
Abstract
Cellulitis is one of the most misdiagnosed disease, which could be lethal when misdiagnosed. There are a lot of diseases to consider in differential diagnosis of cellulitis. Especially when conventional treatment with antibiotics does not seem to work, other radiological examinations and biopsy should be considered to find out what is causing the symptoms. Our case presents a patient with anaplastic large cell lymphoma, who was first thought to have had cellulitis but was later found to have malignancy. We aim to highlight the significance of differential diagnosis in common symptoms.
Introduction
Differential diagnosis is the key step in treatment, for it is directly related to the treatment outcome. Cellulitis is one of the most misdiagnosed diseases, and misdiagnosis can be lethal in some cases. Recently, a subtype of anaplastic large cell lymphoma (ALCL) has become an issue for its prevalence among patients with breast implants, mimicking postoperative seroma. Conversely, one of the other subtypes of ALCL is among the differential diagnoses for cellulitis. In this case, a patient was previously diagnosed as having cellulitis but was later diagnosed as having ALCL.
Case
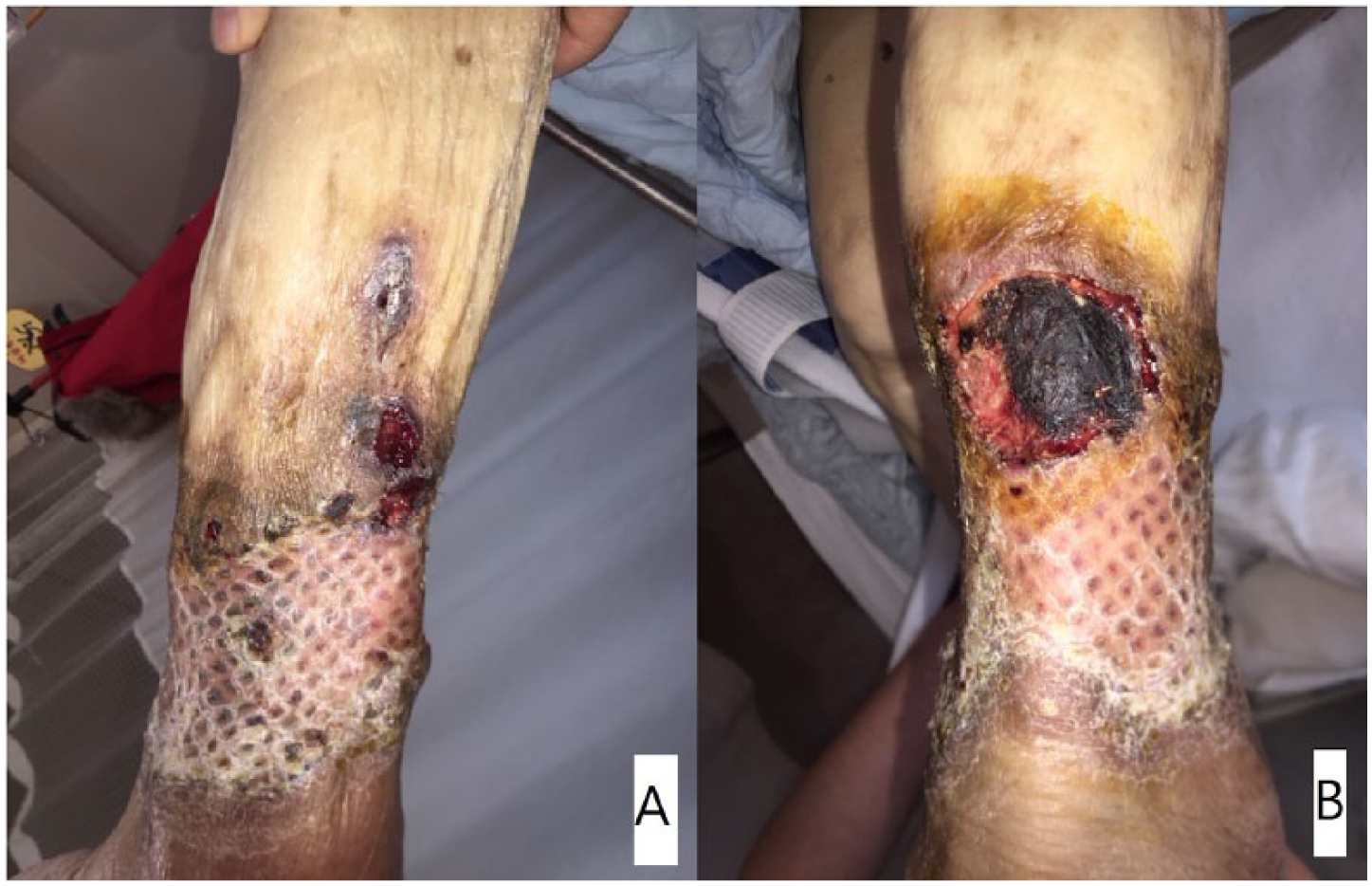
An 86-year-old female patient visited our hospital with a chief complaint of fever and a necrotic wound on her right lower leg, with eschar formation (Figure 1). The patient had fever with a body temperature of 39°C, which did not subside with over-the-counter medication, and the size of her wound increased over time. She was diagnosed as having cellulitis and was admitted to the hospital to receive intravenous antibiotic treatment and symptomatic care.

Skin lesion with eschar formation on the patient’s right lower leg.
After 2 weeks of treatment, the patient’s fever had not subsided. To eliminate the infection source and considering the possibility of necrotizing fasciitis, surgical treatment was planned for debridement of all necrotic tissue and split-thickness skin graft. The patient underwent 4 surgical debridement procedures over 2 weeks, and split-thickness skin graft was performed using skin harvested from her right thigh (Figure 2).

(A) After 4 surgical debridement. (B) Split-thickness skin graft.
The immediate postoperative results, at 2 weeks after the skin graft, showed a relatively good skin graft uptake with no raw surface (Figure 3). At 3 weeks after the operation, small skin erosions were observed on the focal graft sites. The lesion increased over time with necrotic tissue formation (Figure 4). Moreover, the patient’s fever did not subside even after the elimination of the suspicious infection source. While other possible causes were being considered, on physical examination, few small nodular skin necrosis formations (approximately 1 × 1 cm2) were found on her right thigh, similar to the one on the surgical site. The results of the skin biopsy of the nodule-like lesions were CD30-postive and anaplastic lymphoma kinase (ALK)-negative ALCL (Figure 5). In addition, under colonoscopy, shallow ulcers and erosion on the whole rectosigmoid colon was found, and the biopsy results showed ALK-negative ALCL. Thus, considering the biopsy results and symptoms, we made a diagnosis of primary systemic ALK-negative ALCL. Informed consent was received from our patient to publish her details.

Two weeks after the split-thickness skin graft.
(A) Small nodular erosions on graft site. (B) Skin lesion increased within few days.
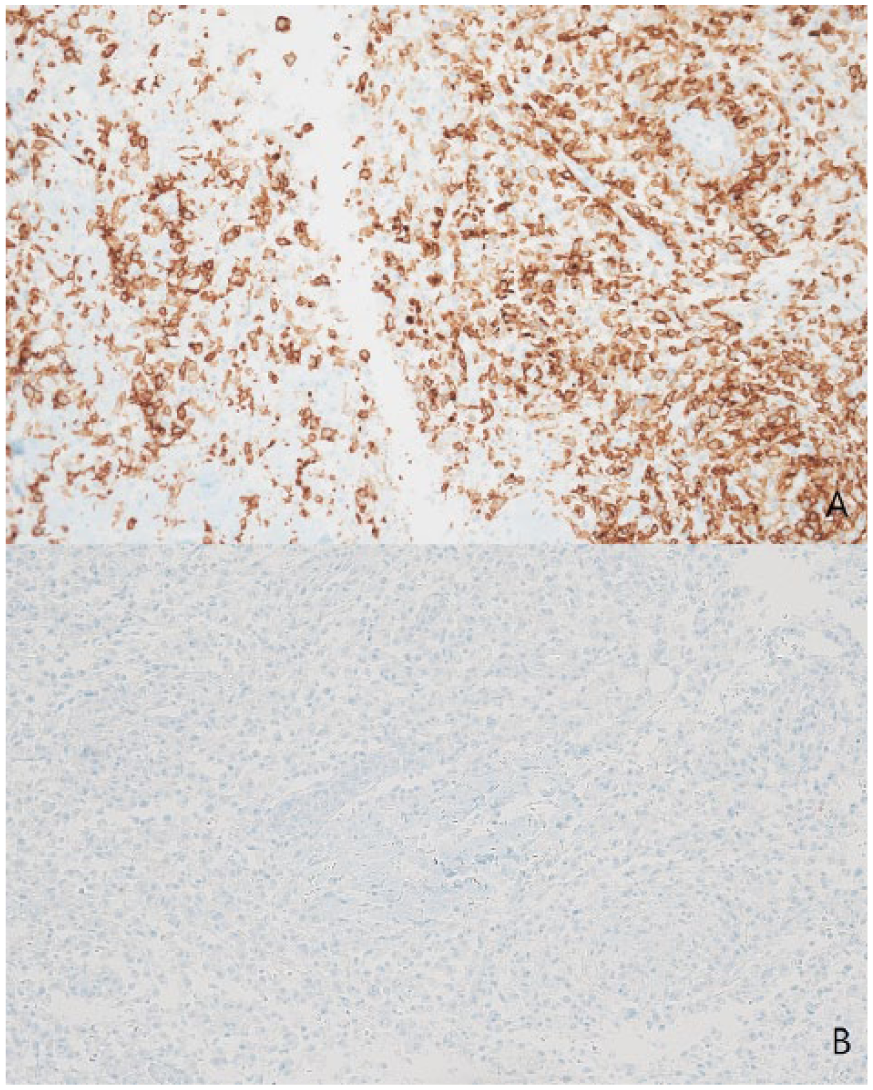
(A) The cells are positive for CD30 immunohistochemistry (immunochemistry stain ×200). (B) The cells show negativity for ALK protein immunohistochemistry (immunochemistry stain ×200).
Discussion
In the diagnosis of cellulitis, many diseases must be considered for differential diagnosis, such as deep vein thrombosis, dermatitis, thrombophlebitis, necrotizing fasciitis, drug rash, stasis ulcers, gout, malignancy, and herpes zoster. 1 One recent study revealed that 31% of patients hospitalized with cellulitis were misdiagnosed. 2 In cases of fever and skin necrosis caused by infection (cellulitis), necrotic tissue should be debrided and antibiotic treatments should be administered, but for cases where symptoms do not resolve after the conventional treatment, other possibilities should be considered.
ALCL is a T-cell non-Hodgkin lymphoma that is diagnosed on the basis of biopsy specimens positive for CD30 on the cell membrane and in the Golgi bodies. 3 ALCL has 4 subtypes, namely, primary systemic ALK-positive ALCL, primary systemic ALK-negative ALCL, primary cutaneous ALCL, and breast implant-associated ALCL. 4 The systemic ALCL subtypes usually present with enlarged lymph nodes or extranodal tumors in multiple regions of the body, such as the skin, bone, intestine, muscle, liver, or spleen. Furthermore, these 2 subtypes usually have symptoms including weight loss, fevers, and night sweats. Meanwhile, cutaneous ALCL usually presents with skin ulcers that persist and may involute and recur. 5 In addition, ALK expression is closely related to the prognosis of the disease. Gascoyne et al reported that patients with ALK-positive systemic ALCL had better prognosis, with a 79.8% 5-year survival rate, as compared with 32.9% for the patients without ALK expression. 6
Our patient had B symptoms with skin and visceral involvements of the tumor. Although a study reported that visceral metastasis of primary cutaneous ALCL occurred between 2 months and 10 years from initial diagnosis, 7 considering the B symptoms, our patient was diagnosed as having primary systemic ALK-negative ALCL. This explained the cause of the relapsing fever and recurring skin lesions. Although surgical debridement was inevitable, considering the extent of the skin necrosis, if ALCL had been diagnosed before the skin graft surgery, the lesion recurrence could have been prevented and malignancy treatment could have been started earlier. In this case, the fever and necrotic wound were misleading and indicated infection. In addition, systemic ALCL presenting with skin lesion is rare. 3
In conclusion, in patients with cellulitis-like lesions, making a conclusive diagnosis of infection could be dangerous, especially when the conventional treatment does not work. Though rare, the possibility of malignancy should be considered. Correct diagnosis is extremely important because of the completely different prognosis that follows after treatment. We strongly recommend biopsy at the beginning of the treatment of a necrotic wound. If biopsy is omitted at the beginning of the treatment, when fever and skin lesion relapse, biopsy should be performed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.