
Abstract
Comprehensive management of a severe diabetic foot infection focus on clear treatment pathways. Including rapid, radical debridement of all infection in addition to intravenous antibiotics and supportive measures. However, inexperienced surgeons can often underestimate the extent of infection, risking inadequate debridement, repeated theatre episodes, higher hospital morbidity, and hospital length of stay (LOS). This study aims to assess protocolized diabetic-foot-debridement: Red-Amber-Green (RAG) model as part of a value-based driven intervention. The model highlights necrotic/infected tissue (red-zone, nonviable), followed by areas of moderate damage (amber-zone), healthy tissue (green-zone, viable). Sequential training of orthopedic surgeons supporting our emergency service was undertaken prior to introduction. We compared outcomes before/after RAG introduction (pre-RAG, n = 48; post- RAG, n = 35). Outcomes measured included: impact on number of debridement/individual admission, percentage of individuals requiring multiple debridement, and length-of-hospital-stay as a function-of-cost. All-patients fulfilled grade 2/3, stage-B, of the Texas-Wound-Classification. Those with evidence of ischemia were excluded. The pre-RAG-group were younger (53.8 ± 11.0 years vs 60.3 ± 9.2 years, P = .01); otherwise the 2-groups were matched: HbA1c, white blood cell count, and C-reactive protein. The post-RAG-group underwent significantly lower numbers of debridement’s (1.1 ± 0.3 vs 1.5 ± 0.6/individual admission, P = .003); equired fewer visits to theatre (8.6% vs 38%, P = .003), their LOS was reduced (median LOS pre-RAG 36.0 vs post-RAG 21.5 days, P = .02). RAG facilitates infection clearance, fewer theatre-episodes, and shorter LOS. This protocolized-management-tools in acute severely infected diabetic foot infection offers benefits to patients and health-care-gain.
Diabetes foot ulceration is common, complex to manage, and can cause significant morbidity. 1 The lifetime risk of a diabetes foot ulceration is between 19% and 34%, and approximately 50% to 60% develop secondary infection leading to a “foot attack.” 2 In the United Kingdom, foot complications are the most common cause of diabetes-related hospitalization with similar trends noted in other countries. 3 Many of such admissions are precipitated by ulceration complicated by infection. More recently, the term “diabetic foot attack” has been suggested to emphasize the urgency of the situation and need for interventions of rapid infection control without which there is a significant risk of nonhealing and amputation. 4
Despite the otherwise visual nature of a diabetic foot attack, recognition of the severity and extent of infection can often be challenging. While initial management includes appropriate intravenous antibiotic therapy and optimization of medical comorbidities, early surgical debridement and excision of all infected, nonviable tissue plays a pivotal role in controlling infection and arresting the spread of tissue destruction. 5
However, the inexperienced surgeon who is at the forefront of emergency service delivery can often underestimate the extent of infection. This can lead to a wide variation in the quality of emergency surgery or in this case foot debridement. Furthermore, the balance of excising enough damaged and infected tissue to minimize ongoing infection against overzealous debridement of healthy margins is a challenge for surgeons in general, and in particular, for those with limited experience in diabetic foot surgery. Furthermore, observational studies suggest higher rates of perioperative and postoperative complications in diabetes. 6 Thus, appropriate early, precise surgical debridement to avoid iatrogenic insult by minimizing the number of theater episodes is also highly desirable.
In a trauma center such as ours, multiple “emergency” teams including orthopedic surgeons with a varying degree of experience in diabetic foot infection surgery are involved. An internal audit demonstrated a higher than anticipated return to theater rate. Furthermore, the hospital length of stay (LOS) in such patients was found to be significantly higher than desirable for such patients. The audit also highlighted a significant intersurgeon variability in the quality of debridement surgery, which was felt to be an important factor contributing to the above-mentioned findings. These findings coincided with an expansion within the orthopedic department, which had led to an increasing number of different surgeons undertaking diabetic foot surgery.
Our aim, therefore, was to establish a practical and protocolized surgical algorithm for diabetic foot infection and determine if this facilitated an improvement in the core metrics of hospital outcomes.
Methods
All patients admitted to King’s College Hospital from the emergency department or the Diabetic Foot Clinic for the management of a severe diabetic foot infection with Texas Wound Classification B2 or B3 grades were included. All patients were assessed by the diabetic foot team comprising a diabetologist, orthopedic and vascular surgeon, and inpatient podiatrist prior to surgery. Those with peripheral arterial disease were excluded from analysis, and thus the overall cohort was representative of a neuropathic severe diabetic foot infection.
As a baseline, we recorded patient demographic and recognized comorbidities at the time of surgery including white blood cell count (WBC), C-reactive protein (CRP), and glycated hemoglobin (HbA1c) and also comorbidities at the time of admission associated with diabetes including ischemic heart disease (previous history of coronary artery bypass graft, cardiac catheterization, medical therapy), nephropathy (chronic kidney disease [CKD] 3+), and retinopathy. Surgical parameters included number of debridements required, number of further debridements within 14 days of the first index surgical procedure, and hospital LOS. All patients followed our standard management protocol for severe diabetic foot infections. Following surgical debridement, patients received multidisciplinary review including bedside wound toilet, negative pressure therapy when indicated, and medical management until stable granulation tissue was achieved.
A prospective audit period began with an initial review of patient outcomes from October 2013 to April 2014 (pre-RAG [Red, Amber, Green] period). Following this, the orthopedic and diabetic foot units undertook training of a protocolized surgical debridement tool with RAG. The follow-up review of outcomes after initiation of the Traffic Light Protocol of diabetic foot debridement (RAG, post-RAG) was from May 2014 to November 2014. The review was conducted as a service improvement project and was carried out in accordance with local governance policy and registered with our governance committee as an audit and deemed not to require ethics committee approval.
In total, 83 consecutive cases between October 2013 and November 2014 met the inclusion criteria of a diabetic foot with severe infection requiring surgical debridement being minimum grade B2 or B3 using the Texas Wound Classification System. In the pre-RAG group, 48 cases of nonstandardized debridement were identified. Following training and implementation of the standardized RAG model, 35 suitable cases were identified.
Traffic Light Training and Protocol
Once the results of the pre-RAG period were released, a decision was taken to develop a program of education aimed at rationalizing the surgical process and following a value-based agenda to improve patient outcomes. This process involved targeting areas of the process and pathway that could be better utilized. We promoted and prospectively educated all surgeons in our unit, through education days, audit meeting, regular case-based discussion, and training to use a Traffic Light RAG model of debridement (see Figure 1). Training started in May 2014, and newer recruits were additionally trained in the process before taking up their emergency work schedules.
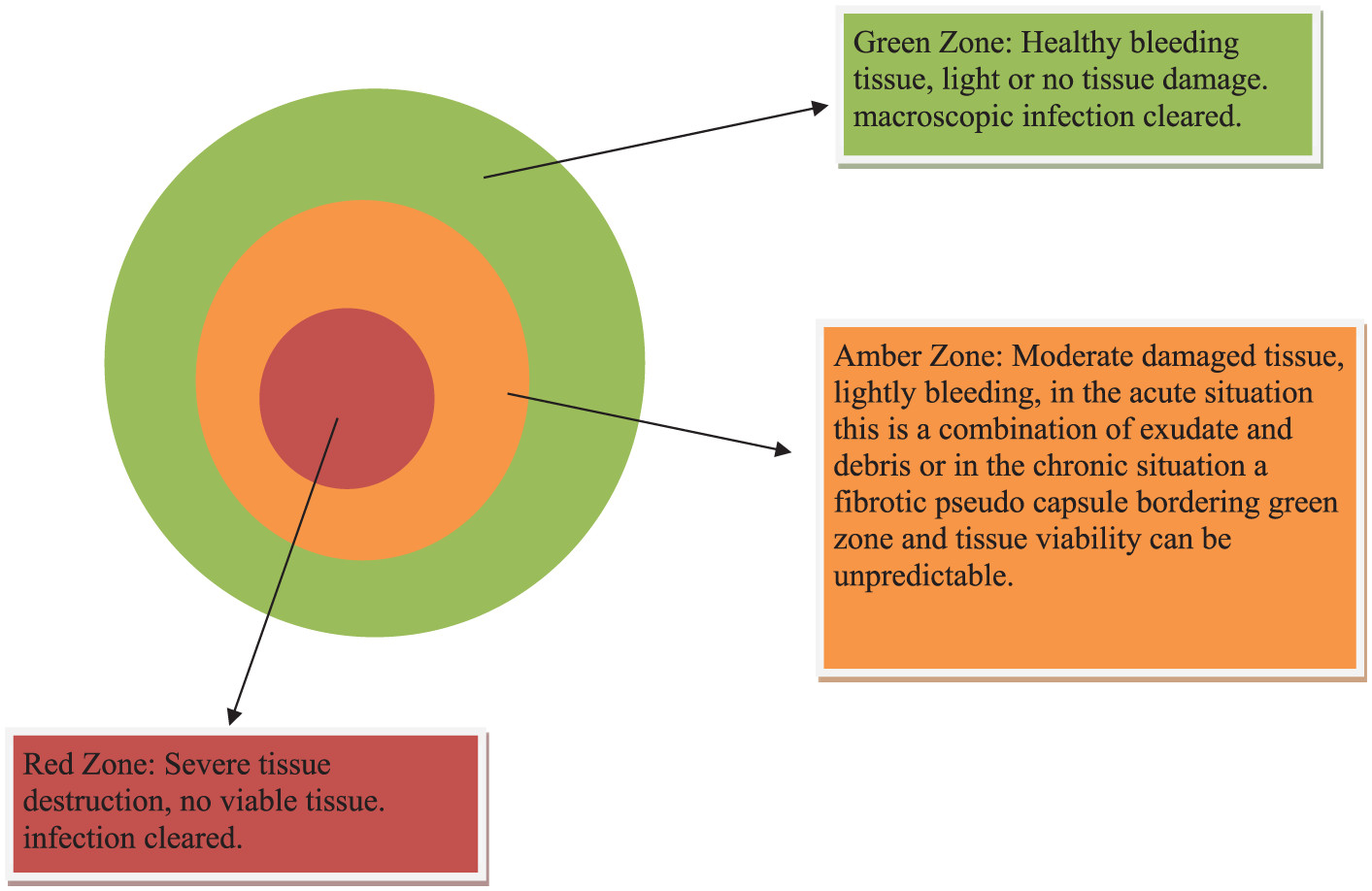
Definition of zones of clearance: red zone of dead necrotic tissue and amber zone of moderate damage where the tissue viability is unpredictable and green zone of healthy bleeding tissue. The zones are defined prior to surgery and confirmed during surgical dissection.
Protocol
The RAG model can be viewed similarly to that of Enneking et al’s guide for tumor resection, whereby a healthy margin is excised to ensure complete eradication. 7 Cuzzell previously described a color for wound healing. 8 However, the RAG model defines areas of debridement rather than possible healing as described by Cuzzell. In our model, we aim to create epithelialization and granulation tissue.
The RAG model employs a combination of clinical and when necessary radiological assessment to mark out necrotic/infected tissue (red zone), followed by the area of moderately damaged tissue that is likely to be colonized with infecting bacteria (amber) and then healthy tissue (green; see Figures 1 and 2 for examples).

Use of the RAG tool on the skin to assess the possible area of debridement - concentric circles suggest the extent of debridement required. combining this with radiological imaging can also help trainees understand the 3 dimensional extent of the RAG zones.
The depth of soft tissue and bone resection is undertaken and correlated with radiographic and imaging modalities such as plain radiography and/or magnetic resonance imaging (MRI) that demarcate the extent of tissue destruction. For example, radiographs showing the extent of gas spreading with soft tissue and T1/2 weighted MRI images showing abnormal fluid and cortical bone destruction, thus allowing the extent of minimum resection and limits of exploration to be ascertained prior to entering the operating room to clear all unhealthy margins.
Prior to surgery, procedure planning and surgical incision marking training were performed initially with a senior surgeon present to encompass the green zone within an elliptical incision.
The red and amber zones were completely excised, extending into healthy, noninfected, outer bleeding edges of the green zone with good potential for healing. We continued to take deep tissue specimens, as they are obtained aseptically at surgery, and thus usually contain only the true pathogens, while cultures of superficial lesions often yield contaminants.9,10
Elliptical incisions are preferred in our unit where possible to facilitate apposition and accommodate negative pressure wound therapy once the debulking and debridement of dead tissue has been completed. This facilitates continued bedside wound management and supplementary soft tissue debridement when necessary. 11
During this training period, all surgeons undertaking such work were given the opportunity to review a presentation outlining the RAG model and were encouraged follow-up of the patient with clinical assessment of patient’s postsurgical outcome with one of the diabetic foot surgeons. Surgeons were divided into the following groups depending on their experience:
Consultant Orthopedic Surgeon: completion of training
Senior Trainee Orthopedic Surgeon: between 3 and 6 years specialty training
Trainee Orthopedic Surgeon: less than 3 years specialty training
The RAG model was put into routine practice from July 2014 for all of our patients when the same prospective demographic and outcome measures were recorded and reviewed independent of the surgical team (AS and SS).
Statistical Analysis
Comparisons between group characteristics were made using a t test, and subsequent analysis of outcomes was made with a 2-tailed test, for example, number of debridements per infection episode and length of hospital stay per infection episode. Analysis was conducted using SPSS (v17) for personal computers. Statistical significance was defined as a P value of <.05.
The relative risk (RR) was calculated to assess the significance of the differences in our primary clinical outcome, the risk of multiple further surgical debridements with 14 days of primary debridement between those treated with the RAG tool and those not treated with the RAG tool.
Results
Patients and Demographics
Pre-RAG
From the 48 patients identified in this group, median age was 53.7 ± 10.9 years, while the mean WBC was 11.56 × 109L ± 3.85, CRP 115.6 ± 74.9 mg/L, and HbA1c 9.42 ± 2.1 mmol/L (see Table 1). The majority of patients were male (86%). In all, 15/48 (31%) had history of ischemic heart disease (composite of angina, myocardial infarction, and cardiac failure), 16/48 (33%) had laser-treated retinopathy, and 10/48 (21%) had CKD stage 3 or higher.
Comparison of Demographics and Inflammatory Markers on Admission (±SD) a .

Abbreviations: RAG, Red, Amber, Green; WBC, white blood cell count; CRP, C-reactive protein; HbA1c, glycated hemoglobin; CKD, chronic kidney disease.
Age was statistically increased in the second group, but no other biological factors were significantly different. We observed that the CRP is slightly higher in the second group, which could be indicative of higher infection loads, but the HbA1c is comparable.
Post-RAG
Within these 35 patients, the median age was 59.2 ± 9.1 years, the mean WBC was 10.86 ± 3.89 × 109L, the CRP was 134.0 ± 99.7 mg/L, and HbA1c was 9.33 ± 2.34 mmol/L. The majority of patients were male (88.9%). Again, 14/35 (40%) had ischemic heart disease, 11/35 (31%) had laser-treated retinopathy, and 9/35 (26%) had CKD stage 3 or higher. The differences in age on admission were found to be statistically different (P = .035), while WBC, CRP, and HbA1c on admission were found to be not statistically significant (see Table 1).
Surgical Results and Outcomes
Surgeon Composition
Pre-RAG
Within this group, the surgery was conducted by a number of surgeons of different grade with varying diabetic foot experience. In 52.1% (25/48) cases, the primary surgeon was an orthopedic trainee (ie, a non-consultant grade surgeon). In addition, 64.6% (31/48) was conducted by an orthopedic trainee who had not worked within the diabetic foot team. In 70.8% (34/48) cases, a consultant-level surgeon was in attendance or scrubbed to supervise cases.
Post-RAG
Surgery was conducted primarily by orthopedic trainees or surgeons not associated within the diabetic foot team whom had been trained with the RAG model of sequential debridement of the zones of tissue injury. Orthopedic trainees conducted 52.7% (19/35) of debridement, and 71.4% (25/35) were not working with or had directly worked with the diabetic foot team. Further analysis revealed that theater supervision by a consultant-level surgeon was seen in 82.8% (29/35), and each trainee conducted a mean of 2.3 (mode 3) debridements after the RAG training.
Operative Outcome
The post-RAG group underwent a significantly lower number of debridement surgeries than the pre-RAG group (1.1 ± 0.3 vs 1.5 ± 0.6/individual admission, P = .003).
Pre-RAG
We observed in the pre-RAG group that 18 of the 48 patients (38%) required a further theater surgical debridement. Of these, 10/18 required repeat debridements within the initial 7 days of the index procedure. The reasons for returning to theater included no progression in wound healing 33.3% (6/18), ongoing serous or purulent fluid discharge with ongoing necrosis 22.2% (4/18), and further radiological investigation demonstrating collections and/or progressive bony change.
Post-RAG
Only 3 patients (8.6%; 3/35) returned to theater for further debridement. None required doing so within the first 7 days. Thus, the RR of further surgery was reduced to 0.2, that is, a 5-fold risk reduction (P = .003).
Hospital Length of Stay
The hospital LOS was significantly reduced before and after intervention with median LOS pre-RAG 36.0 (interquartile range = 47) days versus post-RAG median of 21.5 (interquartile range = 22.5) days, P = .02 (Figure 3 and Table 2).
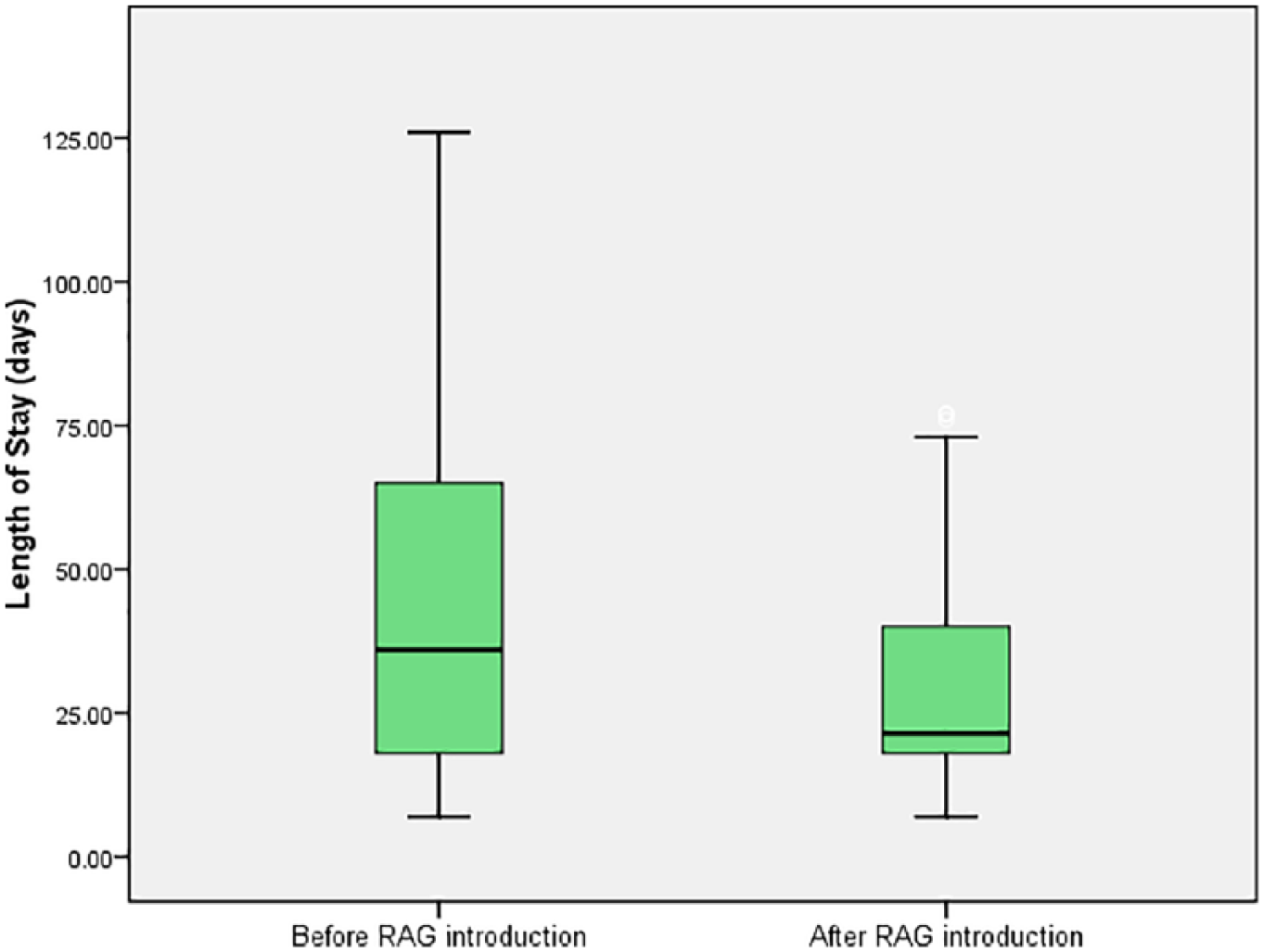
Difference in length of stay after the introduction of the RAG tool. Initial LOS was a median of 36 days and reduced to a median of 21 days after the introduction of the RAG tool (P<0.02).
Assessment of Outcomes a .
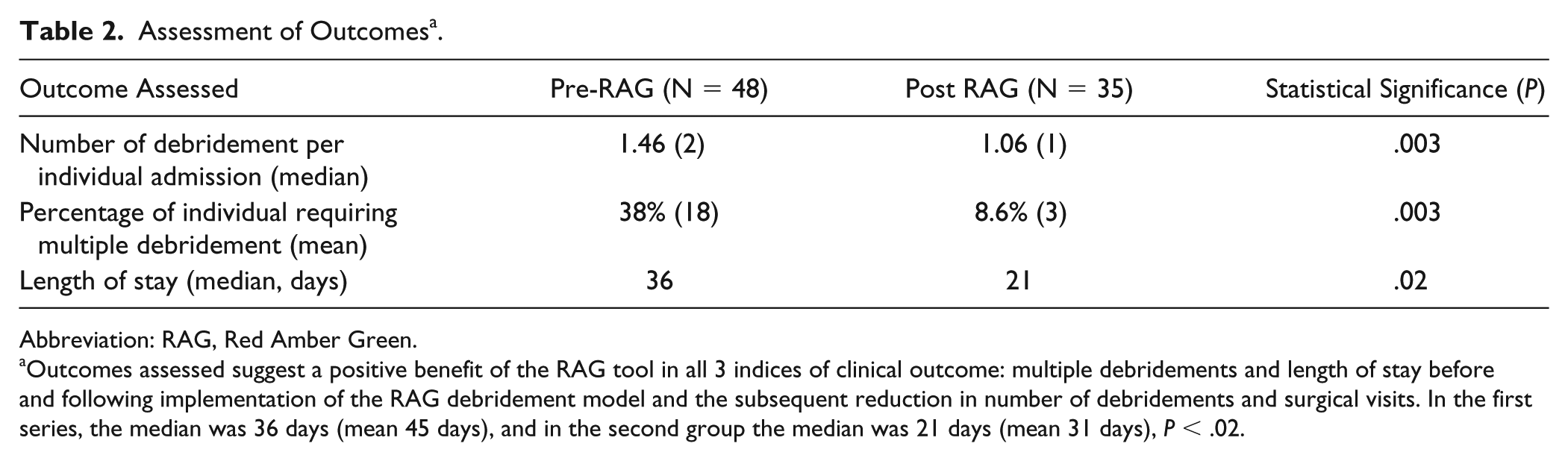
Abbreviation: RAG, Red Amber Green.
Outcomes assessed suggest a positive benefit of the RAG tool in all 3 indices of clinical outcome: multiple debridements and length of stay before and following implementation of the RAG debridement model and the subsequent reduction in number of debridements and surgical visits. In the first series, the median was 36 days (mean 45 days), and in the second group the median was 21 days (mean 31 days), P < .02.
Cost Analysis
To calculate the cost of the hospital episode per patient, we applied Department of Health and National Institute for Health and Care Excellence (NICE) costings to our findings (NG 27, NICE, 2017). 12 At this time, the cost of a generic National Health Service (NHS) bed varied from £222 to £400.00 per day (figures from the Department of Health and NICE for the NHS). This is indicative of a minimum possible saving of £3300 per patient depending on the reimbursement model used by the health care system.
Furthermore, using the time-driven activity-based costing to calculate the price of an individual surgical episode, we found that the mean procedural time was 66.6 minutes (n = 83) and approximated to 60 minutes. Noting that the average cost of running our theater complex was £636 per hour, 13 the relative cost saving in reduced theater time was £255 (£929 vs £674) per patient due to lower numbers of surgical episodes in the post-RAG group (1.1 ± 0.3 vs 1.5 ± 0.6 per individual admission, P = .003).
Discussion
Treatment of the acutely infected diabetic foot or foot attack requires a multidisciplinary approach.14,15 Limb salvage protocols for such individuals include early aggressive surgical debridement. 16 Adequate debridement is pivotal in reducing the infective load, disrupting the antimicrobial-resistant biofilm, and allowing deep sampling, which are required to guide successful antimicrobial therapy.17-19
The RAG tool follows established surgical principles in order to clear infection. We demonstrate that a simple consistent approach using the RAG tool with a clearly delivered education program leads to a significant reduction in the number of attempts required to achieve infection control.
The simplistic tool identified the area of infection and graded local tissue damage, which led to the standardization of surgical practice. In addition, this enabled a 5-fold reduction in the RR of further early debridement for infection control and return to theater within the first 35 patients went that statistical significance was achieved and a change of policy was instituted. The tool utilizes the combination of clinical signs and radiological changes to unmask the extent of infection. For instance, the observation of superficial spreading cellulitis can be unmasked on radiographs with gas within the soft tissues or more consistently on MRI as tendon sheath infection. Furthermore, bony changes can be identified consistent with osteomyelitis and dealt with in the appropriate manner, allowing amber and green zones to be identified and provide preoperative surgical plan.
Trainees and orthopedic surgeons who do not routinely treat diabetic feet alike were thus given a framework to prepare for surgery allowing them to have confidence in theater and establish a process of debridement and treat the surgery in a similar manner to tumor excision. Discussion and review with senior foot team surgeons allowed them to assess and understand the extent of debridement required.
A period of 3 months was required for transformation and introduction of such a structured program of education with ongoing mentoring. At our institution, all trainees are supervised by a senior consultant–level surgeon. The number of debridements conducted with an identified member of the diabetic foot surgical team was less than 30% of cases as RAG training was administered outside the operating room. However, this resulted in a sustainable and statistically significant change that validated the training program, which has now become a departmental policy.
Our prime objective, to reduce unnecessary surgical episodes, was achieved as the number of debridements was reduced to a mean of 1 per admission episode. This is important in a group of patients who have complex comorbidities in whom multiple theater episodes may confer additional perioperative risks such as anesthetic-related complications (eg, myocardial infarction) and decompensating established medical comorbidities.20,21
Our approach using RAG tool offers a value-based health care approach to benefit core hospital metrics, such as LOS, and offers benefits from various perspectives to the patient, for example, faster return to home, possible reduction in adverse events associated with prolonged hospitalization, and medical treatment such as anesthesia. The economic benefit in our health care setting relates to a reduction in provider cost compared with our standard reimbursement and a marginal gain13,22 and identifies with the concepts in transition between inpatient hospital settings and community care for adults’ NICE guideline [NG27]. 23
Our cost analysis suggests that there are possibilities of significant potential cost savings, while avoiding the perils of additional surgery and represents a value-based care-driven improvement. However, one would need to balance the cost of additional outpatient treatment to gain a more accurate picture of the actual finite cost saving, but the benefit offered to “hospital flow” is extremely important.
Limitations
Even so, our study supports the notion that the LOS in a diabetic foot surgical patient is a product of the adequacy of initial debridement. However, in a real-world environment, additional factors are likely to play pivotal roles such as the response to systemic antimicrobial therapy, prior out of hospital management, quality of postoperative wound care, access to multidisciplinary support, in addition to patient factors such as comorbidities, and, very important, social factors.
Furthermore, we are not sure if ischemic patients (eg, Texas grade 2/3 and C/D ulcers) would derive the same benefit. These confounding factors need to be further assessed to define the contribution of each in length of patient stay during the acute foot attack.
The RAG framework may shorten the time to surgical competency, as part of a training program in surgical diabetic foot debridement. We believe further analysis is required to assess how surgical competency is reached, for example, how many supervised debridement procedures are needed for a trainee to become self-sufficient. This in itself requires a program of procedure-based assessment for competency, which is beyond the scope of this article, requiring intraoperative assessment and a controlled trial to validate its significance but could lead to universal acceptance.
We have demonstrated that adopting the Traffic Light Model (RAG) improves efficacy of initial surgical debridement, especially as 50% of such surgeries are primarily conducted by surgeons in training. Trainees have been shown here to respond to protocolized surgical algorithm in debridement.
High-quality initial debridement has the benefit of superior infection clearance and reduction in number of theater episodes, avoiding multiple anesthetics, and the additional cost of a prolonged LOS and follows a value-based agenda in improving patient outcome and lowering cost margins.
Supporting this methodology as a standard process simplifies the procedure for the inexperienced trainee or unfamiliar surgeon, empowering them to successfully manage the acute foot attack definitively.
We propose that every unit providing care for the acutely infected neuropathic patients with preserved vascular supply should consider adopting such a model for treating them.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.