
Abstract
This study investigated cognitive functioning and understanding of peripheral neuropathy in a cohort of individuals with diabetes-related foot ulcers requiring hospitalization. The aim was to examine the association between cognition, understanding of peripheral neuropathy, and diabetic health variables. Thirty inpatients referred to the Diabetic Foot Unit Clinical Psychology service, at the Royal Melbourne hospital, were assessed using the Montreal Cognitive Assessment (MoCA) and the Patient Interpretation of Neuropathy (PIN) questionnaire. Relevant demographic and medical information was collected. In this predominantly middle-aged, male cohort, the average MoCA score (22.37, SD = 3.65) fell below the general population age-matched mean, and a quarter of the MoCA patient scores were consistent with those seen in early dementia samples (<20). There appeared to be several misperceptions regarding peripheral neuropathy, less accurate attributions of blame to self or practitioners, and more accurate attributions of control of ulcer management to practitioners. Correlation analysis indicated that individuals with stronger MoCA scores tended to provide more accurate answers on the Acute Foot Ulcer Onset PIN scale. Individuals with diabetes-related foot ulcers requiring hospitalization demonstrate reduced cognitive functioning and this may affect their understanding of peripheral neuropathy, particularly information regarding foot ulcer onset. Routine screening of cognitive functioning in this cohort may be useful so that health education and care management can be adjusted according to individual patients’ cognitive capabilities.
Introduction
Diabetes-related foot ulcers are associated with significant morbidity and mortality, and significantly increase an individual’s risk of requiring a lower limb amputation, greatly increasing the burden of illness imposed on an individual. 1 Recent evidence-based guidelines for the management of diabetes-related foot disease emphasize that effective self-management is key to positive outcomes. 2 However, difficulties with the adherence to diabetes-related foot ulcer treatment and management recommendations in this patient group are well recognized. 3 To address this, efforts have been made from a medical perspective to implement comprehensive programs for the prevention and management of diabetes-related foot complications. 4 Conversely, the psychological factors that may have an impact on diabetes-related foot wound management have received little attention, and have only recently been recognized as a potentially important determinant of outcomes. 5
The chronic disease literature, in both diabetes and cardiac care, has identified multiple, interlinked factors that modulate individual differences in effective disease self-management, including, demographic factors (such as socioeconomic status, race, age, and educational level), disease knowledge and experience, cognitive functioning (attention, memory, and executive functioning), personality factors, self-efficacy, and psychological well-being.6-9 However, these potential modulating factors are underresearched and not yet well understood in individuals with diabetes-related foot complications.
In general cohorts of individuals with diabetes, variable findings have been reported about rates of cognitive impairment relative to controls. The trend is indicative of neurocognitive dysfunction, most commonly in the areas of verbal memory and executive functioning.10-13 Few studies have specifically examined cognition in diabetes, relative to the presence of foot ulcers. When this has been examined, individuals with foot ulcers had similar estimated premorbid cognitive functioning scores, but were found to have lower cognitive test scores in all tested neurocognitive domains (global cognitive scores, memory, attention and concentration, reaction time, executive function, psychomotor, and verbal fluency). 14 Interestingly, cognitive function has not been found to be predictive for re-ulceration at 12-month follow-up. 15 Based on the small amount of existing research in this area, it is possible that neurocognitive dysfunction in individuals with diabetes-related foot ulcers may contribute to difficulties with treatment adherence and self-management in this cohort. 14
A second important area that may relate to treatment adherence and self-management is an individual’s core beliefs and assumptions about their condition. Preliminary research has been conducted in this area in individuals with diabetes and peripheral neuropathy who were at high risk for developing foot ulcers.16-18 Utilizing the Patients’ Interpretation of Neuropathy questionnaire, 3 clusters of participants have been identified in this patient group with distinct illness schemata.17,18 The first cluster had higher rates of misperceptions about the nature of peripheral neuropathy; the second was described as generally more realistic about the nature of their condition; while the third cluster was uncertain about their condition. Importantly, the misperceptions cluster was found to participate in a higher rate of potentially damaging foot-care behaviors than individuals in the other clusters. 18
Improved understanding of the factors that may modulate self-management could be translated into more effective care and management for individuals, as well as improved education initiatives. Gaining an understanding of an individual’s cognitive level and perception of their conditions may assist clinicians to develop and individualize interventions and ultimately improve the efficacy of foot wound management. The current study sought to characterize the cognitive functioning and understanding of neuropathy in individuals with diabetes and foot ulcers requiring an inpatient admission, and to investigate the association between these factors.
Methods
Population and Selection
A convenience sample of 30 inpatients from the Diabetic Foot Unit (DFU) at the [Royal Melbourne Hospital, Australia] receiving inpatient intervention and management of serious foot wounds were recruited to this study. All DFU inpatients receive an initial session with the unit psychologist (who administered the measures for the study), with a proportion then going on to receive further psychological support or intervention. All participants had a diagnosis of diabetes, diabetes-related complications of peripheral neuropathy (as diagnosed using a 10 g Semmes-Weinstein monofilament), severe foot wound requiring an inpatient admission, and were able to speak English. One of the 30 participants was admitted for management of their first ever foot wound and all other individuals had experienced previous diabetes-related foot ulcers. Excluded from the study were individuals with a preexisting psychiatric diagnosis that would preclude them from participating in the cognitive and health belief assessment measures. In addition, individuals presenting with significant distress relating to their medical admission and treatment were also excluded. Inpatients meeting the inclusion criteria were individually assessed at their bedside, during their hospital admission, by the treating Clinical Psychologist. The study was approved by the [Melbourne Health Service] Human Research Ethics Committee (Project Number QA2016152).
Materials
Detailed demographic and medical information was collected from the participant’s health records. Each participant was administered a cognitive screening assessment and an understanding of neuropathy questionnaire.
Demographic and Medical Information
Demographic information, including sex, age, level of education, and relationship status, was collected from participants. Medical data pertaining to microvascular (retinopathy, neuropathy, and chronic kidney disease) and macrovascular (myocardial infarction, ischemic heart disease, and peripheral arterial disease) disease complications were taken from medical records. In addition, diabetes diagnosis (type 1 or 2), date since diagnosis, and glycosylated hemoglobin (HbA1c) levels measured during the inpatient admission were taken from the medical records for each participant.
Cognitive Functioning
Cognitive functioning was assessed using the Montreal Cognitive Assessment (MoCA), a screening tool for detecting mild cognitive impairment. The MoCA has high internal consistency (Cronbach’s α = 0.83), test-retest reliability (r = 0.92), and concurrent validity (r = 0.87). This screening tool provides a brief measure of memory, attention, executive functions, language, and visuospatial abilities. 19 This measure was chosen due to its brevity, common use in the hospital setting, and measure of domains of cognition that have been reported as impacted in previous studies on cognition in the diabetes-related foot complication population.
Understanding of Peripheral Neuropathy
Participants completed a 39-item self-report questionnaire, the Patient Interpretation of Neuropathy (PIN). The PIN has been shown to be a valid and reliable questionnaire that examines the condition-specific personal beliefs of a person with diabetes-related peripheral neuropathy. The PIN assesses 9 cognitive subscales across 5 domains identified by the Common Sense Model of Illness (identity, cause, time-line, controllability, and consequences). 19 There are also 2 emotional subscales (worry about consequences and anger at health professionals) that represent the emotional domain. 16 The PIN attempts to elicit how individuals interpret their peripheral neuropathy, respond emotionally, and make decisions to engage in foot self-care. 16 The PIN uses a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree). Items 10 and 19 of the PIN (“I could develop a foot ulcer without feeling any pain” and “Foot ulcers take a long time to develop”) are reverse scored.
Statistical Analyses
Descriptive statistics of the demographic and medical variables were calculated, as well as the mean and standard deviation of the total and domain-specific MoCA scores. The PIN items were summated into composite scores for each of the 11 PIN factors, and an average score for each subject’s composite score calculated. Correlation coefficients were calculated between the total MoCA score and each of the 11 interpretation of neuropathy factors of the PIN. In addition, the correlation between cognitive functioning on the MoCA, HbA1c, and length of time since diabetes diagnosis was calculated.
Results
Demographic Variables
The demographic variables (Table 1) indicate a mostly male, middle-aged, cohort of individuals with around 12 years of education. The majority of participants (93.33%) had type 2 diabetes mellitus (T2DM). The average length of diabetes diagnosis was 10 years with a large range between 1 and 38 years. For 2 participants, the number of years since diagnosis was not available. The mean HbA1c was 9.3%. All participants had peripheral neuropathy, microvascular complications included 23.33% of patients with retinopathy and 26.67% with nephropathy, and 60% had macrovascular disease. The sample included 53.33% with neuroischemic wounds and 46.67% with neuropathic wounds. Wound locations were 56.67% toes, 30.00% planter midfoot, 10.00% heel, and 3.33% dorsal foot.
Demographic and Medical Variables.
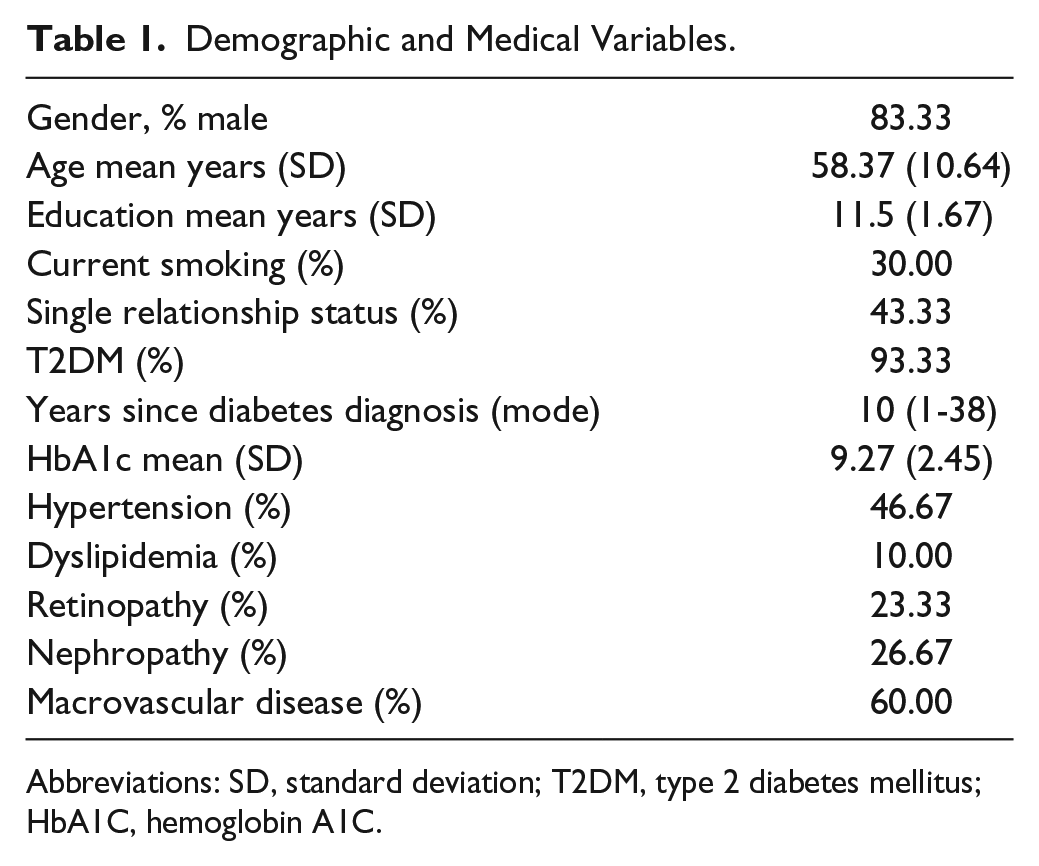
Abbreviations: SD, standard deviation; T2DM, type 2 diabetes mellitus; HbA1C, hemoglobin A1C.
Cognitive Functioning Results
The results indicate an education-corrected mean total MoCA score of 22.37 (SD = 3.65), with no participants obtaining a full 30/30 score (Table 2). Overall, 86.67% of participant total scores fell below the MoCA cutoff score of 27, and just under half (43.33%) of participant total scores fell below the MoCA cutoff score of 23. The mean scores in the domains of recall, executive functioning, and language were the most consistently reduced, with 90% of participants not obtaining a full score for memory recall, 86.67% not obtaining a full score on the executive functioning domain, and 76.67% of participants not obtaining full scores on the language domain. The strongest domain performances were seen in the areas of orientation, naming, and abstraction, with 10% of participants not obtaining full scores on orientation, 23.33% of participants not obtaining full scores on the naming domain, and 36.67% of participants not obtaining full scores on the abstraction domain. About half of the participants (53.33%) did not obtain full scores on the attention domain.
Results of Cognitive Functioning as Assessed With the MoCA.
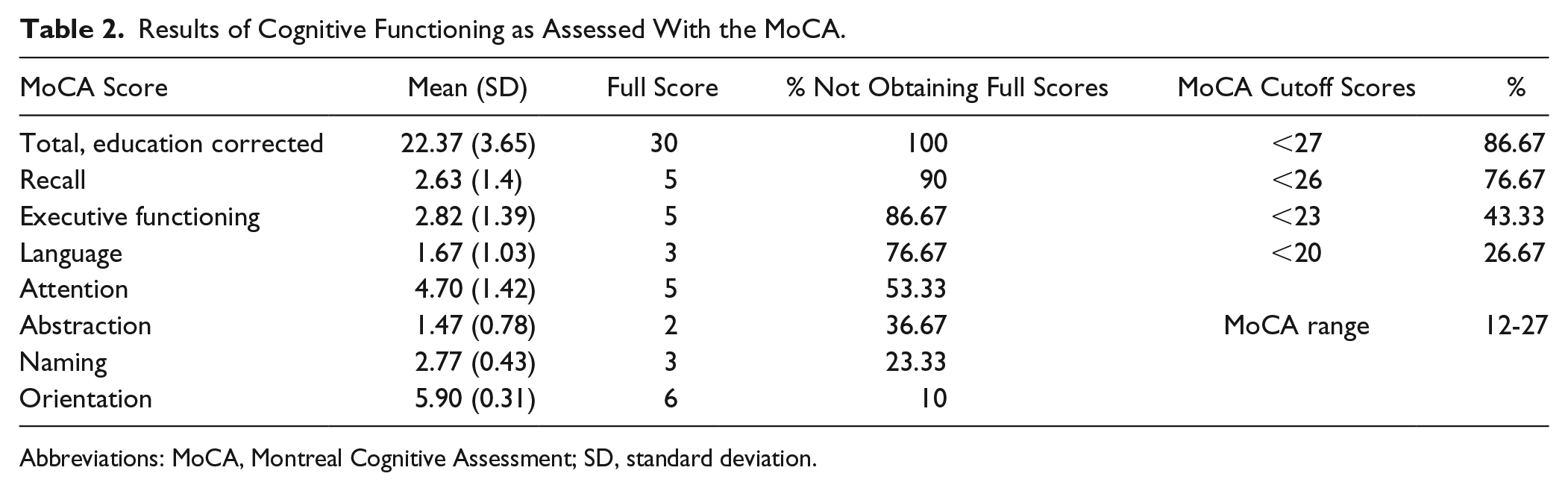
Abbreviations: MoCA, Montreal Cognitive Assessment; SD, standard deviation.
Understanding of Neuropathy Results
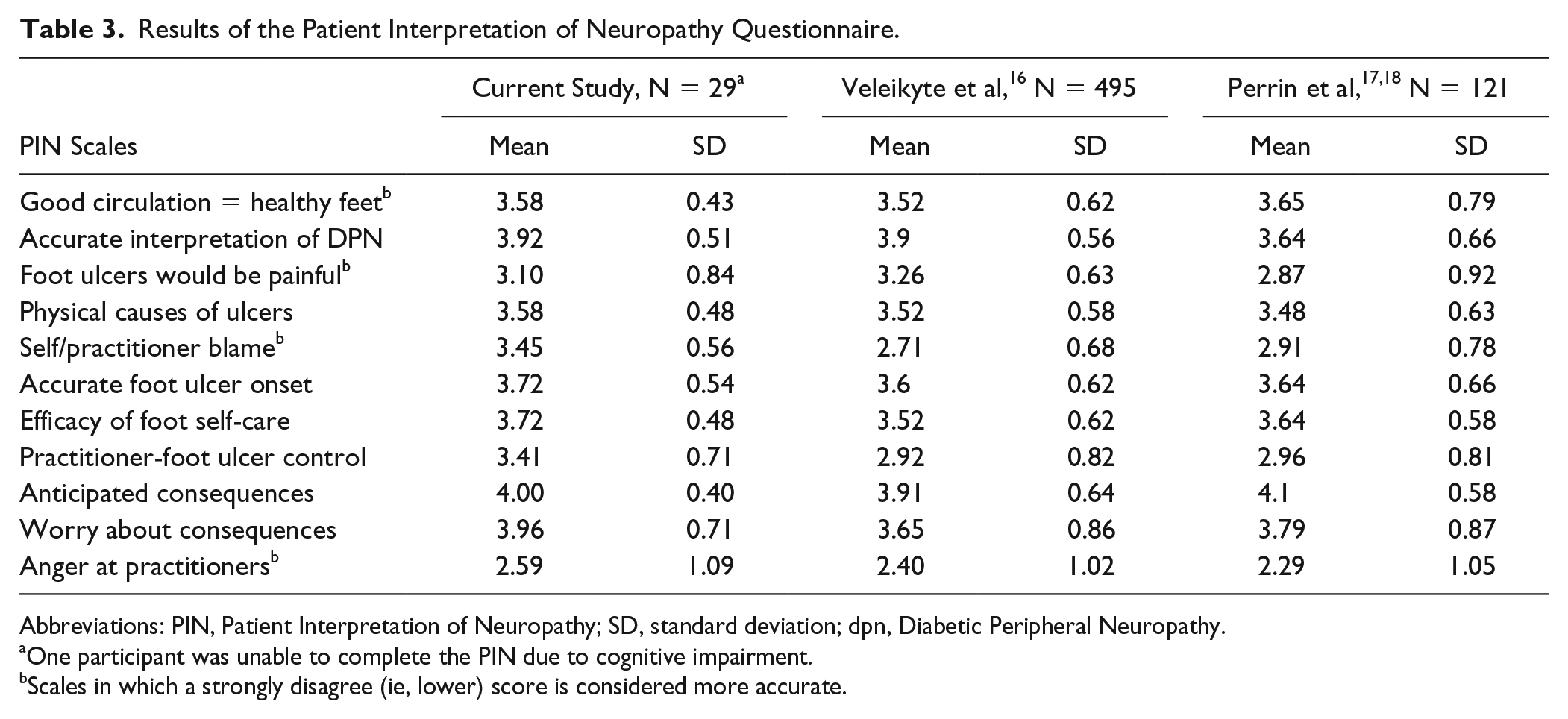
The results of participants’ PIN responses are shown in Table 3, along with the data reported by Vileikyte et al 16 and Perrin et al 18 on this measure. One participant, scoring 12/30 on MoCA, was unable to participate in the PIN, due to cognitive impairment, and thus the PIN results are reported for N = 29. There were also 5 other missing data points from the PIN, when participants had inadvertently skipped items on the form, during administration.
Results of the Patient Interpretation of Neuropathy Questionnaire.
Abbreviations: PIN, Patient Interpretation of Neuropathy; SD, standard deviation; dpn, Diabetic Peripheral Neuropathy.
One participant was unable to complete the PIN due to cognitive impairment.
Scales in which a strongly disagree (ie, lower) score is considered more accurate.
The PIN results from the current study largely parallel the Vileikyte et al 16 and Perrin et al 18 findings with 2 exceptions. The mean scores in the current study on the “Self/Practitioner Blame” subscale, within the cause domain (3.45, SD = 0.56), are higher than those reported by Vileikyte et al 16 (2.71, SD = 0.68) and Perrin et al 18 (2.91, SD = 0.78), along with higher scores on the “Practitioner Foot Ulcer Control” subscale, within the controllability domain (3.41, SD = 0.71) compared with the mean scores reported by Vileikyte et al 16 (2.92, SD = 0.82) and Perrin et al 18 (2.96, SD = 0.81).
Correlation Between Cognitive Functioning, Understanding of Neuropathy, HbA1c, and Length Since Diabetes Diagnosis
A significant moderate positive correlation was found between MoCA scores and the Acute Foot Ulcer-Onset PIN scale (r = 0.45, P = .0158; Table 4). A weak nonsignificant positive correlation was also found between MoCA scores and the Practitioner-Foot Ulcer Control PIN scale (r = 0.32, P = .0965). Similarly, a weak nonsignificant negative correlation was found between MoCA scores and the number of years since diabetes diagnosis (r = 0.30, P = .1185).
Associations Between Cognitive Functioning, Understanding of Neuropathy, and HbA1c.
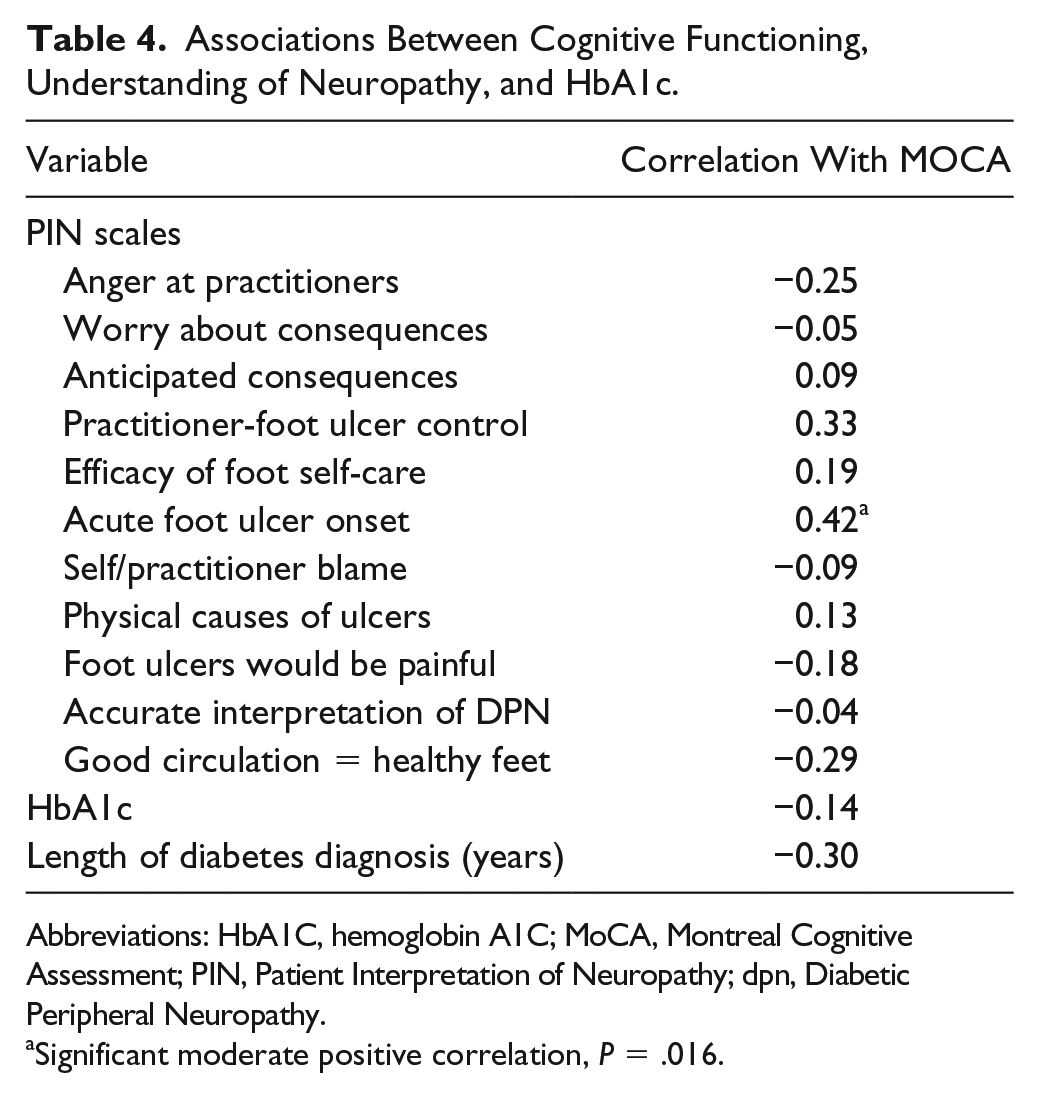
Abbreviations: HbA1C, hemoglobin A1C; MoCA, Montreal Cognitive Assessment; PIN, Patient Interpretation of Neuropathy; dpn, Diabetic Peripheral Neuropathy.
Significant moderate positive correlation, P = .016.
Discussion
The results of the study indicate that cognitive functioning, as assessed by the MoCA screening tool, is reduced in individuals with diabetes-related foot ulcers requiring hospitalization. In this study, the mean MoCA of 22.37 (SD = 3.65) falls below previous studies of English language administered MoCA assessments in cohorts aged late 50s to early 60s where the mean score ranged from 23.37 (SD 3.79) 20 to 27.32 (SD 1.28). 21 MoCA cutoff scores for determining Mild Cognitive Impairment also vary, with some studies recommending a cutoff score of <26 and others a cutoff score of <23.22,23 Three quarters of the current sample scored below the higher cutoff score, with 43% scoring below the lower criterion. Also of note, one quarter of the sample had MoCA means scores (<20) consistent with patients diagnosed with dementia.24,25
In all previously known studies that have used the MoCA for cognitive screening in individuals with diabetes, foot wound status has not been reported.11,12,26 The MoCA results of the current study were higher than those obtained by Özcan and Demir 12 in a much older diabetes cohort (MoCA mean 15.53, SD = 6.18; age mean 71.27, SD = 8.57). The results were similar to those reported by Mori et al 11 in a patient group with comparable HbA1c scores, but an older age group (MoCA mean 26.45, SD = 2.6; HbA1c man 9.6, SD = 1.8; age mean 67.3 years, SD = 9.9). However, the current MoCA scores were lower than those reported by Alagiakrishnan et al 26 in a similar aged diabetes cohort (MoCA mean 26.45, SD = 2.6; age mean 59.9 years, SD = 7.1). This appears to indicate cognitive decline in individuals with foot ulcers, beyond expectation for both their age and diabetes status.
The PIN data of the current cohort are largely similar to the subscale means obtained in the studies by Vileikyte et al 16 and Perrin et al, 18 with the exception of the subscales “Self/Practitioner Blame” and “Practitioner Foot Ulcer Control.” The higher “Self/Practitioner Blame” subscale scores in the current cohort indicates a higher level of blame for participants’ foot health leveled toward poor medical care in the past, not taking good care of their diabetes, or generally not taking care of oneself. Using the framework of the Common Sense Model of Illness, 19 this relates to the Cause domain. The current cohort scored also comparatively higher than previous studies on the “Practitioner Foot Ulcer Control” subscale, indicating a stronger belief that medical practitioners can prevent foot ulceration. This relates to the Controllability domain within the model of illness framework. There may be several reasons for the differences in these areas. All but one participant in the current patient group had experienced multiple foot ulcers. Thus, the cohort may have had difficulty taking in and applying information about how to prevent future wounds. Alternatively, this group may have been more passive in their self-care and disease self-management. Both of these suppositions require further investigation.
Analyzing the results from the PIN questionnaire as an overall illness schema, Perrin et al 18 identified three distinct “clusters” of people with diabetes with differing perceptions of peripheral neuropathy and its sequelae. These included a group who generally reported broad misperceptions about their condition, a group who were more realistic and a group who were uncertain. The “misperceiver” cluster was found to participate in a higher rate of potentially damaging foot-care behaviors, which could contribute to the development of foot ulcers. While specific cluster analysis was not undertaken in this current study, the pattern of results for the PIN subscales closely resembles those for the Misperceivers cluster found by Perrin et al 18 (albeit with a greater standard deviation range for most scale means, consistent with the smaller sample size).
The correlation analysis indicates that participants with higher MoCA scores tend to provide more accurate answers on the Acute Foot Ulcer Onset PIN subscale. This PIN subscale is composed of 3 items related to how quickly and easily foot ulcers can develop. Cognitive impairment may contribute to poorer scoring on this scale. While correlation does not infer causation, it is possible that reduced recall (memory) about foot ulcer education results in lower scores on this scale. Alternatively, reduced executive functioning in the areas of sequential and flexible reasoning may mean that individuals do not make links about causality from their own experiences of foot ulcer(s) with known risks for foot ulcer onset. This is important as individuals with peripheral neuropathy need to be aware that trauma to the skin and subsequent ulceration can occur quickly.
Another important clinical observation about the utilized assessment tools was the difficulty experienced by some participants in completing the PIN. Several participants skipped PIN items, and this appeared to be due to unintentional oversights, related to attentional monitoring. The clinician data collector was present at the time of the questionnaire administration, and available to answer queries about questions the participants did not understand; however, it is also possible that items were skipped due to difficulty in understanding the questions. Additionally, one participant was not able to complete the PIN due to their level of cognitive impairment. Thus, it may not always be possible to administer the PIN to individuals with diabetes-related foot ulcers with higher levels of co-morbid cognitive dysfunction.
Presently, psychological interventions for individuals with diabetes focus on supporting and enabling self-management.27-29 Self-management programs are widely reported to help individuals manage chronic conditions and in diabetic populations self-management education programs have demonstrated improvement in psychological well-being, reduction in glycosylated hemoglobin levels, and improved systolic blood pressure. However, due to reduced cognitive functioning, this may not be a meaningful or useful intervention approach for a proportion of individuals with diabetes with foot ulcers requiring hospitalization due as comprehension of multiple variables in a complex dynamic system is required to solve problems in real-life situations. 30 Techniques, such as motivational interviewing, that focus on an individuals’ motivation to change, without determining an individual’s capacity to translate this motivation into action, due to cognitive impairment, may be less effective. Support for individuals should take into account cognitive difficulties that might affect an individual’s ability to understand, interpret, retain, and implement information. Individuals may have difficulty generating solutions to problems or translating education across varied situations. In addition, individuals with identified misperceptions regarding their understanding of neuropathy may undertake a higher rate of potentially damaging foot-care behaviors, which could contribute to the development of foot ulcers. This should be considered when education is provided, and expectations and support adjusted to accommodate individuals with cognitive impairment and maladaptive health beliefs.
Clinically, knowledge of the MoCA results in this patient cohort can assist in management planning by the interdisciplinary DFU team, as it provides knowledge about cognitive difficulties and enables management plans to be adjusted as a result. 30 Strategies that have been implemented by the DFU to circumvent or minimize the impact of cognitive difficulties include reducing the complexity of ulcer management; changing education strategies and approaches to treatment goal discussions; provision of assistance with the coordination of appropriate services and supports; and clear communication with other services involved in the individual’s foot care. Specifically, the modification of communication and education included repetition of information, the use of visual aids, providing written instructions, simplification of language, reductions in the number of concepts discussed, and reduction in the number of staff present when providing education or discussing treatment goals. Coordination of services the individual required and the support necessary to enable access and utilization of services were informed by the individual’s cognitive functioning, for example, communicating medication blister pack adjustments with pharmacists directly rather than providing an additional prescription to the individual. The MoCA results were also relayed to the participant’s general practitioner in their discharge summary for ongoing monitoring.
The results of the current study support the implementation of routine cognitive screening in individuals admitted with diabetes-related foot ulcers. Further research would be useful that investigates other psychological factors, such as personality, mood, and other mental health conditions in the population and the impact these may have on effective care and management.
Limitations of Study
This study assessed cognition and understanding of neuropathy in a convenience sample of inpatients of a specialized tertiary DFU, all of whom were referred for at least one session with the unit’s psychologist. A limitation of the study is the smaller sample size (N = 30). The results of this study are limited in their interpretation to individuals with diabetes with serious foot ulcers. Investigation of cognition and understanding of neuropathy in individuals accessing routine community outpatient wound management services would allow more generalization to all individuals with diabetes-related foot ulcers. Further research investigating psychological comorbidities, social supports, and detailing previous ulcer management and diabetes-related foot ulcer education would be valuable in gaining an understanding of the variety of factors influencing cognition and health condition knowledge in this population.
Footnotes
Acknowledgements
We thank the Melbourne Health, Royal Melbourne Hospital, Diabetic Foot Unit, and Participants involved in this study for their support in conducting this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.