochanteric ulcers, with HR =1.65 (95% CI = 1.51-1.80; P < .001), followed by sacrum, which has a greater recurrence rate than the trochanter, with HR =1.17 (95% CI = 1.10-1.23; P < .001). This shows a very close correlation with spinal cord injury–induced paraplegia, the most common cause of pressure ulcers, mainly occurring after patients joined a rehabilitation program and started daily activities with wheelchairs. This sitting posture with feet supported resulted in a pressure up to 100 mm Hg over the ischial tuberosities, 1 with a very high probability of developing pressure ulcers on the ischial site. Keys et al 11 also reported ischial wounds as being a predictor of late recurrence (OR = 4.01; P = .001).
Of all 272 pressure ulcers, 28% were stage 4, diagnosed by full-thickness tissue loss with exposed muscle, tendon, or bone. Also, we found that a stage 4 pressure ulcer is also a predictor of recurrence, with HR =1.90 (95% CI = 1.41-2.54; P < .001). The size of the pressure ulcer was evaluated using 2 parameters: the area of skin defect and the volume of the pocket. Bearing in mind the phenomenon “tip of the iceberg,” skin is much more ischemic resistant than muscle, 2 so planning for treatment not only by skin defect but also the depth of the wound is essential. However, in our study, when the recurrence and nonrecurrence groups were compared, there was no statistically significant difference between wound size and recurrence rate.
The advantages and disadvantages regarding the use of muscle for coverage of pressure ulcers is still controversial. The advantages are that the cavity of the pressure ulcer can be obliterated by the bulkiness of the muscle, providing more durable tissue at the closure site, which makes it superior to skin grafts and causes no further tension on the wound as in primary closure. 13 The muscle can also distribute the pressure projected to the skin. But the weakness is that muscle survival depends on good vascularity because it cannot tolerate ischemic necrosis 1 ; it requires more meticulous surgical techniques and a more experienced surgeon, and finally, more frequently leads to flap death and exposes the patients to more risks and complications.
The multivariable analysis from our study indicated that the myocutaneous flap, gluteus or hamstring muscle flap with skin direct closure, and gluteus or hamstring muscle flap with fasciocutaneous flap closure, all of which are muscle-based procedures, were the most effective techniques. The split thickness skin graft, when compared with muscle coverage, promoted recurrence with HR =3.82, a status followed by direct skin closure and fasciocutaneous flap coverage alone with HR =1.56. So, from our study, we recommend a muscle-based procedure rather than primary closure, skin grafts, and fasciocutaneous flaps. The type of muscle should depend on the anatomical location of the pressure ulcer and the experience of surgeons. But the most important point that should always be kept in mind is that pressure ulcers are complications of severe or chronic diseases in which most of the causes are uncorrectable and unchangeable. Recurrence is possible, so the surgeons must ascertain that there is sufficient muscle for a second procedure.
The overall complication rate is 5.9% (16 from 272 pressure ulcers). All complications occurred within 3 weeks postoperation, and there was no significant difference between the recurrence and nonrecurrence groups. In all, 4.1% of all pressure ulcers had incomplete healing before discharge, and this was found to be the strongest prognostic factor for recurrence (HR = 5.42; 95% CI = 3.95-7.44; P < .001). As in a previous report, we found that same-site failure increased the risk of recurrence. 11 There are several possible reasons for this: the same historical skin defect and the loss of normal skin barrier, so the ulcer can easily progress deep down to the underlying structure. With a lack of adequate dressing and debridement, it can aggravate to a worsening of the stage. An additional problem is that patients will alter their position to avoid the pain and discomfort—antalgic position—which can easily lead to the development of pressure ulcers at new pressure-loaded sites.
Complications not only increased morbidity and mortality, but also led to lengthening of hospital stay. This put the patients under more stress, both physically and psychologically, and exposes them to a nosocomial infection, which usually results in disability and being bed ridden and again starts the vicious cycle of pressure ulcers. In our study, a length of stay in hospital of more than 21 days was also a high prognostic factor for recurrence (HR = 2.94; 95% CI = 1.60-5.40; P = .001).
We classified these 9 factors into 2 groups: controllable and uncontrollable. Controllable factors included spasticity, discharge status, serum albumin level, stage of pressure sore, procedure and length of stay; all of these can be addressed. These analytical data strongly suggest the need for a paradigm shift in our management: we need to improve the spasticity with both medical and physical treatment, try to treat all pressure ulcers until healing is completed before discharge, support and improve nutritional status before any operation, ensure adequate dressing of wounds for preventing stage 3 turning into stage 4, and choose the muscle-based procedure if it is compatible with the patient’s condition. Patients who are identified as having uncontrollable factors—being female, older than 45 years, and location of pressure ulcers at the ischium and sacrum—should be identified as being in the high-risk group for recurrence. The controllable factors need addressing: close monitoring and more frequent follow-up can help in the detection of a new problem, allowing early treatment before progression.
Limitations
A retrospective observational design, as used in this study, is dependent on the accuracy of medical records at the time of admission. This study includes 17 years’ worth of data, and some recording errors and incompleteness of data may have inadvertently been included.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Neither author has any financial interest with any products or services involved in the content of this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.