
Abstract
Lymphatic malformations are benign vascular malformations rarely seen in adults. There have been only around 100 cases reported in the literature, most of them located in the head and neck area. The etiology is poorly understood but trauma, infection, or tumors have been suggested as possible causes. We present an unusual case of lymphatic malformations in the lower extremity of a 56-year-old male patient after minor trauma. The masses were asymptomatic but progressively enlarged for a period of 2 months, developing into a mass with a 21-cm-long axis in computed tomography images. Total surgical resection was performed and there were no complications or recurrence during the 1-year follow-up period. We present this rare case with a review of relevant previous literatures.
Lymphatic malformations (LMs) are benign vascular malformations of the lymphatic system with a predilection for head and neck, oral cavity, axilla, and abdomen. Almost half of all lesions are diagnosed at birth, and over 90% manifest before 2 years of age.1,2 Adult-onset LMs are very rare, and only 3 cases of LMs located in the lower extremities of adults have been reported in the English literature.3-5 We present the case of a 56-year-old male, who was diagnosed with cystic LMs in his right thigh. He was managed successfully with direct surgical excision and was free from recurrence in the follow-up period of 1 year.
Case Report
A 56-year-old male patient presented with complaints of multiple palpable masses in his right thigh. According to him, the lesions had been noted incidentally 2 months ago and had enlarged rapidly without any other symptoms such as pain. The patient had a history of minor trauma about half a year before symptom onset. He said he had undergone a contusion injury on his lateral thigh while working. He had not received any treatment at that time because he had sustained only bruises and mild discomfort that had resolved spontaneously. On physical examination, an estimate of 2 nontender, smooth, relatively fixed masses of 16 cm and 12 cm in size were palpated on the lateral aspect of the right thigh (Figure 1). They were smoothly compressed by mild pressure, then returned to their original size like a sponge on release of pressure. There were no abnormalities in the overlying skin. Infection signs such as erythema, swelling, and heating sensation were not observed. Laboratory examinations showed no abnormal findings.
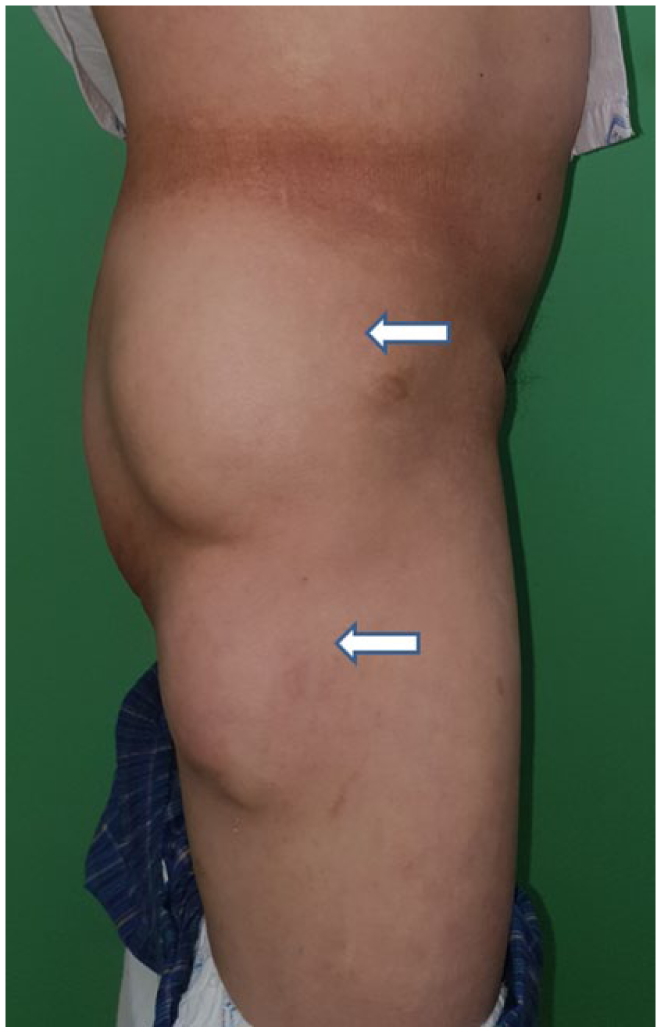
Two masses—16 cm (upper) and 12 cm (lower)—were palpated in the patient’s lateral aspect of his right thigh.
Computed tomography (CT) images revealed multiple lobulated masses with low density in the subcutaneous layer of his right lateral thigh. There were a total of 3 lobes. The lesion in the upper thigh was palpable and measured 16 cm; the other palpable lesion was in mid-thigh with a dimension of 12 cm. The last mass was too deep to palpate and measured 21 cm on its long axis in the CT images (Figure 2).

Computed tomography showed multiple lobulated, low-density masses in the subcutaneous layer abutting onto the buttock and thigh muscles. Each mass was measured as 16 cm (upper arrow), 12 cm (lower arrow), and 21 cm (arrowhead) for the deep-seated longitudinal one.
Physical findings and CT images lead to an impression of LMs. We initially recommended sclerotherapy as a first-line management option, 6 but the patient refused because of the disadvantages: it requires several weeks of treatment, there is relatively high recurrence rate, and additional surgical treatment may be needed. After thorough discussion with the patient, a total surgical resection was planned.
Under general anesthesia, the patient was placed in the left decubitus position, and a 30 cm lazy-S incision was made to the right lateral thigh to expose masses. The fascia of the lateral thigh muscles was partially excised with the mass because the floor of deep-seated one was strongly attached to it. Total excision was performed, after which fibrin sealants and several quilting sutures with bolsters 7 were applied to prevent seroma formation (Figure 3). All suction drains were removed at 5 days from the operation, bolsters at 7 days, and the patient was discharged from the hospital at 10 days. The patient recovered well without complications and recurrence was not observed for 1 year postoperatively.
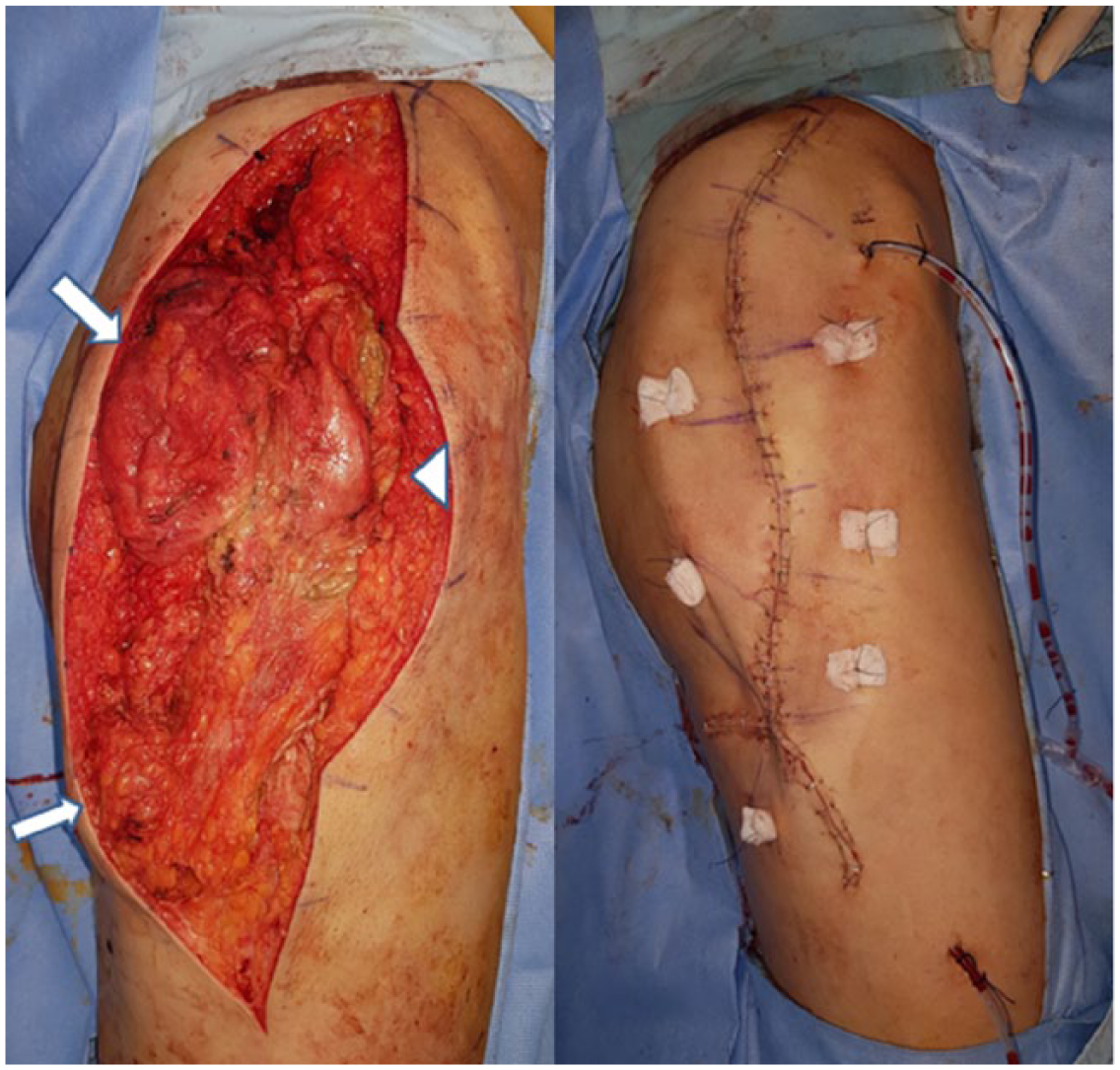
Via a lazy-S incision, all masses were exposed (2 arrows and 1 arrowhead; left). Postoperative clinical photo with suction drains and bolsters (right).
The tumors were described grossly as cystic and had solid areas that seemed to consist of hemorrhage (Figure 4). Histopathological examination of the specimens revealed thin-walled and dilated lymphatic channels with dense lymphoid aggregates and granulation. There were endothelial-lined cystic lesions containing abundant eosinophilic and proteinaceous materials. In immunohistochemistry, endothelial lineage marker CD31 was positive along the dilated lymphatic spaces. These results defined the tumor as LMs (Figure 5).
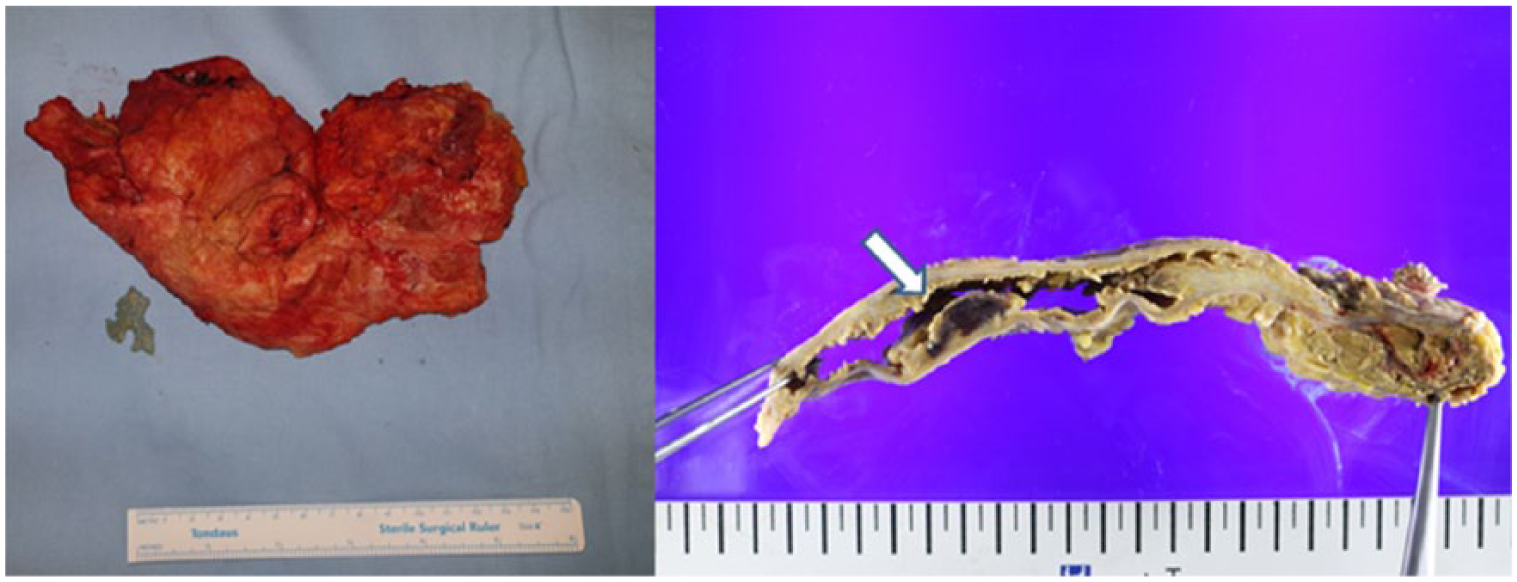
Clinical photograph of resected masses (left). Tumors were described grossly as cystic and had solid areas seemed to be hemorrhage (arrow; right).
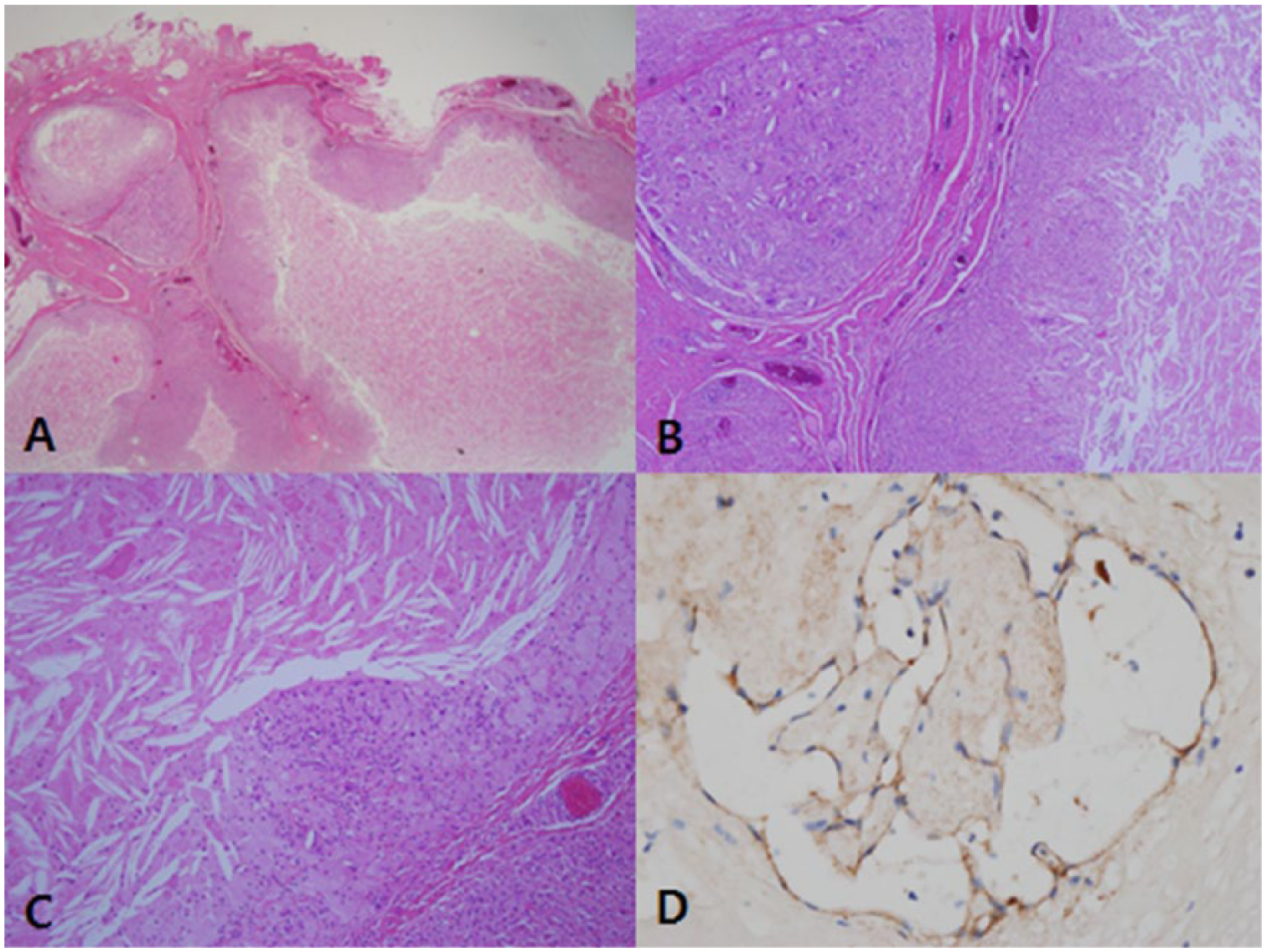
(A) Microscopic examination of specimens showing thin-walled and dilated lymphatic channels with dense lymphoid aggregates and showing granulation (hematoxylin-eosin [H&E] stain, ×10). (B and C) High-power view of specimens. There are endothelial-lined cystic lesions containing abundant eosinophilic and proteinaceous materials (H&E stain; B: ×40, C: ×100). (D) CD31 was positive in immunohistochemistry examination.
Discussion
LMs are benign vascular malformations characterized by complexes of abnormal lymphatic channels. LMs, known previously as cystic hygromas or lymphangiomas, are categorized as low-flow vascular malformations by the International Society for the Study of Vascular Anomalies classification system (1996). The pathogenesis is not fully understood but may be due to abnormal interactions between the lymphatic system and surrounding tissues via the inappropriate expression of lymphatic-specific molecules and genetic influences.8,9 Ninety percent of patients are diagnosed by 2 years of age and 95% by adolescence. Most of the lesions are located in the head and neck area. Adult-onset LMs are very rare.1,2,10 Approximately 100 cases have been reported,5,11 the vast majority found in the head and neck area. Acquired LMs presenting in the lower extremities are extremely rare and only 3 cases have been reported in the literature.3-5
The etiology of adult-onset LMs has not been well established because of their extremely low incidence and ambiguous pathogenesis, but some factors such as trauma, infection, and tumors may be causes. 10 Obstructive or proliferate disorders of lymphatic systems via unknown mechanisms would result in LMs formations. 5 Several case reports suggest local trauma as a causal factor.4,5,12-14 Trauma and the consequential increase in lymphatic substance and/or blockage of lymphatic drainage due to traumatic hematoma and subsequent fibrosis may lead to LMs.4,5 We think that the pathogenesis of LM in our patient corresponds with this theory.
Clinically, LMs are classified by the size of the malformed channels: macrocystic (volume of all loculations ⩾2 cm3), microcystic (<2 cm3), and mixed. 8 Symptoms are mainly associated with their sizes and the adjacent tissues altering structure or function. Although asymptomatic painless swelling is the main problem in most cases, bleeding and infection may be combined. 6 Various imaging techniques such as ultrasound, CT, and magnetic resonance can be helpful to diagnose, determine the types, and examine the relations to the adjacent anatomical structures.
The most effective treatment for LMs is total surgical resection while preserving adjacent anatomical vital structures. However, in cases of LMs with macrocystic/combined nature or in patients with high risk of complications related to surgery, sclerotherapy is also an available treatment option, and it may even need multiple sessions and have a high recurrence rate.6,8 Macrocystic lesions are more susceptible to surgical excision and sclerotherapy, whereas microcystic and infiltrative lesions are more prone to recurrences and complications because they are less likely to allow complete resection.
Conclusion
Adult-onset LMs are scarcely reported and lesions in lower extremities are extremely rare. Exact pathogenesis and etiology are not clearly clarified but trauma can be one of the causal factors. Sclerotherapy can be applied but total surgical resection is the treatment of choice with a low recurrence rate.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.